
Predicting & Preventing Postoperative Pulmonary Complication
Wael A BatobaraFRCPC Internal Med ,Pulmonary & Critical care
medicineABIM Internal Med ,Pulmonary & Critical care medicine

Case Scenarios
A. 65y male septoplasty Asthma
B. 45y female Lung resection COPD
C. 55y male Lap chole Pulmonary fibrosis
D. 50y male CABG heavy smoker

By the end of the talk
• Incidence & importance of postoperative pulmonary complication PPC
• Risk factors Patient Vs procedure related
• Prediction tools & their efficiency
• Available guidelines
• Preventive measures

Incidence & Importance
• As common as postoperative cardiac complication
• Variable reported incidence
Definitions of PPC have varied widely
+ differences in the selection of patients Lawrence VA, J Gen Intern Med 1995

Incidence & Importance
• Recently only complications that either prolongs the hospital stay or to contribute to morbidity and mortality were reported.
I - Pneumonia
II- Underlying chronic lung disease exacerbation
III- Respiratory failure with prolonged
Mechanical Ventilation

Disease Severity Predicting Mortality in CABG
Fuster et al Euro Jr Cardiothorac 2006

Patient related risk factors
Age• Studies suggesting an increased risk of PPC
with older age have not generally controlled for coexisting conditions.
• When data were stratified according to the ASAoverall perioperative mortality for classes II through V is the same in all age groups.
JAMA 1979; Anesthesiology 1973

Patient related risk factors
Obesity • Potential Difficult airway
• Restrictive disease which is accentuated postoperatively
• Obstructive sleep apnea & associated Pulmonary HTN
• Obesity hypoventilation
• Few review article didn’t find that obesity is associated with increased risk of PPC in abdominal Sx or lap chole
Smetana, Chest 1999 Phillips,AJRCC 1994
Patient related risk factors
Smoking
• Prospective study
489 ambulatory pt elective sx
Smoker had a higher incidence of
wound infections odds ratio 1.71
respiratory complications odds ratio 16.3
Myles Anesthesiology. 2002 Oct

Patient related risk factors
Quitting smoking Randomized prospective trial 120 pts
Counseling & nicotine replacement 6-8 weeks before Sx
Smoker Quitter
All complications 52% 18%
Wound complications 31% 5%
2nd Sx 15% 4%
LOS 13 d 11 d
Muller Lancet Jan 2002

Patient related risk factors
The timing of quitting ?!!!200 pts CABG post operative pulmonary complications
Non smoker 11.9% Quit > 8 weeks 14.5%quit < 8 weeks 57%Active smoker 33%
It takes few weeks for an improvement in ciliary and small airway function & a decrease in sputum production to happen.
Abrupt absence of the irritant effect of cigarette inhibits coughing secretions retention &small airway obstruction.
Warner Mayo Clin Proc 1989

Patient related risk factors
The timing of quitting ?!!• 300 patients with Lung Ca going for thoracotomy
• 21% Non smokers
• 62% Past quitters ( more than 2 months)
• 13% recent quitters ( less than 2 months )
• 4% ongoing smokers Barrera chest 2005

Quitting Timing in Thoracotomy
Barrera chest 2005Barrera chest 2005

Patient related risk factorsCOPD / Asthma• Optimal control should be achieved before SX bronchodilators , inhaled & systemic steroids
• potential adrenal insufficiency should be suspected
RCT 40 pt with COPD FEV1 57% CABG & similar EF 55% Oral prednisolone 20 mg po od for 10 days Steroid PlaceboFEV1 63% 57%Reintubation 0 4ICU stay 2 5Hospital stay 9 13No difference in wound dehiscence or infection
Hakan Jr Card Sx 2005

Obstructive Sleep Apnea
American academy of Sleep Medicine 2008


Procedures related risk factors
Anesthesia Effect on Respiratory physiology• Central drive loss blunted response to hypoxia & hypercapnia
• Reduction of respiratory muscle efficacy
• Reduced TV & RR reduced Minute Ventilation hypercapnia
Atelectasis V/Q mismatch & shunts hypoxia

Procedures related risk factors
Thoracic & Abd Sx effect on Respiratory physiology
• Reduced vital capacity 50% & FRC 30%
• Effect may last weeks
• Diaphragm function loss
Diminished cough & mucocilliary clearance induced by anesthetic & analgesic atelectaisis & pneumonia

Procedure Related risk factors
• Surgical siteThoracic sx 19-59% Upper abd sx 17-76% lower abd sx 0-5%
Lap chole FVC reduction 23% Vs 50% with laparotomy
• Surgery Duration < 2 hours PPC 8% Vs >3-4 hours PPC 40%
• Anesthesia TypeAlthough inconsistent result postoperative regional anesthesia had less rate of
PPC than general especially high risk pts
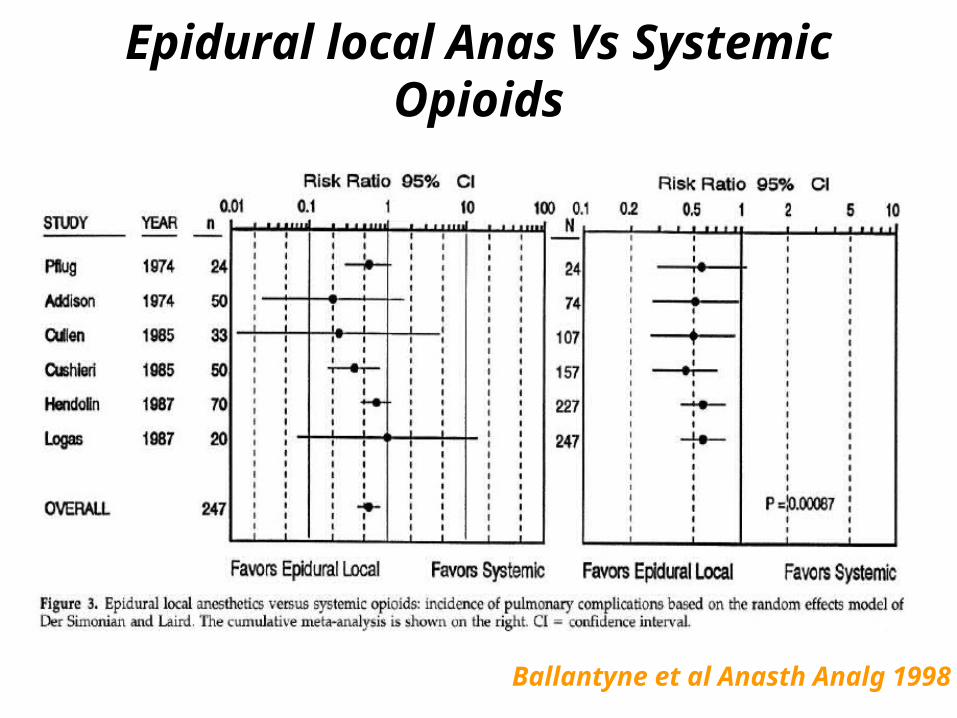
Epidural local Anas Vs Systemic Opioids
Ballantyne et al Anasth Analg 1998

Epidural Opioids Vs Systemic Opioids
Ballantyne et al Anasth Analg 1998

Sematana NEJM 2007








