Download - Neuroleptic anesthesia, agents and uses

NEUROLEPTIC ANESTHESIA, AGENTS AND USES
DR. ARJUN CHHETRI

ANTIPSYCHOTIC (neuroleptic) DRUGS
Diverse group of compounds ( phenothiazines, thioxanthenes, butyrophenones).
Useful in Rx schizophrenia, mania, depression with psychotic.
Also used in tourette syndrome and certain movement disorder.
Antiemetic. Phenothiazines and thioxanthenes have high
T.I accounts safety over wide dose range.
CONTD….
Even large dose unlikely to cause life- threatening depression of ventilation.
Do not produce physical dependence.
Although abrupt discontinuation results skeletal muscle discomfort.

CHEMICAL STRUCTURE
PHENOTHIAZINE
THIOXANTHENE
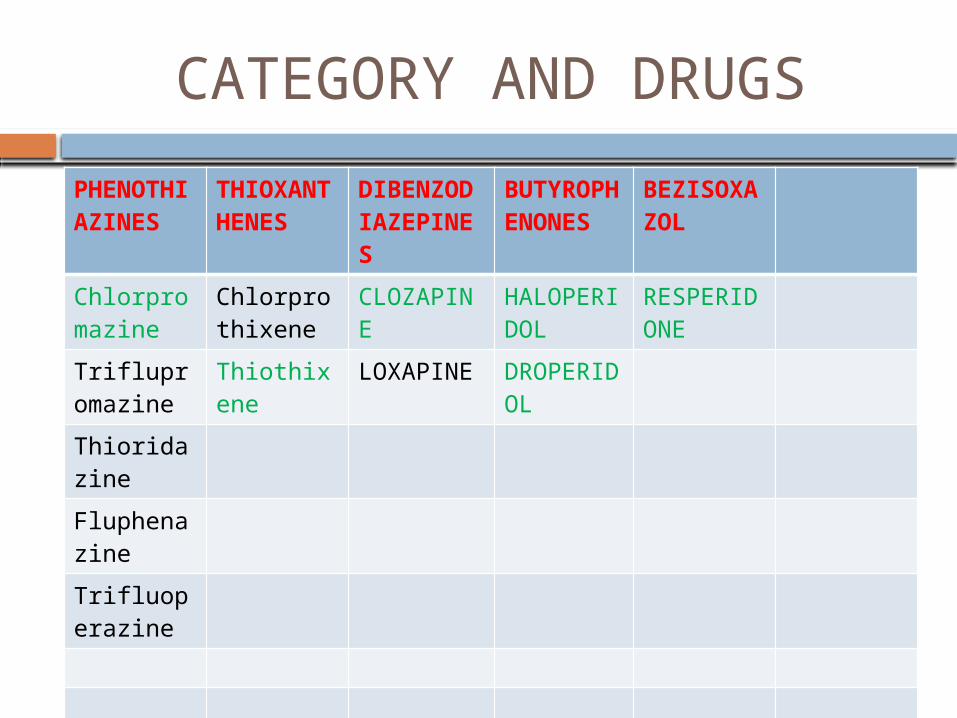
CATEGORY AND DRUGS
PHENOTHIAZINES
THIOXANTHENES
DIBENZODIAZEPINES
BUTYROPHENONES
BEZISOXAZOL
Chlorpromazine
Chlorprothixene
CLOZAPINE
HALOPERIDOL
RESPERIDONE
Triflupromazine
Thiothixene
LOXAPINE DROPERIDOL
Thioridazine
Fluphenazine
Trifluoperazine

COMPARTIVE PHARMAOLOGY

MECHANISM OF ACTION
MOA due to blockade of dopamine receptor(D2 receptor) in the basal ganglia and limbic portion of forebrain.
Achieve max efficacy over a period of weeks.
Interference with neurotransmitter function of dopamine suggested by EPS.
Blockade of dopamine receptor at CTZ of medulla responsible for antiemetic effect.
PHARMACOKINETICS
Phenothiazines & thioxanthenes display erratic and unpredictable patterns of absorption after PO.
Highly lipid soluble and accumulate in well per fused tissues.
Passage across the placenta and accumulation is possible.
Avid protein binding in plasma and tissues limits effectiveness of hemodialysis in removing these drugs.
CONTD….
METABOLISM Principally by oxidation in liver followed by
conjugation. Most oxidative metabolite pharmacologically
inactive exception being 7- hydroxychlorpromazine.
Appear primarily in urine and lesser extent in bile. Elimination half life 10-20 hrs permitting OD dose
interval. Elimination half-life prolonged in fetus and elderly.

SIDE EFFECTS
Exception of clozapine, chronic use of Phenothiazines & thioxanthenes Complicated by serious side effects. Reflecting drug-induced blockade Of dopamine receptors, especially in Forebrain. Despite side effects , have large margin
of safety and overdoses are rarely fatal.

EXTRAPYRAMIDAL EFFECTS
Tardive dyskinesia may occur 20% who receive APD > 1years.
Elderly and women of all age are more sussceptible
Manifestations include abnormal involuntary movements i.e may effects tounge, facial and neck muscles, upper & lower extremities, truncal musculature.
Occasionally skeletal muscle group involved in breathing and swallowing.
EPS CONTD…
TD rarely remits and there is no treatment. Compensatory dopamine increases in B.G may
responsible.
Acute dystonic reactions Occur in approx 2% of treated patients with in
first 72 hrs of therapy. Young men and in patients taking high-potency
drugs. Acute skeletal muscle rigidity & cramping may
develop

EPS CONTD….
Musculature of the neck, tongue, face, and back.
Opisthotonos and oculogyric crises may occur.
Sudden respiratory distress reflects laryngeal dyskinesia (laryngospasm).
Respond dramatically to diphenhydramine 25-50 mg IV.
Patient with antipsychotic- induced akathisia often appears restless which may confused with underlying psychotic disorder.

CARDIOVASCULAR EFFECTS
IV administration of chlorpromazine causes decrease in systemic BP resulting from
I. Depression of vasomotor reflexes mediated by brainstem.
II. Peripheral alpha- adrenergic blockade.III. Direct relaxant effects on vascular smooth
muscle.IV. Direct cardiac depression. Risperidone associated with exaggerated
systemic hypotension during spinal anesthetic. Reflecting risperidone-induced alpha blockade.

CVS CONTD….
Alpha- adrenergic blockade is sufficient to blunt or prevent the pressor effects of epinephrine.
Miosis occur also due to alpha-adrenergic blockade. A cardiac antidysrhythmic effects of chlorpromazine may reflect potent LA activity of this drugs. Antipsychotic drugs prolong the QTc interval on ECG
thus predispose to the development of VT. Oral administration associated with less systemic BPlowering effects.

NEUROLEPTIC MALINGNAT SYNDROME
Occur in 0.5%- 1%. Risk factor for development dehydration &
intercurrent illness. Typically develop over 24- 72 hrs in young men
and characterized byi. Hyperthermia.ii. Generalized hyper tonicity of skeletal muscle.iii. Instability of ANS manifesting as alteration in
SBP, tachycardia, and cardiac dysrhythmias.iv. Fluctuating levels of consciousness.

NMS CONTD….
Increased skeletal muscle tone may decreased chest wall expansion which required mechanical support for ventilation.
Skeletal muscle rigidity may severe enough cause myonecrosis, leading to raised CPK level, myoglobinuria, and renal failure.
Liver transaminase enzyme may elevated. Mortality 20%- 30%. common cause of death being ventilatory
failure, cardiac failure/ dysrhythmias, renal failure and thromboembolism.

NMS CONTD….
Cause unknown As a result Rx is empirical and supportive
measure. Direct acting muscle relaxant DONTROLENE. Dopamine agonist BROMORIPTINE &
AMANTADINE. Malignant hyperthermia & central
anticholinergic syndrome may mimic NMS. Distinguished by NDMA produced flaccid
paralysis in NMS not in malignant hyperthermia.
ENDOCRINE EFFECTS
Prolactin level increased due to blockade of dopamine receptors.
Galactorrhea and gynecomasita. Amenorrhea possible but rare. Chlorpromazine may impair glucose
tolerance and release of insulin. Hypothalamic effects manifest as weight
gain and abnormal thermoregulation.

SEDATION
Sedation due to antagonism of α1-adrenergic, muscarinic, and H1 receptors.
With chronic therapy tolerance develop to the sedation effects.
ANTIEMITIC EFFECTS
Antiemetic effects reflects interaction with dopamine receptors in CTZ in medulla.
Effecting in preventing opioid induced NOV. Perphenazine 5 mg IV as effective as
ondansetron 4 mg IV. Droperidol 1.25 mg IV prevent PONV after in
gynecologic surgery. Unlike others, Perphenazine not associated
with sedation and hypotension so useful as an inexpensive prophylactic antiemetic.

OBSTRUCTIVE JAUNDICE
OJ considered as an allergic reaction.
Occur rarely 2 to 4 weeks after phenothiazines or thioxanthenes administration.
If jaundice not observed in first months of therapy, unlikely to occur later.

HYPOTHERMIA
Effects of chlorpromaizine on hypothalamus responsible for poikilothermic effects.
In past this effects used to facilitate the production of surgical hypothermia.

DRUG INTRACTIONS
Ventilatory depressant effects of opioids exaggerated.
Likewise, miotic and sedative effects of opioid increased.
Analgesic action likely to be potentiated.
Interfere with exogenously administered dopamine.

CLOZAPINE
Belongs to DIBENZODIAZEPINES category.
Only APD does not cause tardive dyskinesia or EPS.
Common side effects- sedation, NOV, orthostatic hypotension.
Low grade fever sometimes occurs in early use.
Safely combined with lithium and other APD.
Excessive sedation if combined with benzodiazepine.

CONTD….
AGRANULOCYTOSIS is the serious side effects.
Occur in < 1% WBC weekly monitoring is required. High dose associated with incident of
seizure in 2% to 4%. Anticonvulsant is required. Valporic acid may be selected as it does
not alter clozapine metabolism.

BUTYROPHENONS
DROPERIDOL and HALOPERIDOL Structurally and pharmacologic effects similar
to Phenothiazines and thioxanthenes. Decrease anxiety that accompanies psychosis
but less effective that accompanies preoperative period
Droperidol most often administered pre-op period.
Haloperidol has longer duration of action and lack α-adrenergic antagonist effect thus decreased SBP are unlikely.
CONTD….
Principle use of haloperidol as long acting APD and Rx of agitation and delirium in ICU.
ZIPRASIDONE atypical APD use an alternative in delirium.
Like haloperidol it is also associated with EPS and tardive dyskinesia and cause prolongation of QTc interval on ECG.
Not recommended in patient with QTc>500msec, recent MI, uncompensated CHF.

PHARMACOKINETICS
Patient anesthetized with N2O-Fentanyl, elimination half-time of Droperidol is 104 min.
Clearance is 14.1mL/kg/min, Vd 2.04L/kg.
Short elimination half-life is not consistent with prolonged CNS effects which reflects slow dissociation of the drug from receptors or retention of Droperidol in brain.
Metabolized in liver with maximal excretion of metabolites occur during first 24 hrs.

SIDE EFFECTS
Side effects is nearly as same as Phenothiazines and thioxanthenes.
CNS: As a dopamine antagonist, Droperidol evoke EPS in
abt 1% of patients. As a result should be avoided in Parkinson disease. Acute laryngeal dystonia is rare. Diphenhydramine IV is effective. Droperidol is a cerebral vasoconstrictors i.e cause in
CBF bur CBMO2 is not altered. Droperidol does not produce amnesia nor have
anticonvulsant action.

CONTD….
CVS: SBP decrease due to its action on CNS and
by peripheral α-adrenergic blockade. Hypotension is minimal, occasionally patient may
experience marked hypotension. Myocardial contractility is not altered by droperidol. Hypertension has been reported after droperidol
administration in a patients with pheochromocytoma.

CONTD….
Droperidol is a cardiac antidysrhythmic drug. Protect against epinephrine-induced
dysrhythmias. Mechanism is unknown but may reflects
blockade of α-adrenergic receptors in myocardium, decreased in SBP i.e decrease the likelihood of pressure dependent cardiac dysrhythmias.
Large dose 0.2 – 0.6 mg/kg decrease conduction of cardiac impulses along accessory pathways responsible for tachydysrhythmias i.e. occur in patient with wolf Parkinson- white syndrome
CONTD…
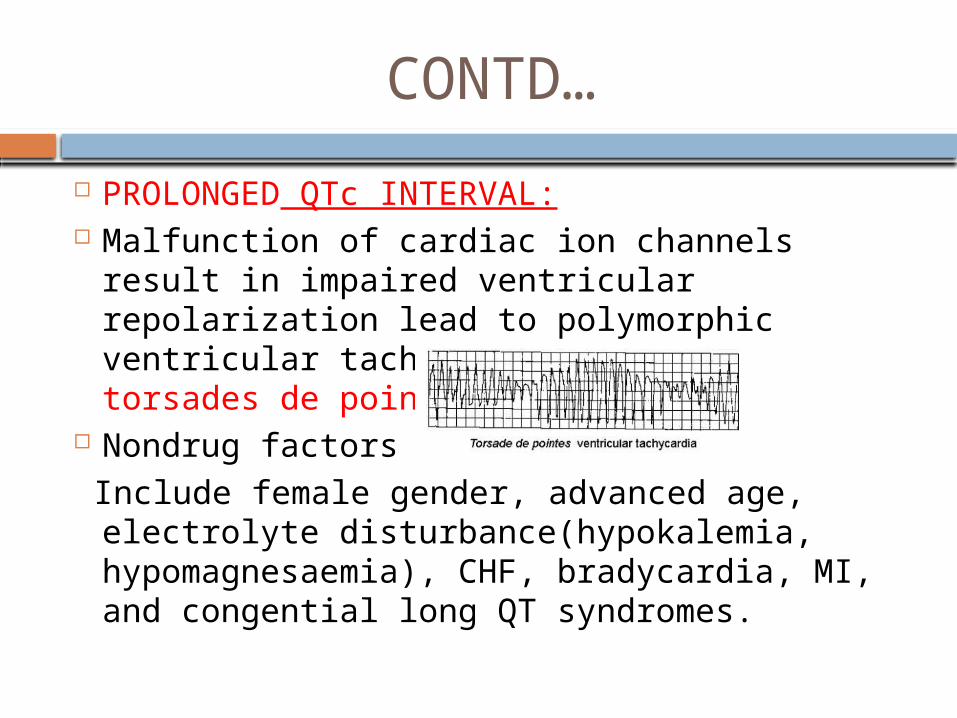
PROLONGED QTc INTERVAL: Malfunction of cardiac ion channels result in
impaired ventricular repolarization lead to polymorphic ventricular tachycardia known as torsades de points.
Nondrug factors Include female gender, advanced age,
electrolyte disturbance(hypokalemia, hypomagnesaemia), CHF, bradycardia, MI, and congential long QT syndromes.

CONTD…..
Noncardiac drugs, droperidol, thiopental, propofol, isoflurane, sevoflurane, SUX, neostigmine, atropine, glycopy, metoclopramide, macrolide.
Produce dose dependent QTc prolongation on ECG.
Droperidol induced QTc prolongation effects peak 2-3 min following IV , effects last for several hours.
Case of QTc prolongation occurred in patient receiving at 1.25-2.5mg as well as 0.625-1.25mg.
CONTD….
“BLACK BOX WARNING” has been added to the package of droperidol.
All patient should undergo 12 lead ECG prior to given
When Rx with droperidol is selected ,ECG monitoring should been performed before and continuous for 2-3 hrs.
Caution to the patient who are at risk of developing QTc prolongation(CHF, BRADYCARDIA, HYPOKALEMIA, ELDERLY) .
Sudden death during HALOPERIDOL reflects drug induced prolongation of the QTc interval in ECG.

NEUROLEPTANALGESIA
Droperidol combined with fentanyl. Commercially available 50:1 combination
of droperidol with fentanyl known as INNOVAR.
This fixed combination not associated depression of ventilation as either drug alone.
Droperidol does not enhance analgesia but rather prolongs duration of action.
Orthostatic hypotension and dysphoria are more with innovar compared with fentanyl alone.
CONTD….
Neuroleptanalgesia characterized by trance-like immobility in a patient who is dissociated and indifferent to the external surrounding.
Analgesia is intense.
Suitable in diagnostic and minor surigical procedureLike bronchoscopy and cystoscopy.
Disadvantage like prolonged CNS depression and failure to depress sympathetic NS.

CONTD…
Mechanism is unknown but likely involves inhibition of synaptic transmission by ligand-gated ion channels.
Evidence suggest that droperidol inhibits activation of GABA and nACHRs receptors that might results in anxiety, dysphoria, and restlessness that limits its clinical usefulness of high-dose droperidol anesthesia.

ANTIEMETIC
Powerful antiemetic .
Inhibit dopamine receptors in CTZ of the medulla.
Over three decades, Droperidol (0.625-1.25mg IV) become widely accepted as a safe, cost effective first line therapy for PONV.
Motion sickness is not influneced by droperidol.
THANK YOU







