October 28, 2003
Gases and Toxic Inhalation
1
Hazardous Material Medical CareGas and Toxic Inhalationน.พ . สั�มมน โฉมฉาย
สาขาพิ�ษวิ�ทยาคลิ�นิ�ค อาชี�วิเวิชีศาสตร์� แลิะ เวิชีศาสตร์�ส��งแวิดลิ�อม
ภาควิ�ชีาเวิชีศาสตร์�ป้�องกั นิแลิะส งคมคณะแพิทยศาสตร์�ศ�ร์�ร์าชีพิยาบาลิ
มหาวิ�ทยาลิ ย มห�ดลิ
[email protected]@hotmail.com

October 28, 2003
Gases and Toxic Inhalation
2
Outline• Inhalation exposure• Asphyxiants
– Simple asphyxiants– Systemic asphyxiant
• Irritant gases• Smoke inhalation• Semiconductors gases

October 28, 2003
Gases and Toxic Inhalation
3
Inhalation exposure
• The most common hazardous material exposure
• Involves large number of cases• Low potential for secondary
contamination• Asphyxiant:
– Simple asphyxiant– Systemic asphyxiants

October 28, 2003
Gases and Toxic Inhalation
4
Simple asphyxiants• Displace oxygen from ambient air
• Decrease FiO2
• Inadequate oxygen for hemoglobin saturation• No pharmacological effects• Needs high ambient concentration to cause
asphyxia• Situations:
– Confined space– High ambient concentration -- compressed
liquefied gas
October 28, 2003
Gases and Toxic Inhalation
5
Simple asphyxiants: Clinical manifestations• Symptoms of hypoxia• CVS and CNS effects predominate• No hypercapnia• No dyspnea until severe hypoxia• Many cases pass out and die
before developing obvious symptoms
October 28, 2003
Gases and Toxic Inhalation
6
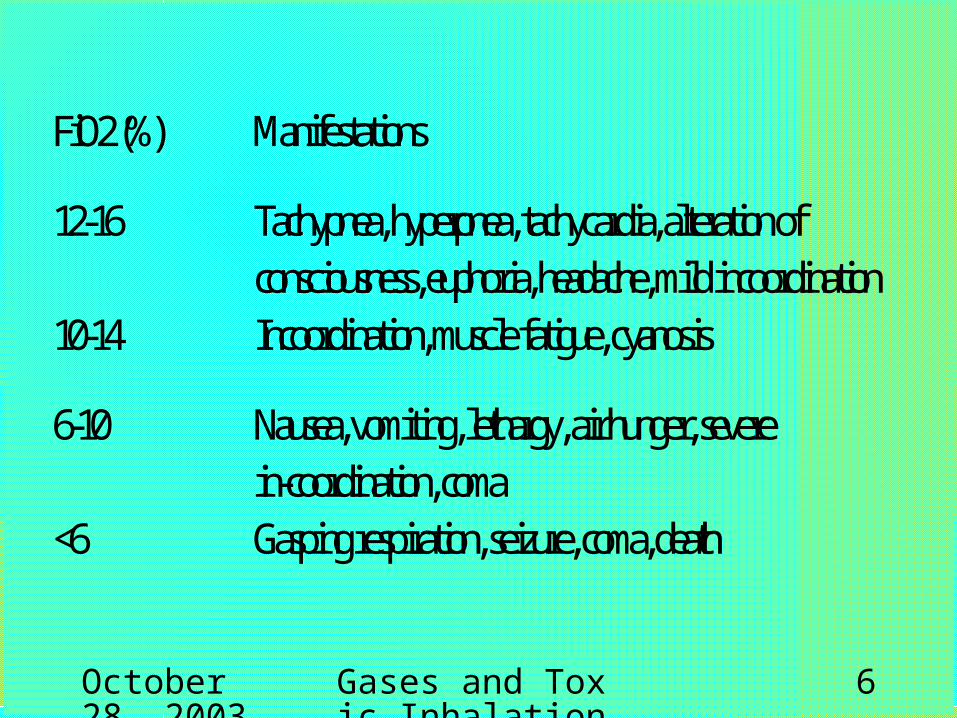
FiO2 (%) Manifestations
12-16 Tachypnea, hyperpnea, tachycardia, alteration ofconsciousness, euphoria, headache, mild incoordination
10-14 Incoordination, muscle fatigue, cyanosis
6-10 Nausea, vomiting, lethargy, air hunger, severein-coordination, coma
<6 Gasping respiration, seizure, coma, death

October 28, 2003
Gases and Toxic Inhalation
7
Simple asphyxiants: specific agents• Noble gases: Helium, argon, xenon• Short chain-aliphatic hydrocarbon
gases: methane, ethane, propane, butane
• Carbon dioxide• Nitrogen gases
October 28, 2003
Gases and Toxic Inhalation
8
Simple asphyxiants: treatment• Decontamination: not needed• Removal from exposure• Respiratory support
– Supplemental oxygen– Ventilation if needed– No role of hyperbaric oxygen
October 28, 2003
Gases and Toxic Inhalation
9
Systemic asphyxiants
• Carbon monoxide• Cyanide• Hydrogen sulfide

October 28, 2003
Gases and Toxic Inhalation
10
Carbon monoxide (CO)
• A leading cause of death from poisoning in western countries
• Carbon monoxide: product of combustion of organic materials
• Colorless, odorless and non-irritating gas• Major sources in Thailand:
– Smoke inhalation – Exposure to methylene chloride (paint remover):
•inhalation, skin, ingestion•conversion into carbon monoxide
October 28, 2003
Gases and Toxic Inhalation
11
Carbon monoxide poisoning• CO is inhaled and absorbed at the rate proportional
to respiration• Confined to blood and 15% to tissue predominately
myoglobin• Elimination by gas exchange with half-life 4-6
hours at room air• CO 200-250 times affinity to hemoglobin when
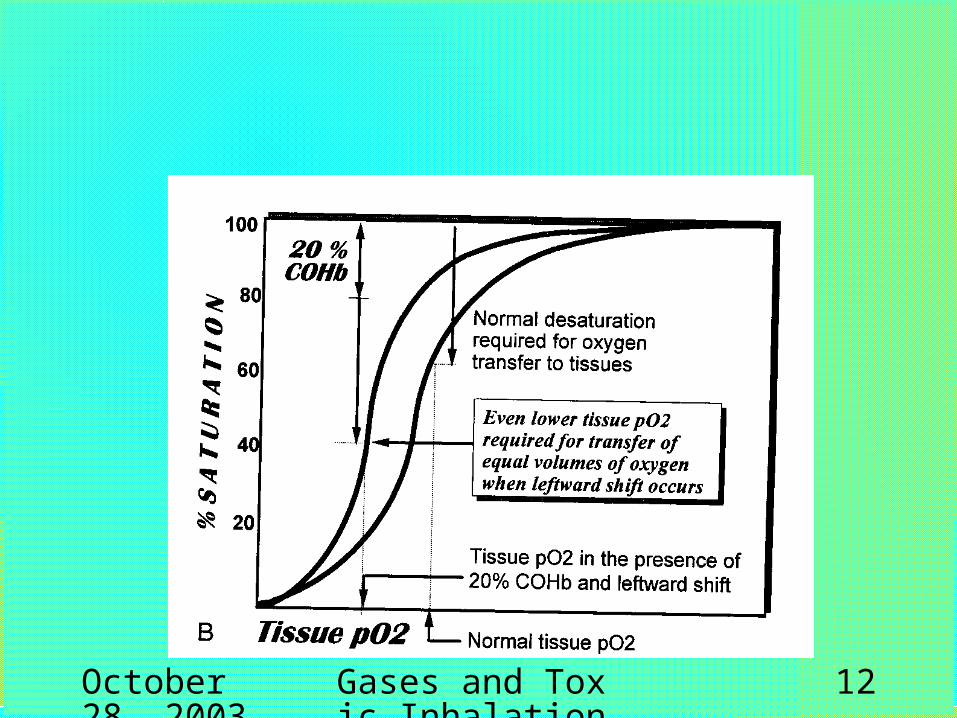
compared to oxygen• Shift oxyhemoglobin dissociation curve leftward• CO 60 times affinity to myoglobin when compared
to oxygen
October 28, 2003
Gases and Toxic Inhalation
12

October 28, 2003
Gases and Toxic Inhalation
13
Acute carbon monoxide poisoning• ‘Flu-like symptoms’• Headache and dizziness• Nausea, weakness, difficulty with
concentration• Mild tachycardia and tachypnea • Syncope, seizures, altered mental status• Acute metabolic acidosis• Cherry red skin
October 28, 2003
Gases and Toxic Inhalation
14
• Anginal chest pain in patients with predisposing coronary artery disease
• Ischemic heart disease, cardiac arrhythmias and complications of IHD
Acute carbon monoxide poisoning
October 28, 2003
Gases and Toxic Inhalation
15
Acute carbon monoxide poisoning: Diagnosis• History: exposure history• Acute unconsciousness/ acute
metabolic acidosis• Pulse oximetry may overestimate
oxygen saturation; thus ABG should be used.
• Confirmation: Carboxyhemoglobin

October 28, 2003
Gases and Toxic Inhalation
16
• Normal (non-smoker): 5% or less/Normal smoker: up to 12%
• Serious toxicity with level 25% or more• A comatose person may have a level close to
zero.• Elevation of carboxyhemoglobin just confirms the
poisoning.• In a patient with altered mental status, CT scan
may show hypodensity change in globus pallidus and subcortical white matter as early as 6 hours after severe poisoning
Acute carbon monoxide poisoning: Carboxyhemoglobin

October 28, 2003
Gases and Toxic Inhalation
17
October 28, 2003
Gases and Toxic Inhalation
18
• Removal from exposure• 100% oxygen therapy
– Promotes tissue oxygenation– Enhance CO elimination– Half-life of 1-2 hours– Treat until patients become
asymptomatic, CarboxyHb< 10%
Acute carbon monoxide poisoning: Management
October 28, 2003
Gases and Toxic Inhalation
19
• 40% of cases– treated, completely recovered and appear fine.– Return of symptoms on day 20-40
• Headache, memory and learning problems• Parkinsonism• Symptomatic treatment• 50% recover and 50% permanent
symptoms
Acute carbon monoxide poisoning: long-term complications
October 28, 2003
Gases and Toxic Inhalation
20
Cyanide poisoning• A powerful cellular poisoning• Inhalation exposure
– Hydrogen cyanide gas– Combustion products
• Other exposures: – Ingestion
•Cyanide salts•Cyanogenic plants
– Iatrogenic: infusion of degraded nitroprusside

October 28, 2003
Gases and Toxic Inhalation
21
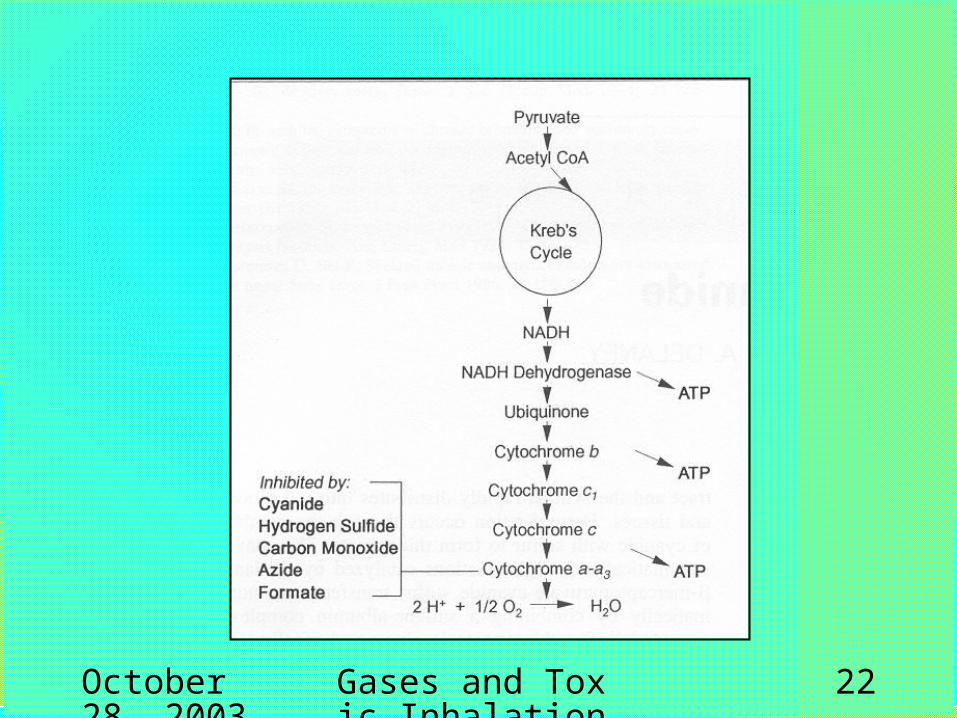
• Rapidly absorbed from respiratory tract• Distribute to RBC and tissues• Elimination by forming thiocyanate and
excrete in urine• Half-life of 2.5 days in persons with normal
renal function
• Binds to Ferric ion in cytochrome a-a3:
– enzyme in mitochondria – catalyzing electron transfer to oxygen
Cyanide poisoning
October 28, 2003
Gases and Toxic Inhalation
22
October 28, 2003
Gases and Toxic Inhalation
23
Cyanide poisoning: Clinical manifestation
• Inhalation: Immediate onset• Low concentration (50 ppm or less): anxiety,
restlessness, dyspnea, palpitation, headache
• Higher concentration (100 ppm): death in 30 minute, tachycardia, tachypnea, syncope, seizures
• High dose (250 ppm): Immediate onset: seizures, bradycardia or asystole, CVS collapse, respiratory depression, coma

October 28, 2003
Gases and Toxic Inhalation
24
Cyanide poisoning: Diagnosis• History
– Exposure: laboratories, jewelry, metal works
• Clinical manifestation– Rapid onset and progression of manifestations– Arterialization of veins in fundoscopy
• Severe type B lactic acidosis• Confirmation: erythrocyte cyanide level (<
50 mcg/L), retrospective
October 28, 2003
Gases and Toxic Inhalation
25
• Removal from exposure• 100% oxygen• Cyanide antidote may not be needed for
inhalation victims who are asymptomatic or recovered before presentation
• Cyanide antidote kit:– Amyl nitrite– Sodium nitrite– Sodium thiosulfate
Cyanide poisoning: treatment

October 28, 2003
Gases and Toxic Inhalation
26
Sodium nitrite• Induces ‘methemoglobinemia’: Hb with
Fe3+
• Cyanide binds with Fe3+
• Sodium nitrite 300 mg ( 10 ml of 3% NaNO2) IV over 5-10 minutes
• Hypotension due to vasodilation• Amyl nitrite in cases of
– Non-medical personal– No available IV line

October 28, 2003
Gases and Toxic Inhalation
27
Sodium thiosulfate
• Enhances cyanide elimination from the body
• Sodium thiosulfate donates sulfur atom to rhodanase-catalyzed reactions to form thiosulfate
• Thiosulfate excreted in urine• Hemodialysis in renal failure• Sodium thiosulfate 12.5 g (50 ml of 25%
sodium thiosulfate)

October 28, 2003
Gases and Toxic Inhalation
28
Hydrogen sulfide
• Colorless gas with sweet odor• Intermediate water solubility• Product of bacterial decomposition
of protein • Industries at risk: Liquid manure &
fertilizer, fishing, brewers, tanning, natural gas & oil exploration, sewer construction

October 28, 2003
Gases and Toxic Inhalation
29
• Inhalation• Irritation of upper and lower respiratory
system• No bioaccumulation• Detoxification within 1 hour• Thiosulfate formation and renal excretion
• Inhibits cytochrome oxidase a3
• Inhibits aerobic metabolism
Hydrogen sulfide poisoning

October 28, 2003
Gases and Toxic Inhalation
30

October 28, 2003
Gases and Toxic Inhalation
31
• Odor threshold 1 ppm characteristic sweet, rotten egg odor
• Olfactory fatigue within 10 minutes with 100 ppm; ‘loss of warning properties’
• Low level: 10 ppm muscle fatigue on chronic exposure
• 50 ppm: Rapid onset of upper respiratory mucosal irritation: ocular pain, keratitis, cough, sore throat, corneal ulceration
Hydrogen sulfide poisoning

October 28, 2003
Gases and Toxic Inhalation
32
• 250 ppm: systemic effects of cellular anoxia– Dyspnea, cough, tachypnea, chest pain– Headache, dizziness, lethargy, confusion,
delirium, seizures, coma– Hypotension, tachycardia, myocardial
ischemia and infarction, arrhythmias
• 1000 ppm: immediate death from respiratory depression and respiratory paralysis
Hydrogen sulfide poisoning

October 28, 2003
Gases and Toxic Inhalation
33
• No specific laboratory from biological sample
• History, clinical manifestations, metabolic acidosis and environmental sampling
• Environmental sampling: ambient hydrogen sulfide level
Hydrogen sulfide poisoning

October 28, 2003
Gases and Toxic Inhalation
34
• Removal from exposure• 100% oxygen• Do not perform mouth to mouth
resuscitation• Amyl nitrite and sodium nitrite for cases
with manifestations of cellular hypoxia• Methemoglobin binds with hydrogen
sulfide into sulfmethemoglobin
Hydrogen sulfide poisoning

October 28, 2003
Gases and Toxic Inhalation
35
Irritant gases
• Large variety of chemicals• Final common pathway:
destruction of the integrity of respiratory mucosal barrier

October 28, 2003
Gases and Toxic Inhalation
36
• Rapid onset of symptoms (seconds to Rapid onset of symptoms (seconds to minutes)minutes)
• Signal to escape the exposureSignal to escape the exposure• Oral, nasal and pharyngeal pain• Mucosal edema, cough, stridor• Conjunctival injection, chemosis, skin
irritation• Gases with good water solubility• Upper airway obstructionUpper airway obstruction
Irritant gases: Clinical manifestationsShort exposureShort exposure

October 28, 2003
Gases and Toxic Inhalation
37
Irritant gases: Clinical manifestationsProlonged exposureProlonged exposure• Gases without rapid onset of manifestation• Entry into lower respiratory tract• Tracheobronchitis, bronchiolitis,
bronchospasm• Acute lung injury, non-cardiogenic
pulmonary edema• Dyspnea, chest tightness, cough, frothy
sputum, wheezing, crackles• CXR: alveolar infiltration• Arterial hypoxemia

October 28, 2003
Gases and Toxic Inhalation
38
Irritant gases: highly water-soluble gases
• Ammonia– Common industrial (plastic, fertilizer,
refrigeration, explosives, cleaning agents) and household gases
– Characteristic odor
– Dissolution: NH4OH
• Chloramine (NH2Cl)– Mixture of hypochlorite and ammonia– Dissolution: hypochlorous acid, ammonia,
oxygen radicals

October 28, 2003
Gases and Toxic Inhalation
39
• Hydrogen chloride– Industrial acid, combustion product of
vinyl chloride– Dissolution: hydrochloric acid
• Hydrogen fluoride– Glassware and semiconductor industry– Hydrofluoric acid– Upper and lower airway irritation,
systemic hypocalcemia
Irritant gases: highly water-soluble gases

October 28, 2003
Gases and Toxic Inhalation
40
• Sulfur dioxide– Smelting and oil refining – Warning properties: odor– Dissolution: sulfurous and sulfuric
acids
Irritant gases: highly water-soluble gases

October 28, 2003
Gases and Toxic Inhalation
41
• Chlorine • Exposure: mixing hypochlorite with acid,
aged hypochlorite tablet, compressed chlorine gas for water chlorination
• Dissolution: Hypochlorous acid• Mild initial upper respiratory symptoms• Delayed symptoms of lower respiratory
tract injury for hours
Irritant gases: intermediate water-soluble
gases

October 28, 2003
Gases and Toxic Inhalation
42
• Phosgene– Colorless gas, heavier than air– Musty odor– exposure
•Combustion products of polyvinyl or isocyanate compounds
•Chemical warfare
Irritant gases: poorly water-soluble gases

October 28, 2003
Gases and Toxic Inhalation
43
• Phosgene– Slowly dissolves into hydrochloric
acid– Prolonged exposure – Upper and lower respiratory tract
irritation– Delayed non-cardiogenic
pulmonary edema up to 72 hours

October 28, 2003
Gases and Toxic Inhalation
44
• Nitrogen dioxide– Reddish-brown color– Water insoluble– Heavier than air– Sources
•Silos: grains•Combustion: nitrocellulose in films and bed mattress
Irritant gases: poorly water-soluble gases

October 28, 2003
Gases and Toxic Inhalation
45
Nitrogen dioxide
• Mild upper airway irritation• Dissolution into nitric and nitrous acids
in bronchiole, terminal bronchiole and alveoli
• Acute non-cardiogenic pulmonary edema
• Pulmonary inflammation and bronchiolitis obliterans 2-6 after the exposure

October 28, 2003
Gases and Toxic Inhalation
46
Nitrogen dioxide
• 1-3 ppm odor• 15 ppm minimal irritation• 50-150 ppm mild irritation• LD50 for 1 hour exposure = 175
ppm• Acute phase: Mucosal irritation (may
last up to 2 weeks), methemoglobinemia

October 28, 2003
Gases and Toxic Inhalation
47
• Delayed: 3-36 hours– Fever dyspnea rales hypoxemia
cyanosis– Perihilar infiltration on CXR
Nitrogen dioxide

October 28, 2003
Gases and Toxic Inhalation
48
• Decontamination: Removal from gas exposure
• Airway management & intubation • Oxygenation and PEEP• Bronchodilator for bronchospasm
•Monitor ECG for patients with hydrocarbon exposure who receive bronchodilator
Irritant gases: management

October 28, 2003
Gases and Toxic Inhalation
49
• Patient with hydrogen fluoride inhalation– Nebulization of 2.5% calcium
gluconate solution (1.5 mL of 10% calcium gluconate with 4.5 ml or NSS or water)
– Prevent fluoride induced hypocalcemia

October 28, 2003
Gases and Toxic Inhalation
50
Smoke inhalation
• Another major mortality factor for patients with burns
• Half of all fire-related deaths are due to smoke inhalation
• Risk for smoke inhalation– Closed-space fire– Decreased mentation: overdose,
alcohol intoxication, drug abuse, head injury

October 28, 2003
Gases and Toxic Inhalation
51
• Combustion or pyrolysis: the rapid decomposition or oxidation of a substance by heat
• Flame (light), heat, smoke• Components of smoke are unpredictable:
composition of the fuels, oxygen availability, heat• Components of exposure from smoke inhalation
– Particulate matters, fumes, aerosols, vapors– Toxic gases
Smoke inhalation

October 28, 2003
Gases and Toxic Inhalation
52
• Heat: Thermal injury– Thermal injury occurs only at
upper airway levels– Quick onset and rapid
progression– Injury below vocal cord occur
only in cases of steam inhalation
Smoke inhalation

October 28, 2003
Gases and Toxic Inhalation
53
• Particulate matters: – Diameter less than 0.5 micrometer
– Products of incomplete combustion of organic materials
– Bronchospasm – Edema of mucosa from upper respiratory
system down to terminal bronchiole– Onset of edema may be delayed up to
24 hours
Smoke inhalation

October 28, 2003
Gases and Toxic Inhalation
54
• Toxic gases from smoke– Carbon monoxide: incomplete
combustion of organic substance– Hydrogen cyanide: Combustion
of nitrogen-containing organic substances: wool, silk, polyurethane, vinyl
Smoke inhalation

October 28, 2003
Gases and Toxic Inhalation
55
Examples of combustion products from common household materials
Materials Combustion products
Wool Carbonmonoxide, hydrogen chloride, phosgene, cyanide
Nylon Ammonia, cyanide
Wood, cotton, paperCarbonmonoxide, formaldehyde
Plastics Cynaide, hydrogen chloride, aldehydes, ammonias, oxides of nitrogen, phosgene, chlorine
Polyvinyl chloride Carbonmonoxide, hydrogen chloride, phosgene, chlorine
Rubber Hydrogen sulfide, sulfur dioxide

October 28, 2003
Gases and Toxic Inhalation
56
• Clues for diagnosis of smoke inhalation– History of closed-space fire– Physical signs
•facial burns, singed nasal hair, soot in the nose and throat, hoarseness, carbonaceous sputum, wheezing
– Carboxyhemoglobin level as a document of exposure to incomplete combustion in a enclosed space
– Chest x-ray may be normal at early stages
Smoke inhalation

October 28, 2003
Gases and Toxic Inhalation
57
• Treatment should start before the definite diagnosis is made
• Early intubation may be needed to maintain airway: Indications for early intubation– Full-thickness burns of the face or perioral region– Circumferential neck burns– Progressive hoarseness– supraglottic edema or inflammation
• 100% humidified oxygen• Carboxyhemoglobin level
Smoke inhalation

October 28, 2003
Gases and Toxic Inhalation
58
Empirical treatment for cyanide poisoning
• A patient with elevated carboxyhemoglobin
• Suspected cyanide poisoning:history, comatose, lactic acidosis
• Administration of sodium nitrite may worsen impaired oxygen transport
• IV Sodium thiosulfate alone

October 28, 2003
Gases and Toxic Inhalation
59
Arsine
• A colorless, non-irritating gas• Heavier than air• Garlic-like odor• Semiconductor industry:
production of gallium arsenide• Reaction of acids with arsenical
compounds

October 28, 2003
Gases and Toxic Inhalation
60
• Arsine depletes RBC glutathione• RBC cell membrane instability• Intravascular hemolysis• Absorbed into the body and is
oxidized to trivalent arsenic compounds and cause chronic arsenic poisoning
Arsine

October 28, 2003
Gases and Toxic Inhalation
61
• Acute inhalation of level 250 ppm or more can cause death
• Long term exposure of level 10-50 ppm can cause acute symptoms
• Chronic low level exposure may cause arsenic poisoning
Arsine

October 28, 2003
Gases and Toxic Inhalation
62
• Intravascular hemolysis• Headache, dizziness, malaise &
weakness• Nausea and vomiting, abdominal pain• Dark-red ‘Cola color urine’ in 4-6 hours• Jaundice in 24-48 • Acute (nephrotoxic) tubular necrosis:
secondary to deposition of RBC breakdown products
Arsine

October 28, 2003
Gases and Toxic Inhalation
63
• Chronic arsenic poisoning• Malaise, nausea, headache• Painful peripheral neuropathy• Hepatitis• Bone marrow suppression• Mee’s line• Skin changes: hyper keratosis and
hyper pigmentation, Bowen’s disease
Arsine

October 28, 2003
Gases and Toxic Inhalation
64
• History of exposure, cluster of cases
• Abdominal pain• Intravascular hemolysis• Garlic-like odor
Arsine

October 28, 2003
Gases and Toxic Inhalation
65
• Acute cases: Transient elevation of urine arsenic levels
• Acute anemia with decreased haptoglobin• Negative Coomb’s test• Hemoglobinuria without hematuria• Hyperkalemia• Acute renal failure• Chronic cases: Elevation of urine arsenic
level
Arsine

October 28, 2003
Gases and Toxic Inhalation
66
Arsine : Treatment
• Decontamination: Removal from exposure
• ABC: 100% oxygen• Supportive care:
– Blood transfusion in case of severe anemia
– Urine alkalinization and maintain urine flow
– Hemodialysis

October 28, 2003
Gases and Toxic Inhalation
67
• No enhancement of elimination• Chelation therapy:
– No indications in acute cases– May be indicated for chronic exposure with
persistent elevation of urine arsenic level• Follow up
– Until stable hemolysis ceases and stable hematocrit
– Subacute and long-term follow up for renal function and chronic arsenic poisoning
• Asymptomatic exposed person should be observed for at least 6 hours

October 28, 2003
Gases and Toxic Inhalation
68
Thank you•Do you have any question?







