
Pose de pace maker et défibrillateurschez le patient IRC ou dialysé :
le point de vue du rythmologue
Pascal Defaye
CHU Grenoble-Alpes

Total 2012 = 493,573 PMs implanted70,000 in France
Total 2012 = 84,716 ICDs implanted20,000 in France
« Europe » = 893 M inhabitants
Arribas F et al., Europace 2014,16:i1-i78

Nephrol Dial Transplant 2016 31: 2115–2122
3X greater hazard PM implantation in dialysis patient/ control patients
10% of the population : PM/ICD
Risk of infections +++
Risk of thrombosis+++

Goldenberg et al. JACC 2008
Peu de bénéfice de la prévention I : DAI chez IRC/dialysé
Williams EH et al. Symptomatic deep venous thrombosis of the armassociated with permanent transvenous pacing electrodes. Chest. 1978;73(5):613-5.
- Subclavian vein thrombosis and symptoms are rare
212 pacemakers implanted between 1970 and 1978
Symptoms of subclavian vein thrombosis very rare : 2%
Subclavian re-canalization for Pace-Maker and ICD Implantation

Subclavian re-canalizationfor Pace-Maker and ICD Implantation
J Interv Card Electrophysiol 2010; 29:199–202
86 patients : veinography 19±16 months after CRT-P implantation
Subclavian vein was patent in 61% of all participants. 33 patients with subclavian obstruction : 39%
- mild obstruction : 8- severe obstruction : 15- total occlusion : 10
Correlates of venous obstruction on linearregression analysis
Atrial fibrillation after CRT-P and ICD implantation was significantly related with total occlusion(r=0.3, p=0.005 and r=0.24, p=0.003).

THROMBOSIS or VENOUS STENOSIS
Heart Rhythm 2009

Mr G… 73 y.o. Superior vena cava syndrome
Single chamber ICD 2005 (primary prevention/post MI - LV EF 30%) 2011: box change + upgrading to a dual chamber ICD 2012 :Severe SVC syndrome: Balloon venoplasty of the SVC (no stenting) transient
improvement 2014 : Referred for superior vena cava syndrome recurrence

OcclusionInnominate vein
Collaterals Collaterals
Azygous vein dilation
SVC stenosis

How to reimplant?
Subcutaneous-ICD

Mr R …Gilles , born in 1961, End of Stage Renal failure, DDD-PM 5 years before : left side• Right arteriovenous fistula thrombosis• Left arteriovenous fistula associated to arm oedema +trophic disorders
Necessity of femoral dialysis
Subclavian thrombosis Inominate vein thrombosis Femoral extraction
Extraction Right reimplantationLeft subclavian +inominate vein stenting
Stenting
1 year post procedure : complete resolution of the oedema + trophic disordersWith fonctionnal left dialysis fistula

Failure to cross with Laser(calcifications)

Success with Tightrail®
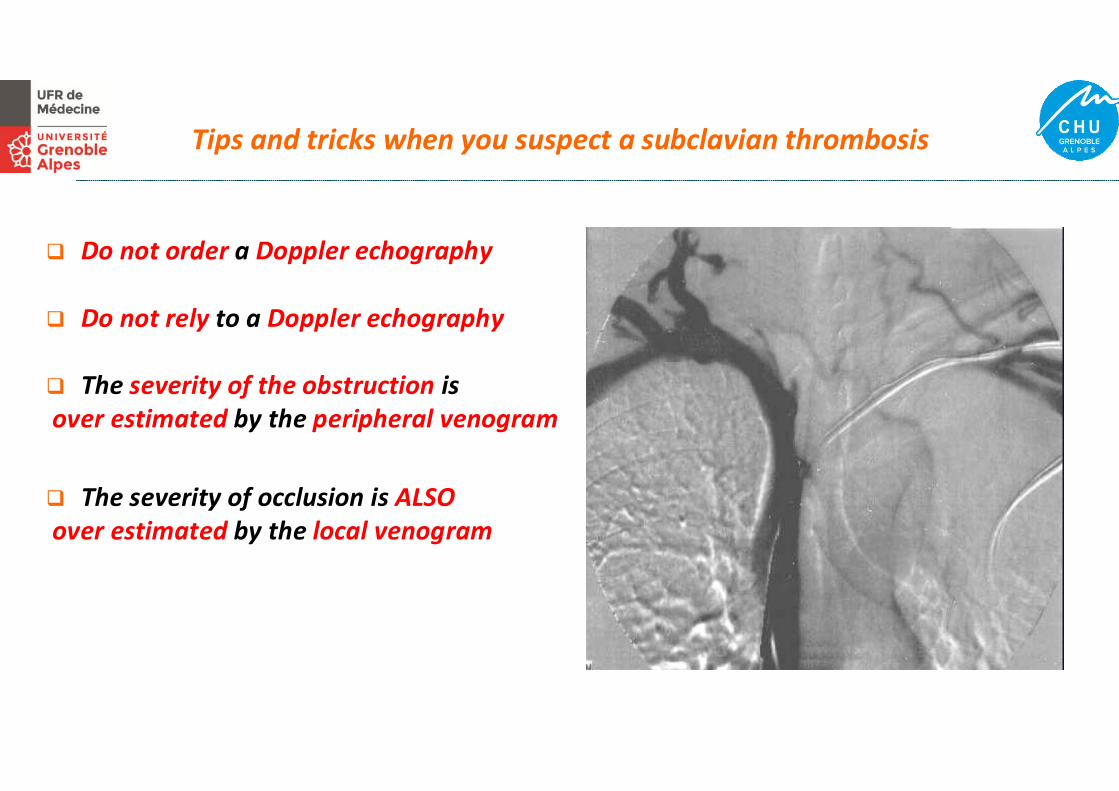
Do not order a Doppler echography
Do not rely to a Doppler echography
The severity of the obstruction is over estimated by the peripheral venogram
The severity of occlusion is ALSOover estimated by the local venogram
Tips and tricks when you suspect a subclavian thrombosis

Heart Rhythm 2017;14:839–845

Heart Rhythm 2017;14:839–845

Leadless pacemakersLCP™ Nanostim/SJM Micra™ Medtronic
December 2012 December 2013

N Engl J Med September 2015
Leadless II
526 patients Efficacy 90%Safety 93.3%
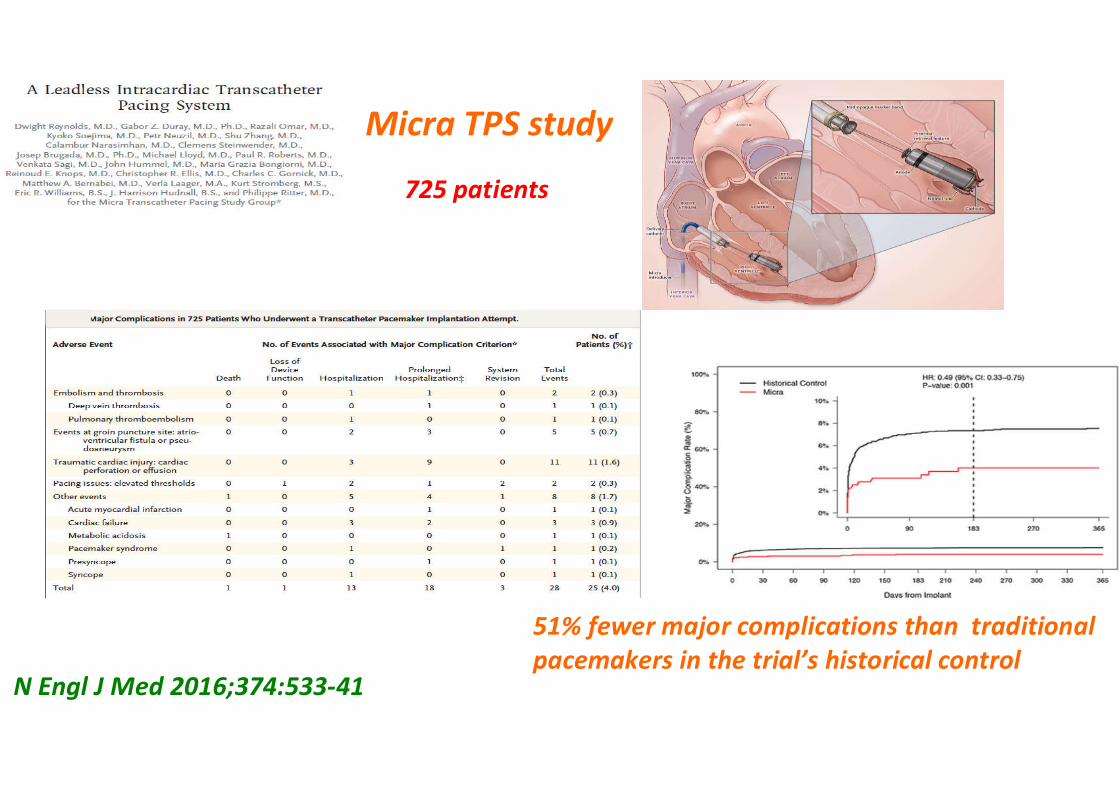
N Engl J Med 2016;374:533-41
725 patients
Micra TPS study
51% fewer major complications than traditional pacemakers in the trial’s historical control





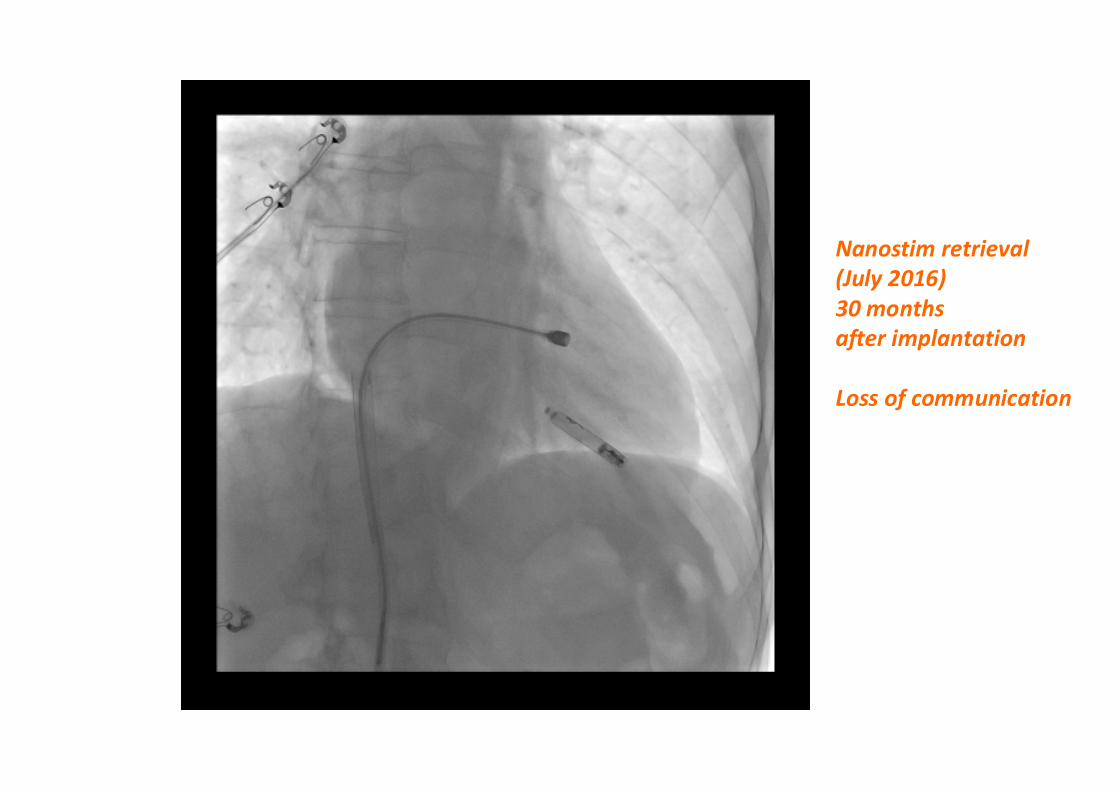
Nanostim retrieval(July 2016)30 months after implantation
Loss of communication

Subcutaneous ICDSensing Electrodes Distal (D) and Proximal (P)
Parasternal Coil of 8 cm (C)
•Totally sub- cutaneous : • No electrode« in or on » the heart
• No need of fluoroscopy

3 differents vectors for sensing : primary (yellow),secondary (red) and alternative vector (blue)

DAI sous cutané

Électrodes ECG•sèches et non adhésives•4 électrodes pour 2 dérivations
Électrodes de défibrillation à application
automatique de gel
Boutons de réponse
Moniteur•150 joules biphasique•Enregistre l’ECG, le temps de port de la veste, etc.
Electrodes sêches Pour le confort du pt

J + 15
TYRX antibacterial envelope

Pose de pace maker et défibrillateurs chez le patient IRC ou dialysé : le point de vue du rythmologue
Conséquences importantes de l’association PM/DAI et IRC ou dialyseRisque de sténose/thrombose homolatérale : 30% des patients
Attention à l’association entre PM/DAI endocavitaire et Catheters central tunnelisés
Préférer les accès permanents pour dialyse : fistule AV, dialyse péritonéale
Rationnel de la prévention I notamment avec le DAI mérite discussion : pas de bénéfice clinique
Quand nécessité impérieuse de PM : préférer Leadless PM +++
Quand nécessité de DAI préférer : S-ICD ++++







