
KAROLINSKA
INSTITUTET
Perioperativ Metabolism och Nutrition
Jonas Nygren, Kliniken för Kirurgi och Anestesi, Ersta Sjukhus
SwERAS-dagarna,
Stockholm, 21-22 November, 2019
Disclosures
None


The response to major surgery leads to morbidity
Metabolic homeostasis Inflammation, insulin resistance, catabolism
Fluid balance Hypoperfusion, overhydration, oedemia
Pain Somatic, visceral, neuropathic
Gut dysfunction Nausea, vomiting, paralysis
Cognitive dysfunction Delirium, confusion, sleep disruption
Post-operative deconditioning Immobilisation, fatigue, anemia, starvation It´s more to it than a perfect operation

Metabolic response to trauma
Neuroendocrine response
Cortisol, catecholamines, glucagon, GH
Insulin resistance
Catabolism
Lipolysis
Protein breakdown
Hyperglycemia
Inflammation
Cytokines
The Surgical Stress Response
Salt and water retention
Increased CO and O2 consumption
Mobilisation of energy reserves
Catabolism
Insulin resistance
Hyperglycemia
Surgical patients with low reserves are vulnerable
Malnutrition
Frailty
Sarcopenia

Gillis C, Anesthesiology, 2015

Mitochondrial
dysfunction
Energy production / oxidative phosphorylation / ATP
Decrerased fatty acid oxidation
Inhibiting insulin action / Insulin resistance
Toxic lipid metabolite accumulation
ROS production / oxidative stress
Uncoupling

Gonzalez-Franquesa A, Adv Exp Med Biol, 2017
Harmful positive feedback loop

Gonzalez-Franquesa A, Adv Exp Med Biol, 2017
Mitochondrial dysfunction and insulin resistance

Preoperative insulin resistance
increased risk for complications
The ORs were adjusted for potential confounders
Complication OR for every decrease by
1 mg/kg/min
(Insulin sensitivity)
P
value
Death 2.33 (0.94-5.78) 0.067
Major complication 2.23 (1.30-3.85) 0.004
Severe infection 4.98 (1.48-16.8) 0.010
Minor infection 1.97 (1.27-3.06) 0.003
Sato et al, JCEM 2010; 95: 4338-44
273 patients open cardiac surgery, insulin sensitivity determined at the end of op

Controlling perioperative physiologyMany small pieces of the puzzle

Gillis C
, Anesth
esiolo
gy, 2
015

ERAS
Regional
analgesia
Prevention
of ileus/
prokinetics
CHO -loading/
no fasting
Early
mobilisation
Periop fluid
management
DVT
prophylaxis
Preopcouncelling
Avoiding opioids
No premedication
No oral bowel prep
Perioperative
Nutrition
Active warming
Oral analgesics/
NSAID’s
Incisions
No NG tubes
Early removal
of catheters/drains

LOS
Compl
Lap CRC surgery
ERAS vs Trad
Meta-analysis
13 RCT, n=1298
• Shorter LOS
• Reduced
complications
• Faster return
• bowel function
• Less SIRS• CRP
• IL6
Ni X, J Gastrointest Surg, 2019

*
*
*
*
*
ERAS
Lap Colonic resection
• n=48
• 2 Complications
• 1 Readmission
Patel G, Am J Surg, 2010, Levy BF, Dis Col Rect, 2009

Gillis C
, Anesth
esiolo
gy, 2
01
5*
*
*
*

Summary
Major surgery
significant morbidity and surgical stress
ERAS are evidence based perioperative protocols
reduces surgical stress
improves postoperative outcome

ERAS
Epidural
Anaesthesia
Prevention
of ileus/
prokinetics
CHO - loading/
no fasting
Early
mobilisation
Peri-op fluid
management
DVT
prophylaxis
Pre-op councelling
Remifentanyl
No - premed
No bowel prep
Perioperative
Nutrition
Bairhugger
Oral analgesics/
NSAID’s
Incisions
No NG tubes
Early removal
of catheters/drains

Malnutrition
Nearly 50% of patients admitted to hospital
Increased mortality and morbidity
Longer hospital stay and increased costs
Meta analysis 15 RCTs n= 3831, 2015
Cochrane review, GI surgery, 13 RCTs, n= 548, 2012
Obstruction
Malabsorbtion
Drug / Treatment related side effects
Metabolic abnormalities
Patient related factors
After surgery Organisational barriers in hospital
Missed meals etc

Pre‐operative nutrition and the elective surgical patient: why, how and what?
Anaesthesia, Volume: 74, Issue: S1, Pages: 27-35, First published: 02 January 2019, DOI: (10.1111/anae.14506)

ERAS Guidelines / Nutrition
ColoRectal surgery Patients should be screened for nutritional status
If deemed to be at risk of under-nutrition, they should be given active nutritional support.
Preoperative fasting should be minimised.
Patients should be encouraged to take normal food as soon as possible after surgery.
ONS can be used to supplement total intake.
Gustafsson, ClinNutr, 2012

Preoperative optimisationPrepare before surgical stress
Cardiopulmonary function
Anemia
Glucose / Diabetes control (HbA1C < 7.5)
Smoking cessation
Alcohol abstinence
Physical function / exercise
Nutritional state
Weight loss
Morbid obesity
Electrolytes / Trace elements
Fluid homeostasis / Dehydration
PR
EH
AB
ILIT
AT
ION

Preoperative weight lossAdverse postoperative outcome
Studley, JAMA, 1936, Meguid, Am J Surg, 1988
Weight loss Mortality
<20% 3.5 %
>20% 33 %

Current practice
132 patients in Manchester, UK
resectable CRC, 2-4 weeks preoperatively
50 % weight losing
20% malnourished
173 departments in Swiss and Austria
80% aware of reduced complications / reduced LOS
Only 20 % had nutritional screening
Only 14% used a nutrition score
Grass et al, Eur J Clin Nutr. 2011, Burden, J HND, 2010

Detect and Correct to Protect
Screening
Assessment
Nutrition care plan
Preoperatively
Avoid preoperative fasting
Postoperatively
After discharge
In malignant disease, interventions need to be initiated immediately at outpatient clinic

Nutritional screening
SGA Medical-surgical hospitalized and outpatients
NRS-2002 Medical-surgical and acute hospitalized
MNA-SF Ambulatory and subacute
MST Acute hospitalized and oncology outpatients
MUST Medical and surgical hospitalized
NST/BAPEN Acute hospitalized
Simple, 2-part Acute hospitalized
NRS Acute care, medical and surgical
Screen-II/AB Seniors in the community/geriatric clinics
Rapid screen Subacute care (rehabilitation center)
Tool #1 Elderly in acute care and long-term care
SNAQ V Not evaluated against a reliable standard
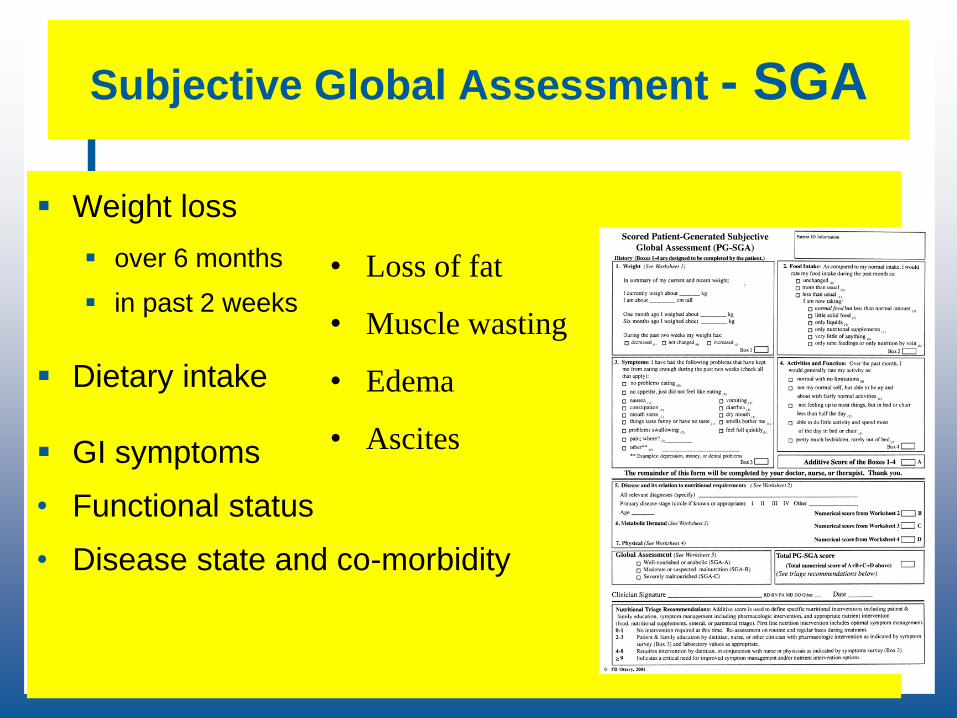
Subjective Global Assessment - SGA
Weight loss
over 6 months
in past 2 weeks
Dietary intake
GI symptoms
• Functional status
• Disease state and co-morbidity
• Loss of fat
• Muscle wasting
• Edema
• Ascites

Signs of malnutrition
Loss of muscle
Loss of fat
Nails
Hair
Mouth
Teeth
Edema
Ascites
Loss of function
Lethargy (Depression)

Muscle wasting in obese may be difficult to determine

Nutritional assessment
History Diet and weight loss
Physical examination BMI
Tissue stores of muscle and fat
Mid arm circumference and triceps skin fold
Grip strength and FEV
BIA and DEXA and indirect calorimetry
CT scan
Lab Albumin and pre-albumin
Transferrin and retinol-binding protein
Postoperatively these proteins are markers for surgical stress

Preoperative assessment
Current nutritional status
Starvation (anorexia, stricture)
Chronic disease
Acute disease
Severity of the surgical insult
Procedures with high infection rates and long hospital
stay

Malnutrition using SGA screening
and postoperative outcome
Baker NEJM, 1982, Machija, NCP 2008
0
10
20
30
40
50
60
70
80
Infections (%) LOS (days)
SGA A
SGA B
SGA C
P<0.005 (infections)
P<0.0001 (LOS)
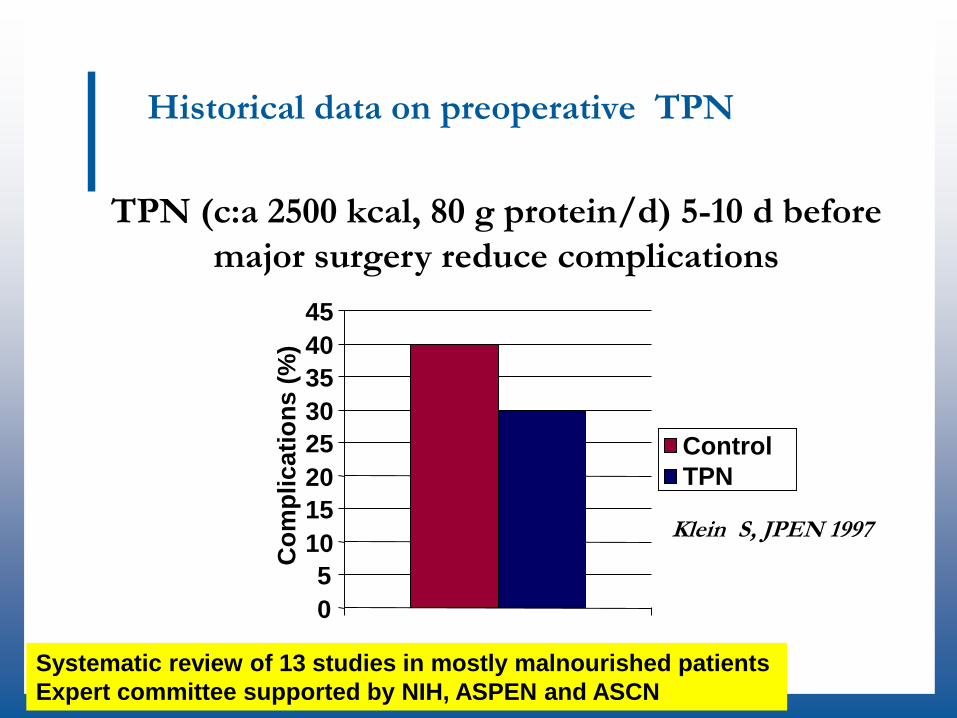
Historical data on preoperative TPN
TPN (c:a 2500 kcal, 80 g protein/d) 5-10 d before
major surgery reduce complications
Klein S, JPEN 1997
0
5
10
15
20
25
30
35
40
45C
om
pli
cati
on
s (
%)
Control
TPN
Systematic review of 13 studies in mostly malnourished patients
Expert committee supported by NIH, ASPEN and ASCN

Nutrition before GI surgery
Immune-enhancing nutrition before GI surgery (7 RCT. N=548) Mostly well-nourished patients
5-7 days before surgery
Additional Arginine, Omega 3, (RNA), (Glutamin)
Reduced total complications
Reduced infectious complications
Reduced hospital stay
Preoperative PN (3 RCT)
Mostly malnourished
10 days before surgery
Reduced major complications
No difference in infectious complications
Oral (3 RCT) or Enteral(2 RTC) standard nutrition
vs no nutrition
No effect on outcomes
Preoperative nutrition
Need to be evaluated in conjunction with ERAS protocols
Burd
en. C
och
rane
revi
ew, 2012

ERAS / ESSO guidelines
Position paper
Nice short review
Sandrucci S, EJSO, 2018

Nutritional support
RCT, CRS, n=101
Weight losing patients > 1kg /6 months
250 ml ONS for 8 (5-15) days preop
vs dietary advice alone
Less weight loss postop (7 vs 10 %)
Fewer infections (30 vs 47%)
Burden S, J Cach Sarc Muscle, 2017
*

ImmunonutritionNutrients, which influence immunity
Omega-3 polyunsaturated fatty acids
Inhibits inflammation, enhances T cell functions
Changes in membrane phospholipids
Changes in cytokine and lipid-derived mediator production
Arginine
Enhances T cell function
Stimulation of growth hormone production
Altered nitric oxide production?
Glutamine
Stimulates T cell function, inhibits inflammation?
Stimulation of glutethione synthesis?
Enhances cell proliferation, increases
Sulphur amino acids and related compounds
Inhibits inflammation enhances T cell function
Suppression of oxidant effects and NFkB activation
Maintenance of glutathione status

Fig. 1
European e-Journal of Clinical Nutrition and Metabolism 2009 4, e10-e13DOI: (10.1016/j.eclnm.2008.07.015)
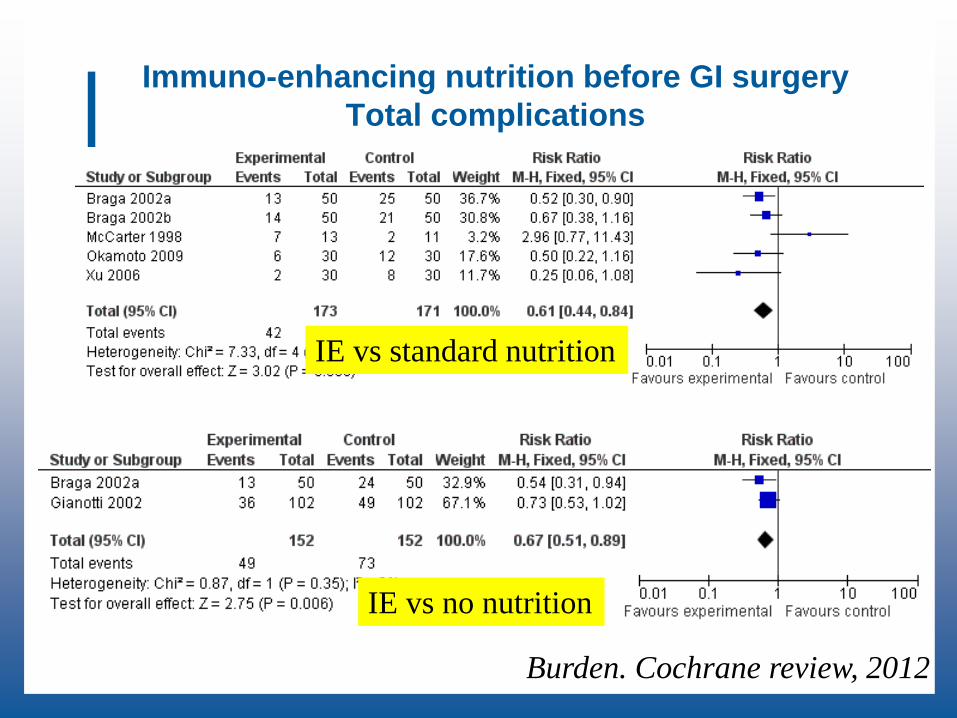
Immuno-enhancing nutrition before GI surgery
Total complications
IE vs no nutrition
Burden. Cochrane review, 2012
IE vs standard nutrition
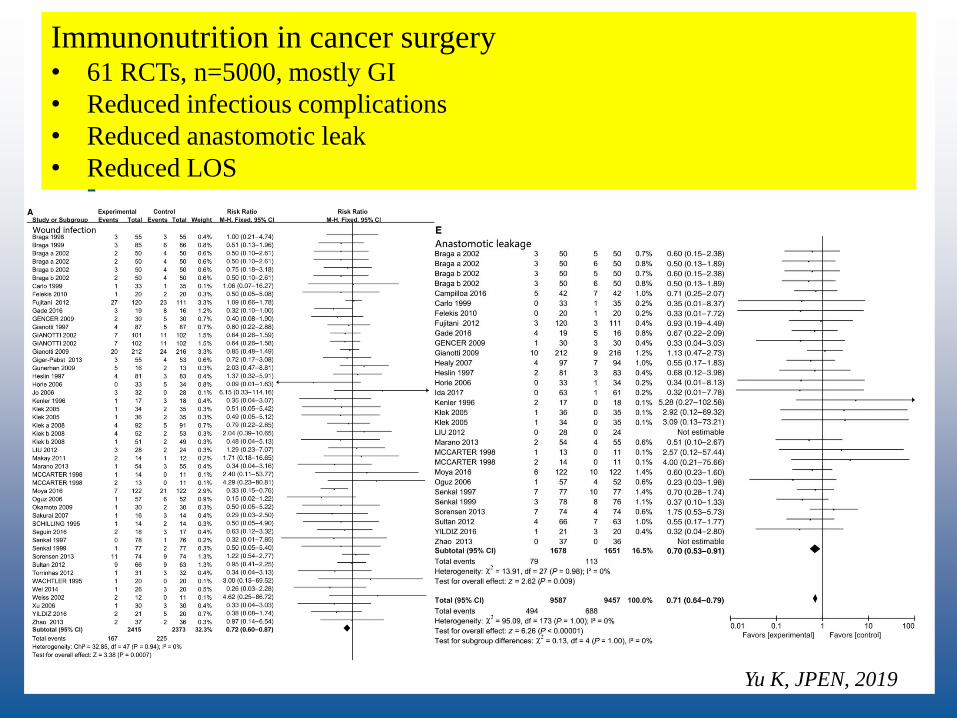
Immunonutrition in cancer surgery• 61 RCTs, n=5000, mostly GI
• Reduced infectious complications
• Reduced anastomotic leak
• Reduced LOS
Yu K, JPEN, 2019

Criticism Immunonutrition literature
Recent meta analysis in BJS (83 RCTs, n=7116) Overall
Reduced total (OR 0,79) and infectious complications (OR 0,58)
Reduced Shorter LOS (-1,79 days)
Little evidence from studies in
Minimally invasive surgery
ERAS
Bias
Reporting bias
Publication bias
Industry bias
When studies with high or unclear risk of
bias was excluded;
evidence was substantially lowered Probst P, BJS, 2017

Immunonutrition in ERAS
264 pat undergoing colorectal resection in ERAS
Randomised to Immunonutrition 400 ml
7 days before and 5 days after surgery
Standard nutrition 400 ml
In addition to normal food ad lib
Reduced Total complications (35 vs 23%)
Infections complications (24 vs 11%)
Wound infections (16 vs 6 %)
Moya P, Medicine, 2016

Preoperative Nutrition Recommendations
•Screen all patients undergoing major GI surgery
•If malnourished (SGA B och C)
•Provide oral supplements
•In case of a stricturing process or GI tolerance
•ONS covering energy and protein requirements
•Sometimes residue low diet, if possible
•Consider parenteral nutrition
•Tailored nutrition depending on GI tolerance
Summary
Preoperative Nutrition
Malnutrition is related to adverse outcome
Current practice rarely include
Nutritional screening
Nutritional intervention
Even brief nutritional intervention improve outcomes
All malnourished patients before any procedure
Consider all patients before major surgery (IE)

Summary Nutritional support
Nutritional supplements
More energy
More protein
1.2-2 g/ kg/ 24h in surgical patients
Immunonutrition
Vitamin D
Omega 3 FFA
Exercise
Improves anabolic effect from feeding
20 g protein maximally stimulates protein synthesis
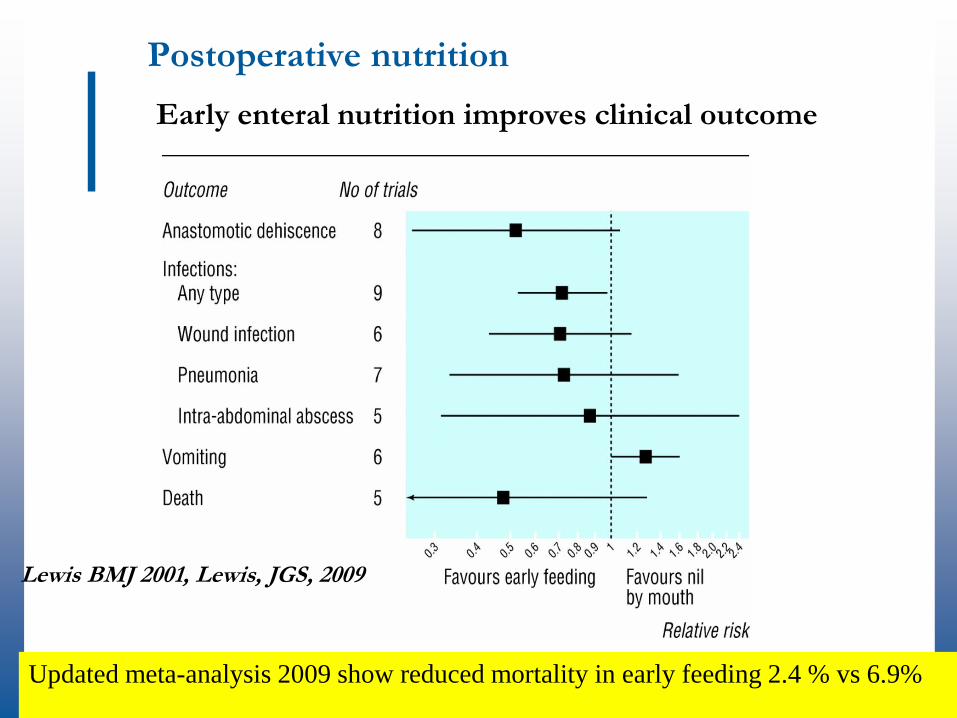
Postoperative nutrition
Early enteral nutrition improves clinical outcome
Lewis BMJ 2001, Lewis, JGS, 2009
Updated meta-analysis 2009 show reduced mortality in early feeding 2.4 % vs 6.9%

Oral energy intake after major open
colorectal surgery in ERASNot a big problem
0
500
1000
1500
2000
0 1 2 3 4 5 6 7
Postop days
Kc
al /
24
h
N=143
Data from Ersta Hospital

Oral supplements in addition to a normal diet
Henriksen Nutrition 2002
Postoperative nutrition
1340 Kcal
in a 70 kg person

Fascilitate nutrition
Avoid fasting Preoperative carbohydrate loading
Enhance nutritient utilization Epidural analgesia
Optimize fluid dynamics
Control PONV Multimodal analgesia
Fascilitate mobilization

Chewing gum
Coffee
Prokinetics (Prucalopride)
Early NG in case of gastric retention !!
Stoma tubing
Avoid aspirationGianotti L, Clin Nutr, 2019
Day of surgery Free oral intake
≥600 kcal ONS /24h
Postoperatively ≥900 kcal ONS / 24h
Post discharge ONS if inadequate food intake or preoperative malnutrition
Postoperative Nutrition Recommendations

Parenteral nutrition:
Well fed INFECTIONS
Malnutrition Mortality
Postoperative nutrition
Braunschweig Am J Clin Nutr 2001
Parenteral Nutrition in reduced GI tolerance
ALWAYS TRY ORAL or ENTERAL ROUTE FIRST !
SGA A PN after 5 days with a low energy intake
(<800 kcal/24h)
SGA B-C PN after 2 days with a low energy intake
(<800 kcal/24h)
Postoperative Nutrition Recommendation

Infectious complications
Fish oil based postoperative PN, 21 RCTs
Li, Clin Nutr, 2014
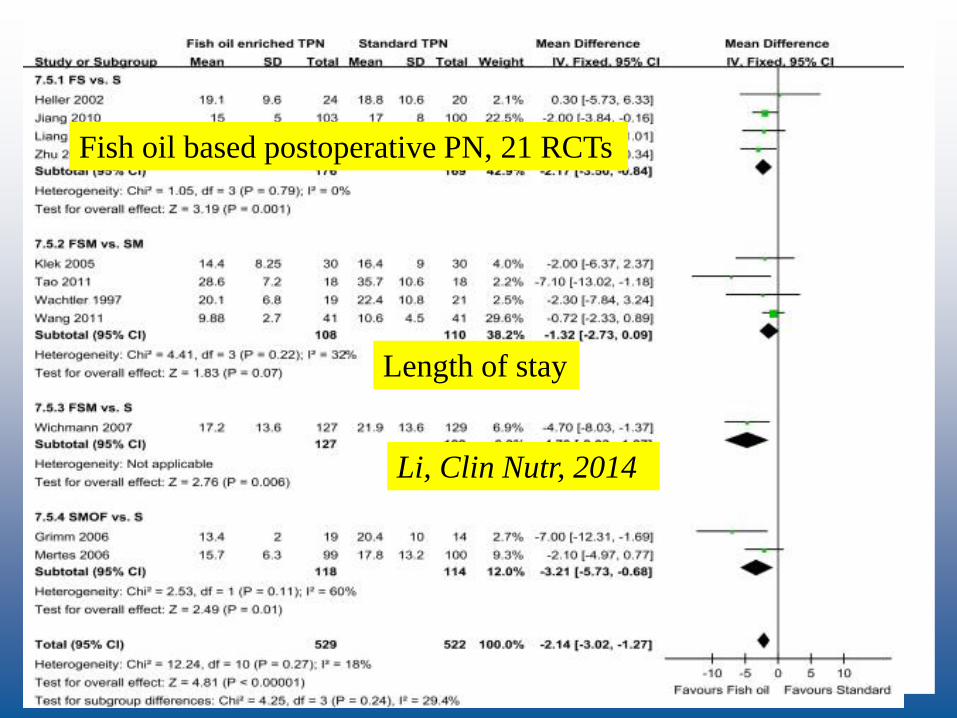
Length of stay
Fish oil based postoperative PN, 21 RCTs
Li, Clin Nutr, 2014

Post-discharge nutrition
No evidence for improved clinical outcome
1-4 months treatment with ONS
4 RCTs
Lack of robust data
Lidder, NCP, 2009

Conclusion
Nutritional screening
Nutritional intervention In malnutrition, 7-14 days of preoperative nutrition
Consider Immune-enhancing nutrition for 5-7 days
before major surgery
Postoperative multimodal ERAS interventions Early oral feeding
Enhancing GI recovery
Consider ONS or Immune-enhancing nutrition
Studies on nutritional interventions in ERAS surgery is needed
KAROLINSKA
INSTITUTET

KAROLINSKA
INSTITUTETIt´s more to it than a perfect operation

ONS preoperatively
RCT, CRS, n=125
400 ml ONS >10 days
Including well-nourished pats No effect
RCT, CRS, n=179 ONS ad lib, mean 15 days (7-61)
Including well-nourished pats
Less weight loss, less minor complications
RCT, CRS, n=101
Weight losing patients > 1kg /6 months
250 ml ONS for 8 (5-15) days preop
vs dietary advice alone
Less weight loss postop (7 vs 10 %)
Fewer infections (30 vs 47%)
Burden S, J Cach Sarc Muscle, 2017, Burden S, J Hum Nutr Diet 2011, Smedley, BJS, 2004
*

Gillis C, Anesthesiology, 2015

Permissive underfeeding ?
Meta analysis on 12 studies (8 RCT)
Short term nutritional support
>50% but less than 100 % of energy requirements
Improved outcomes
Reduced morbidity
From short term underfeeding
However, poor study design and heterogeneity common
Owais, APT, 2010

LAFA trial, n=79Veenhof A, Ann Surg, 2012
LS Lap Standard
LFT Lap FT
OS Open Standard
OFT Open FT
HLA-DR
CRP IL6

Refeeding syndromecan be fatal
Hypophosphatemia
Hypokalemia
Hypomagnesemia
Volume overload
Cardiopulmonary
Neurologic
Hematologic
Increased BMR
ATP depletion
Provide only 50-70% of energy intake normally required first 3-5 days in severe cases
Monitor electrolytes
Tiamin. vitamins
Pro-kinetics and PPI to support enteral/oral route

Gillis C, Anesthesiology, 2015







