
PRINCIPLES OFSYSTEM SAFETY
ENGINEERING AND MANAGEMENT
Felix RedmillRedmill Consultancy, London

(c) Felix Redmill, 2011 2
RISK
CERN, May '11
(c) Felix Redmill, 2011 3
SAFETY ENGINEERING AND MANAGEMENT
It is necessary both to achieve appropriate safety and to demonstrate that it has been achieved
• Achieve - not only in design and development, but in all stages of a system’s life cycle
• Appropriate - to the system and the circumstances
• Demonstrate - that all that could reasonably have been done has been done, at every stage of the life cycle
CERN, May '11

(c) Felix Redmill, 2011 4
THE U.K. LAW ON SAFETY
Health and Safety at Work Etc. Act 1974:
Safety risks imposed on others (employees and
the public at large) must be reduced ‘so far as is
reasonably practicable’ (SFAIRP)
CERN, May '11

(c) Felix Redmill, 2011 5
THE HSE’S ALARP PRINCIPLE
Limit of tolerability thresholdBroadly Acceptable Region(Risk is tolerable without reduction. But it is
necessary to maintain assurance that it remains at this level)
Broadly acceptable thresholdALARP or Tolerability Region(Risk is tolerable only if its reduction is
impracticable or if the cost of reduction is grossly disproportinate to the improvement
gained)
Increasing risk
Unacceptable Region(Risk cannot be justified except in
extraordinary circumstances)
CERN, May '11

(c) Felix Redmill, 2011 6
THE HSE’S ALARP PRINCIPLE
Intolerable region
The ALARP or
tolerability region
Broadly acceptable
region
Risk cannot be justified
except in extraordinary
circumstances
Risk is tolerable only if
further reduction is
impracticable or if its
cost is grossly
disproportionate to the
improvement gained
It is necessary to maintain
assurance that risk
remains at this level
CERN, May '11

(c) Felix Redmill, 2011 7
CALIBRATION OF THE ALARP MODELRecommended for Nuclear Industry
• Intolerability threshold:
– 1/10000 per year (for the public)
– 1/1000 per year (for employees)
• Broadly acceptable threshold:
– 1/1000000 per year (for everyone)
CERN, May '11

(c) Felix Redmill, 2011 8
A VERY SIMPLE SYSTEM
• Chemicals A and B are mixed in the tank to form product P
P opens & closes input and output valves• If emergency signal arrives, then cease operation
APEmergency signal P ControllerB
CERN, May '11

(c) Felix Redmill, 2011 9
QUESTIONS
• How could the accident have been avoided?
– Better algorithm
• How could the software designer have known that a better algorithm was required?
– Domain knowledge
• But we can’t be sure that such a fault won’t be made, so how can we find and correct such faults?
– Risk analysis techniques
CERN, May '11

(c) Felix Redmill, 2011 10
A SIMPLE THOUGHT EXPERIMENT
• Draw an infusion pump
– Note its mechanical parts
• Think about designing and developing software to control its operation
• Safety consideration: delivery of either too much or too little of a drug could be fatal
• How would you guarantee that it would kill no more than 1 in 10,000 patients per year?
– What level of confidence - on a percentage scale - do you have in your estimate?
CERN, May '11

(c) Felix Redmill, 2011 11
CONFIDENCE IN SAFETY IN ADVANCE
• What is safety?
• How can it be measured?
• What can give confidence that safety is high?
• Need also to demonstrate safety in advance
• Therefore, need to find hazards in advance
CERN, May '11

(c) Felix Redmill, 2011 12
NEW RISKS OF NEW TECHNOLOGY - STRASBOURG AIR CRASH
• Mode: climbs and descents in degrees to horizontal
– 3.3 descent represented as ‘minus 3.3’
• Mode: climbs and descents in units of 100 feet
– 3300 feet/minute descent represented as ‘minus 33’
• Plane was descending at 3300 feet/minute
• Needed to descend at angle of 3.3 to horizontal
• To interpret correctly, pilot needed to know the mode
• ‘Mode error’ in the system
• Human error? If so, which human made it?
CERN, May '11

(c) Felix Redmill, 2011 13
CONCERN WITH TECHNOLOGICAL RISKS
• We are concerned no longer exclusively with making
nature useful, or with releasing mankind from
traditional constraints, but also and essentially with
problems resulting from techno-economic development
itself [Beck]
• Risks induce often irreversible harm; not restricted to
their places of origin but threaten all forms of life in all
parts of the planet; in some cases could affect those
not alive at the time or place of an accident [Beck]
• People who build, design, plan, execute, sell and
maintain complex systems do not know how they may
work [Coates]
CERN, May '11
(c) Felix Redmill, 2011 14
RISK - AN IMPORTANT SUBJECT
• Risk is a subject of research in many fields,
e.g. Psychology, Sociology, Anthropology, Engineering
• It is a critical element in many fields
e.g. Geography (climate change), Agriculture, Sport, Leisure activities, Transport, Government policy
• It influences government policy (e.g. on bird flu) and local government decisions (e.g. closure of children’s playgrounds)
• An influential Sociological theory is that it is the most influential factor in modern society
(we are in ‘the risk society’)
• Every activity carries risk
• All decisions are ‘risky’
CERN, May '11

(c) Felix Redmill, 2011 15
FUNCTIONAL SAFETY:ACHIEVING UTILITY AND CREATING
RISK
We are concerned with safety that depends on the correct functioning of equipment
Control system
Utility(plus risks)
Equipment under control
CERN, May '11

(c) Felix Redmill, 2011 16
FUNCTIONAL SAFETY 2
Functional safety depends on hardware, software, humans, data, and interactions between all of these
Control system
Utility(plus risks)
Equipment under controlHumans (design, operation,
maintenance, etc.)(human factors)
Environment (management, culture, etc.)
CERN, May '11
(c) Felix Redmill, 2011 17
ORGANISATIONS ARE ALSO COMPLEX (Vincristine example)
• Child received injection for leukaemia into spine instead of into vein
• Root cause analysis showed 40 points at which the accident could have been averted
• Complexity of modern organisational systems• Need to identify risks in advance
– But no standard can do this for us• Requires a risk-based approach
CERN, May '11

(c) Felix Redmill, 2011 18
SAFETY - A DEFINITION
• Safety: freedom from unacceptable risk (IEC)
• Safety is not directly measurable
– But it may be addressed via risk
CERN, May '11

(c) Felix Redmill, 2011 19
VOCABULARY
• In common usage, “Risk” is used to imply:
– Likelihood (e.g. there’s a high risk of infection)
– Consequence (e.g. infection carries a high risk)
– A combination of the two
– Something, perhaps unspecified, to be avoided (e.g. going out into the night is risky)
CERN, May '11

(c) Felix Redmill, 2011 20
RISK - DEFINITIONS
• Risk: A combination of the probability of occurrence
and the severity of its consequences if the event did
occur (IEC)
• Tolerable risk: a willingness to live with a risk, so as to
secure certain benefits, in the confidence that the risk
is one that is worth taking and that it is being properly
controlled (HSE)
CERN, May '11

(c) Felix Redmill, 2011 21
SAFETY AND RISK
• Safety is only measurable in retrospect
• Safety is gauged by trying to understand risk
• Risk, being of the future, is estimable but not measurable
• The higher the risk, the lower the confidence in safety
• We increase safety by reducing risk
• Two components of risk are significant:
– Likelihood of occurrence
– Magnitude of outcome
CERN, May '11
(c) Felix Redmill, 2011 22
SOME PRINCIPLES
• Absolute safety (zero risk) cannot be achieved
• ‘Doing it well’ does not guarantee safety
– Correct functionality safety
– We must address safety as well as functionality
• Reliability is not a guarantee of safety
• We require confidence of safety in advance, not retrospectively
• We must not only achieve safety but also demonstrate it
CERN, May '11

(c) Felix Redmill, 2011 23
A RISK-BASED APPROACH
• If safety is addressed via risk
– We must base our safety-management actions on risk
• We must understand the risks in order to manage safety
CERN, May '11

(c) Felix Redmill, 2011 24
SAFETY AS A WAY OF THINKING
• If risk is too high, it must be reduced
• But how do we know how high it is?
– Carry out risk analysis
• But even if the risk is high, does it need to be
reduced?
– We must understand what risk is tolerable in
the circumstances (in the UK, apply the ALARP
Principle)
• Achieving safety demands a combination of
engineering and management approaches
CERN, May '11
(c) Felix Redmill, 2011 25
RISK - TWO COMPONENTS
• Two components:
– Probability (likelihood) of occurrence
– Consequence (magnitude of outcome)
• R = f(P.C) or f(L.C)
CERN, May '11

(c) Felix Redmill, 2011 26
A SIMPLE CALCULATION
Probability of a 100-year flood = 0.01/year
Expected damage = £50M
R (financial (Expected Value)
= 0.01 x £50,000,000 =
£500,000/year
CERN, May '11

(c) Felix Redmill, 2011 27
CONFIDENCE IN RISK VALUES
Accuracy of the result depends on the reliability of information
Reliability of information depends on the pedigree of its source
• What are the sources of the probability and consequence values?
• What are their pedigrees?
• What confidence do we have in the risk values?
• Why do we need confidence?
– Because we derive risk values in order to inform decisions
CERN, May '11
(c) Felix Redmill, 2011 28
CONFIDENCE IN RISK CALCULATIONS
• Where did the information come from?
– What trust do we have in the source?
– When and by whom was it collected?
– Was it ever valid? If so, is it still valid?
• What assumptions have we made?
– How valid are they?
– Are we aware of them?
CERN, May '11

(c) Felix Redmill, 2011 29
COT DEATH CASE
• A study concluded that the risk of a mature, non-smoking, affluent couple suffering a cot death is 8543 to 1
• Prof. Meadows deduced that Pr. of two cot deaths in the same family = 8543 x 8543 = 73 million to one
• Three cot deaths in her family resulted in Mrs Clark being convicted of infanticide
CERN, May '11

(c) Felix Redmill, 2011 30
DEPENDENCE AND NOT RANDOMNESS
• But deaths in the same family are not
independent events
(probability theory assumes independence)
• One death in the family rendered Mrs Clark “in the
highest-risk category” for another
– Probability of a second death is considerably
greater than 8543 to 1
CERN, May '11

(c) Felix Redmill, 2011 31
COMMON-MODE FAILURES
• Identifying common-mode failures is a crucial
part of traditional risk analysis
CERN, May '11
(c) Felix Redmill, 2011 32
ASSUMPTIONS
• We never have full knowledge
• We fill the gaps with assumptions
• Assumptions carry uncertainty, and therefore
risk
• Recognise your assumptions (if possible)
• If you admit to them (document them)
– Readers will recognise uncertainty
– Other persons may provide closer
approximations
CERN, May '11
(c) Felix Redmill, 2011 33
CONTROL OF RISK
• Risk is eliminated if either Pr or C is reduced to zero
• And risk is reduced by reduction of Pr or C or both
• In many cases we have no control over C, but we may be able to estimate it
• It may be difficult or impossible to derive Probability, but we may be able to reduce it (e.g. by software testing & fixing)
CERN, May '11

(c) Felix Redmill, 2011 34
WHY TAKE RISKS?
• Progress demands risk
– e.g. exploration, bridge design
– e.g. drug development (TeGenero’s TGN1412)
• Technology provides utility - at the cost of risk
• Suppliers want cheap designs
– e.g. Ronan Point (need to foresee hazards)
• To save money
– e.g. Cutting corners on a project
• To save face
– E.g. “I’d rather die than make a fool of myself”
• We can’t avoid taking risks in every decision and action
CERN, May '11

(c) Felix Redmill, 2011 35
RISK VS. RISK
• Decision is often not between risk and no risk
– But between one risk and another
– Decisions may create risks (unintended consequences)
• Surgery, medication, or keep the illness
• Consequences of being late vs. risks of driving fast
• Solar haze vs. global warming
• Software maintenance can introduce a new defect
– Change creates a new product; test results obsolete
• Recognise both risks
• Assess both
• Carry out impact analysis to identify new hazards
CERN, May '11
(c) Felix Redmill, 2011 36
SOME NOTES ON RISK
• A single-system risk may be tiny, but the overall risk of many systems may be high (individual vs. societal risk)
• Risk per usage may be remote, but daily use may accrue a high risk (one-shot vs. lifetime risk)
• Beware of focusing on a single risk; a system is likely to carry numerous risks
• Confidence in probabilities attributed to rare events must be low
• For random events with histories (e.g. electromechanical equipment failure) frequencies may be deduced
– Given similar circumstances, they may be predictive
• For systematic events (such as software failure) history is not an accurate predictor of the future
CERN, May '11

(c) Felix Redmill, 2011 37
RISK AND UNCERTAINTY
• Risk is of the future - there is always uncertainty
• Risk may be estimated but not measured
• Risk is open to perception
• Identifying and analysing risks requires information
• The quality of information depends on the source
• 'Facts' are open to different interpretations
• Risk cannot be eliminated if goals are to be achieved
• Risk management activities may introduce new risks
• In the absence of certainty, we need to increase confidence
• Reducing uncertainty depends on gathering information
CERN, May '11
(c) Felix Redmill, 2011 38
RISK MANAGEMENT STRATEGIES
• Avoid• Eliminate• Reduce• Minimise - within defined constraints• Transfer or share
- Financial risks may be insured- Technical risks may be transferred to experts,
maintainers• Hedge
- Make a second investment, which is likely to succeed if the first fails
• Accept- Must do this in the end, when risks are deemed
tolerable- Need contingency plans to reduce consequences
CERN, May '11

(c) Felix Redmill, 2011 39
RISK IS OPEN TO PERCEPTION
• Voluntary or involuntary• Control in hands of self or another• Statistical or personal• Level of knowledge, uncertainty• Level of dread or fear evoked• Short-term or long-term view• Severity of outcome• Value of the prize• Level of excitement• Status quo bias
Perception determines where we look for risks and what we identify as risks
CERN, May '11
(c) Felix Redmill, 2011 40
PROGRAMME FOR COMBATTING DISEASE (1)
• The country is preparing for the outbreak of a disease which is expected to kill 600 people. Two alternative programmes to combat it have been proposed, and the experts have deduced that the precise estimates of the outcomes are:
• If programme A is adopted, 200 people will be saved
• If programme B is adopted, there is a one third probability that 600 people will be saved and a two thirds probability that nobody will be saved
CERN, May '11

(c) Felix Redmill, 2011 41
PROGRAMME FOR COMBATTING DISEASE (2)
• The country is preparing for the outbreak of a disease which is expected to kill 600 people. Two alternative programmes to combat it have been proposed, and the experts have deduced that the precise estimates of the outcomes are:
• If programme C is adopted, 400 people will die
• If programme D is adopted, there is a one third probability that nobody will die and a two thirds probability that 600 people will die
CERN, May '11
(c) Felix Redmill, 2011 42
UNINTENDED CONSEQUENCES
• Actions always likely to have some unintended results
– Downsizing but loose the wrong staff
e.g. University redundancies in UK
– Staff come to rely entirely on a support system
– Building high in mountain causes landslide
– Abolishing DDT increased malaria
– Store less chemical at plant, more trips by road
• Unintended, but not necessarily unforeseeable
• Foreseeable, but not necessarily obvious
• Carry out hazard and risk analysis
– Better to foresee them than encounter them later
CERN, May '11

(c) Felix Redmill, 2011 43
RISK COMMUNICATION
• The risk analyst is usually not the decision maker– Risk information must be transferred (liver
biopsy)• Usually only results are communicated
– e.g. There’s an 80% chance of success• But are they correct (Bristol Royal Infirmary)?
– Overconfidence bias• Managers rely heavily on risk information,
collected, analysed, packaged, by other staff• But what confidence does the staff have in it
– What were the information sources, analysis methods, and framing choices?
– What uncertainties exist?– What assumptions were made?
CERN, May '11

(c) Felix Redmill, 2011 44
COMMUNICATION OF RISK INFORMATION
• ‘The risk is one in a million’
• One in seventeen thousand of dying in a road accident
– Age, route, time of day
• Framing
• Appropriate presentation of numbers
– 1 x 10-6
– One in a million
– One in a city the size of Birmingham
– (A launch per day for 300 years with only one failure)
CERN, May '11

(c) Felix Redmill, 2011 45
RISK IS TRICKY
• We manage risks daily, with reasonable success
• Our risk management is intuitive
– We do not recognise mishaps as the results of poor risk management
• Risk is a familiar subject
• We do not realise what we don’t know
• We do not realise that our intuitive techniques for managing simple situations are not adequate for complex ones
• Risk estimating can be simple arithmetic
• The difficult part is obtaining the correct information on which to base estimates - and decisions
CERN, May '11

(c) Felix Redmill, 2011 46
SAFETY ENGINEERING PRINCIPLES
CERN, May '11

CERN, May '11 47
A SIMPLE MODEL OF SYSTEM SAFETY
DisasterDangerSafe state (in any mode)
Failureor unsafe deviation
RestorationAccidentRecovery
(c) Felix Redmill, 2011

(c) Felix Redmill, 2011 48
SAFETY ACROSS THE LIFE CYCLE
• Safety activities must extend across the life of a system
– And must be planned accordingly
• Modern safety standards call for the definition and use of a safety life cycle
• A life-cycle model shows all the phases of a system’s life, relative to each other
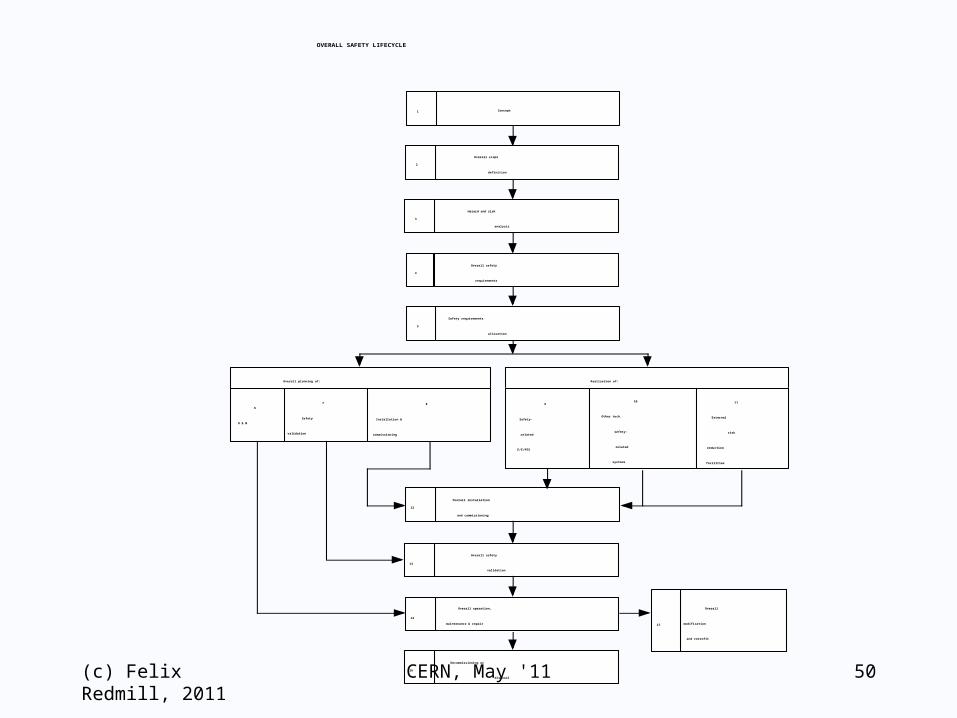
• The ‘overall safety lifecycle’ defined in safety standard IEC 61508 is the best known model
CERN, May '11

(c) Felix Redmill, 2011 49
SAFETY LIFE CYCLE MODELS
• Provide a framework for planning safety engineering and management activities
• Provide a guide for creating an infrastructure for the management of project and system documentation
• Remind engineers and managers at each phase that they need to take other phases into consideration in their planning and activities
• Facilitate the demonstration as well as the achievement of safety
• The model in safety standard IEC 61508 is the best known
CERN, May '11
(c) Felix Redmill, 2011 50
Overall
modification
and retrofit
1 Concept
2
Overall scope
definition
3
Hazard and risk
analysis
Overall safety
requirements
Safety requirements
allocation
4
5
6
O & M
7
Safety
validation
8
Installation &
commissioning
Overall planning of:
9
Safety-
related
E/E/PES
10
Other tech.
safety-
related
systems
11
External
risk
reduction
facilities
Realisation of:
12
Overall installation
and commissioning
13
Overall safety
validation
14
Overall operation,
maintenance & repair
16
Decommissioning or
disposal
15
OVERALL SAFETY LIFECYCLE
CERN, May '11
(c) Felix Redmill, 2011 51
AFTER STAGE THREE
Work done after stage 3 of the model creates
additions to the overall system that were not
included in the hazard and risk analysis of
stage 3
CERN, May '11

SAFETY LIFECYCLE SUMMARY
Understand the functional goals and design
Identify the hazards
Analyse the hazards
Determine and assess the risks posed by the hazards
Specify the risk reduction measures and their SILs
Define the required safety functions (and their SILs)
Carry out safety validation
Operate, maintain, change, decommission, dispose safely
(c) Felix Redmill, 2011 52CERN, May '11

(c) Felix Redmill, 2011 53
THE SAFETY-CASE PRINCIPLE
• The achievement of safety must be demonstrated in advance of deployment of the system
• Demonstration is assessed by independent safety assessors
• Safety assessors will not (cannot)
– Examine a complex system without guidance
– Assume responsibility for the system’s safety
• Their assessment is guided by claims made by developers, owners and operators of the system
• The claims must be for the adequacy of safety in defined circumstances, considering the context and application and the benefits of accepting any residual risks
CERN, May '11

(c) Felix Redmill, 2011 54
THE SAFETY CASE
• The purpose: Demonstration of adequate and appropriate safety of a system, under defined conditions
– To convince ourselves of adequate safety
– The basis of independent safety assessment
– Provides later requirements for proof
(It can protect and it can incriminate)
• The means
– Make claims of what is adequately safe
o And for what it is adequately safe
– Present arguments for why it is adequately safe for the intended purpose
– Provide evidence in support of the arguments
CERN, May '11

(c) Felix Redmill, 2011 55
GENERALIZED EXAMPLE
• Claim: System S is acceptably safe when used in Application A
• Claims are presented as structured arguments
– The use of System S in Application A was subjected to thorough hazard identification
– All the identified hazards were analysed
– All risks associated with the hazards either were found to be tolerable or have been reduced to tolerable levels
– Emergency plans are in place in case of unexpected hazardous events
• The safety arguments are supported by evidence
– e.g., Evidence of all activities and results, descriptions of all relevant documentation, and references to it
CERN, May '11

(c) Felix Redmill, 2011 56
THE CASE MUST BE STRUCTURED
• Demonstration of adequate safety of a system requires demonstration of justified confidence in its components
• Some components may be COTS (commercial off-the-shelf)
– Don’t wait until too late to find that they cannot be justified
• Evidence is derived from different sources, and different categories of sources
• The evidence for each claim must be structured so as to support a logical argument for the “top-level” claim
CERN, May '11

(c) Felix Redmill, 2011 57
PRESENTATION OF SAFETY CLAIMS
• The claims must be structured so that the logic of the overall case is demonstrated
• The principal claims may be presented in a “top-level” document
– With references out to the sources of supporting evidence (gathered throughout the life cycle)
• Modern software-based tools are available for the documentation of safety cases (primarily: GSN (goal-structured notation))
CERN, May '11

CERN, May '11 58
THE NATURE OF EVIDENCE
• Evidence may need to be probabilistic
– e.g. for nuclear plants
• It may be qualitative
– e.g. for humans, software
• In applications of human control it may need to include
– Competence, training, management, guidelines
• It is collected throughout the system’s life
– Importantly during development
(c) Felix Redmill, 2011

CERN, May '11 59
EVIDENCE PLANNING - 1
• Any system-related documentation (project, operational, maintenance) may be required as evidence
• It should be easily and quickly accessible to
– Creators of safety arguments
– Independent safety assessors
• Numbering and filing systems should be designed appropriately
• Principal safety claims should be identified in advance
– Activities may need to be planned so that appropriate evidence is collected and stored
• The safety case should be developed throughout a development project
– And maintained throughout a system’s life
(c) Felix Redmill, 2011

CERN, May '11 60
EVIDENCE PLANNING - 2
• The safety case structure should be designed early
• Evidential requirements should be identified early and planned for
• Safety case development should be commenced early
• Evidence of software adequacy may be derived from
– Analysis
– Testing
– Proven-in-use
– Process
(c) Felix Redmill, 2011

(c) Felix Redmill, 2011 61
VALIDITY OF A SAFETY CASE
Validity (and continued validity) depends on (examples only)
• Observance of design and operational constraints, e.g.:
– Use only specified components
– Don’t exceed maximum speed
• Environment, e.g.:
– Hardware: atmospheric temperature between T1 & T2C
– Software: operating system remains unchanged
• Assumptions remain valid, e.g.:
– Those underlying estimation of occurrence probability
– Routine maintenance carried out according to spec.
CERN, May '11

(c) Felix Redmill, 2011 62
HAZARD AND RISK ANALYSIS
CERN, May '11

(c) Felix Redmill, 2011 63
NEED FOR CLARITY
• Is a software bug a risk?
• Is a banana skin on the ground a risk?
• Is a bunker on a golf course a risk?
CERN, May '11

(c) Felix Redmill, 2011 64
THE CONCEPT OF A HAZARD
• A hazard is the source of risk
– The risks that may arise depend on context
• What outcomes could result from the hazard?
• What consequences might the outcomes lead to?
• Hazards form the basis of risk estimation
CERN, May '11

(c) Felix Redmill, 2011 65
GOLF-SHOT RISK
• What is the probability of hitting your golf ball into a bunker?
• What is the consequence (potential consequence) of hitting your ball into a bunker?
• Should I “take the risk”?
– In this case: What level of risk should I take?
• What’s missing is a question about benefit!
CERN, May '11

WHAT IS RISK ANALYSIS?
• If we take risk to be a function of Probability (Pr) & Consequence (C)– Then, in order to estimate a value of a Risk, we
need to derive values of Pr and C for that risk• Values may be qualitative or quantitative• They may need to be more or less “accurate”,
depending on importance• Thus, risk analysis consists of:
– Identifying relevant hazards– Collecting evidence that could contribute to the
determination of values of Pr and C for a defined risk
– Analysing that evidence– Synthesising the resulting values of Pr and C
(c) Felix Redmill, 2011 CERN, May '11 66

(c) Felix Redmill, 2011 67
PROBABILITY OF WHAT EXACTLY?
• Automobile standards focus on the control of a vehicle (and the possible loss of it)
• Each different situation will
– Occur with a different probability
– Result in different consequences
– Carry different risks
CERN, May '11

(c) Felix Redmill, 2011 68
CHOICE OF CONSEQUENCE ESTIMATES
• Worst possible
• Worst credible
• Most likely
• “Average”
CERN, May '11

(c) Felix Redmill, 2011 CERN, May '11 69
DETERMINATION OF RISK VALUES
Threat to security
Safety hazard
Threat of damage
Potential for unreliability
Potential for unavailability
Causal analysis
Consequence analysis
Risk

(c) Felix Redmill, 2011 CERN, May '11 70
PRELIMINARY REQUIREMENTS
• Knowledge of the subject of risk
• Understanding of the current situation and context
• Knowledge of the purpose of the intended analysis
– The questions (e.g. tolerability) that it must answer
Such knowledge and understanding are essential to searching for the appropriate information

(c) Felix Redmill, 2011 CERN, May '11 71
BOTTOM-UP ANALYSIS(Herald of Free Enterprise)
Bowsun asleep in his cabin when ship is due to depart↓
Bow doors not closed↓
Ship puts to sea with bow doors open↓
Water enters car deck↓
, As ship rolls water rushes to one side↓
Ship capsizes↓ Lives lost

(c) Felix Redmill, 2011 CERN, May '11 72
TOP-DOWN ANALYSIS(Herald of Free Enterprise)
Ship puts to sea with bow doors openBosun did not close doorsBosun not availableto close doors
Problem with doors& bosun can’t close them
Bosun noton shipDoor or hinge problem
Problem with closing
mechanism
Problem with power supply
Bosun on board but not at stationBosun asleepin cabinBosun in bar

(c) Felix Redmill, 2011 73
RISK MANAGEMENT PROCESS
• Define scope of study
• Identify the hazards
• Analyse the hazards to determine the risks they pose
• Assess risks against tolerability criteria
• Take risk-management decisions and actions
• It may also be appropriate to carry out emergency planning and prepare for the unexpected
– If so, we need to carry out rehearsals
CERN, May '11
(c) Felix Redmill, 2011 74
FOUR STAGES OF RISK ANALYSIS(But be careful with vocabulary)
• Definition of scope– Define the objectives and scope of the study
• Hazard identification– Define hazards and hazardous events
• Hazard analysis– Determine the sequences leading to hazardous
events– Determine likelihood and consequences of
hazardous events• Risk assessment
– Assess tolerability of risks associated with hazardous events
CERN, May '11
(c) Felix Redmill, 2011 75
DEFINITION OF SCOPE
• Types of risks to be studied
– e.g. safety, security, financial
• Risks to whom or what
– e.g. employees, all people, environment, the company, the mission
• Study boundary
– Plant boundary
– Region
• Admissible sources of information
– e.g. stakeholders (which?), experts, public
CERN, May '11

(c) Felix Redmill, 2011 76
SCOPE OF STUDY
• How will the results be used?
– What questions are to be answered?
– What decisions are to be made?
• What accuracy and confidence are required?
• Define study parameters
– What effort to be invested?
– What budget afforded?
– How much time allowed?
CERN, May '11

CERN, May '11 77
OUTCOME SUBJECTIVELY INFLUENCED
• Defining scope is subjective– Involves judgement– Includes bias– Can involve manipulation
• Scope definition– Influences the nature and direction of the
analysis– Is a predisposing factor on its results
(c) Felix Redmill, 2011

(c) Felix Redmill, 2011 CERN, May '11 78
VOCABULARY - CHOICE OF TERMS
• Same term means different things to different people
• Same process given different titles
• There is no internationally agreed vocabulary
• Even individuals use different terms for the same process
• Beware: ask what others mean by their terms
• Have a convention and define it

(c) Felix Redmill, 2011 CERN, May '11 79
SOME TERMS IN USE
Hazard identification,Risk identification
Hazard analysis,Risk analysis
Risk assessment,Risk evaluation
Risk mitigation,Risk reduction,Risk management
Risk analysis,Risk assessment, Risk management

(c) Felix Redmill, 2011 CERN, May '11 80
AN APPROPRIATE CONVENTION?
Scope definition
Hazard identification
Hazard analysis
Risk assessment
Risk communication
Risk mitigation
Emergency planning
Risk analysis
Risk management

(c) Felix Redmill, 2011 81
HAZARD AND RISK ANALYSIS
• Obtaining appropriate information, from the most appropriate sources, and analyzing it, while making assumptions that are recognized, valid, and as few as possible
CERN, May '11

(c) Felix Redmill, 2011 82
HAZARD IDENTIFICATION
• The foundation of risk analysis
- Identify the hazards (what could go wrong)
- Deduce their causes
- Determine whether they could lead to undesirable outcomes
• Knowing chains of cause and effect facilitates decisions on where to take corrective action
• But many accidents are caused by unexpected interactions rather than by failures
CERN, May '11

(c) Felix Redmill, 2011 83
HAZARD ID METHODS
• Checklists• Brainstorming
• Expert judgement
• What-if analysis
• Audits and reports
• Site inspections
• Formal and informal staff interviews
• Interviews with others, such as customers, visitors
• Specialised techniques
CERN, May '11

(c) Felix Redmill, 2011 84
WHAT WE FIND DEPENDS ON WHERE WE LOOK
• We don’t find hazards where we don’t look• We don’t look because
– We don’t think of looking there– We don’t know of that place– We assume there are no hazards there– We assume that the risks are small
• Must take a methodical approach– And be thorough
CERN, May '11

(c) Felix Redmill, 2011 85
CRACK IN “TIRELESS” COOLING SYSTEM
CERN, May '11

(c) Felix Redmill, 2011 86
EXTRACT FROM ‘FILE ON 4’ INTERVIEW (12/12/00)
• (O'Halloran) For the Navy Captain Hurford concedes that the possibility that this critical section of pipework might fail was never even considered in the many years that these 12 submarines of the Swiftsure and Trafalgar classes have been in service.
• (Hurford) "This component was analysed against its duty that it saw in service and was supposed never to crack and so the fact that this crack had occurred in this component in the way that it did and caused a leak before we had detected it, is a serious issue.”
• (O'Halloran) How big a question mark does this place over your general risk probability assumptions … about the whole working of one of these nuclear reactors.
• (Hurford) "It places a question on the surveillance that we do when the submarines are in refit and maintenance, unquestionably”
• (O'Halloran) How long have these various submarines been in service ?• (Hurford) "The oldest of the Swiftsure class came into service in the early seventies”• (O'Halloran) So has this area of the pipework ever been looked at in any of the submarines,
the 12 hunter killer submarines now in service ?• (Hurford) "No it hasn't, because the design of the component was understood and the
calculations showed and experience showed that there would be no problem.”• (O'Halloran) But the calculations were wrong ?• (Hurford) "Clearly there is something wrong with that component that caused the crack and
we don't know if it was the calculations or whether it was the way it was made and that what is being found out in the analysis at the moment"
CERN, May '11

(c) Felix Redmill, 2011 87
REPEAT FORMAL HAZARD ID
• Hazard identification should be repeated
when new information becomes available and when significant change is proposed. e.g.– At the concept stage
– When a design is available
– When the system has been built
– Prior to system or environmental change during operation
– Prior to decommissioning
CERN, May '11

(c) Felix Redmill, 2011 88
HAZARD ANALYSIS
• Analyse the identified hazards to determine
– Potential consequences
Worst credible
Most likely
– Ways in which they could lead to undesirable outcomes
– Likelihood of undesirable outcomes
• Sometimes rough estimates are adequate
• Sometimes precision is essential
– Infusion pump (too much: poison; too little: no cure)
– X-ray dose (North Stafford)
CERN, May '11

(c) Felix Redmill, 2011 89
NOTES ON HAZARD ANALYSIS
• Two aspects of a hazard: likelihood and consequence
• Consequence is usually closely related to system goals
– So risk reduction may focus on reduction of likelihood
• Usually numerous hazards associated with a system
• Analysis is based on collecting and deriving appropriate information
• Pedigree of information depends on pedigree of its source
• The question of confidence should always be raised
• Likelihood and consequences may be expressed quantitatively or qualitatively
CERN, May '11

CERN, May '11 90
NOTES ON HAZARD ANALYSIS - 2
• For random events (such as hardware component failure)
– Historic failure frequencies may be known
– Probabilistic hazard analysis may be possible
• For systematic events (such as software failures)
– History is not an accurate predictor of the future
– Qualitative hazard analysis is necessary
• When low event frequencies (e.g. 10-6 per year) are desired, confidence in figures must be low
(c) Felix Redmill, 2011

CERN, May '11 91
THE NEED FOR QUALITATIVE ANALYSIS AND ASSESSMENT
• When failures and hazardous events are random
– Historic data may exist
– Numerical analysis may be possible
• When failures and hazardous events are systematic, or historic data do not exist
– Qualitative analysis and assessment are necessary
• Example of qualitative techniques is the risk matrix
(c) Felix Redmill, 2011
(c) Felix Redmill, 2011 92
HAZARD ANALYSIS TECHNIQUES
• FMEA analyses the effects of failures
• FMECA analyses the risks attached to failures
• HAZOP analyses both causes and effects
• Event tree analysis (ETA) works forward from
identified hazards or events (e.g. component
failures) to determine their consequences
• Fault tree analysis (FTA) works backwards from
identified hazardous events to determine their
causes
CERN, May '11

(c) Felix Redmill, 2011 93
USING THE RESULTS
• The purpose is to derive reliable information on which to base decisions on risk-management action
• ‘Derive’ - by carrying out risk analysis
• ‘Reliable’ - be thorough as appropriate
• ‘Information’ - the key to decision-making
• ‘Decisions’ - risk analysis is not carried out for its own sake but to inform decisions (usually made by others)
• Hazard identification and analysis may be carried out concurrently
CERN, May '11

(c) Felix Redmill, 2011 94
RISK ASSESSMENT
• To determine the tolerability of analysed risks
– So that risk-management decisions can be taken
• Need tolerability criteria
• Tolerability differs according to circumstance
– e.g. medical
• Tolerability differs in time
– e.g. nuclear
• Tolerability differs according to place
– e.g. oil companies treatment of staff and environment in different countries
CERN, May '11

(c) Felix Redmill, 2011 95
TOLERABLE RISK
• Risk accepted in a given context based on the current values of society
• Not trivial to determine• Differs across industry sectors• May change with time• Depends on perception• Should be determined by discussion among
parties, including– Those posing the risks– Those to be exposed to the risks– Other stakeholders, e.g. regulators
CERN, May '11
(c) Felix Redmill, 2011 96
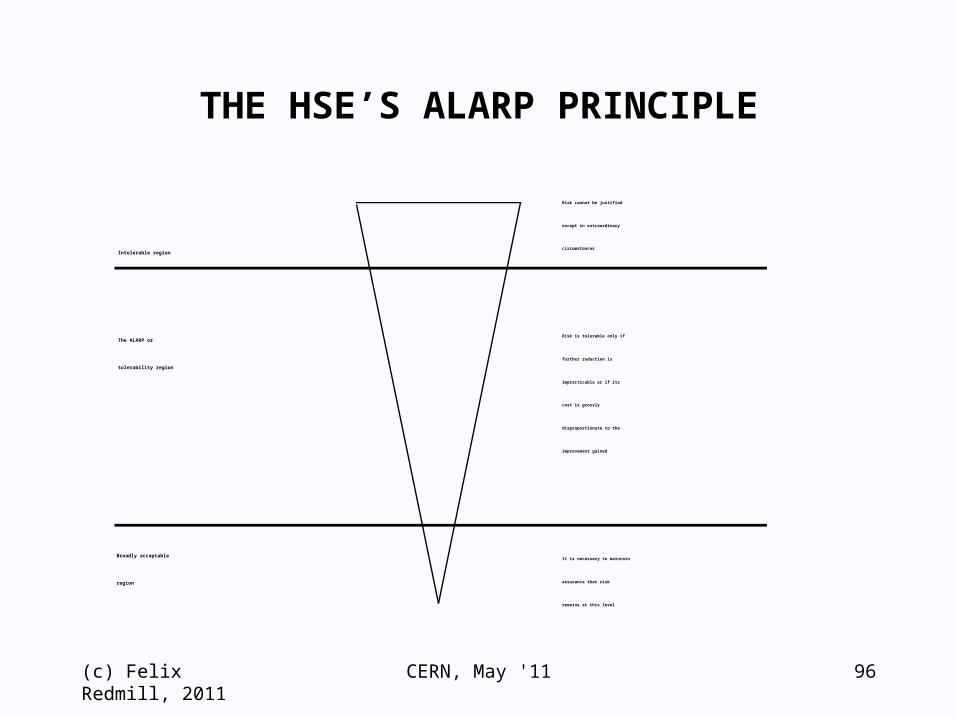
THE HSE’S ALARP PRINCIPLE
Intolerable region
The ALARP or
tolerability region
Broadly acceptable
region
Risk cannot be justified
except in extraordinary
circumstances
Risk is tolerable only if
further reduction is
impracticable or if its
cost is grossly
disproportionate to the
improvement gained
It is necessary to maintain
assurance that risk
remains at this level
CERN, May '11

(c) Felix Redmill, 2011 97
RISK TOLERABILITY JUDGEMENT
• In the case of machinery
– We may know what could go wrong (uncertainty is low)
– It may be reversible (can fix it after one accident)
• In the case of BSE or genetically modified organisms
– The risk may only be suspected (uncertainty is high)
– It may be irreversible
• Moral values influence the judgement of how much is enough
• If we don’t take risks we don’t make progress
CERN, May '11

(c) Felix Redmill, 2011 98
HAZARD AND RISK ANALYSIS TECHNIQUES
CERN, May '11

(c) Felix Redmill, 2011 CERN, May '11 99
TECHNIQUES
Techniques support risk analysis
– They should not govern it

(c) Felix Redmill, 2011 CERN, May '11 100
TECHNIQUES TO BE CONSIDERED
• Failure (fault) modes and effects analysis (FMEA)• Failure (fault) modes, effects and criticality analysis
(FMECA)• Hazard and operability studies (HAZOP)• Event tree analysis (ETA)• Fault tree analysis (FTA)• Risk matrices• Human reliability analysis (HRA - mentioned only)• Preliminary hazard analysis (PHA)

(c) Felix Redmill, 2011 CERN, May '11 101
A SIMPLE CHEMICAL PLANT
P1V1V2P2 Vat RFluid BFluid AV3
(c) Felix Redmill, 2011 CERN, May '11 102
FAILURE MODES AND EFFECTS ANALYSIS
• Usually qualitative investigation of the modes of failure of individual system components
• Components may be at any level (e.g. basic, sub-system)
• Components are treated as black boxes
• For each failure mode, FMEA investigates
– Possible causes
– Local effects
– System-level effects
• Corrective action may be proposed
• Best done by a team of experts with different viewpoints

(c) Felix Redmill, 2011 CERN, May '11 103
FAILURE MODES AND EFFECTS ANALYSIS
• Boundary of study must be clearly defined
• Does not usually find the effects of
– Multiple faults or failures
– Failures caused by communication and interactions between components
– Integration of components
– Installation

(c) Felix Redmill, 2011 CERN, May '11 104
EXAMPLE FMEA OF A SIMPLE CHEMICAL PROCESS
StudyNo.
Item Failuremode
Possiblecauses
Localeffects
System-level
effects
Proposedcorrection
1 PumpP1
Fails tostart
1. No power
2. Burnt out
Fluid Adoes notflow
Excess ofFluid B inVat R
Monitorpumpoperat ion
2 Burns out 1. Loss oflubricant
2. Excessivetemperature
Fluid Adoes notflow
Excess ofFluid B inVat R
Add alarmto pumpmonito r
3 ValveV1
Sticksclosed
1. No power
2. Jammed
Fluid Acannotflow
Excess ofFluid B inVat R
MonitorValveoperat ion
4 Sticksopen
1. No power
2. Jammed
Cannotst opflow ofFluid A
Danger ofexcess ofFluid A inVat R
Introduceaddit ionalvalve inseries

(c) Felix Redmill, 2011 CERN, May '11 105
FAILURE MODES, EFFECTS AND CRITICALITY ANALYSIS
• FMECA = FMEA + analysis of the criticality of each failure
• Criticality in terms of risk or one of its components
– i.e. severity and probability or frequency of occurrence
– Usually quantitative
• Purpose: to identify the failure modes of highest risk
– This facilitates prioritization of corrective actions, focusing attention and resources first where they will have the greatest impact on safety
• Recording: add one or two columns to a FMEA table

(c) Felix Redmill, 2011 CERN, May '11 106
HAZARD AND OPERABILITY STUDIES (HAZOP)
• The methodical study of a documented representation of a system, by a managed team, to identify hazards and operational problems.
• Correct system operation depends on the attributes of the items on the representation remaining within design intent. Therefore, studying what would happen if the attributes deviated from design intent should lead to the identification of the hazards associated with the system's operation. This is the principle of HAZOP.
• 'Guide words' are used to focus the investigation on the various types of deviation.
(c) Felix Redmill, 2011 CERN, May '11 107
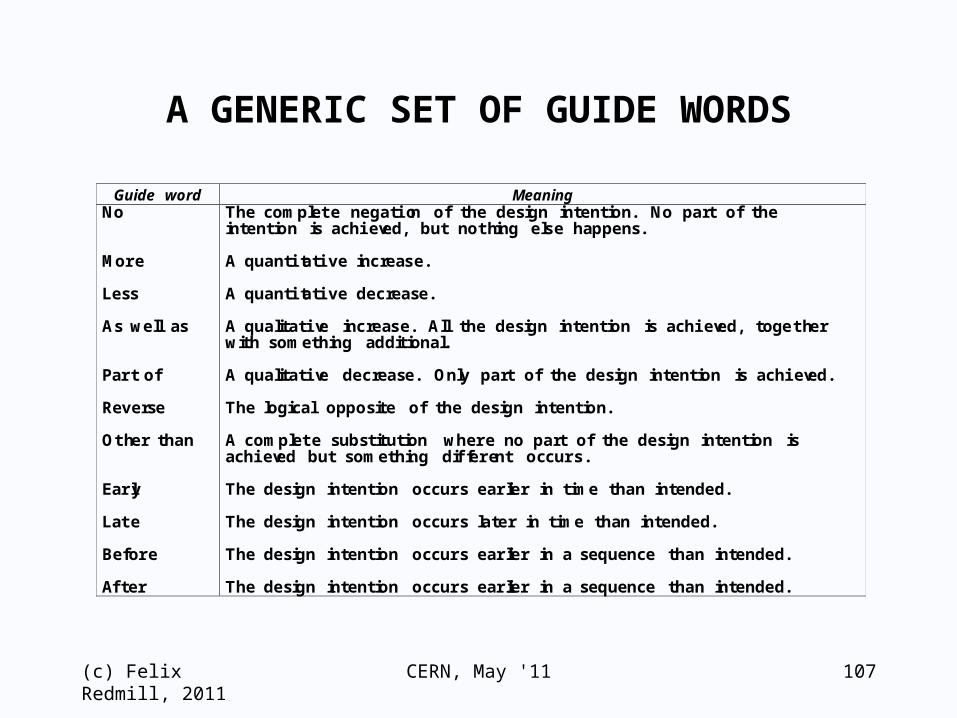
A GENERIC SET OF GUIDE WORDS
Guide word MeaningNo
More
Less
As well as
Part of
Reverse
Other than
Early
Late
Before
After
The complete negation of the design intention. No part of theintention is achieved, but nothing else happens.
A quantitative increase.
A quantitative decrease.
A qualitative increase. All the design intention is achieved, togetherwith something additional.
A qualitative decrease. Only part of the design intention is achieved.
The logical opposite of the design intention.
A complete substitution where no part of the design intention isachieved but something different occurs.
The design intention occurs earlier in time than intended.
The design intention occurs later in time than intended.
The design intention occurs earlier in a sequence than intended.
The design intention occurs earlier in a sequence than intended.

(c) Felix Redmill, 2011 CERN, May '11 108
HAZOP OVERVIEWPresentation of design
representationExamine
design representation methodically
Possibledeviation from design intent
?
Examine consequences
and causes
Document results
Define follow-up work
Time up, or completed study?
Agree documentationSign off meetingIntroductionsYesNoNoYes

(c) Felix Redmill, 2011 CERN, May '11 109
HAZOP SUMMARY
• HAZOP is a powerful technique for hazard identification - and analysis
• It requires a team of carefully chosen members• It depends on planning, preparation, and
leadership• A study usually requires several meetings• Study proceeds methodically• Guide words are used to focus attention• Outputs are the identified hazards,
recommendations, questions
(c) Felix Redmill, 2011 CERN, May '11 110
EVENT TREE ANALYSIS
• Starts with an event that might affect safety
• Follows a cause-and-effect chain to the system-level consequence
• Does not assume that an event is hazardous
• Includes both operational and fault conditions
• Each event results in a branch, so N events = 2N branches
• If event probabilities can be derived
– They may be assigned to the branches of the tree
– The probability of the final events may be calculated

(c) Felix Redmill, 2011 CERN, May '11 111
A SIMPLE EVENT TREE
Valve operatesValve monitor O.K.
Alarm relay O.K.Claxon O.K.Operator respondsYesNoYesYesNoNoNoOutcomeYesNoSafe outcomeUnsafe outcomes

(c) Felix Redmill, 2011 CERN, May '11 112
REFINED EVENT TREE
Valve operatesValve monitor functions
Alarm relay operates
Claxon soundsOperator respondsYesYesYesYesNoNo

(c) Felix Redmill, 2011 CERN, May '11 113
EVENT TREE: ANOTHER EXAMPLE
Fire startsFire spreads quickly
Sprinkler fails to work
People cannot escape
Resulting eventNo (P=0.6)Yes (P=0.1)Yes (P=0.2)No (P=0.9)No (P=0.8)YesYes (P=0.4)Multiple fatalitiesDamage and lossFire controlledFire contained

(c) Felix Redmill, 2011 CERN, May '11 114
BOTTOM-UP ANALYSIS(Herald of Free Enterprise)
Bowsun asleep in his cabin when ship is due to depart↓
Bow doors not closed↓
Ship puts to sea with bow doors open↓
Water enters car deck↓
, As ship rolls water rushes to one side↓
Ship capsizes↓ Lives lost

(c) Felix Redmill, 2011 CERN, May '11 115
TOP-DOWN ANALYSIS(Herald of Free Enterprise)
Ship puts to sea with bow doors openBosun did not close doorsBosun not availableto close doors
Problem with doors& bosun can’t close them
Bosun noton shipDoor or hinge problem
Problem with closing
mechanism
Problem with power supply
Bosun on board but not at stationBosun asleepin cabinBosun in bar

(c) Felix Redmill, 2011 CERN, May '11 116
FAULT TREE ANALYSIS
• Starts with a single 'top event' (e.g., a system failure)• Combines the chains of cause and effect which could
lead to the top event• Next-level causes are identified and added to the tree
and this is repeated until the most basic causes are identified
• Causal relationships are defined by AND and OR gates• One lower-level event may cause several higher-level
events• Examples of causal events: component failure, human
error, software bug• Each top-level undesired event requires its own fault
tree• Probabilities may be attributed to events, and from
these the probability of the top event may be derived
(c) Felix Redmill, 2011 CERN, May '11 117
EXAMPLE FTA OF SIMPLE CHEMICAL PROCESS
ORORORExcess of Fluid Ain Vat R
Too much of Fluid A enters Vat R
Insufficient Fluid B enters Vat R
Run out of Fluid B
Pump P2 fails
Valve V2 sticks shut
Valve V1 sticks openTank leakingTank not filled
(c) Felix Redmill, 2011 CERN, May '11 118
THE PRINCIPLE OF THE PROTECTION SYSTEM
Required event frequency
10-7 per hour
Dangerous failure frequency of
equipt.: 10-3 / hour
Reliability of safety function
10-4 / hour
AND

(c) Felix Redmill, 2011 CERN, May '11 119
COMPLEMENTARITY OF TECHNIQUES
• Compare results of FMEA with low-level causes from FTA
• Carry out HAZOP on a sub-system identified as risky by a high-level FMEA
• Carry out ETA on low-level items identified as risky by FTA

(c) Felix Redmill, 2011 CERN, May '11 120
A RISK MATRIX(An example of qualitative risk
analysis)
Likelihoodor
Frequency
Consequence
Negligible Moderate High Catastrophic
High
Medium
Low
(c) Felix Redmill, 2011 CERN, May '11 121
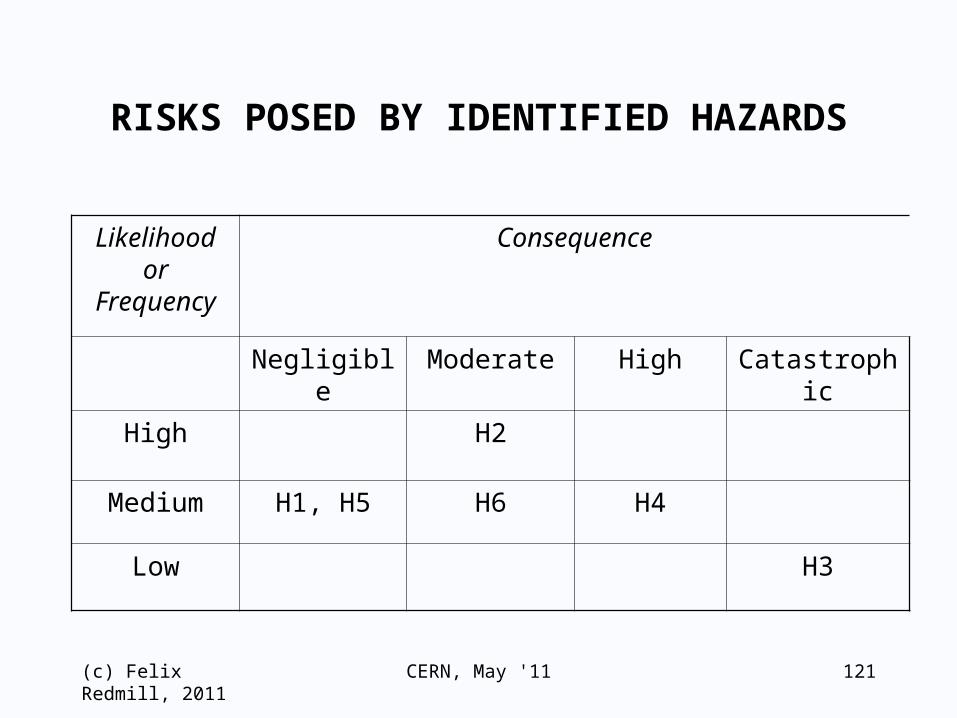
RISKS POSED BY IDENTIFIED HAZARDS
Likelihoodor
Frequency
Consequence
Negligible Moderate High Catastrophic
High H2
Medium H1, H5 H6 H4
Low H3

(c) Felix Redmill, 2011 CERN, May '11 122
A RISK CLASS MATRIX(example only)
Likelihoodor
Frequency
Consequence
Negligible Moderate High Catastrophic
High C B A A
Medium D C B A
Low D D C B

(c) Felix Redmill, 2011 CERN, May '11 123
TOLERABILITY OF ANALYSED RISKS
• Refer the cell of each analysed hazard in the risk matrix to the equivalent cell in the risk class matrix to determine the class of the analysed risks
– So, Hazard 1 poses a D Class risk, Hazard 2 a B, etc.
• Risk class
– Defines the (relative) importance of risk reduction
– Provides a means of prioritising the handling of risks
– Can be equated to a defined type of action
• Risk class gives no indication of time criticality
– This must be derived from an understanding of the risk
• What is done to manage risks depends on circumstances

(c) Felix Redmill, 2011 CERN, May '11 124
THOUOGHTS ON THE USE OF TECHNIQUES
• Techniques are intended to support what you have decided to do– They should not define what you do
• Each is useful on its own for a given purpose– Thorough analysis requires a combination of
techniques
• Risk analysis is not achieved in a single activity– It should be continuous throughout a system’s life
• Early analysis (PHA) is particularly effective• Techniques may be used to verify each other’s
results• And to expand on them and provide further detail

(c) Felix Redmill, 2011 CERN, May '11 125
IMPORTANCE OF EARLY ANALYSIS
• Too many causes to start with bottom-up analysis– Effort and financial cost would be too great– Would lead to over-engineering for small risks– Would miss too many important hazards
• Fault trees commence with accidents or hazards• Carry out Preliminary Hazard Analysis early in a
project
Root causes1000s
Hazards<100
Accidents<20
(c) Felix Redmill, 2011 CERN, May '11 126
PRELIMINARY HAZARD ANALYSIS
• At the ‘Objectives’ or early specification stage– Potential then for greatest safety effectiveness
• Take a ‘system’ perspective• Consider historic understanding of such systems• Address differences between this system and
historic systems (novel features)• Consider such matters as: boundaries, operational
intent, physical operational environment, assumptions
• Identify accident types, potential accident scope and consequences
• Identify system-level hazards• If a checklist is used, review it for obsolescence• Create a new checklist for future use

(c) Felix Redmill, 2011 CERN, May '11 127
HUMAN RELIABILITY ASSESSMENT
• Human components of systems are unreliable
• Hazards posed by them should be included in risk analysis
• Several Human Reliability Assessment (HRA) techniques have been developed for the purpose
– These will be covered later in the degree course

CERN, May '11 128
RISKS POSED BY HUMANS
• We need to
– Extend risk analysis to include HRA
– Pay more attention to ergonomic considerations in design
– Consider human cognition in interface design
– Produce guidelines on human factors in safety
• Safety is multi-dimensional, so take an interdisciplinary approach
– Include ergonomists and psychologists in development and operational teams
(c) Felix Redmill, 2011

CERN, May '11 129
RISKS POSED BY SENIOR MANAGERS
• Senior managers (should)
– Define safety policy
– Make strategic safety decisions
– Provide leadership in safety (or not)
– Define culture by design or by their behaviour
• They predispose an organisation to safety or accident
• Accident inquiry reports show that the contribution of senior management to accident causation is considerable
• Yet their contributions to risk are not included in risk analyses
• Risk analyses therefore tend to be optimistic
• Risk analyses need to include management failure
• Management should pay attention to management failure
(c) Felix Redmill, 2011

CERN, May '11 130
RISK ANALYSIS SUMMARY
• Risk analysis is the cornerstone of modern safety engineering and management
• It can be considered as a four-staged process
• The first stage, hazard identification, is the basis of all further work - risks not identified are not analysed or mitigated
• All four stages include considerable subjectivity
• Subjectivity, in the form of human creativity and judgement, is essential to the effectiveness of the process
• Subjectivity also introduces bias and error
• HRA techniques need to be included in risk analyses
• We need techniques to include management risks
• Often the greatest value of risk analysis is having to do it
(c) Felix Redmill, 2011
(c) Felix Redmill, 2011 131
SAFETY INTEGRITY LEVELS(SILs)
CERN, May '11
(c) Felix Redmill, 2011 132
SAFETY AS A WAY OF THINKING
• Reliability is not a guarantee of safety• If risk is too great, it must be reduced
(the beginning of 'safety thinking')• But how do we know if the risk is too great?
– Carry out risk analysis
(safety engineering enters software and systems engineering)
• But even if the risk is high, does it need to be reduced?– Determine what level of risk is tolerable
(this introduces the concept of safety management)
CERN, May '11

(c) Felix Redmill, 2011 133
SAFETY INTEGRITY
• If risk is not tolerable it must be reduced• High-level requirement of safety function is 'to
reduce the risk'• Analysis leads to the functional requirements• The safety function becomes part of the overall
system– Safety depends on it
• So, will it reduce the risk to (at least) a tolerable level?
• We try to ensure that it does by defining the reliability with which it performs its safety function– In IEC 61508 in terms of Pr. of dangerous failure
• This is referred to as 'safety integrity'
CERN, May '11
(c) Felix Redmill, 2011 134
SAFETY INTEGRITY IS A TARGET REQUIREMENT
• Safety integrity sets a target for the maximum tolerable rate of dangerous failures of a safety function
– (This is a ‘reliability-type’ attribute)
• Example: S should not fail dangerously more than once in 7 years
• Example: There should be no more than 1 dangerous failure in 1000 demands
• If the rate of dangerous failures of the safety function can be measured accurately, achievement of the defined safety integrity may be claimed
CERN, May '11

(c) Felix Redmill, 2011 135
WHY SAFETY INTEGRITY LEVELS?
• A safety integrity target could have an infinite number of values
• It is practical to divide the total possible range into bands (categories)
• The bands are 'safety integrity levels' (SILs)– In IEC 61508 there are four
• N.B. Interesting that the starting point was that
safety and reliability are not synonymous
and the end point is the reliance of safety
on a reliability-type measure (rate of dangerous failure)
CERN, May '11
(c) Felix Redmill, 2011 136
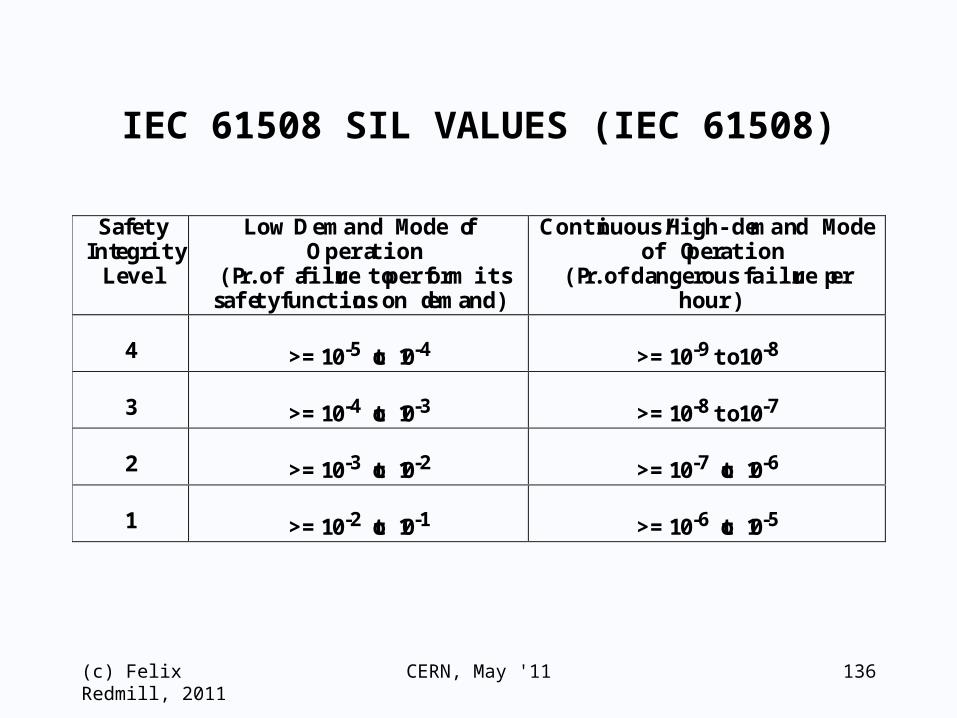
IEC 61508 SIL VALUES (IEC 61508)
SafetyIntegrity
Level
Low Demand Mode ofOperation
(Pr. of failure to perform itssafety functions on demand)
Continuous/High-demand Modeof Operation
(Pr. of dangerous failure perhour)
4 >= 10-5 to 10-4 >= 10-9 to 10-8
3 >= 10-4 to 10-3 >= 10-8 to 10-7
2 >= 10-3 to 10-2 >= 10-7 to 10-6
1 >= 10-2 to 10-1 >= 10-6 to 10-5
CERN, May '11

(c) Felix Redmill, 2011 137
RELATIONSHIP (IN IEC 61508) BETWEEN
LOW-DEMAND AND CONTINUOUS MODES
• Low-demand mode:'Frequency of demands ... no greater than one per year'
• 1 year = 8760 hours (approx. 104)
• Continuous and low-demand figures related by factor of 104
• Claims for a low-demand system must be justified
CERN, May '11

(c) Felix Redmill, 2011 138
APPLYING SAFETY INTEGRITY TO DEVELOPMENT PROCESS
• When product integrity cannot be measured with confidence (particularly when systematic failures dominate)
– The target is related, in IEC 61508, to the development process
• Processes are equated to safety-integrity levels
• But
– Such equations are judgemental
– Process may be an indicator of product, but not an infallible one
CERN, May '11

(c) Felix Redmill, 2011 139
IEC 61508 DEFINITIONS
• Safety integrity:
Probability of a safety-related system satisfactorily performing the required safety functions under all the stated conditions within a stated period of time
• Safety integrity level:
Discrete level (one out of a possible four) for specifying the safety integrity requirements of the safety functions to be allocated to the E/E/PE safety-related systems, where SIL 4 has the highest level of safety integrity and SIL 1 the lowest
CERN, May '11

(c) Felix Redmill, 2011 140
SIL IN TERMS OF RISK REDUCTION (IEC 61508)
EUC
risk
Increasing
risk
Necessary risk
reduction
Tolerable
risk
• The necessary risk reduction effected by a safety function
• Its functional requirements define what it should do• Its safety integrity requirements define its tolerable
rate of dangerous failure
CERN, May '11

(c) Felix Redmill, 2011 141
THE IEC 61508 MODEL OF RISK REDUCTION
EUC
Control
system
Protection
system
Safety functionsSafety functions
Utility + risks
CERN, May '11

(c) Felix Redmill, 2011 142
PRINCIPLE OF THE PROTECTION SYSTEM
Event frequency
10-7
EUC dangerous
failure frequency
10-3
Reliability of
safety function
10-4
10-4
10-3
AND
CERN, May '11

(c) Felix Redmill, 2011 143
BEWARE
• Note that a ‘protection system’ claim requires total independence of the safety function from the protected function
CERN, May '11

CERN, May '11 144
EACH HAZARD CARRIES A RISK
Tolerable level of risk 1
Risk1
Increasing riskNecessary reduction of risk 1Actual reduction of risk 1Residual
risk 1Tolerable
level of risk 2
Risk 2
(c) Felix Redmill, 2011
(c) Felix Redmill, 2011 145
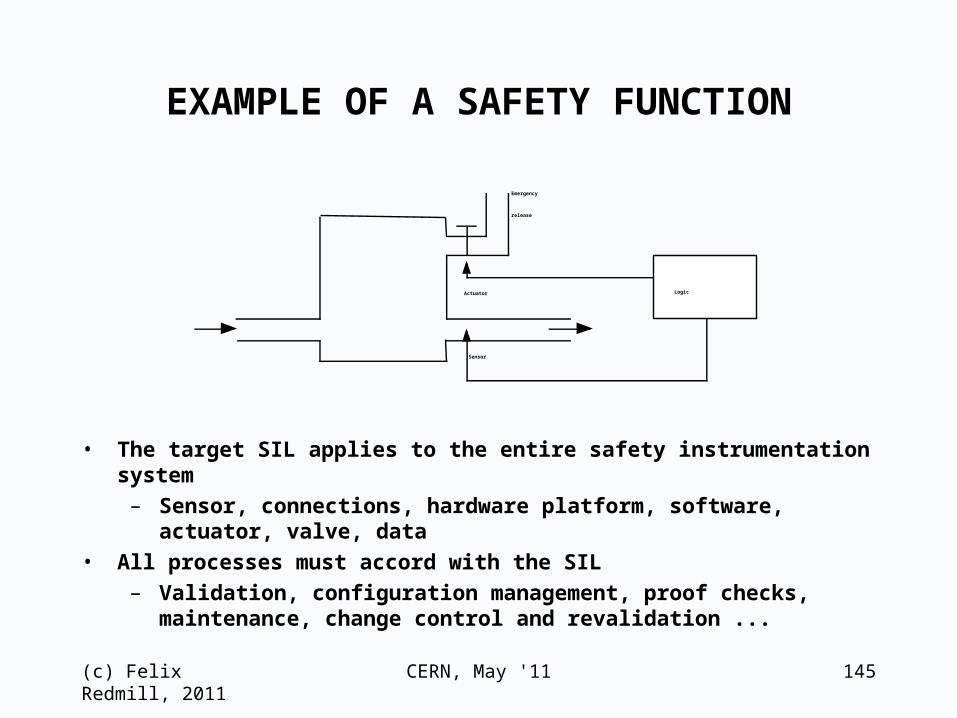
EXAMPLE OF A SAFETY FUNCTION
Logic
Sensor
Actuator
Emergency
release
• The target SIL applies to the entire safety instrumentation system– Sensor, connections, hardware platform, software,
actuator, valve, data• All processes must accord with the SIL
– Validation, configuration management, proof checks, maintenance, change control and revalidation ...
CERN, May '11
(c) Felix Redmill, 2011 146
PROCESS OF SIL DERIVATION
• Hazard identification• Hazard analysis• Risk assessment
– Resulting in requirements for risk reduction• Safety requirements specification
– Functional requirements– Safety integrity requirements
• Allocation of safety requirements to safety functions– Safety functions to be performed– Safety integrity requirements
• Allocation of safety functions to safety-related systems– Safety functions to be performed– Safety integrity requirements
CERN, May '11

(c) Felix Redmill, 2011 147
THE IEC 61508 SIL PRINCIPLE
Risk
assessment
S
I
L
Development
process
Necessary
risk
reduction
CERN, May '11

(c) Felix Redmill, 2011 148
BUT NOTE
• IEC 61508 emphasises process evidence but does not exclude the need for product or analysis evidence
• It is impossible for process evidence to be conclusive
• It is unlikely that conclusive evidence can be derived for complex systems in which systematic failures dominate
• Evidence of all types should be sought and assembled
CERN, May '11
(c) Felix Redmill, 2011 149
SIL ALLOCATION - 1 (from IEC 61508)
• Functions within a system may be allocated different SILs
• The required SIL of hardware is that of the software safety function with the highest SIL
• For a safety-related system that implements safety functions of different SILs, the hardware and all the software shall be of the highest SIL unless it can be shown that the implementations of the safety functions of the different SILs are sufficiently independent
• Where software is to implement safety functions of different SILs, all the software shall be of the highest SIL unless the different safety functions can be shown to be independent
CERN, May '11

(c) Felix Redmill, 2011 150
SIL ALLOCATION - 2(from IEC 61508)
• Where a safety-related system is to implement both safety and non-safety functions, all the hardware and software shall be treated as safety-related unless it can be shown that the implementation of the safety and non-safety functions is sufficiently independent (i.e. that the failure of any non-safety-related functions does not affect the safety-related functions). Wherever practicable, the safety-related functions should be separated from the non-safety-related functions
CERN, May '11
(c) Felix Redmill, 2011 151
SIL — ACHIEVED OR TARGET RELIABILITY?
• SIL is initially a statement of target rate of dangerous failures
• There may be reasonable confidence that achieved reliability = or > target reliability (that the SIL has been met), when– Simple design– Simple hardware components with known fault
histories in same or similar applications– Random failures
• But there is no confidence that the target SIL is met when– There is no fault history– Systematic failures dominate
• Then, IEC 61508 focuses on the development process
CERN, May '11

(c) Felix Redmill, 2011 152
APPLICATION OF SIL PRINCIPLE
• IEC 61508 is a meta standard, to be used as the basis for sector-specific standards
• The SIL principle may be adapted to suit the particular conditions of the sector
• An example is the application of the principle in
the Motor Industry guideline
CERN, May '11

(c) Felix Redmill, 2011 153
EXAMPLE OF SIL BASED ON CONSEQUENCE
(Motor Industry)• In the Motor Industry Software Reliability Association
(MISRA) guidelines (1994), the allocation of a SIL is determined by 'the ability of the vehicle occupants … to control the situation following a failure'
• Steps in determining an integrity level:
a) List all hazards that result from all failures of the system
b) Assess each failure mode to determine its controllability category
c)The failure mode with the highest associated controllability category determines the integrity level of the system
CERN, May '11

(c) Felix Redmill, 2011 154
MOTOR INDUSTRY EXAMPLE
Controllability category
Acceptable failure rate Integrity level
Uncontrollable Extremely improbable 4
Difficult to control
Very remote 3
Debilitating Remote 2
Distracting Unlikely 1
Nuisance only Reasonably possible 0
CERN, May '11

(c) Felix Redmill, 2011 155
SIL CAN BE MISLEADING
• Different standards derive SILs differently• SIL is not a synonym for overall reliability
– Could lead to over-engineering and greater costs• When SIL claim is based only on development process
– What were competence, QA, safety assessment, etc.?• Glib use of the term ‘SIL’
– No certainty of what is meant– Is the claim understood by those making it?– Be suspicious until examining the evidence
• SIL X may be intended to imply use in all circumstances– But safety is context-specific
• SIL says nothing about required attributes of the system– Must go back to the specification to identify them
CERN, May '11

(c) Felix Redmill, 2011 156
THREE QUESTIONS
• Does good process necessarily lead to good product?
• Instead of using a safety function, why not simply improve the basic system (EUC)?
• Can the SIL concept be applied to the basic system?
CERN, May '11

(c) Felix Redmill, 2011 157
DOES GOOD PROCESS LEAD TO GOOD PRODUCT?
• Adhering to “good” process does not guarantee reliability
– Link between process and product is not definitive
• Using a process is only a start
– Quality, and safety, come from professionalism
• Not only development processes, but also operation, maintenance, management, supervision, etc., throughout the life cycle
• Not only must development be rigorous but also the safety requirements must be correct
– And requirements engineering is notoriously difficult
• Meeting process requirements offers confidence, not proof
CERN, May '11

(c) Felix Redmill, 2011 158
WHY NOT SIMPLY IMPROVE THE BASIC SYSTEM?
• IEC 61508 bases safety on the addition of safety functions
• This assumes that EUC + control system are fixed
• Why not reduce risk by making EUC & control system safer?
• This is an iterative process
– Then, if all risks are tolerable no safety functions required
– But (according to IEC 61508) claim cannot be lower than 10-5 dangerous failures/hour (SIL 1)
• If there comes a time when we can't (technological) or won't (cost) improve further
– We must add safety functions if all risks are not tolerable
• We are then back to the standard as it is
CERN, May '11

(c) Felix Redmill, 2011 159
CAN THE SIL CONCEPT BE APPLIED TO THE BASIC SYSTEM?
• Determine its tolerable rate of dangerous failure and translate this into a SIL (as in the MISRA guidelines)
• But note the limit on the claim that can be made (10-5 dangerous failures per hour) to satisfy IEC 61508
CERN, May '11

(c) Felix Redmill, 2011 160
DOES MEETING THE SIL GUARANTEE SAFETY?
• Derivation of a SIL is based on hazard and risk analyses
• Hazard and risk analyses are subjective processes
• If the derived risk value is an accurate representation of the risk AND the selected level of risk tolerability is not too high THEN meeting the SIL may offer a good chance of safety
• But these criteria may not hold
• Also, our belief that the SIL has been met may not be justified
CERN, May '11

(c) Felix Redmill, 2011 161
SIL SUMMARY
• The SIL concept specifies the tolerable rate of dangerous failures of a safety-related system– It defines a “safety-reliability” target
• Evidence of achievement comes from product and process– IEC 61508 SIL defines constraints on
development processes• Different standards use the concept differently
– SIL derivation may be sector-specific• It can be misleading in numerous ways• The SIL concept is a tool
– It should be used only with understanding and care
CERN, May '11







