

P A I Nfocus on
LBP and HEADACHE
Department Of Neurology
dr. Hasan Sadikin Hospital Padjadjaran University

Definition of PAIN
Pain is unpleasent sensory and emotional experience associated with actual or potential tissue damage, or discribed in term of such damage ( IASP, 1986 )
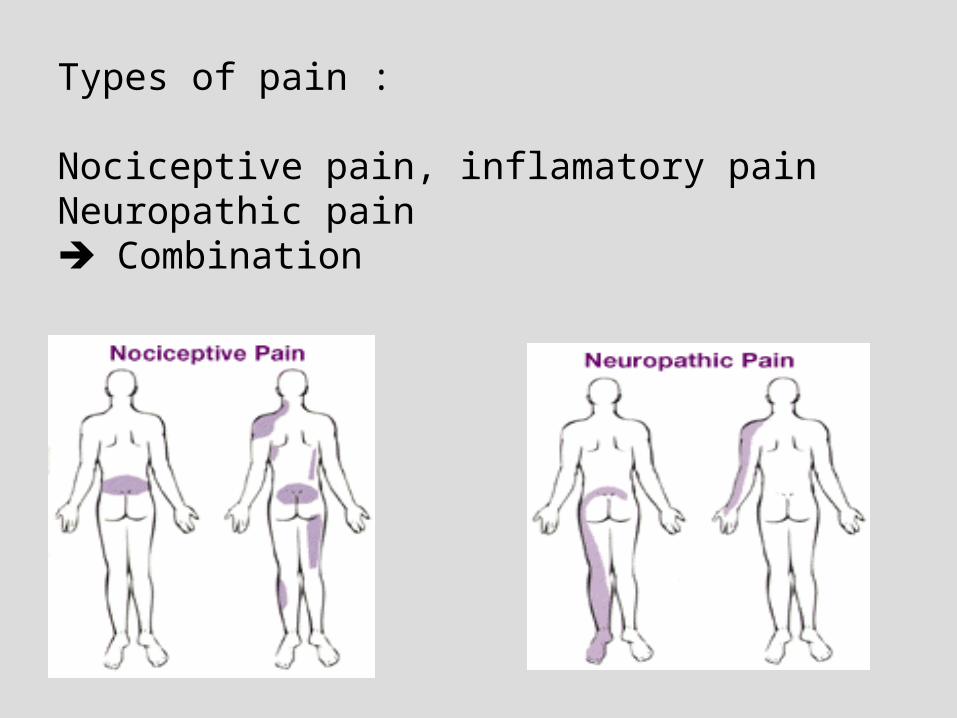
Types of pain :
Nociceptive pain, inflamatory painNeuropathic pain Combination

Pain Clinical Diagnosis
• History taking
• Physical examination, Neurological exam.
• Laboratory examination :
Lab.
Neurophysiology exam.
Neuroimaging

Visual Analog ScalesVisual Analog Scales
00 1010
NoNopainpain
ExcruciatingExcruciatingpainpain
00 1010
CompleteCompletepain reliefpain relief
NoNopain reliefpain relief
McQuay, 1998.Note: Lines must be exactly 100 mm long
FACES SCALES

THE DERMATOMES


Bagaimana Gejala Nyeri Neuropatik ?
HAS/Neuro/RSHS-FKUP
Nyeri Spontan Nyeri dibangkitkan stimulus

Syndromes of Epiconus, Conus and Cauda EquinaSyndrome of lumbal-radiculopathy
LOW BACK PAIN(NYERI PUNGGUNG BAWAH)
• Nyeri di antara sudut iga terbawah dan lipat bokong bawah yaitu di daerah lumbal atau lumbo-sakral dan sering disertai dengan penjalaran nyeri kearah tungkai-kaki

Pain sensitive L-S structures
• Skin, subcutaneous, adipose tissue
• Muscles
• Facet joints, sacroiliaca joints
• Post/ant.longitudinal lig.• Periosteum vertebra (fascia,tendon,aponeurosis)
• Nerve roots• Blood vessels (spinal joint,sacroiliaca joint, verteb,
L-S muscles)

Estimated Prevalence of NeP
HAS/Neuro/RSHS-FKUP
Indonesia : 40% population, men>women hospital based : 3-17%
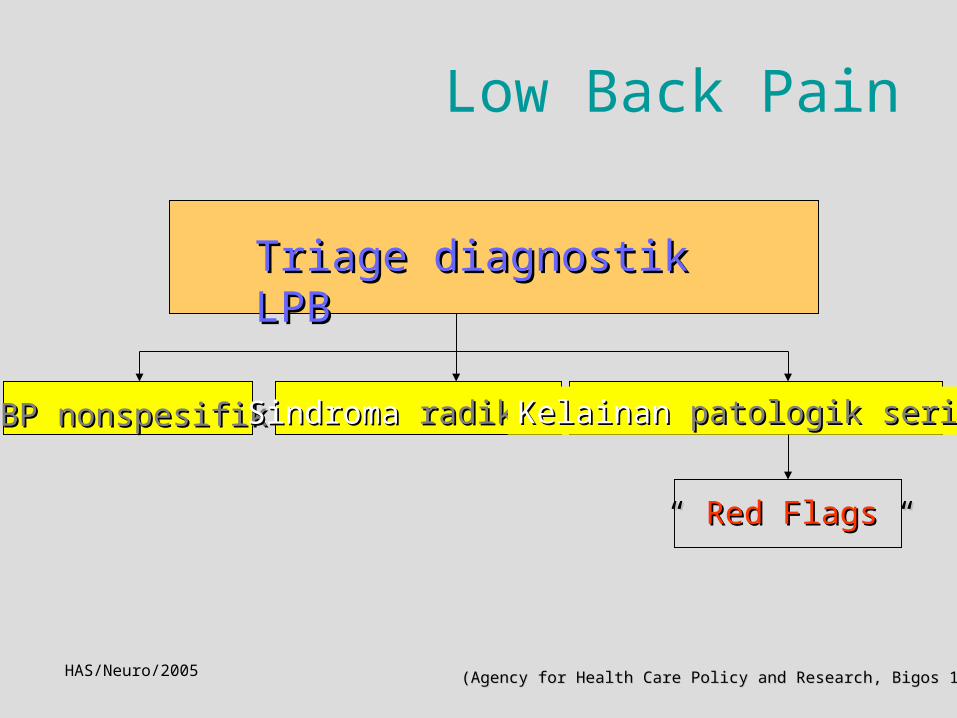
Low Back Pain
Triage diagnostik LPBTriage diagnostik LPB
LBP nonspesifikLBP nonspesifik SindromaSindroma radikulerradikuler KelainanKelainan patologik seriuspatologik serius
“ “ Red FlagsRed Flags “ “
(Agency for Health Care Policy and Research, Bigos 1994)(Agency for Health Care Policy and Research, Bigos 1994)HAS/Neuro/2005

Low Back pain
• Seriuos pathology: neoplasm
infection
fracture
cauda equina syndrome
• Ischialgia, radicular syndrome
• Nonspecific LBP

Syndromes of Epiconus, Conus and Cauda EquinaSyndrome of lumbal-radiculopathy


Low Back Pain
• Diagnostic triage• History taking and physical examination to
exclude red flags• Neurological examination (including
Lassegue test)• Consider psychosocial factors if there is no
improvement• X-rays, MRI ??

Red Flags of LBP
• Cancer
• Infection
• Vertebral fractur
• Cauda equina syndrome or
Severe neurological deficit

Yellow Flags
• Recognition of psychosocial factors
as predictors of chronicity and
obstacles to recovery
Acute subacute chronic

Risk Factors of LBP
• Physical : 35 – 55 y past history of LBP
• Occupational : vibration bending, twisting heavy lifting low job satisfaction
• Psychosocial : attitudes cognition fear-avoidance beliefs depression anxiety distress and related emotion
Management of acute LBP
• Diagnostic classification, D/ triage
• Reassurance
• Early and progressive activation
• Analgetics ?: acetaminophen
NSAID
consider muscle relaxants
• Recognition yellow flags

HAS/P3D
Management of Chronic LBP
• Behavioral therapy
• Education
• Intensive exercise therapy
Multidisciplinary

HEADACHE
HAS/P3D

ALL ACHES AND PAINS LOCATED IN THE HEAD
ORBITA OCCIPUT
HEADACHEDEFINITION :
HAS/P3D

The International Classification of Headache Disorders ICHD 2 ( IHS 2004 )
The Primary Headaches Migraine Tension-type headache (TTH) Cluster headache Other primary headaches
The Secondary Headaches Headache attributed to head and/or neck trauma Headache attributed to cranial or cervical vascular disorders Headache attributed to non-vascular intracranial disorders Headache attributed to a substance or its withdrawal Headache attributed to infection Headache attributed to disorder of homoeostasis Headache or facial pain attributed disorder of cranial, neck, eyes, ears, nose, sinuses, teeth, mouth or other facial or cranial structures Headache attributed to psychiatric disorders
Cranial Neuralgias, central & primary facial pain & other headaches Cranial neuralgias & central causes of facial pain Others headache, cranial neuralgias & central or primary facial pain

The International Classification of Headache Disorders ICHD 2 ( IHS 2004 )
The Primary Headaches Migraine Tension-type headache (TTH) Cluster headache Other primary headaches
The Secondary Headaches Headache attributed to head and/or neck trauma Headache attributed to cranial or cervical vascular disorders Headache attributed to non-vascular intracranial disorders Headache attributed to a substance or its withdrawal Headache attributed to infection Headache attributed to disorder of homoeostasis Headache or facial pain attributed disorder of cranial, neck, eyes, ears, nose, sinuses, teeth, mouth or other facial or cranial structures Headache attributed to psychiatric disorders
Cranial Neuralgias, central & primary facial pain & other headaches Cranial neuralgias & central causes of facial pain Others headache, cranial neuralgias & central or primary facial pain

PAIN SENSITIVE CRANIAL STRUCTURES
• Skin,subcutan., muscle• Extracranial arteries• Skull periosteum• Eye,ear, nasal cavities,
sinuses• Intracran.venous sinuses,
large vein, pericavernous structures
• Basis dura, meningeal arteries, prox.ant/middle cerebral A, IC int.carotis A
• Superf.temporal A• Cranial nerves:II.III,V,IX,X,C1-
3


THE ROLE OF NEUROTRANSMITTER :THE ROLE OF NEUROTRANSMITTER : SEROTONIN (5 HT) SEROTONIN (5 HT) THE ENDOGENOUS PAIN CONTROL MECHANISM -> OPIOIDTHE ENDOGENOUS PAIN CONTROL MECHANISM -> OPIOID GABAGABA
MECHANISMS OF CRANIAL PAIN :
TRACTION ON OR DILATATION OF THE INTRACRANIAL
ARTERIES
DISTENTION OF EXTRACRANIAL ARTERIES
TRACTION ON OR DISPLACEMENT OF THE LARGE
INTRACRANIAL VEINS OR DURAL ENVELOPE
COMPRESSION, TRACTION OR INFLAMATION OF THE
CRANIAL AND SPINAL NERVES
SPASM, INFLAMATION & TRAUMA TO CRANIAL & CERVICAL
MUSCLE

MECHANISM OF CRANIAL PAIN (con’d)
DISEASE OF THE TISSUES OF THE SCALP, FACE, EYE,
NOSE, EAR AND NECK
MENINGEAL IRRITATION
INTRACRANIAL MASS LESION
RAISED INTRACRANIAL PRESSURE
LOWERED INTRACRANIAL PRESSURE : LP HEADACHE

ATTACK ONSET QUALITY SEVERITY LOCATION MODE OF ONSET TIME, INTENSITY, CURVE, DURATION CONDITION WHICH EXACERBATE / RELIEVE THE PAIN ASSOCIATED FEATURES SOCIAL HISTORY, FAMILY HISTORY PAST HEADACHE HISTORY HEADACHE IMPACT
HISTORY taking:

HAS/NEURO

Faktor pencetus Nyeri Kepala
StresKurang/kebanyakan tidurTidak/telat makanBau menyengat : parfum,rokokLingkungan: cahaya silau/berkedip,gaduh ketinggian,panas,lembab ruang berasapMakanan/minuman
HAS/Neuro/Bdg/04

RED FLAGS of HEADACHE


Secondary Headache Red Flags “SSNOOP”
• Systemic symtoms (fever, weight loss) or• Secondary risk factors : underlying diseases
(HIV,systemic cancer)• Neurologic symtoms or abnormal signs (confusion,
impaired alertness,or consciousness)• Onset: sudden,abrupt, or split-second (first,worst)• Older: new onset and progressive headache, especially
in middle age>50 (giant cell arteritis)• Previous headache history or headache progression:
pattern change, first headache or different
(change in attack frequency, severity, or clinical pictures)


HAS/P3D

HAS/P3D

CLUSTER HEADACHE
YOUNG ADULT MEN ( M : F = 5 : 1 ) UNILATERAL PAIN
HAS/NEURO

Tension Type Headache
• Psychologic factors• Muscle contraction and myofacial tenderness• Vascular factorsn : NO• Humoral factors : 5HT• Central factors : central pain control system

HAS/P3D

PHYSICAL EXAMINATION
NEUROLOGICAL EXAMINATION


HAS/P3D
Trigeminal neuralgia

HEADACHE TREATMENT
• PRIMARY HEADACHE TREATMENT
Abortive
Preventive
• SECONDARY HEADACHE
TREATMENT
Causal Symtomatic : Analgesic

PRIMARY HEADACHE TREATMENT
TTHAbortive :Simple analg : acetaminophen/
ASA/NSAID
Preventive : Amitriptylin
Nonpharmacologic therapy
MIGRAINEAbortive :Simple analg : acetaminophen/
ASA/ NSAIDSpecific analg : ergot alkaloids ( ergotamine/ DHE )/ triptanAntiemetics : metoclopramide/
domperidone
Preventive : Anticonvulsants / Adrenoceptor blockers (propranolol)/ Antidepressants/ Ca-channel blockers
Nonpharmacologic therapy

CLUSTER HA
abortive : – o2 inhalation– ergot alkaloids, – triptans
preventive : – verapamil– ergot alkaloid
Cranial Neuralgias,Central Pain
(Neuropathic Pain) Treatment • Antidepressants• Anticonvulsants• Antiarrhitmic• Local anesthetic

Penanganan tanpa obat
EdukasiMengenal & menghindari faktor pencetus
Modifikasi perilakuLatihanRelaksasiBiofeedbackTerapi perilaku kognisiTerapi fisik
TENS (transcutaneus electric nerves stimulation)
HAS/Neuro/Bdg/04
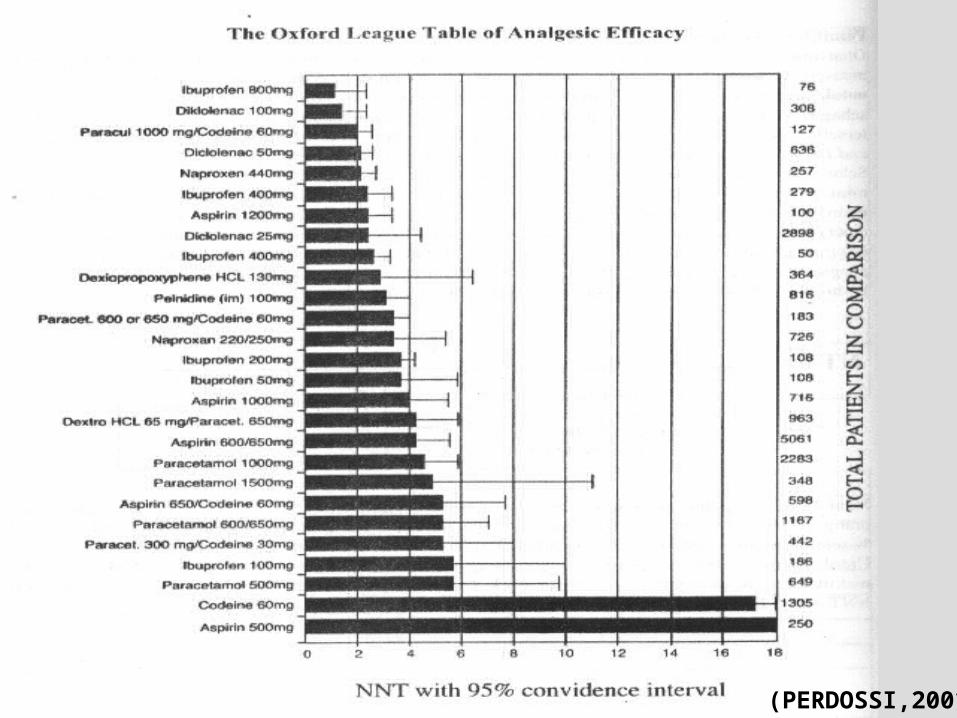
(PERDOSSI,2001)

HAS/Neuro/2004

(Rowbotham MC, Petersen KL, 2001)
Antikonvulsants

(PERDOSSI,2001)HAS/Neuro/RSHS-FKUP
(I.C.H.E.)
MononeuropahiesMononeuropahies








