
ORIGINAL ARTICLES
R1 Resection by Necessity for Colorectal Liver MetastasesIs It Still a Contraindication to Surgery?
Robbert J. de Haas, MD,*† Dennis A. Wicherts, MD,*† Eduardo Flores, MD,*Daniel Azoulay, MD, PhD,* Denis Castaing, MD,*‡§ and Rene Adam, MD, PhD*‡§
Objective: To compare long-term outcome of R0 (negative margins)and R1 (positive margins) liver resections for colorectal liver metastases(CLM) treated by an aggressive approach combining chemotherapy andrepeat surgery.Summary Background Data: Complete macroscopic resection withnegative margins is the gold standard recommendation in the surgicaltreatment of CLM. However, due to vascular proximity or multinodu-larity, complete macroscopic resection can sometimes only be per-formed through R1 resection. Increasingly efficient chemotherapy mayhave changed long-term outcome after R1 resection.Methods: All resected CLM patients (R0 or R1) at our institution between1990 and 2006 were prospectively evaluated. Exclusion criteria were:macroscopic incomplete (R2) resection, use of local treatment modalities,and presence of extrahepatic disease. We aimed to resect all identifiedmetastases with negative margins. However, when safe margins could notbe obtained, resection was still performed provided complete macroscopictumor removal. Overall survival (OS) and disease-free survival werecompared between groups, and prognostic factors were identified.Results: Of 840 patients, 436 (52%) were eligible for the study, 234(28%) of whom underwent R0 resection, and 202 (24%) underwent R1resection. Number and size of CLM were higher, and distribution wasmore often bilateral in the R1 group. After a mean follow-up of 40months, 5-year OS was 61% and 57% for R0 and R1 patients (P �0.27). Five-year disease-free survival was 29% in the R0 group versus20% in the R1 group (P � 0.12). In the R1 group, intrahepatic (but notsurgical margin) recurrences were more often observed (28% vs. 17%; P �0.004). Preoperative carcinoembryonic antigen level �10 ng/mL andmajor hepatectomy, but not R1 resection, were independent predictors ofpoor OS. Size �30 mm, bilateral distribution, and intraoperative bloodtransfusions independently predicted positive surgical margins.Conclusions: Despite a higher recurrence rate, the contraindicationof R1 resection should be revisited in the current era of effectivechemotherapy because survival is similar to that of R0 resection.
(Ann Surg 2008;248: 626–637)
Liver resection is still the only chance of cure for patientswith colorectal metastases, resulting in 5-year survival rates up
to 67% for highly selected patients.1 Unfortunately, at the time ofdiagnosis, only one-fifth of patients with colorectal liver metastases(CLM) presents with resectable lesions.2 Nowadays, an importantamount of patients initially considered as having unresectable CLMcan be converted to resectability by the aid of modern chemother-apy regimens consisting of 5-fluorouracil, leucovorin, oxaliplatin,and/or irinotecan.3–6 In addition, chemotherapy efficacy can befurther increased by the use of monoclonal antibodies like cetux-imab and bevacizumab.7–9 Besides this, surgical improvements likeportal vein embolization, which allows hypertrophy of a smallremnant liver volume, and vascular resection and reconstructiontechniques enable hepatic resection in an additional number ofpatients.10,11 However, due to the increased number of patients withmultinodular disease and/or CLM close to important vascular struc-tures, macroscopic complete resection of all CLM can sometimesonly be performed with positive surgical margins.
Within the literature, the inability to achieve clearresection margins is generally considered as contraindicationto surgery because it has been associated with significantlyreduced survival rates,12–20 and an increased risk of surgicalmargin recurrence.16,21 Several cutoff points for the optimalnegative resection margin width have been proposed, varyingbetween 2 and 10 mm;22–28 however, complete macroscopicremoval of all lesions with negative resection margins, irre-spective of the width, is currently the gold standard recom-mendation in the surgical treatment of CLM.
At our institute, the inability to obtain a free surgicalmargin during liver resection for CLM has never been con-sidered a contraindication to surgery, provided completemacroscopic removal of all metastatic lesions. As increas-ingly effective chemotherapy regimens might have changedthe spectrum of this particular situation, we compared long-term outcome in patients with microscopically positive andnegative resection margins who were all treated by an ag-gressive approach consisting of chemotherapy and repeatsurgery to assess the validity of this policy.
METHODS
Study PopulationAll consecutive patients treated by hepatic resection for CLM
at our hospital between January 1990 and January 2006, and whofulfilled the following criteria were eligible for the study: (1)macroscopic complete resection; (2) clear description of surgical
From the *AP-HP Hopital Paul Brousse, Centre Hepato-Biliaire, Villejuif,France; †Department of Surgery, University Medical Center Utrecht,Utrecht, The Netherlands; ‡Universite Paris-Sud, Villejuif, France; andthe §Inserm, Villejuif, France.
Reprints: Rene Adam, MD, PhD, AP-HP Hopital Paul Brousse, CentreHepato-Biliaire, 12 Avenue Paul Vaillant Couturier, 94804 Villejuif,France. E-mail: [email protected].
Copyright © 2008 by Lippincott Williams & WilkinsISSN: 0003-4932/08/24804-0626DOI: 10.1097/SLA.0b013e31818a07f1
Annals of Surgery • Volume 248, Number 4, October 2008626

margin status by the pathologist for each metastasis; (3) no evidenceof concomitant extrahepatic disease; (4) no simultaneous use oflocal treatment modalities (ie, radiofrequency ablation and/or cryo-surgery). Patients were selected from our prospectively maintainedinstitutional database, and each medical chart was reviewed.
Preoperative EvaluationAll patients were preoperatively evaluated by thoracoab-
dominal imaging (ultrasonography, computed tomography (CT)),routine blood tests, serum tumor marker levels (carcinoembryonicantigen (CEA) and/or CA19.9), and colonoscopy. Preoperativechemotherapy was administered when liver metastases were ini-tially unresectable (ie, inability to completely remove all CLM witha sufficient remnant liver volume), or in a neoadjuvant setting incase of synchronous (diagnosed before, during, or within 3 monthsafter colorectal resection) or in case of marginally resectable (�5bilateral nodules) CLM. Chemotherapy response was monitoredevery 2 months by CT imaging, according to the World HealthOrganization guidelines29 or, more recently, by using theResponse Evaluation Criteria in Solid Tumors (RECIST).30 Ifthe estimated future remnant liver volume was still insuffi-cient after chemotherapy, portal vein embolization was per-formed to induce compensatory hypertrophy of the remainingliver.10
Hepatic ResectionDuring laparotomy, thorough abdominal exploration was
performed to rule out extrahepatic disease sites. Palpation of theliver and intraoperative ultrasound were carried out to confirm thenumber and size of the lesions, to define their relation with intra-hepatic vascular structures, and to search for occult CLM. Paren-chymal transection was performed using the ultrasonic dissector(Cavitron Ultrasonic Surgical Aspirator, Valleylab, Boulder, CO)and a fenestrated bipolar forceps. The goal of surgery was to resectall identified tumor deposits with a tumor-free margin. However,when a tumor-free resection margin could not be obtained, owing tovascular proximity or multinodularity, resection was still performedprovided that all metastatic lesions were macroscopically com-pletely removed. To prevent local recurrences in these cases, appli-cation of argon beam or bipolar coagulation was routinely per-formed on the cut section. Postoperatively, all resection specimenswere examined by conventional histopathological examination. Ac-
cording to the guidelines of the International Union Against Cancer,R0 and R1 resections were defined by the absence (tumor-freemargin �1 mm for all detected lesions) or presence (tumor-free margin 0 mm) of microscopic tumor invasion of the resectionmargins, respectively.31 In case of microscopic tumor invasion, theadditional opinion of the operating surgeon with regard to thecomplete macroscopic resection of all lesions, differentiated R1from R2 resections.
Postoperative Follow-UpRegular postoperative follow-up started at 1 month pos-
thepatectomy, and then every 4 months, consisting of routineblood tests, serum tumor marker evaluation (CEA and/orCA19.9), and hepatic ultrasound. Thoracoabdominal CT imag-ing was performed every 8 months. After hepatectomy, patientswere treated by systemic chemotherapy to decrease the recur-rence risk. If an intrahepatic and/or extrahepatic recurrenceoccurred, repeat surgery was performed if potentially curative.32
Statistical AnalysisTo assess the impact of R1 resections on long-term outcome,
patients were divided according to their surgical margin status intoa R0 group and a R1 group. �2 test was used to compare categoricaldata, and continuous data were compared using the independent-samples t test. Survival time was calculated from the date of hepaticresection until death or last follow-up. Progression-free survival(PFS) was defined as the time-interval between hepatectomy andfirst postoperative recurrence or death, whereas disease-free sur-vival (DFS) was defined as the time-interval between the hepatec-tomy and either the first recurrence that could not be curativelytreated (resection or ablation) or death. Survival curves were gen-erated by the Kaplan-Meier method, and were compared by thelog-rank test. To identify predictors of survival, univariate andmultivariate analyses were performed, using the log-rank test andthe Cox proportional hazard model, respectively. Furthermore, in-dependent predictors of R1 resection were identified at multivariateanalysis (logistic regression), including all factors most likely toinfluence surgical margin status with a P value �0.10 at univariateanalysis. Statistical significance was defined as P � 0.05. Allstatistical analyses were performed by using SPSS version 13.0(SPSS Inc., Chicago, IL).
FIGURE 1. Flowchart study population.
Annals of Surgery • Volume 248, Number 4, October 2008 R1 Liver Resection for Colorectal Metastases
© 2008 Lippincott Williams & Wilkins 627
RESULTS
PatientsBetween January 1990 and January 2006, 840 patients
underwent hepatic resection for CLM at our hospital, 436(52%) of whom fulfilled the inclusion criteria (Fig. 1). Fifty-seven patients (7%) were excluded because of a macroscopicincomplete (R2) liver resection, 128 patients (15%) because aclear description of the microscopic surgical margin statuswas not available for all metastases, 134 patients (16%)because of concomitant extrahepatic disease, and 85 patients(10%) because of a concomitant local treatment. Among the436 eligible patients, microscopic tumor invasion at patho-logic analysis was present in 202 patients (24%) (R1 group),whereas in 234 patients (28%) no viable tumor cells could beidentified at the resection margin (R0 group).
Patients in the R1 group presented with more extensiveliver disease, reflected by the higher number and larger sizeof metastases, which were more often bilaterally distributedand initially unresectable (Table 1).
Perioperative CharacteristicsIn both groups, the majority of patients were treated by
preoperative chemotherapy; however, significantly more patientsreceived preoperative chemotherapy in the R1 group (81% vs. 67%,
TABLE 1. Patient and Tumor Characteristics
VariableR0 GroupN � 234
R1 GroupN � 202 P
Patients
Mean age at HR,yr � SD
62 � 11 59 � 11 0.01
Male/female 140 (60%)/94 (40%) 118 (58%)/84 (42%) 0.77
Primary tumor
Colon/rectum 179 (77%)/55 (23%) 154 (76%)/48 (24%) 0.95
T-stage31 0.34
1/2 21 (12%) 21 (15%)
3/4 159 (88%) 116 (85%)
N-stage31 0.30
0 70 (38%) 45 (32%)
1/2 116 (62%) 95 (68%)
Liver metastases atdiagnosis
Synchronous* 107 (46%) 118 (58%) 0.008
No. CLM �0.001
1 116 (50%) 61 (32%)
2–3 82 (36%) 61 (32%)
�3 32 (14%) 69 (36%)
Mean maximumsize, mm � SD
39 � 29 56 � 32 �0.001
Bilateral 77 (33%) 118 (58%) �0.001
Mean CEA level,ng/mL � SD
91 � 299 253 � 624 0.003
Initialunresectability
72 (31%) 113 (56%) �0.001
*Synchronous indicates diagnosed before, during, or within 3 mo after colorectalresection.
HR indicates hepatic resection; SD, standard deviation; CLM, colorectal livermetastases; CEA, carcinoembryonic antigen.
TABLE 2. Hepatectomy Characteristics
VariableR0 GroupN � 234
R1 GroupN � 202 P
Preop. chemotherapy 157 (67%) 164 (81%) 0.001
Total No. lines 0.64
1 124 (79%) 126 (77%)
�1 33 (21%) 38 (23%)
Total No. cycles 0.04
�6 45 (31%) 33 (21%)
�6 99 (69%) 126 (79%)
Regimen last preop. line 0.40
5-FU LV 34 (22%) 26 (16%)
5-FU LV oxaliplatin 73 (47%) 82 (52%)
5-FU LV irinotecan 31 (20%) 28 (18%)
Other 16 (10%) 23 (14%)
Clinical response at CT scan 0.98
Response 84 (55%) 90 (55%)
Stabilization 56 (37%) 59 (36%)
Progression 13 (8%) 15 (9%)
Hepatectomy
Mean preop. CEA level,ng/mL � SD
60 � 286 116 � 421 0.15
PVE 14 (6%) 30 (15%) 0.002
Major hepatectomy (�3 segments) 96 (41%) 115 (57%) 0.001
Mean intraop. No. CLM � SD 2 � 2 4 � 3 �0.001
Resection type �0.001
Anatomical 112 (48%) 85 (42%)
Nonanatomical 57 (24%) 26 (13%)
Both 65 (28%) 91 (45%)
Vascular proximity of CLM 79 (35%) 102 (51%) �0.001
Vascular occlusion 0.001
None 46 (20%) 17 (9%)
Selective inflow 44 (19%) 26 (14%)
Total pedicular 111 (48%) 107 (56%)
Total vascular 29 (13%) 41 (22%)
Mean RBC transfusions, units � SD 1 � 3 2 � 4 �0.001
Histopathology
Mean No. CLM � SD 2 � 2 4 � 3 �0.001
Mean maximum size of CLM � SD 34 � 27 54 � 41 �0.001
Postop. outcome
Postop. mortality (�2 mo) 3 (1%) 1 (0.5%) 0.38
Postop. complications 75 (32%) 85 (42%) 0.03
Hepatic35* 49 (21%) 70 (35%) 0.001
Clavien grade I/II 36 (73%) 56 (80%) 0.40
Clavien grade III/IV 13 (27%) 14 (20%)
Clavien grade V 0 (0%) 0 (0%)
General35† 46 (20%) 41 (20%) 0.87
Clavien grade I/II 38 (83%) 29 (71%) 0.12
Clavien grade III/IV 5 (11%) 11 (27%)
Clavien grade V 3 (6%) 1 (2%)
Postop. chemotherapy 182 (78%) 178 (88%) 0.002
*As hepatic complications were considered biliary leak/bilioma, hemorrhage,infected collection, noninfected collection, and transient liver insufficiency.
†As general complications were considered: pulmonary, cardiovascular, urinarytract, infectious (other than local hepatic), and iatrogenic complications.
5-FU indicates 5-fluorouracil; LV, leucovorin; CT, computed tomography; CEA,carcinoembryonic antigen; SD, standard deviation; PVE, portal vein embolization;CLM, colorectal liver metastases; RBC, red blood cell.
de Haas et al Annals of Surgery • Volume 248, Number 4, October 2008
© 2008 Lippincott Williams & Wilkins628
P � 0.001; Table 2). Although the number of preoperative chemo-therapy lines was similar between both groups, a higher meannumber of preoperative cycles was administered within the R1group (9 � 6 cycles vs. 7 � 4 cycles, respectively; P � 0.004).
Preoperative portal vein embolization was more often neededto allow safe resection in patients in the R1 group (15% vs. 6%,P � 0.002), and significantly more patients within the R1 groupunderwent a major hepatectomy (defined as �3 segments33,34)(Table 2). Intraoperative ultrasound examination revealed in the R1group significantly more often metastases located close (�1.0 cm)to a large blood vessel (51% vs. 35%, P � 0.001). Furthermore, ahigher need of intraoperative vascular occlusion and red blood celltransfusion emerged in the R1 group.
In the R0 group, 3 patients (1%) died within 60 dayspostoperatively, compared with 1 postoperative death (0.5%) inthe R1 group (P � 0.38). Causes of death were ischemiccardiovascular accident (N � 1), aspiration pneumonia(N � 1), cardiac arrest of unknown cause (N � 1), and ischemiccolitis (N � 1). The postoperative complication rate was higherin the R1 group (42% vs. 32%, P � 0.03), more often related tohepatic causes (Table 2). However, severity of the complicationsaccording to the Clavien classification was equally distributedbetween both groups.35 Postoperatively, most patients receivedadjuvant chemotherapy, which was again more frequently ad-ministered in the R1 group (88% vs. 78%, P � 0.002).
Long-Term OutcomeMean follow-up for the entire study population was 40
months. At last follow-up, 75 patients (32%) in the R0 group haddied, and 159 (68%) were alive, of whom 93 (40%) weredisease-free (Table 3). Within the R1 group, 63 patients (31%)had died at last follow-up, and 139 (69%) were alive, 63 (31%)of whom were without evidence of disease recurrence.
Disease recurrence tended to occur more often in patientswho had undergone R1 resection. When subdivided according torecurrence location, significantly more intrahepatic recurrenceswere observed after R1 resections. However, the rate of recurrenceslocated at the surgical margin was similar between both groups(Table 3). Thirty-nine percent of the total study population devel-oped a recurrence within the first year after hepatic resection, afurther 19% had a first recurrence in the second year, and a further11% had a first recurrence in the next 2 to 5 years. A total of 182patients (42%) developed an intrahepatic recurrence, 99 (54%) ofwhom underwent repeat hepatectomy. An extrahepatic locateddisease recurrence was diagnosed in 234 patients (54%), 85 (36%)of whom were treated by repeat surgery.
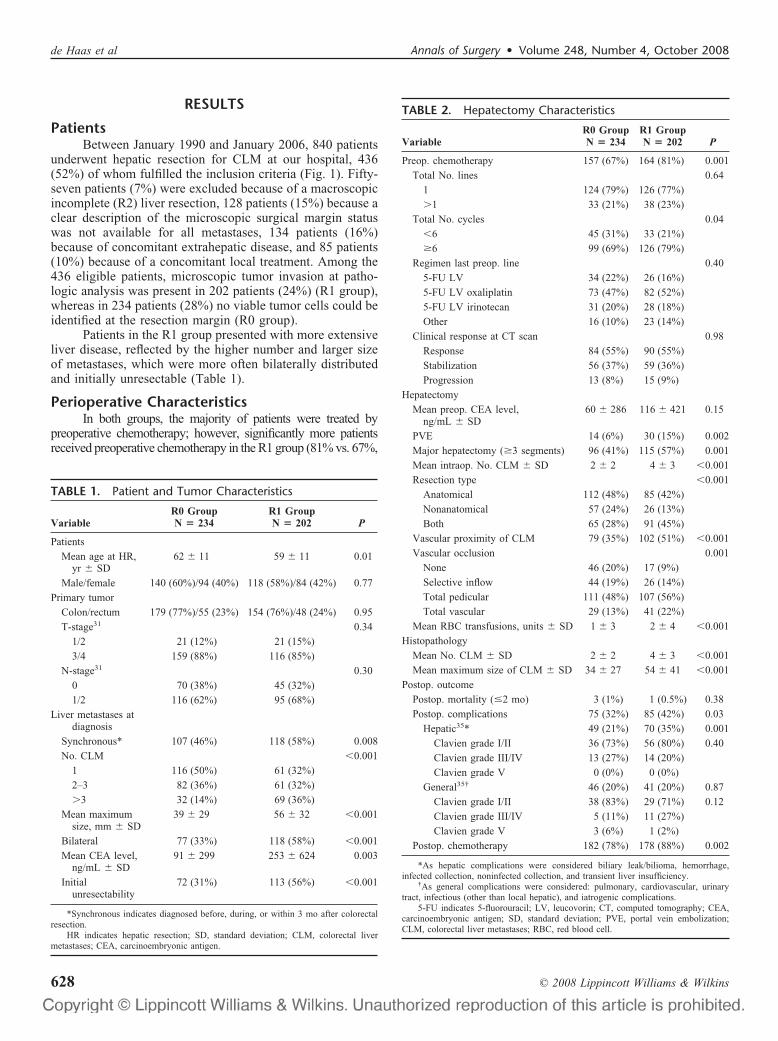
Five-year and 10-year overall survival (OS) rates were61% and 43% in the R0 group, versus 57% and 37% in the R1
TABLE 3. Long-Term Outcome
VariableR0 GroupN � 234
R1 GroupN � 202 P
Recurrence 153 (65%) 149 (74%) 0.06
Intrahepatic 26 (17%) 42 (28%) 0.004
Extrahepatic 74 (48%) 46 (31%)
Both 53 (35%) 61 (41%)
Location intrahepatic recurrence 0.72
Surgical margin 12 (15%)* 13 (12%)*
Elsewhere 59 (75%) 79 (75%)
Both 8 (10%) 14 (13%)
Repeat hepatectomy 53 (23%) 46 (23%) 0.98
Repeat EHD resection 56 (24%) 29 (14%) 0.01
Status at last follow-up 0.07
Alive without disease 93 (40%) 63 (31%)
Alive with disease 66 (28%) 76 (38%)
Dead 75 (32%) 63 (31%)
*Of all recurrences, 8% in the R0 group and 9% in the R1 group was located at thesurgical margin.
EHD indicates extrahepatic disease.
FIGURE 2. OS stratified according to surgical mar-gin status.
Annals of Surgery • Volume 248, Number 4, October 2008 R1 Liver Resection for Colorectal Metastases
© 2008 Lippincott Williams & Wilkins 629
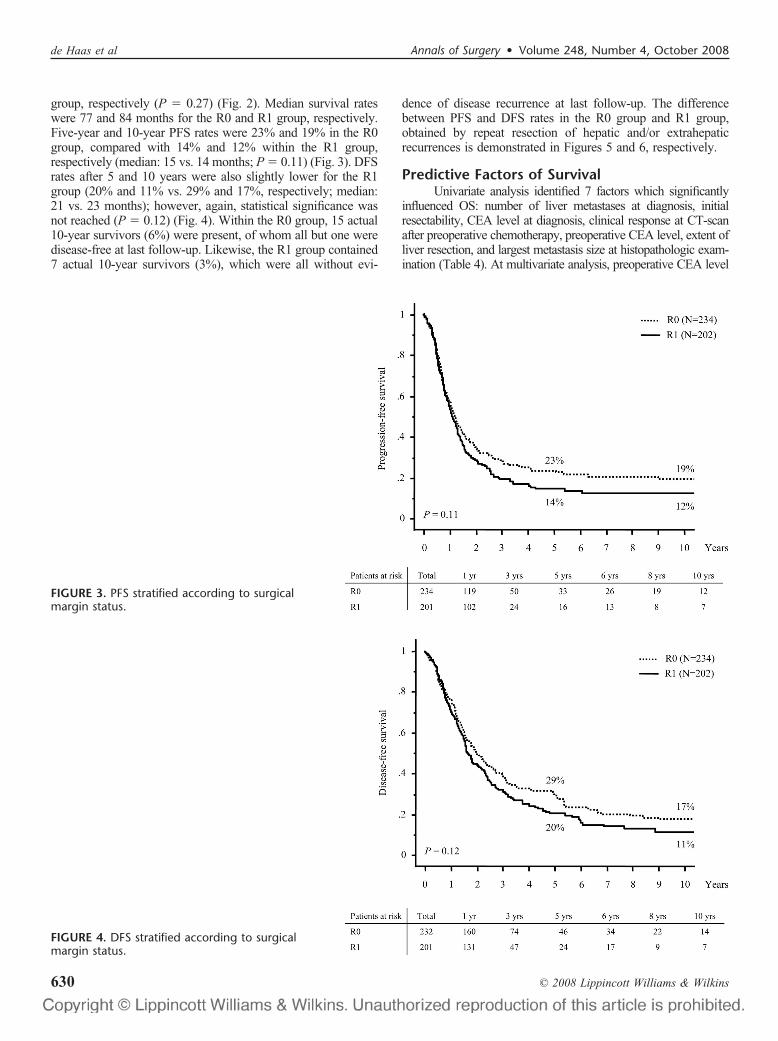
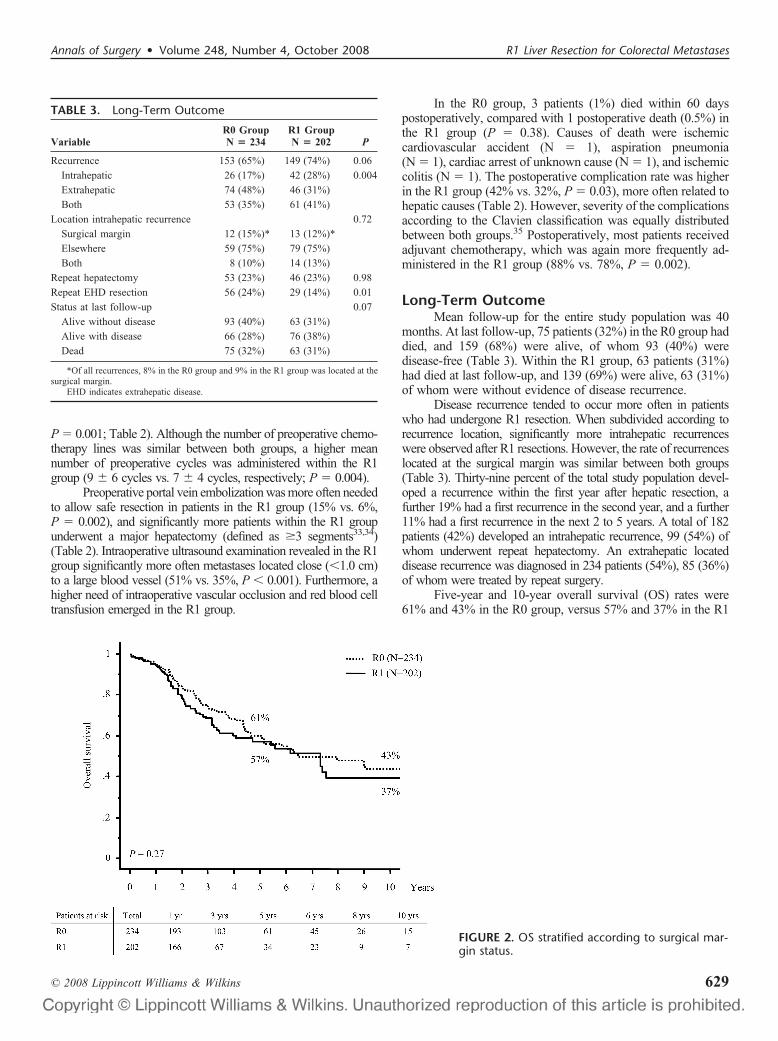
group, respectively (P � 0.27) (Fig. 2). Median survival rateswere 77 and 84 months for the R0 and R1 group, respectively.Five-year and 10-year PFS rates were 23% and 19% in the R0group, compared with 14% and 12% within the R1 group,respectively (median: 15 vs. 14 months; P � 0.11) (Fig. 3). DFSrates after 5 and 10 years were also slightly lower for the R1group (20% and 11% vs. 29% and 17%, respectively; median:21 vs. 23 months); however, again, statistical significance wasnot reached (P � 0.12) (Fig. 4). Within the R0 group, 15 actual10-year survivors (6%) were present, of whom all but one weredisease-free at last follow-up. Likewise, the R1 group contained7 actual 10-year survivors (3%), which were all without evi-
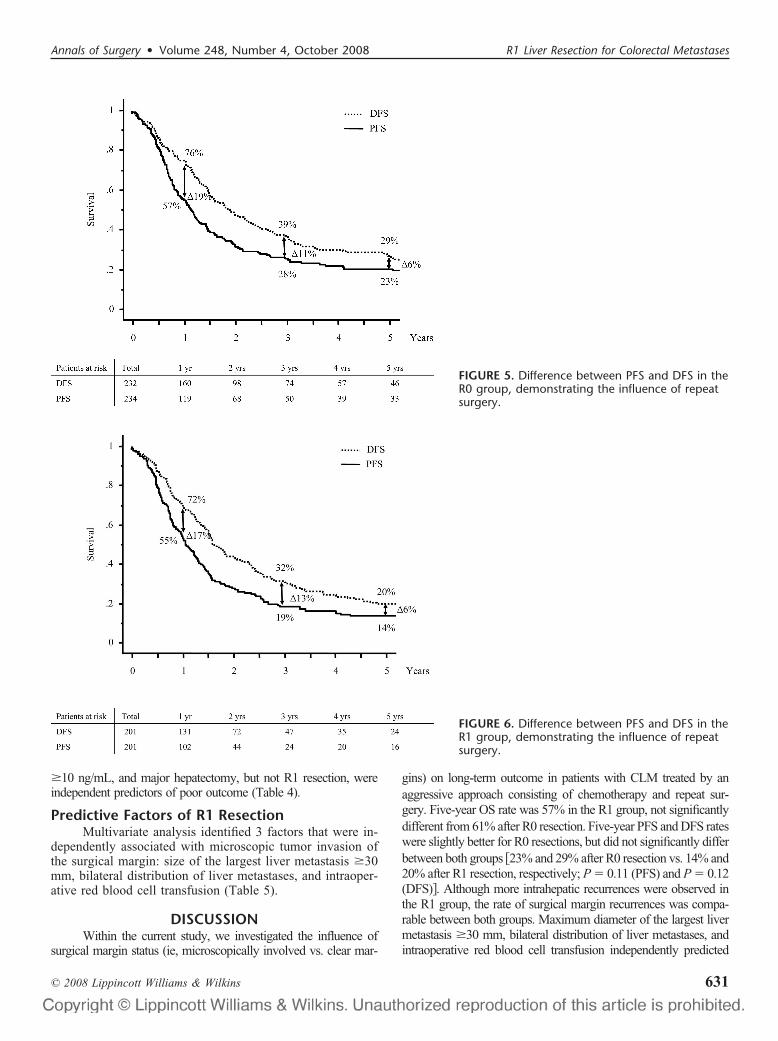
dence of disease recurrence at last follow-up. The differencebetween PFS and DFS rates in the R0 group and R1 group,obtained by repeat resection of hepatic and/or extrahepaticrecurrences is demonstrated in Figures 5 and 6, respectively.
Predictive Factors of SurvivalUnivariate analysis identified 7 factors which significantly
influenced OS: number of liver metastases at diagnosis, initialresectability, CEA level at diagnosis, clinical response at CT-scanafter preoperative chemotherapy, preoperative CEA level, extent ofliver resection, and largest metastasis size at histopathologic exam-ination (Table 4). At multivariate analysis, preoperative CEA level
FIGURE 3. PFS stratified according to surgicalmargin status.
FIGURE 4. DFS stratified according to surgicalmargin status.
de Haas et al Annals of Surgery • Volume 248, Number 4, October 2008
© 2008 Lippincott Williams & Wilkins630
�10 ng/mL, and major hepatectomy, but not R1 resection, wereindependent predictors of poor outcome (Table 4).
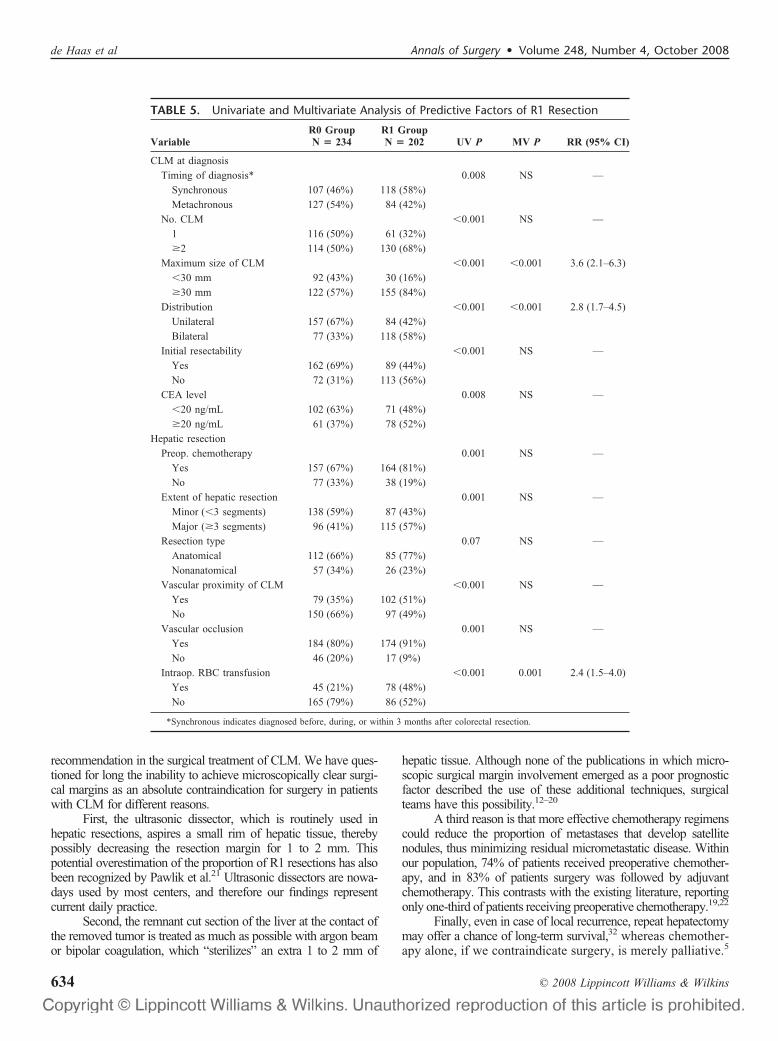
Predictive Factors of R1 ResectionMultivariate analysis identified 3 factors that were in-
dependently associated with microscopic tumor invasion ofthe surgical margin: size of the largest liver metastasis �30mm, bilateral distribution of liver metastases, and intraoper-ative red blood cell transfusion (Table 5).
DISCUSSIONWithin the current study, we investigated the influence of
surgical margin status (ie, microscopically involved vs. clear mar-
gins) on long-term outcome in patients with CLM treated by anaggressive approach consisting of chemotherapy and repeat sur-gery. Five-year OS rate was 57% in the R1 group, not significantlydifferent from 61% after R0 resection. Five-year PFS and DFS rateswere slightly better for R0 resections, but did not significantly differbetween both groups �23% and 29% after R0 resection vs. 14% and20% after R1 resection, respectively; P � 0.11 (PFS) and P � 0.12(DFS)�. Although more intrahepatic recurrences were observed inthe R1 group, the rate of surgical margin recurrences was compa-rable between both groups. Maximum diameter of the largest livermetastasis �30 mm, bilateral distribution of liver metastases, andintraoperative red blood cell transfusion independently predicted
FIGURE 5. Difference between PFS and DFS in theR0 group, demonstrating the influence of repeatsurgery.
FIGURE 6. Difference between PFS and DFS in theR1 group, demonstrating the influence of repeatsurgery.
Annals of Surgery • Volume 248, Number 4, October 2008 R1 Liver Resection for Colorectal Metastases
© 2008 Lippincott Williams & Wilkins 631
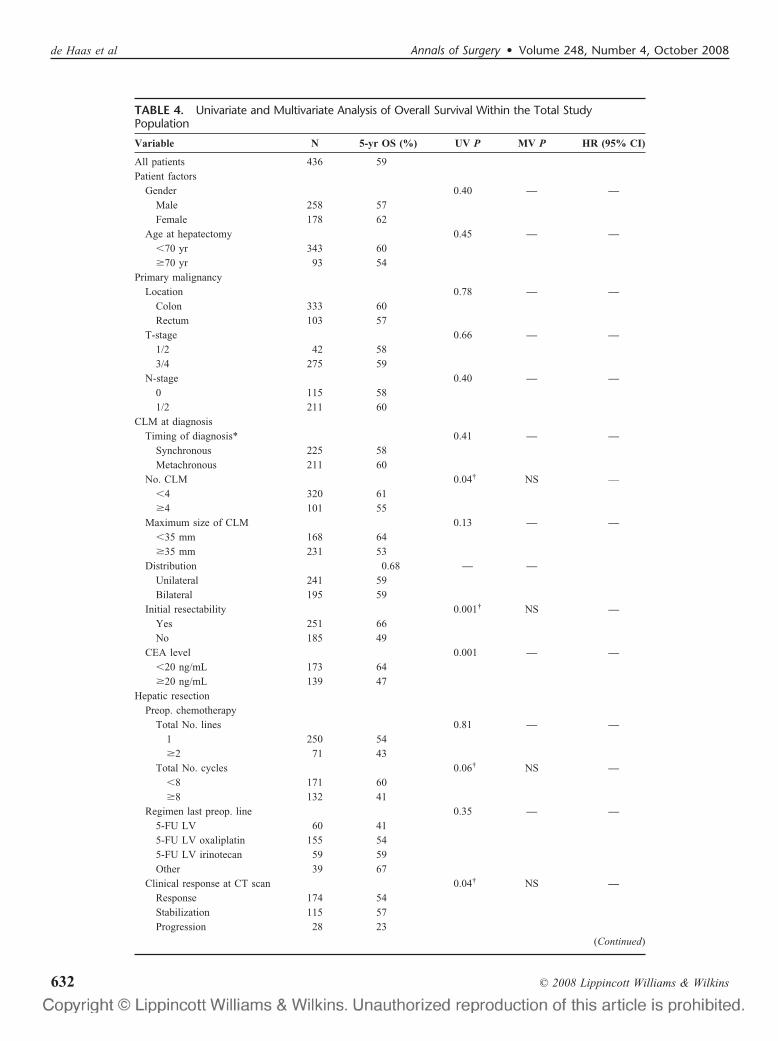
TABLE 4. Univariate and Multivariate Analysis of Overall Survival Within the Total StudyPopulation
Variable N 5-yr OS (%) UV P MV P HR (95% CI)
All patients 436 59Patient factors
Gender 0.40 — —Male 258 57Female 178 62
Age at hepatectomy 0.45 — —�70 yr 343 60�70 yr 93 54
Primary malignancyLocation 0.78 — —
Colon 333 60Rectum 103 57
T-stage 0.66 — —1/2 42 583/4 275 59
N-stage 0.40 — —0 115 581/2 211 60
CLM at diagnosisTiming of diagnosis* 0.41 — —
Synchronous 225 58Metachronous 211 60
No. CLM 0.04† NS —�4 320 61�4 101 55
Maximum size of CLM 0.13 — —�35 mm 168 64�35 mm 231 53
Distribution 0.68 — —Unilateral 241 59Bilateral 195 59
Initial resectability 0.001† NS —Yes 251 66No 185 49
CEA level 0.001 — —�20 ng/mL 173 64�20 ng/mL 139 47
Hepatic resectionPreop. chemotherapy
Total No. lines 0.81 — —1 250 54�2 71 43
Total No. cycles 0.06† NS —�8 171 60�8 132 41
Regimen last preop. line 0.35 — —5-FU LV 60 415-FU LV oxaliplatin 155 545-FU LV irinotecan 59 59Other 39 67
Clinical response at CT scan 0.04† NS —Response 174 54Stabilization 115 57Progression 28 23
(Continued)
de Haas et al Annals of Surgery • Volume 248, Number 4, October 2008
© 2008 Lippincott Williams & Wilkins632
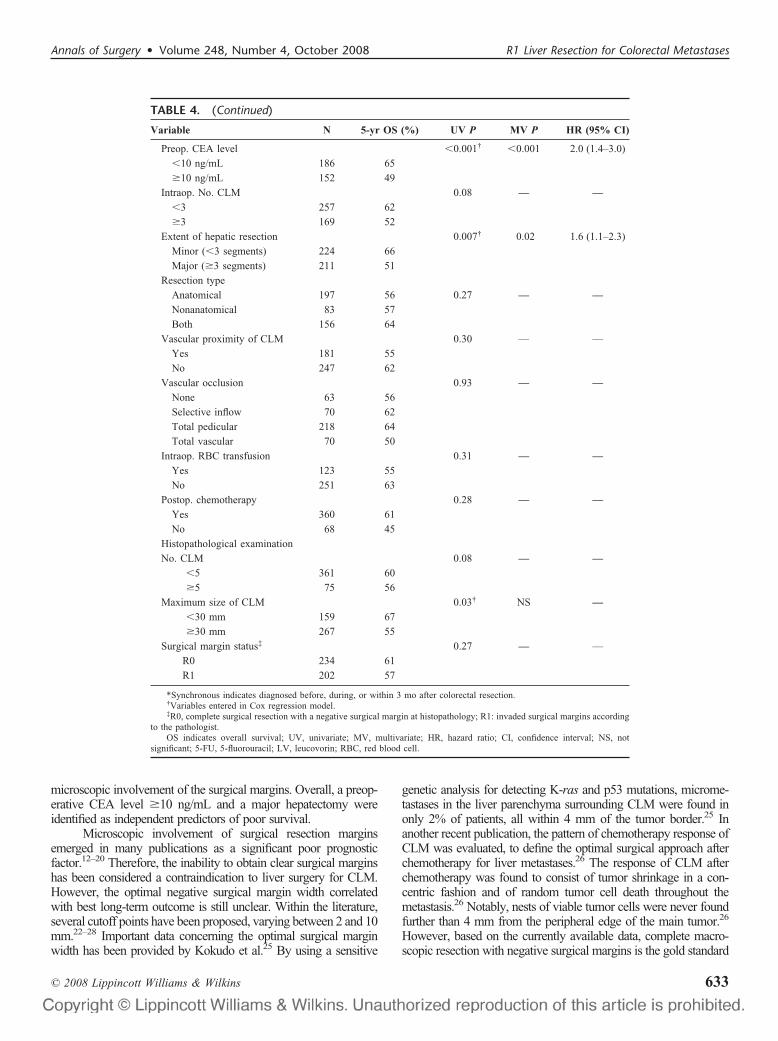
microscopic involvement of the surgical margins. Overall, a preop-erative CEA level �10 ng/mL and a major hepatectomy wereidentified as independent predictors of poor survival.
Microscopic involvement of surgical resection marginsemerged in many publications as a significant poor prognosticfactor.12–20 Therefore, the inability to obtain clear surgical marginshas been considered a contraindication to liver surgery for CLM.However, the optimal negative surgical margin width correlatedwith best long-term outcome is still unclear. Within the literature,several cutoff points have been proposed, varying between 2 and 10mm.22–28 Important data concerning the optimal surgical marginwidth has been provided by Kokudo et al.25 By using a sensitive
genetic analysis for detecting K-ras and p53 mutations, microme-tastases in the liver parenchyma surrounding CLM were found inonly 2% of patients, all within 4 mm of the tumor border.25 Inanother recent publication, the pattern of chemotherapy response ofCLM was evaluated, to define the optimal surgical approach afterchemotherapy for liver metastases.26 The response of CLM afterchemotherapy was found to consist of tumor shrinkage in a con-centric fashion and of random tumor cell death throughout themetastasis.26 Notably, nests of viable tumor cells were never foundfurther than 4 mm from the peripheral edge of the main tumor.26
However, based on the currently available data, complete macro-scopic resection with negative surgical margins is the gold standard
TABLE 4. (Continued)
Variable N 5-yr OS (%) UV P MV P HR (95% CI)
Preop. CEA level �0.001† �0.001 2.0 (1.4–3.0)
�10 ng/mL 186 65
�10 ng/mL 152 49
Intraop. No. CLM 0.08 — —�3 257 62
�3 169 52
Extent of hepatic resection 0.007† 0.02 1.6 (1.1–2.3)
Minor (�3 segments) 224 66
Major (�3 segments) 211 51
Resection type
Anatomical 197 56 0.27 — —Nonanatomical 83 57
Both 156 64
Vascular proximity of CLM 0.30 — —
Yes 181 55
No 247 62
Vascular occlusion 0.93 — —None 63 56
Selective inflow 70 62
Total pedicular 218 64
Total vascular 70 50
Intraop. RBC transfusion 0.31 — —Yes 123 55
No 251 63
Postop. chemotherapy 0.28 — —Yes 360 61
No 68 45
Histopathological examination
No. CLM 0.08 — —�5 361 60
�5 75 56
Maximum size of CLM 0.03† NS —�30 mm 159 67
�30 mm 267 55
Surgical margin status‡ 0.27 — —
R0 234 61
R1 202 57
*Synchronous indicates diagnosed before, during, or within 3 mo after colorectal resection.†Variables entered in Cox regression model.‡R0, complete surgical resection with a negative surgical margin at histopathology; R1: invaded surgical margins according
to the pathologist.OS indicates overall survival; UV, univariate; MV, multivariate; HR, hazard ratio; CI, confidence interval; NS, not
significant; 5-FU, 5-fluorouracil; LV, leucovorin; RBC, red blood cell.
Annals of Surgery • Volume 248, Number 4, October 2008 R1 Liver Resection for Colorectal Metastases
© 2008 Lippincott Williams & Wilkins 633
recommendation in the surgical treatment of CLM. We have ques-tioned for long the inability to achieve microscopically clear surgi-cal margins as an absolute contraindication for surgery in patientswith CLM for different reasons.
First, the ultrasonic dissector, which is routinely used inhepatic resections, aspires a small rim of hepatic tissue, therebypossibly decreasing the resection margin for 1 to 2 mm. Thispotential overestimation of the proportion of R1 resections has alsobeen recognized by Pawlik et al.21 Ultrasonic dissectors are nowa-days used by most centers, and therefore our findings representcurrent daily practice.
Second, the remnant cut section of the liver at the contact ofthe removed tumor is treated as much as possible with argon beamor bipolar coagulation, which “sterilizes” an extra 1 to 2 mm of
hepatic tissue. Although none of the publications in which micro-scopic surgical margin involvement emerged as a poor prognosticfactor described the use of these additional techniques, surgicalteams have this possibility.12–20
A third reason is that more effective chemotherapy regimenscould reduce the proportion of metastases that develop satellitenodules, thus minimizing residual micrometastatic disease. Withinour population, 74% of patients received preoperative chemother-apy, and in 83% of patients surgery was followed by adjuvantchemotherapy. This contrasts with the existing literature, reportingonly one-third of patients receiving preoperative chemotherapy.19,22
Finally, even in case of local recurrence, repeat hepatectomymay offer a chance of long-term survival,32 whereas chemother-apy alone, if we contraindicate surgery, is merely palliative.5
TABLE 5. Univariate and Multivariate Analysis of Predictive Factors of R1 Resection
VariableR0 GroupN � 234
R1 GroupN � 202 UV P MV P RR (95% CI)
CLM at diagnosis
Timing of diagnosis* 0.008 NS —
Synchronous 107 (46%) 118 (58%)
Metachronous 127 (54%) 84 (42%)
No. CLM �0.001 NS —
1 116 (50%) 61 (32%)
�2 114 (50%) 130 (68%)
Maximum size of CLM �0.001 �0.001 3.6 (2.1–6.3)
�30 mm 92 (43%) 30 (16%)
�30 mm 122 (57%) 155 (84%)
Distribution �0.001 �0.001 2.8 (1.7–4.5)
Unilateral 157 (67%) 84 (42%)
Bilateral 77 (33%) 118 (58%)
Initial resectability �0.001 NS —
Yes 162 (69%) 89 (44%)
No 72 (31%) 113 (56%)
CEA level 0.008 NS —
�20 ng/mL 102 (63%) 71 (48%)
�20 ng/mL 61 (37%) 78 (52%)
Hepatic resection
Preop. chemotherapy 0.001 NS —
Yes 157 (67%) 164 (81%)
No 77 (33%) 38 (19%)
Extent of hepatic resection 0.001 NS —
Minor (�3 segments) 138 (59%) 87 (43%)
Major (�3 segments) 96 (41%) 115 (57%)
Resection type 0.07 NS —
Anatomical 112 (66%) 85 (77%)
Nonanatomical 57 (34%) 26 (23%)
Vascular proximity of CLM �0.001 NS —
Yes 79 (35%) 102 (51%)
No 150 (66%) 97 (49%)
Vascular occlusion 0.001 NS —
Yes 184 (80%) 174 (91%)
No 46 (20%) 17 (9%)
Intraop. RBC transfusion �0.001 0.001 2.4 (1.5–4.0)
Yes 45 (21%) 78 (48%)
No 165 (79%) 86 (52%)
*Synchronous indicates diagnosed before, during, or within 3 months after colorectal resection.
de Haas et al Annals of Surgery • Volume 248, Number 4, October 2008
© 2008 Lippincott Williams & Wilkins634

The value of repeat (extra) hepatic surgery in our populationis clearly demonstrated by the difference between PFS andDFS (Figs. 5 and 6).
Accordingly, the results of our study demonstrate thatnot considering the inability to obtain microscopically clearsurgical margins as an absolute contraindication for surgeryhas been a reasonable treatment strategy. Importantly, byexcluding patients who underwent R2 resection, or withconcomitant local ablative techniques, and those presentingwith concomitant extrahepatic disease, the real impact ofsurgical margin status on survival could be identified.
In the recent multicenter study reported by Pawlik et al,21 apositive surgical margin was significantly associated with surgicalmargin recurrence. Similarly, Hamady et al observed a higherrecurrence rate located at the surgical margin in patients withpositive resection margins.16 Likewise, Choti et al identified micro-scopically positive resection margins as an independent factor pre-dicting worse DFS; however, recurrences were not stratified accord-ing to their location.12 In addition, Kokudo et al reported an increasein resection margin recurrences in patients with surgical marginsnarrower than 2 mm.25 In the present study, although more intra-hepatic recurrences were observed in patients with positive resec-tion margins, the rate of surgical margin recurrences and intrahe-patic recurrences away from the surgical margin were equallybalanced between the R0 group and the R1 group. This is inagreement with a recent publication by Bodingbauer et al, in whichit was demonstrated that surgical margin status was not associatedwith an increased hepatic recurrence risk, either at the surgicalmargin or elsewhere.36 Figueras et al also recently reported thatsubcentimeter nonpositive surgical margins did not influence he-patic recurrence rates after hepatectomy for CLM.37
That positive surgical margins expose to a higher recurrencerisk is obvious, but this should not be the only criterion considered.By stating R1 resection as a contraindication to surgery, whatshould be the alternative? Even with the increasingly efficientchemotherapy regimens, median survivals reach currently 20 to 24months.38,39 By combining liver resection (even R1), we quadruplethe survival expectancy, since median survival was in our study 88months after R1 resection. Therefore, no doubt is allowed, providedthat the resection is complete.
Our multivariate analysis demonstrated that an increasedpreoperative CEA level and the performance of a major hepa-tectomy independently predicted poor outcome. In several otherpublications, an increased preoperative CEA level also emergedas a predictor of worse long-term outcome.12,14,27 By contrast,major hepatectomy by itself is not a widely reported poorprognostic factor; however, it reflects the number, size, anddistribution of CLM, which are well known risk factors foradverse long-term outcome.14,40,41
Not surprisingly, size and distribution of CLM were identi-fied as risk factors for the inability to obtain microscopically tumor-free surgical margins, which reflect tumor load and thereby com-plexity of achieving a radical clearance. Are et al and Pawlik et al,both, recently reported similar predictors of surgical margin in-volvement.21,22 Interestingly, in the present study we identifiedthe need for red blood cell transfusion as a significant risk factorfor R1 resection. A possible explanation relies on the fact thatthe need for an intraoperative red blood cell transfusion reflects
a more complex operation with higher blood loss, in which it istechnically more difficult to obtain free surgical margins.
In conclusion, despite a higher intrahepatic recurrence rate,OS, PFS and DFS rates were almost similar for patients with R0and R1 resections for CLM, treated by an aggressive strategyconsisting of chemotherapy and surgery. As chemotherapy regi-mens are nowadays increasingly effective, the inability to obtainmicroscopically free surgical margins as a contraindication to he-patic resection for CLM, provided macroscopic complete removal,should be revisited. As a result, long-term outcome after R1 resec-tions should no longer be considered as poor as that observed afterR2 resections, but closer to that observed after R0 resections. Theabsolute contraindication to hepatic resection for CLM shouldtherefore not include R1 resection anymore.
REFERENCES1. Simmonds PC, Primrose JN, Colquitt JL, et al. Surgical resection of
hepatic metastases from colorectal cancer: a systematic review of pub-lished studies. Br J Cancer. 2006;94:982–999.
2. Adam R. Chemotherapy and surgery: new perspectives on the treatmentof unresectable liver metastases. Ann Oncol. 2003;14(suppl 2):ii13–ii16.
3. Alberts SR, Horvath WL, Sternfeld WC, et al. Oxaliplatin, fluorouracil,and leucovorin for patients with unresectable liver-only metastases fromcolorectal cancer: a north central cancer treatment group phase II study.J Clin Oncol. 2005;23:9243–9249.
4. de la Camara J, Rodriguez J, Rotellar F, et al. Triplet therapy withoxaliplatin, irinotecan, 5-fluorouracil and folinic acid within a combinedmodality approach in patients with liver metastases from colorectalcancer. Proc Am Soc Clin Oncol. 2004;23:3593.
5. Giacchetti S, Itzhaki M, Gruia G, et al. Long-term survival of patientswith unresectable colorectal cancer liver metastases following infusionalchemotherapy with 5-fluorouracil, leucovorin, oxaliplatin and surgery.Ann Oncol. 1999;10:663–669.
6. Pozzo C, Basso M, Cassano A, et al. Neoadjuvant treatment of unre-sectable liver disease with irinotecan and 5-fluorouracil plus folinic acidin colorectal cancer patients. Ann Oncol. 2004;15:933–939.
7. Adam R, Aloia T, Levi F, et al. Hepatic resection after rescue cetuximabtreatment for colorectal liver metastases previously refractory to con-ventional systemic therapy. J Clin Oncol. 2007;25:4593–4602.
8. Cunningham D, Humblet Y, Siena S, et al. Cetuximab monotherapy andcetuximab plus irinotecan in irinotecan-refractory metastatic colorectalcancer. N Engl J Med. 2004;351:337–345.
9. Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plusirinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer.N Engl J Med. 2004;350:2335–2342.
10. Azoulay D, Castaing D, Smail A, et al. Resection of nonresectable livermetastases from colorectal cancer after percutaneous portal vein embo-lization. Ann Surg. 2000;231:480–486.
11. Azoulay D, Andreani P, Maggi U, et al. Combined liver resection andreconstruction of the supra-renal vena cava: the Paul Brousse experi-ence. Ann Surg. 2006;244:80–88.
12. Choti MA, Sitzmann JV, Tiburi MF, et al. Trends in long-term survivalfollowing liver resection for hepatic colorectal metastases. Ann Surg. 2002;235:759–766.
13. Elias D, Cavalcanti A, Sabourin JC, et al. Resection of liver metastasesfrom colorectal cancer: the real impact of the surgical margin. Eur J SurgOncol. 1998;24:174–179.
14. Fong Y, Fortner J, Sun RL, et al. Clinical score for predicting recurrenceafter hepatic resection for metastatic colorectal cancer: analysis of 1001consecutive cases. Ann Surg. 1999;230:309–318.
15. Gayowski TJ, Iwatsuki S, Madariaga JR, et al. Experience in hepaticresection for metastatic colorectal cancer: analysis of clinical and patho-logic risk factors. Surgery. 1994;116:703–710.
16. Hamady ZZ, Cameron IC, Wyatt J, et al. Resection margin in patientsundergoing hepatectomy for colorectal liver metastasis: a critical ap-praisal of the 1cm rule. Eur J Surg Oncol. 2006;32:557–563.
17. Jamison RL, Donohue JH, Nagorney DM, et al. Hepatic resection formetastatic colorectal cancer results in cure for some patients. Arch Surg.1997;132:505–510.
Annals of Surgery • Volume 248, Number 4, October 2008 R1 Liver Resection for Colorectal Metastases
© 2008 Lippincott Williams & Wilkins 635

18. Shirabe K, Takenaka K, Gion T, et al. Analysis of prognostic risk factorsin hepatic resection for metastatic colorectal carcinoma with specialreference to the surgical margin. Br J Surg. 1997;84:1077–1080.
19. Welsh FK, Tekkis PP, O’Rourke T, et al. Quantification of risk of a positive(R1) resection margin following hepatic resection for metastatic colorectalcancer: an aid to clinical decision-making. Surg Oncol. 2008;17:3–13.
20. Yamamoto J, Shimada K, Kosuge T, et al. Factors influencing survivalof patients undergoing hepatectomy for colorectal metastases. Br J Surg.1999;86:332–337.
21. Pawlik TM, Scoggins CR, Zorzi D, et al. Effect of surgical margin statuson survival and site of recurrence after hepatic resection for colorectalmetastases. Ann Surg. 2005;241:715–722.
22. Are C, Gonen M, Zazzali K, et al. The impact of margins on outcome afterhepatic resection for colorectal metastasis. Ann Surg. 2007;246:295–300.
23. Cady B, Jenkins RL, Steele GD Jr, et al. Surgical margin in hepaticresection for colorectal metastasis: a critical and improvable determinantof outcome. Ann Surg. 1998;227:566–571.
24. Ekberg H, Tranberg KG, Andersson R, et al. Determinants of survival inliver resection for colorectal secondaries. Br J Surg. 1986;73:727–731.
25. Kokudo N, Miki Y, Sugai S, et al. Genetic and histological assessmentof surgical margins in resected liver metastases from colorectal carci-noma: minimum surgical margins for successful resection. Arch Surg.2002;137:833–840.
26. Ng JK, Urbanski SJ, Mangat N, et al. Colorectal liver metastasescontract centripetally with a response to chemotherapy: a histomorpho-logic study. Cancer. 2008;112:362–371.
27. Nordlinger B, Guiguet M, Vaillant JC, et al. Surgical resection ofcolorectal carcinoma metastases to the liver. A prognostic scoringsystem to improve case selection, based on 1568 patients. AssociationFrancaise de Chirurgie. Cancer. 1996;77:1254–1262.
28. Rees M, Plant G, Bygrave S. Late results justify resection for multiplehepatic metastases from colorectal cancer. Br J Surg. 1997;84:1136–1140.
29. World Health Organization. Handbook for Reporting Results of CancerTreatment. Geneva: World Health Organization; 1979.
30. Therasse P, Arbuck SG, Eisenhauer EA, et al. New guidelines toevaluate the response to treatment in solid tumors. European Organiza-tion for Research and Treatment of Cancer, National Cancer Institute ofthe United States, National Cancer Institute of Canada. J Natl CancerInst. 2000;92:205–216.
31. Sobin LH, Wittekind Ch. TNM Classification of Malignant Tumours.Hoboken, NJ: John Wiley & Sons; 2002.
32. Adam R, Bismuth H, Castaing D, et al. Repeat hepatectomy for colo-rectal liver metastases. Ann Surg. 1997;225:51–60.
33. Bismuth H. Surgical anatomy and anatomical surgery of the liver. WorldJ Surg. 1982;6:3–9.
34. Couinaud C. Le foie: etudes anatomiques et chirurgicales. Paris: Massonet Cie; 1957.
35. Dindo D, Demartines N, Clavien PA. Classification of surgical compli-cations: a new proposal with evaluation in a cohort of 6336 patients andresults of a survey. Ann Surg. 2004;240:205–213.
36. Bodingbauer M, Tamandl D, Schmid K, et al. Size of surgical margindoes not influence recurrence rates after curative liver resection forcolorectal cancer liver metastases. Br J Surg. 2007;94:1133–1138.
37. Figueras J, Burdio F, Ramos E, et al. Effect of subcentimeter nonpositiveresection margin on hepatic recurrence in patients undergoing hepatec-tomy for colorectal liver metastases. Evidences from 663 liver resec-tions. Ann Oncol. 2007;18:1190–1195.
38. Falcone A, Ricci S, Brunetti I, et al. Phase III trial of infusionalfluorouracil, leucovorin, oxaliplatin, and irinotecan (FOLFOXIRI) com-pared with infusional fluorouracil, leucovorin, and irinotecan (FOLFIRI)as first-line treatment for metastatic colorectal cancer: the GruppoOncologico Nord Ovest. J Clin Oncol. 2007;25:1670–1676.
39. Tournigand C, Andre T, Achille E, et al. FOLFIRI followed byFOLFOX6 or the reverse sequence in advanced colorectal cancer: arandomized GERCOR study. J Clin Oncol. 2004;22:229 –237.
40. Minagawa M, Makuuchi M, Torzilli G, et al. Extension of the frontiersof surgical indications in the treatment of liver metastases from colo-rectal cancer: long-term results. Ann Surg. 2000;231:487–499.
41. Scheele J, Stangl R, Altendorf-Hofmann A, et al. Resection of colorectalliver metastases. World J Surg. 1995;19:59–71.
DiscussionsDR. MICHAEL A. CHOTI (BALTIMORE, MARYLAND): Surgi-
cal management of hepatic colorectal metastases has evolvedsignificantly in recent years. Increasingly aggressive opera-tions and the use of more active systemic agents, and im-provements in imaging and patient selection have all contrib-uted to improved outcomes and increased optimism for patientswith advanced colorectal cancer. Even resectability has beenredefined, rather than basing it on prognostic factors such asmetastases size and number, it is based more on the capabilityto safely perform complete or R0 resection. In this study, youchallenge even the necessity to achieve negative margins.
As you mentioned, several factors may be contributingto this observation. One factor may be the method fortransecting the liver parenchyma and achieving hemostasis ofthe surface, resulting in an extra margin. Your group uses theultrasonic dissector and the argon beam coagulation device.Newer techniques used by some include thermal devices forpretransection ablation. Can you comment on the role of theseother coagulation devices? Is there a role for deeper thermalsurface ablation in cases where the margin may be close?
The second point relates to defining exactly what an R1resection margin is. I think a distinction needs to be made betweenan R1 resection in which the tumor truly extends microscopically tothe specimen margin, compared with the situation in which a grossmargin seems to have been achieved, but in the pathology report, afocal positive margin is noted. Often, the surface can fracture orcrumble, resulting in ink at the tumor edge, perhaps leading to afalse positive margin. Were you able to distinguish between these 2variations and, if so, were there differences in outcome? Perhaps itis time to consider some kind of stratification of the R1 designation,something like R 0.5 versus R 1.5.
Finally, I would like to comment on the high marginrecurrence rate seen in this study. Although you saw no signif-icant difference between R0 and R1, the isolated margin recur-rence rate was 12% and 15% respectively. This is higher thanour experience and that of others, where we find a 10%–15%margin recurrence in R1 resection and approximately 5% for R0.Can you comment on how margin recurrences were determinedin this study and why the local recurrence rate was so high?
DR. LESLIE H. BLUMGART (NEW YORK, NEW YORK): Ihave no quarrel with your conclusion, but can I ask you todefine your R0 cases? Were they all a centimeter?
Also, were the patients in the R0 group treated with thesame chemotherapy, or was there a much greater preponderanceof the new chemotherapy, which is much more effective, in yourR1 group?
DR. FREDERICK L. GREENE (CHARLOTTE, NORTH CAROLINA):As editor of the TNM Staging Manual, I have a practicalquestion as we are preparing our seventh edition. The currentdefinition of R0 is no histologic evidence of a tumor. Should
de Haas et al Annals of Surgery • Volume 248, Number 4, October 2008
© 2008 Lippincott Williams & Wilkins636

we change our definition to mean that if there is tumor within1 or 2 mm that should be an R1 and should not be R0?
DR. BRYAN M. CLARY (DURHAM, NORTH CAROLINA): As Irecall from one of your group’s prior landmark publications,you demonstrated that patients with initially unresectabledisease can be downsized to resectability. My recollectionfrom that paper, though, is that those patients who requireddownsizing to resectability had a poorer outcome than thosewho were initially unresectable. I suspect a large number ofyour R1 patients were probably in that group who requireddownsizing. My question is, is there a difference in outcomesin people who require downsizing and have an R1 resectionversus those who undergo an R1 without downsizing?
DR. RENE ADAM (VILLEJUIF, FRANCE): I would like to thankall the discussants for their interesting comments and questions.With regard to the question of Michael Choti, I would say that thereis certainly a role of additional ablation in patients with R1 resec-tion. I have mentioned the application of argon beam or bipolarcoagulation to the raw surface of the transected liver. We have alsoused in the past, contact cryotherapy. Indeed, our routine policy wasto cut the specimen just after the hepatectomy and when we sawthat the resection margin was close to the tumor, we used wheneverpossible any “ablative” means to obtain a little increase (1–2 mm)in tumor-free hepatic tissue rim. However, we have not usedradiofrequency ablation since our multiarray probes were notadapted to direct application surface.
The R1 definition is clearly an important point. We haveused a combined definition meaning that the pathologist had toconclude that microscopically the minimal tumor-free marginwas 0 mm, while the surgeon has to be sure that macroscopicallyall of the tumoral tissue has been removed. So, our definition ofan R1 resection was based on the presence of these two condi-tions. With regards to the different subtypes of R1 resection Iwould agree with you that in some cases when we see intraop-eratively a fractionated tumor, we may challenge the fact that wehave removed all the tumor. This obviously may be differentfrom a gross margin apparently negative macroscopically butturned positive on microscopy. However, to avoid subjectivefactors, we have considered all of the patients for whom thepathologist stated that the minimal tumor-free margin was 0mm, and for whom the surgeon was convinced of havingremoved all macroscopic tumor deposits, irrespective of otherfactors of consideration.
It is true that among the total number of intrahepaticrecurrences, 15% were located at the surgical margin followingR0 liver resection, compared with 12% after an R1 liver resec-tion. However, when the rate of surgical margin recurrences iscalculated within the total group of patients that developed arecurrence (either intra- or extrahepatic), the percentages fall to8% after an R0 resection and 9% after an R1 resection. The factthat these percentages do not widely differ could possibly rely on
the presence in the R0 resection group of patients with no morethan 1 or 2 mm safe margins, known to be at higher risk ofrecurrence than patients with larger margins. It further under-lines that long-term outcome following R1 resections is close tothat observed after R0 resections.
With regard to the question of Leslie Blumgart about thedefinition of R0 resections, I know that some discrepancy may existregarding this definition, but clearly, R0 resection in our studyconcerned all patients in whom all tumoral deposits were removedby the surgeon with a tumor-free margin of at least 1 mm for eachlesion. The fact that our definition of R0 resection includes atumor-free margin for each lesion is, of course, an important point.In practice, when we were dealing with a patient that had 10metastatic lesions, if only 1 lesion did not have a margin of security,this was for us sufficient not to consider this patient as R0 but as R1.For R0 resection, all lesions should have been removed with atumor-free margin of at least 1 mm.
The type of chemotherapy used could, of course, have beencritical for the results. In the current study, patients operated in 1990were already treated with effective chemotherapy regimens. Wehad the chance to be one of the first hospitals in Europe usingoxaliplatin since we used a chronomodulated regimen of 5-FU andoxaliplatin from 1988. This combination still continues to be part ofthe standard oncologic therapy. We did not use biotherapies at thetime of the study, but clearly, chemotherapy treatment has beenrelatively homogeneous during the study period.
The question of Dr. Greene about the possible changeof the TNM classification is of major importance. Maybe 1 or2 mm-only safe margins could be better considered as an R1resection if the recurrence rates are really different with sucha modification of the present classification. However, thedesign and definitions used in our study do not allow us toanswer the question of the potentially better discriminativevalue of 1 to 2 mm rather than 0 mm. The results, showingnot so much difference between R0 (� 0 mm margin) and R1(0 mm margin) resections, only argue for extending resectionto patients of the latter group.
Coming to the last question of Dr. Clary about the rateof initial unresectability in the R1 patient group, clearly amajority of R1 patients were initially unresectable (56%), andthis explains indeed why this population differs from that inthe R0 patient group (only 31% initially unresectable). Con-cerning the point about a possible difference between patientsthat underwent an R1 resection while initially unresectable andR1 patients that were initially resectable, no differences inlong-term outcome were observed in our study between bothgroups. However, in an even larger group of R1 patients, a survivaldifference might occur, as patients presenting with initially unre-sectable disease probably have less favorable tumor biology.
Many thanks again to all the discussants and to theASA for giving me the opportunity to present this study.
Annals of Surgery • Volume 248, Number 4, October 2008 R1 Liver Resection for Colorectal Metastases
© 2008 Lippincott Williams & Wilkins 637







