Download - Professor Chris Denton - Emerging therapies
Christopher P. Denton PhD FRCP Professor of Experimental Rheumatology
Royal Free Hospital and UCL Medical School, London, UK
Emerging therapies for systemic sclerosis
Disclosures
Consultancy: Actelion, Pfizer, GSK, Sanofi Aventis, Boehringer Ingelheim,
Roche, CSL Behring, Genzyme, Inventiva
Research grant funding: Actelion, Novartis, CSL Behring
Clinical trial investigator and steering committee :
Pfizer, Actelion, Sanofi-Aventis, MedImmune, United Therapeutics, Novartis, Celgene, Bayer
Overview: emerging therapies • Scleroderma is now treatable
– Licensed therapies for 2 major vascular complica<ons PAH and DU
– Recommenda<ons and guidelines are important – Pathways to access treatments must be developed
• Immunosuppression is beneficial – benefit and risk need to be balanced
• Targeted approach to therapy is possible • Three recent clinical trials are encouraging
– Posi<ve trials inform about disease mechanism and underpin further advances in therapy
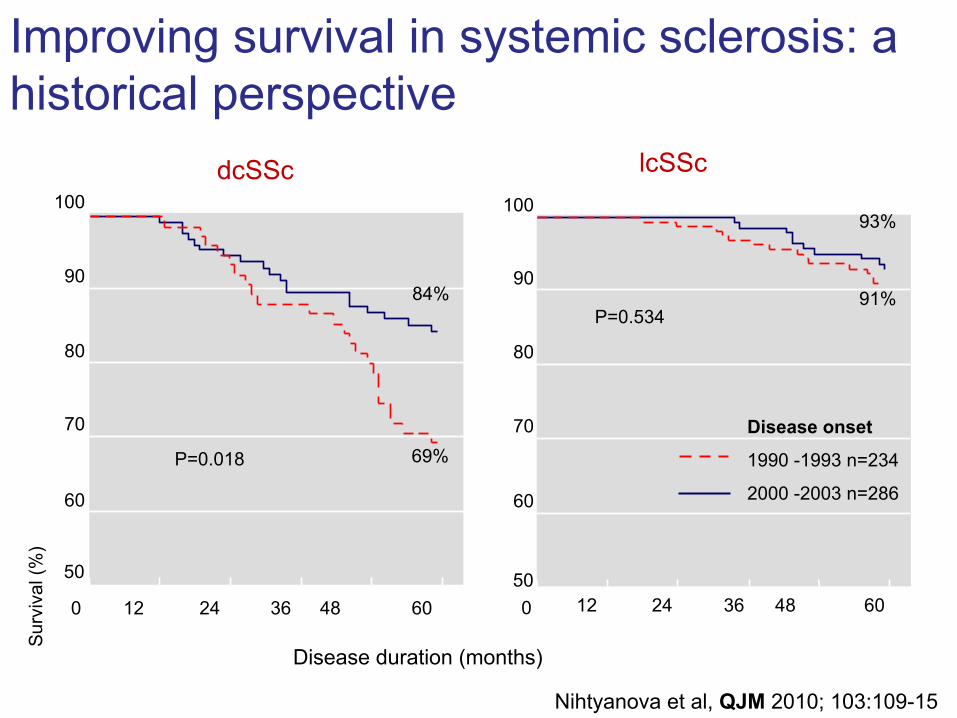
dcSSc lcSSc
0 12 24 36 48 60 50
60
70
80
90
100 93%
91% P=0.534
Disease duration (months)
Sur
viva
l (%
)
Disease onset
1990 -1993 n=234
2000 -2003 n=286
0 12 24 36 48 60
50
60
70
80
90
100
84%
69% P=0.018
Nihtyanova et al, QJM 2010; 103:109-15
Improving survival in systemic sclerosis: a historical perspective
EULAR/EUSTAR recommenda<ons for the treatment of systemic sclerosis
I SSc-‐related digital vasculopathy (RP, digital ulcers) 1. Calcium channel blockers and iloprost for Raynaud’s 2. Intravenous prostanoids (in par<cular iloprost) should be considered for treatment of digital ulcers in SSc 3. Bosentan should be considered in SSc with mul<ple digital ulcers
II SSc-‐PAH 4. Bosentan should be strongly considered to treat SSc-‐PAH 5. Sildenafil may be considered to treat SSc-‐PAH 6. Sitaxentan is withdrawn and should not be used for SSc-‐PAH 7. Intravenous epoprostenol should be considered for the treatment of severe SSc-‐PAH
III SSc-‐related skin involvement 8. Methotrexate may be considered for treatment of skin manifesta<ons of early diffuse SSc
IV SSc-‐ILD 9. Cyclophosphamide should be considered for treatment of SSc-‐ILD
V SRC 10. ACE inhibitors should be used in the treatment of SRC 11. Pa<ents on steroids should be carefully monitored for SRC
VI SSc-‐related gastrointes<nal disease 12. PPI should be used for the treatment of SSc-‐related gastro-‐oesophageal reflux, 13. Prokine<c drugs should be used for the management of SSc-‐related symptoma<c mo<lity disturbances 14. When malabsorp<on is caused by bacterial overgrowth, an<bio<cs may be useful in SSc
Kowal-‐Bielecka et al, Ann Rheum Dis 2009;68:620-‐628
• Best prac<ce documents available on UKSSG page of the Scleroderma-‐Royal Free website
• Stand-‐alone publica<ons are emerging – GI – published – excellent North American feedback – Digital vasculopathy – in press – Lung fibrosis – for submission – Cardiac – in prepara<on – Renal – in drag form
UKSSG Best prac<ce project (2011-‐14)
h,p://www.scleroderma-‐royalfree.org.uk/UKSSG.html
• Work started September 2012 • February 2015 -‐ submihed to BSR and first stage of external peer review – presented drag April 2015
• Target for comple<on September 2015
• Scope and structure of drag guideline A. General approach to SSc management B. Key therapies and treatment of organ based disease
C. Service organiza<on and delivery within NHS England
BSR and BHPR guideline for the management of systemic sclerosis
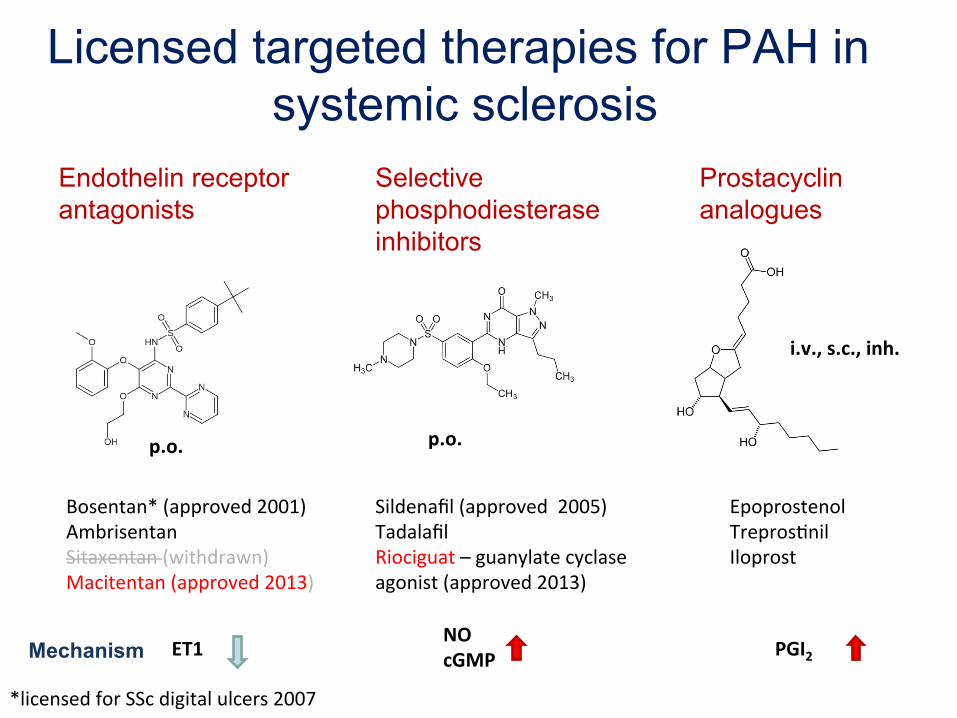
Licensed targeted therapies for PAH in systemic sclerosis
Endothelin receptor antagonists
Selective phosphodiesterase inhibitors
Prostacyclin analogues
Bosentan* (approved 2001) Ambrisentan Sitaxentan (withdrawn) Macitentan (approved 2013)
Sildenafil (approved 2005) Tadalafil Riociguat – guanylate cyclase agonist (approved 2013)
Epoprostenol Trepros<nil Iloprost
ET1 NO cGMP PGI2 Mechanism
p.o. p.o.
i.v., s.c., inh.
*licensed for SSc digital ulcers 2007
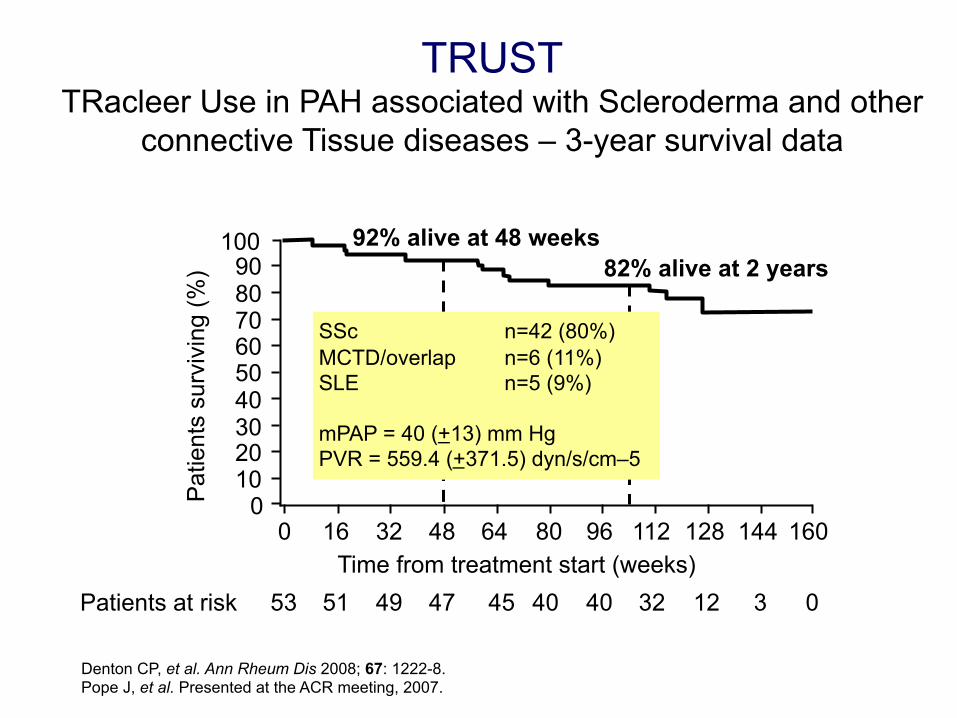
Denton CP, et al. Ann Rheum Dis 2008; 67: 1222-8. Pope J, et al. Presented at the ACR meeting, 2007.
100
80 90
70 60 50 40 30 20 10
0 Pat
ient
s su
rviv
ing
(%)
Time from treatment start (weeks) 0 16 32 48 64 80 96 112 128 144 160
Patients at risk 53 51 49 47 45 40 40 32 12 3 0
82% alive at 2 years 92% alive at 48 weeks
TRUST TRacleer Use in PAH associated with Scleroderma and other
connective Tissue diseases – 3-year survival data
SSc n=42 (80%) MCTD/overlap n=6 (11%) SLE n=5 (9%) mPAP = 40 (+13) mm Hg PVR = 559.4 (+371.5) dyn/s/cm–5
NHS England policy for DU in SSc* • Sildenafil • Prostenoids (iloprost) • Bosentan access for severe cases
– Severe refractory disease: persistent or progressive ulcera<on of one or more digits causing or threatening <ssue loss despite op<mal treatment with vasodilators including IV prostanoids and oral sildenafil, or
– Mul<ple DUs: 3 or more DUs either currently or occurring in the last 12 months despite IV prostanoids and sildenafil.
Challenging process (18 months) with reduced access during development compared with previous arrangements (IFR)
*First published: January 2015 Prepared by NHS England Specialised Services Clinical Reference Group for Specialised Rheumatology Published by NHS England, in electronic format only.
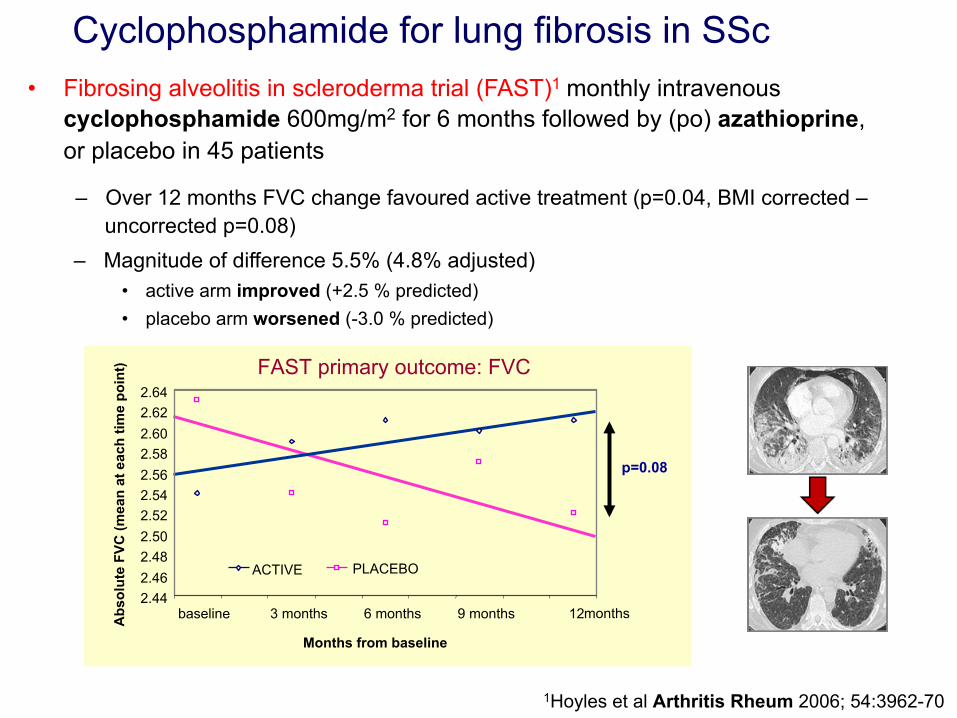
1Hoyles et al Arthritis Rheum 2006; 54:3962-70
Cyclophosphamide for lung fibrosis in SSc • Fibrosing alveolitis in scleroderma trial (FAST)1 monthly intravenous
cyclophosphamide 600mg/m2 for 6 months followed by (po) azathioprine, or placebo in 45 patients
– Over 12 months FVC change favoured active treatment (p=0.04, BMI corrected – uncorrected p=0.08)
FAST primary outcome: FVC
p=0.08
2.44 2.46 2.48 2.50 2.52 2.54 2.56 2.58 2.60 2.62 2.64
baseline 3 months 6 months 9 months 12 months
Months from baseline
Abs
olut
e FV
C (m
ean
at e
ach
time
poin
t)
ACTIVE PLACEBO
– Magnitude of difference 5.5% (4.8% adjusted) • active arm improved (+2.5 % predicted) • placebo arm worsened (-3.0 % predicted)
Agreed pathway for UK pa<ents to be evaluated for autologous stem cell transplanta<on
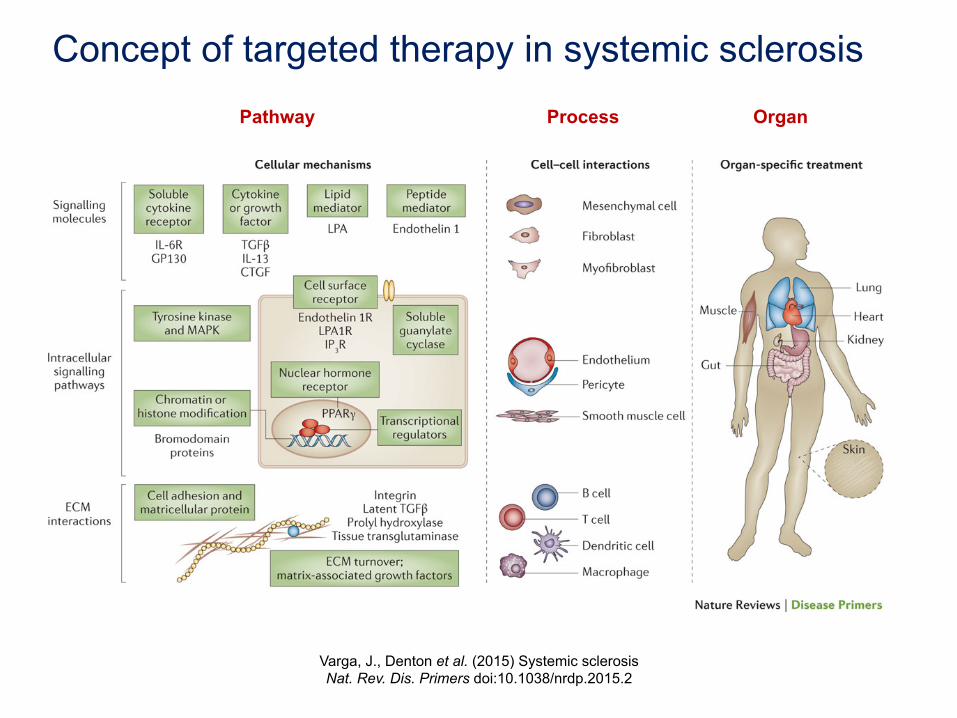
Concept of targeted therapy in systemic sclerosis
Varga, J., Denton et al. (2015) Systemic sclerosis Nat. Rev. Dis. Primers doi:10.1038/nrdp.2015.2
Pathway Process Organ
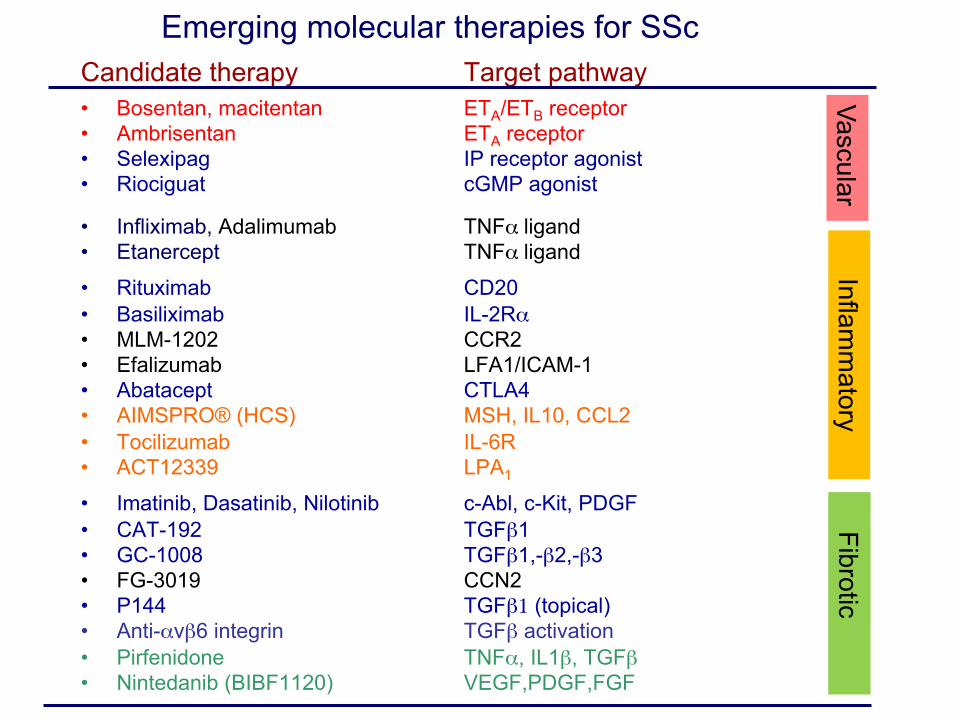
Emerging molecular therapies for SSc Candidate therapy Target pathway
• Bosentan, macitentan ETA/ETB receptor • Ambrisentan ETA receptor • Selexipag IP receptor agonist • Riociguat cGMP agonist
• Infliximab, Adalimumab TNFα ligand • Etanercept TNFα ligand
• Rituximab CD20 • Basiliximab IL-2Rα • MLM-1202 CCR2 • Efalizumab LFA1/ICAM-1 • Abatacept CTLA4 • AIMSPRO® (HCS) MSH, IL10, CCL2 • Tocilizumab IL-6R • ACT12339 LPA1
• Imatinib, Dasatinib, Nilotinib c-Abl, c-Kit, PDGF • CAT-192 TGFβ1 • GC-1008 TGFβ1,-β2,-β3 • FG-3019 CCN2 • P144 TGFβ1 (topical) • Anti-αvβ6 integrin TGFβ activation • Pirfenidone TNFα, IL1β, TGFβ • Nintedanib (BIBF1120) VEGF,PDGF,FGF
Vascular Inflam
matory
Fibrotic
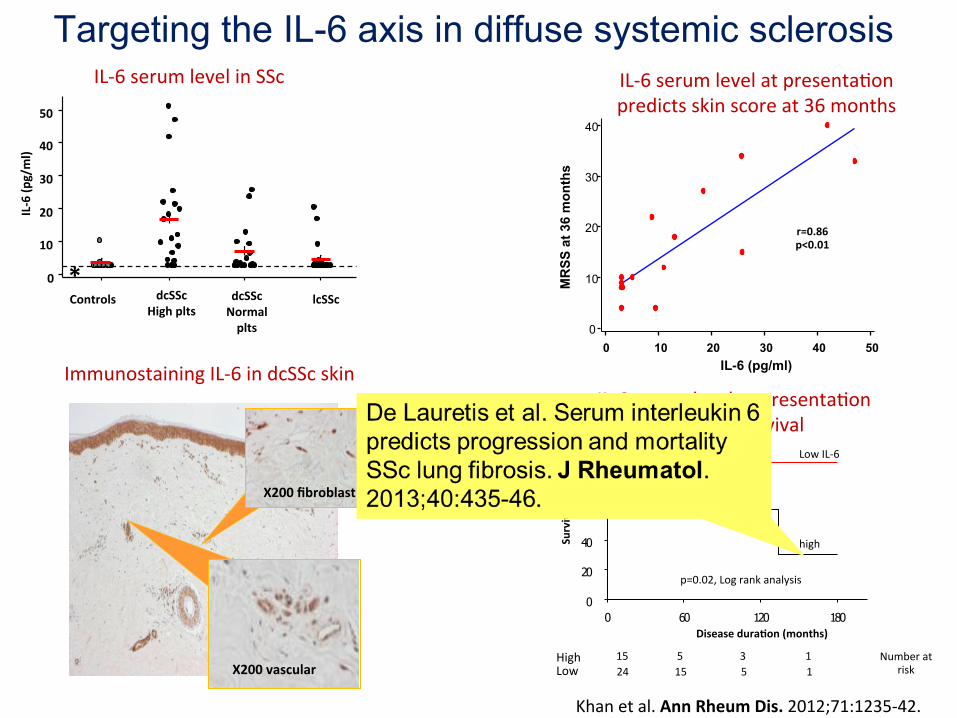
Targeting the IL-6 axis in diffuse systemic sclerosis
1 8 0 1 2 0 6 0 0
1 0 0
8 0
6 0
4 0
2 0
0
Disease duraNon (months)
Number at risk
High Low
15 5 3 1 24 15 5 1
IL-‐6 serum level at presenta<on predicts survival
Survival %
p=0.02, Log rank analysis
high
Low IL-‐6
Khan et al. Ann Rheum Dis. 2012;71:1235-‐42.
X200 vascular
Immunostaining IL-‐6 in dcSSc skin
X200 fibroblast
IL-‐6 (p
g/ml)
Controls
50
40
30
20
10
0 dcSSc
High plts dcSSc Normal plts
lcSSc *
IL-‐6 serum level in SSc
50 40 30 20 10 0
40
30
20
10
0
IL-6 (pg/ml)
MR
SS a
t 36
mon
ths
r=0.86 p<0.01
IL-‐6 serum level at presenta<on predicts skin score at 36 months
Conclusions • Treatment of scleroderma is improving • Established treatments are being used in beher ways e.g. immunosuppression
• Licensed drugs are available for specific complica<ons • Access to treatment requires co-‐ordinated and persistent efforts of medical teams, pa<ents and pa<ent organisa<ons
• Recent clinical suggest more targeted skin treatments are likely to emerge over the next few years
• New scleroderma lung fibrosis trials are being planned

Many thanks to …. • Our patients • The “Scleroderma team” at Royal Free • Research Funders • Colleagues in many institutions and organisations • UKSSG colleagues • International collaborators – EUSTAR, SCTC and FESCA, WSF
Arthritis Research UK, Raynaud’s and Scleroderma Association (UK), Wellcome Trust (UK), Nuffield Foundation, Scleroderma Society (UK), Rosetrees Trust, Scleroderma Research Foundation (USA), MRC, EULAR, Royal Free Charity







