
Rheumatoid arthritis
W. Katchamart MD, MSc (Clin Epi)
Associate professor, Division of Rheumatology
Department of Medicine, Siriraj Hospital
Mahidol University

Epidemiology
Chronic systemic inflammatory condition + chronic inflammation of synovium
Peak incidence of RA occurs in bimodal pattern at aged of 20-30 years and 40-60 years
Women are affected by rheumatoid arthritis (RA) approximately 3 times more often than men
Sex differences diminish in older age groups , especially age of > 75 years
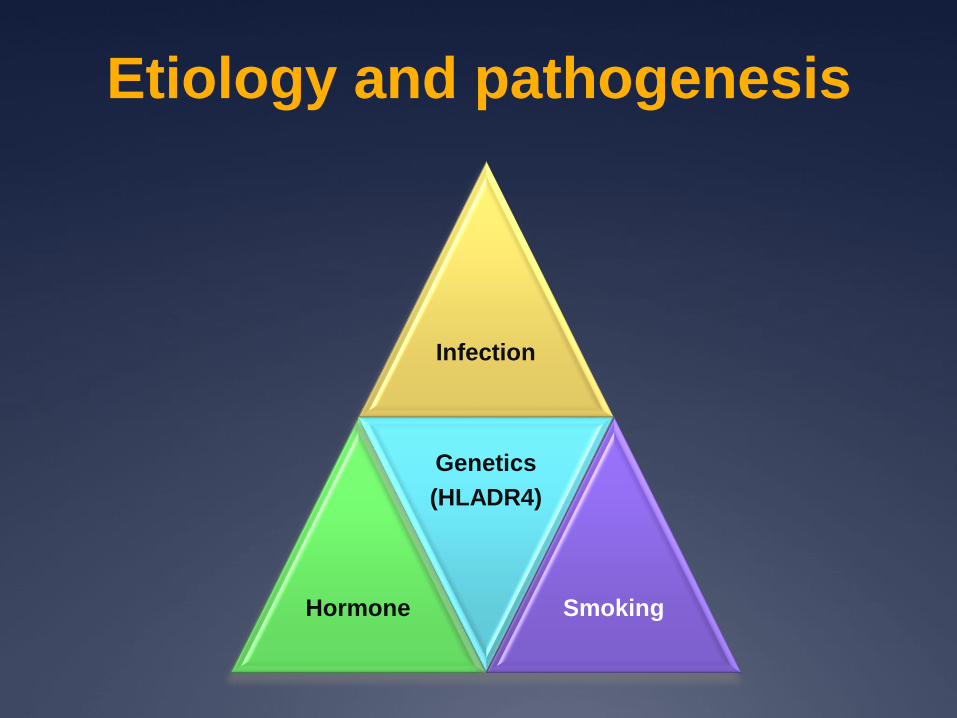
Etiology and pathogenesis
Infection
Hormone
Genetics
(HLADR4)
Smoking
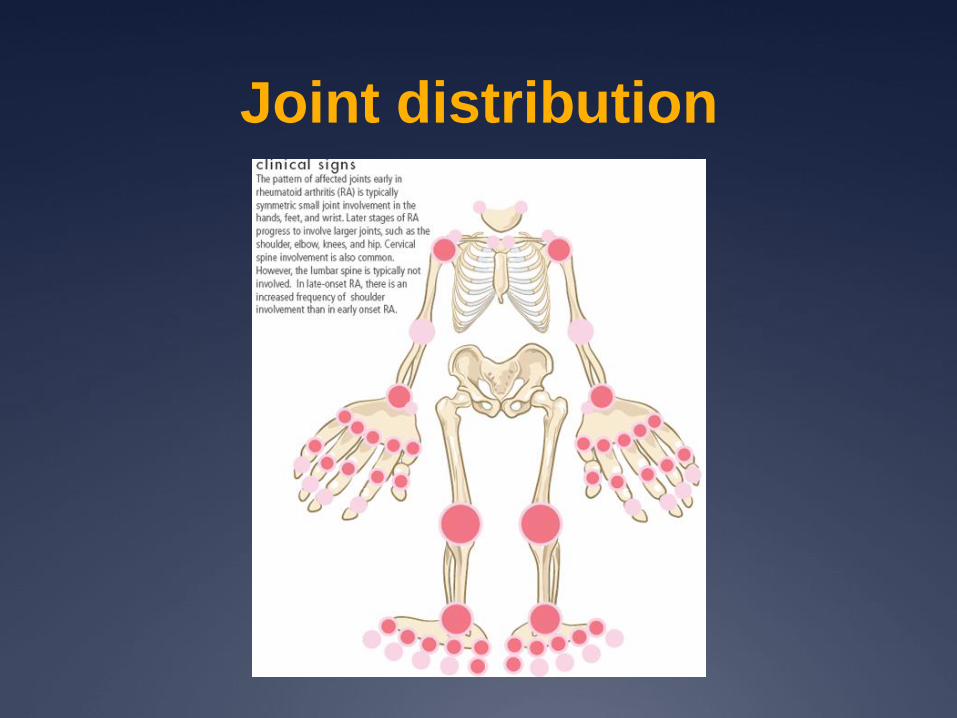
Joint distribution

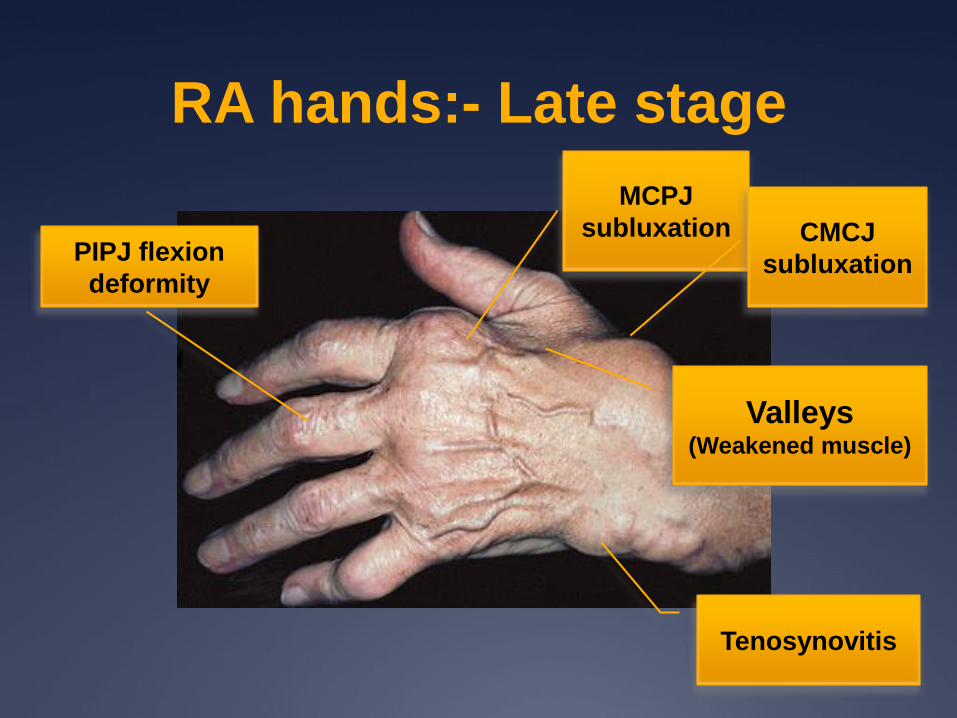
RA hands:- Late stage
Ulnar
deviation
of fingers
Subluxation
of MCPJProtusion of
ulnar styloid
Radial deviation
of wrists
Zigzag deformity

RA hands:- Late stage
RA hands:- Late stage
Valleys(Weakened muscle)
MCPJ
subluxationPIPJ flexion
deformity
Tenosynovitis
CMCJ
subluxation
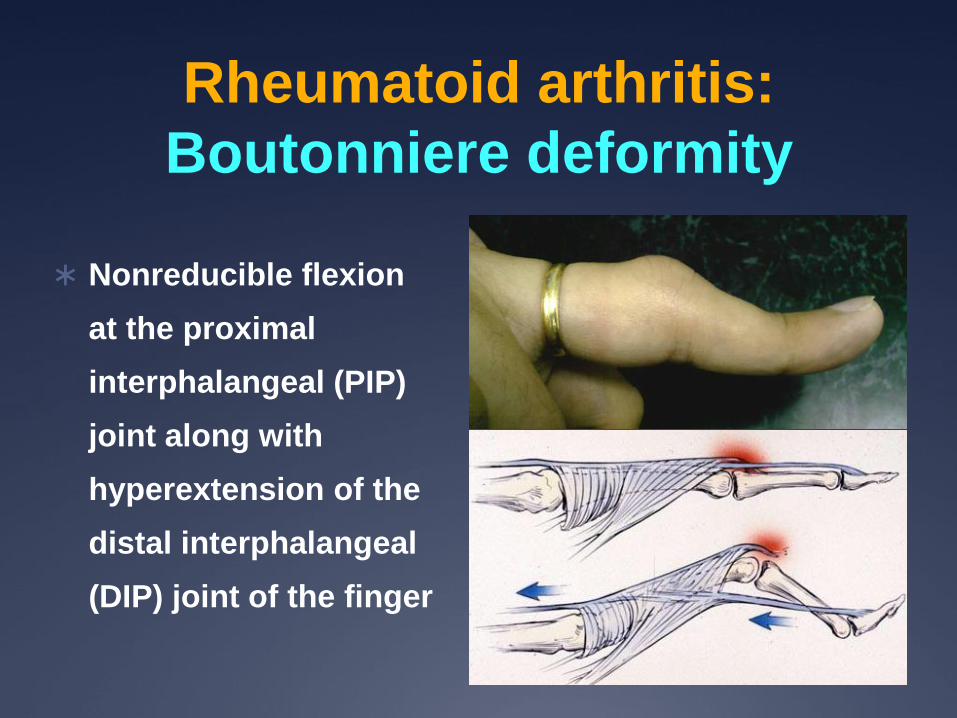
Rheumatoid arthritis:
Boutonniere deformity
Nonreducible flexion
at the proximal
interphalangeal (PIP)
joint along with
hyperextension of the
distal interphalangeal
(DIP) joint of the finger
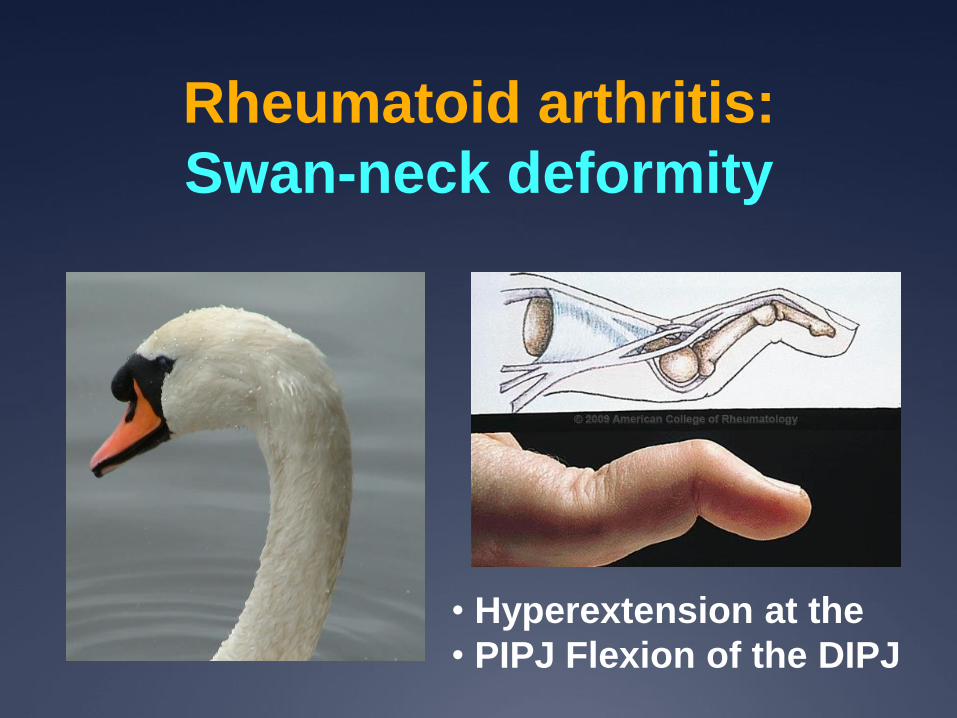
Rheumatoid arthritis:
Swan-neck deformity
• Hyperextension at the
• PIPJ Flexion of the DIPJ

Rheumatoid arthritis: Arthritis mutilans,
Opera glass hands, Telescopic fingers
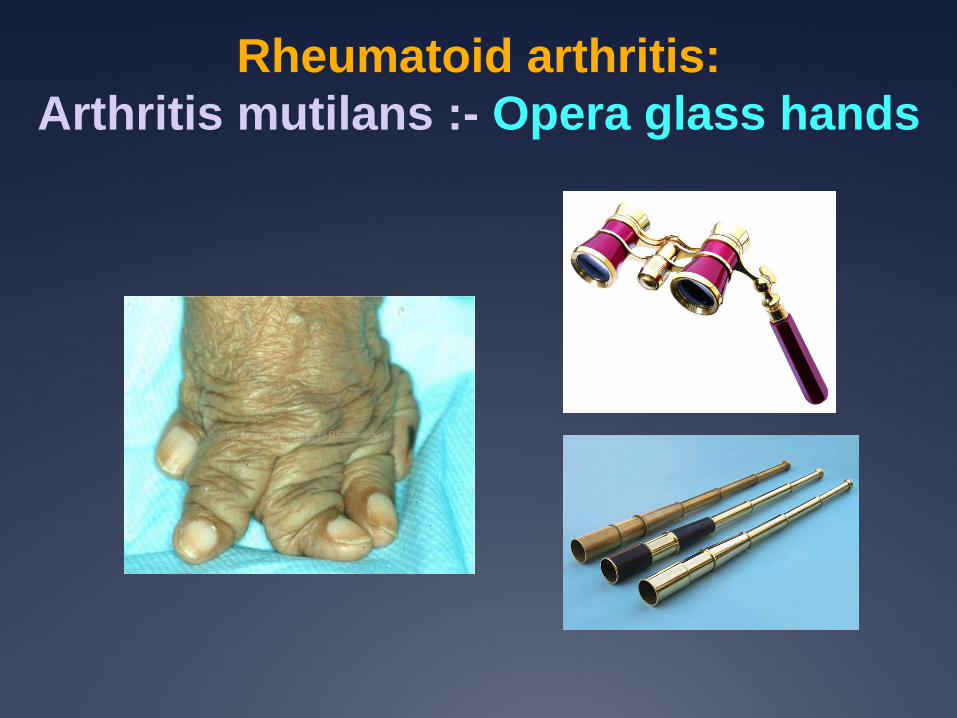
Rheumatoid arthritis:
Arthritis mutilans :- Opera glass hands

RA:- feet

Rheumatoid arthritis: cervical spine,
posterior atlantoaxial subluxation
Lateral neck extension Lateral neck flexion

Rheumatoid arthritis: cervical spine,
basilar invagination

Rheumatoid arthritis: cervical spine,
vertical atlantoaxial subluxation
(MRI)
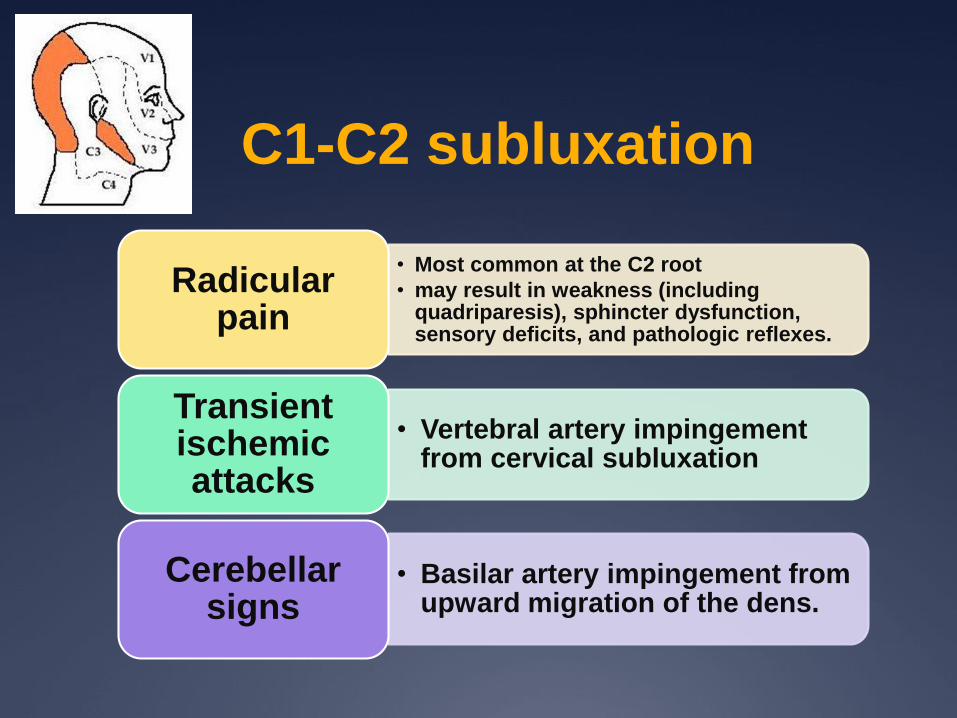
C1-C2 subluxation
• Most common at the C2 root
• may result in weakness (including quadriparesis), sphincter dysfunction, sensory deficits, and pathologic reflexes.
Radicularpain
• Vertebral artery impingement from cervical subluxation
Transient ischemic attacks
• Basilar artery impingement from upward migration of the dens.
Cerebellarsigns
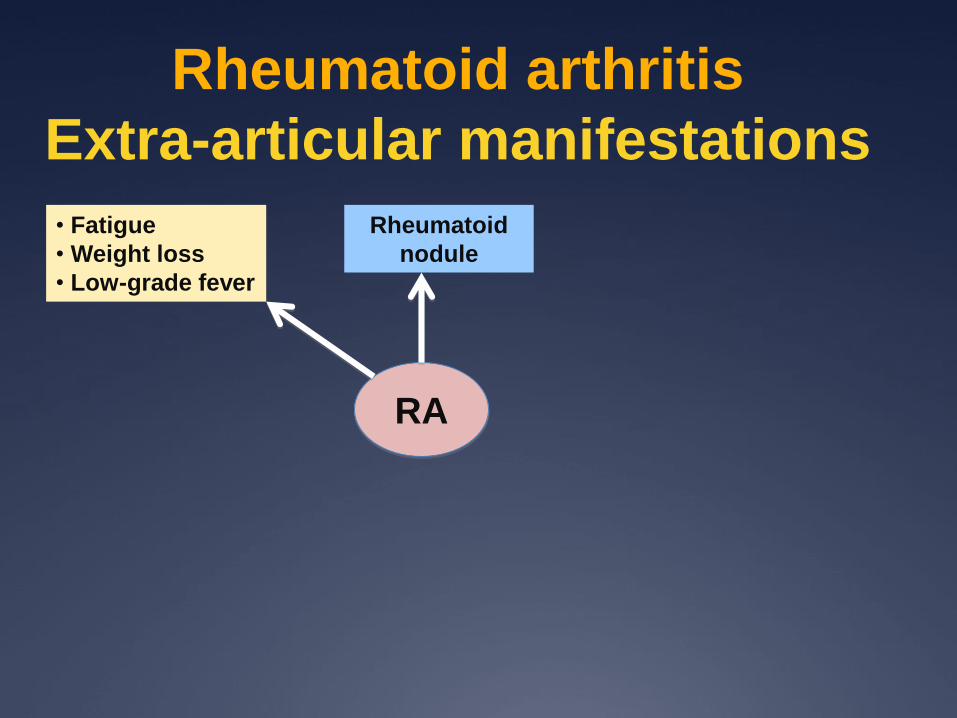
Rheumatoid arthritis
Extra-articular manifestations
RA
Rheumatoid
nodule
• Fatigue
• Weight loss
• Low-grade fever

Extra-articular manifestations
Rheumatoid nodule

Extra-articular manifestations
Rheumatoid nodule

Extra-articular manifestations
Rheumatoid nodule: - lung

Rheumatoid arthritis
Extra-articular manifestations
RA
• Atherosclerosis
• Pericarditis
• Myocarditis
• Vasculitis
Rheumatoid
nodule
• Fatigue
• Weight loss
• Low-grade fever

Rheumatoid arthritis
Vasculitis

Inflammation leads to atherosclerosis
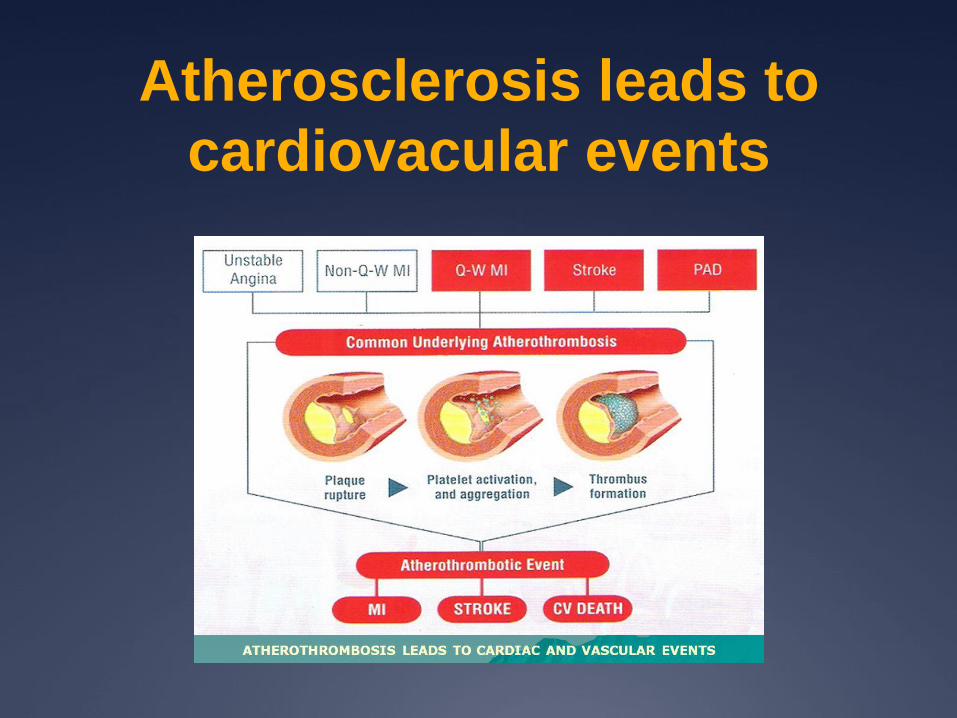
Atherosclerosis leads to
cardiovacular events

Cardiovascular Mortality of RAMeune et al Rheumatology 2009
Standarized mortality rate (SMR) = 1.61
(1.48-1.75 , p< 0.0001)
Increased risk of CVS death
= 60%

Rheumatoid arthritis
Extra-articular manifestations
RA
• Atherosclerosis
• Pericarditis
• Myocarditis
• Vasculitis
• Pleuritis
• Interstitial pneumonitis
• Lung fibrosis
• Pulmonary nodule
• Broncheolitis
• Pulmonary hypertension
Rheumatoid
nodule
• Fatigue
• Weight loss
• Low-grade fever
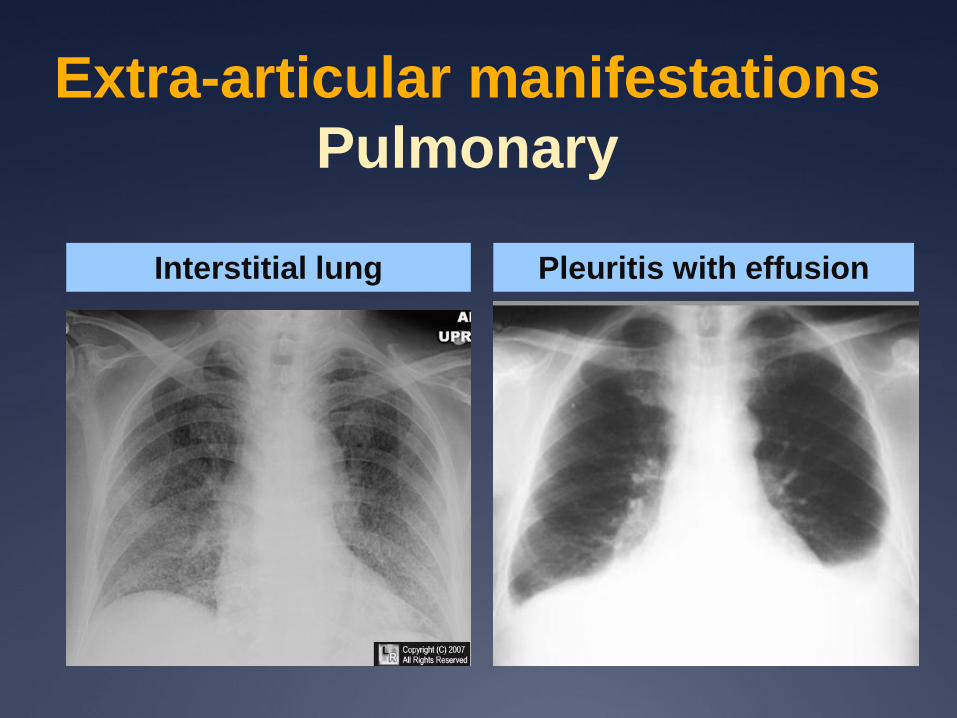
Extra-articular manifestations
Pulmonary
Pleuritis with effusionInterstitial lung

Rheumatoid arthritis
Extra-articular manifestations
RA
• Atherosclerosis
• Pericarditis
• Myocarditis
• Vasculitis
• Pleuritis
• Interstitial pneumonitis
• Lung fibrosis
• Pulmonary nodule
• Broncheolitis
• Pulmonary hypertension
Rheumatoid
nodule
• Fatigue
• Weight loss
• Low-grade fever
• Anemia
• Hematologic malignancy
• Felty’s syndrome
• LGL syndrome
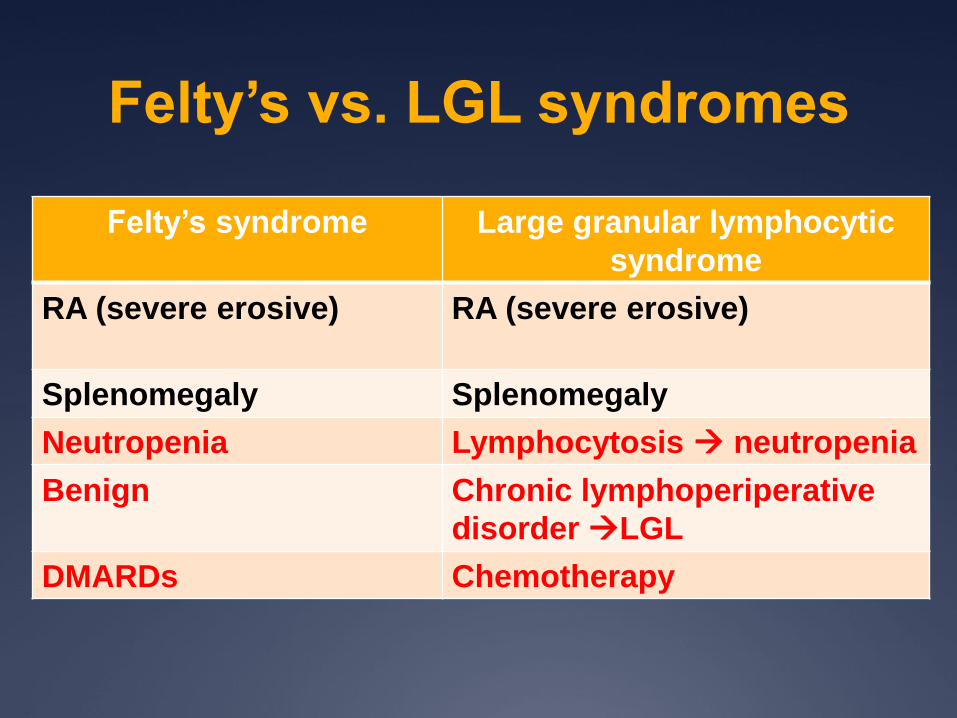
Felty’s vs. LGL syndromes
Felty’s syndrome Large granular lymphocytic
syndrome
RA (severe erosive) RA (severe erosive)
Splenomegaly Splenomegaly
Neutropenia Lymphocytosis neutropenia
Benign Chronic lymphoperiperative
disorder LGL
DMARDs Chemotherapy

Large granular lymphocyte
syndrome
Large granular lymphocyte is an irregular nuclear contour, coarse
chromatin, and azurophilic granules with pale blue cytoplasm

Rheumatoid arthritis
Extra-articular manifestations
RA
• Atherosclerosis
• Pericarditis
• Myocarditis
• Vasculitis
• Pleuritis
• Interstitial pneumonitis
• Lung fibrosis
• Pulmonary nodule
• Broncheolitis
• Pulmonary hypertension
•Keratoconjunctivitis
sicca
• Scleritis
• Episcleritis
• Scleromalacia
perforan
Rheumatoid
nodule
• Fatigue
• Weight loss
• Low-grade fever
• Anemia
• Hematologic malignancy
• Felty’s syndrome
• LGL syndrome

Extra-articular manifestations
Eye
Keratoconjunctivitis Sicca

Extra-articular manifestations
Eye (2)
Episcleritis Scleritis

Extra-articular manifestations
Eye (3)
Scleromalacia perforans

Investigation

RA :- Radiography
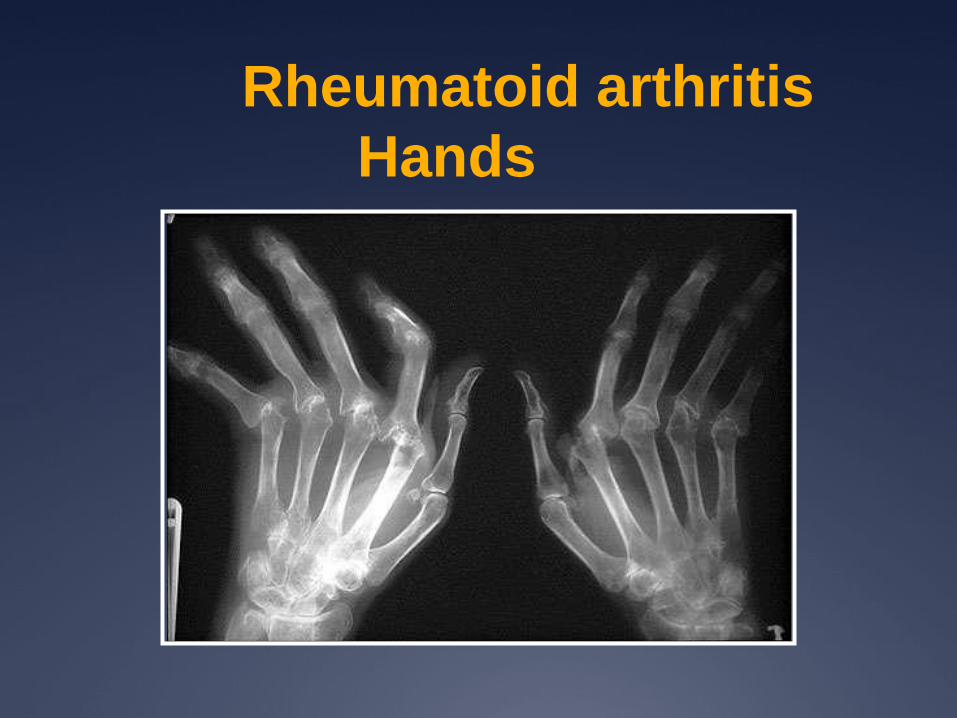
Rheumatoid arthritis
Hands

Rheumatoid arthritis
PIPJ and MCPJ erosion
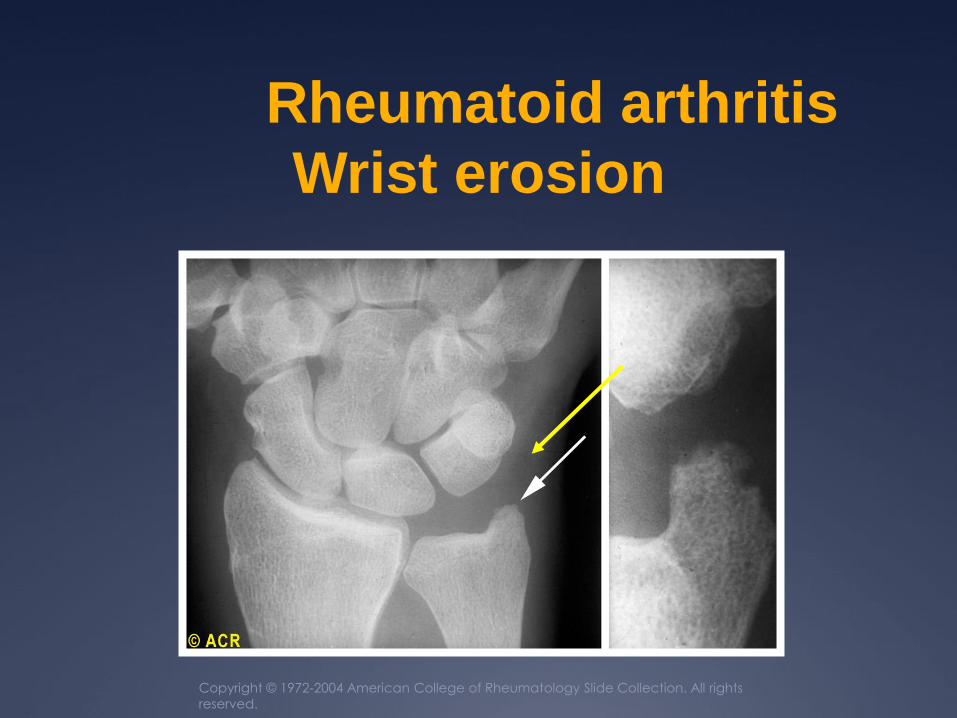
Copyright © 1972-2004 American College of Rheumatology Slide Collection. All rights
reserved.
Rheumatoid arthritis
Wrist erosion

Rheumatoid factor
Anti-citrullinated peptide antibody
Avouac et al Ann Rheum Dis 2006;65:845-851
Test
Pooled
Sensitivity
(95%CI)
Pooled
Specificity
(95%CI)
Pooled
+ LR
(95%CI)
Pooled
- LR
(95%CI)
IgM-RF
(n=50)
69%
(68-70%)
85%
(84-86%)
4.86
(4-6)
0.38
(0.3- 0.4)
ACPA
(n=37)
67%
(65-68%)
95%
(95%-96%)
12.5
(9.7-16)
0.36
(0.3-0.4)
Diagnosis

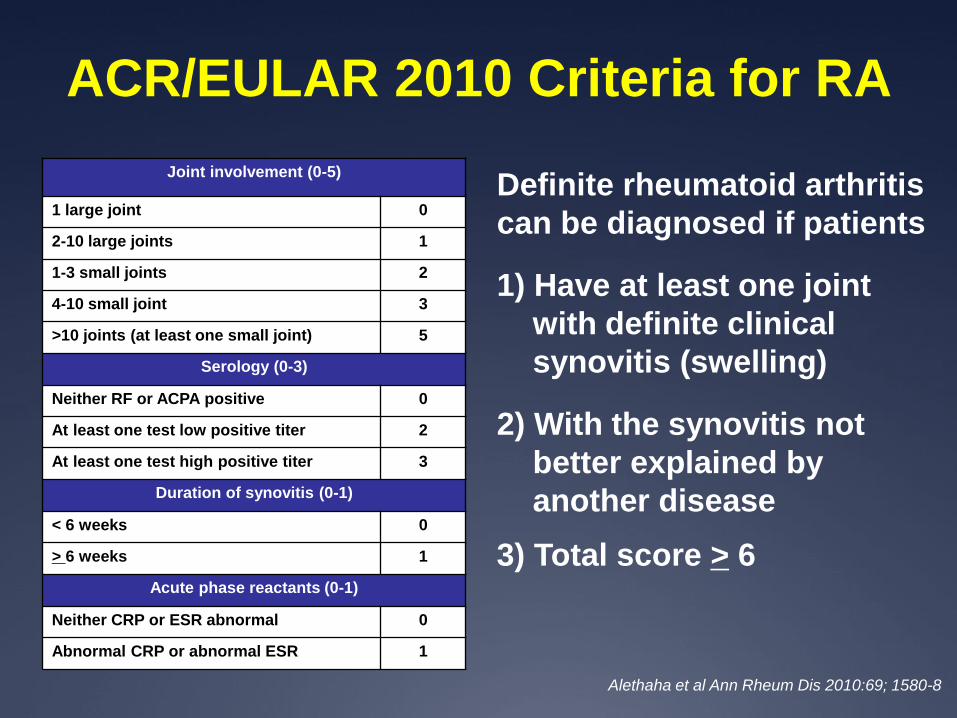
Joint involvement (0-5)
1 large joint 0
2-10 large joints 1
1-3 small joints 2
4-10 small joint 3
>10 joints (at least one small joint) 5
Serology (0-3)
Neither RF or ACPA positive 0
At least one test low positive titer 2
At least one test high positive titer 3
Duration of synovitis (0-1)
< 6 weeks 0
> 6 weeks 1
Acute phase reactants (0-1)
Neither CRP or ESR abnormal 0
Abnormal CRP or abnormal ESR 1
Definite rheumatoid arthritis
can be diagnosed if patients
1) Have at least one joint
with definite clinical
synovitis (swelling)
2) With the synovitis not
better explained by
another disease
ACR/EULAR 2010 Criteria for RA
Except
CMCJ, DIPJ,
and 1st MTPJ
High = > 3
times of ULN
Alethaha et al Ann Rheum Dis 2010:69; 1580-8

Differential diagnosis for
polyarthritis
Symmetrical Asymmetrical
Inflammatory RA, Still’s disease
CNTD (SLE,MCTD)
Rheumatic fever
Polymyalgia rheumatica
Ankylosing spondylitis
Reactive arthritis
Psoriatic arthritis
Enteropatic arthritis
Degenerative OA(generalized,nodal)
Crystal induced CPPD (pseudo RA)
Milwaukee shoulder
Hemochromatosis
Chronic tophaceous gout
CPPD (pseudogout)
Infectious Viral arthritis
Lyme disease
Bacterial arthritis
Bacterial endocarditis
Malignancy Leukemia
Lymphoma
Joint involvement (0-5)
1 large joint 0
2-10 large joints 1
1-3 small joints 2
4-10 small joint 3
>10 joints (at least one small joint) 5
Serology (0-3)
Neither RF or ACPA positive 0
At least one test low positive titer 2
At least one test high positive titer 3
Duration of synovitis (0-1)
< 6 weeks 0
> 6 weeks 1
Acute phase reactants (0-1)
Neither CRP or ESR abnormal 0
Abnormal CRP or abnormal ESR 1
Definite rheumatoid arthritis
can be diagnosed if patients
1) Have at least one joint
with definite clinical
synovitis (swelling)
2) With the synovitis not
better explained by
another disease
ACR/EULAR 2010 Criteria for RA
Alethaha et al Ann Rheum Dis 2010:69; 1580-8
3) Total score > 6

Treatment
Aim and strategies
Goal Strategy
Pain relief • NSAIDS
• Analgesics
• Corticosteroid (low dose)

Treatment
Aim and strategies
Goal Strategy
Pain relief • NSAIDS
• Analgesics
• Corticosteroid (low dose)
Prevent irreversible
structural damage and
functional disability
• Early diagnosis
• Aggressive treatment
• Tight control strategy

Disease modifying anti-rheumatic drugs
(DMARDs)
DMARDs
Synthetic
Conventional synthetic
(csDMARD)
Antimalarial
Methotrexate
Sulfasalazine
Leflunomide
Cyclosporin A
Azathioprine
Gold
Targeted synthetic
(tsDMARD)
JAK-inhibitor (Tofacitinib)
Biological
Biological originator
(boDMARD)
anti-TNF
anti-CD20
anti-IL 6
anti-CTLA-4
Biosimilar
(bsDMARD)
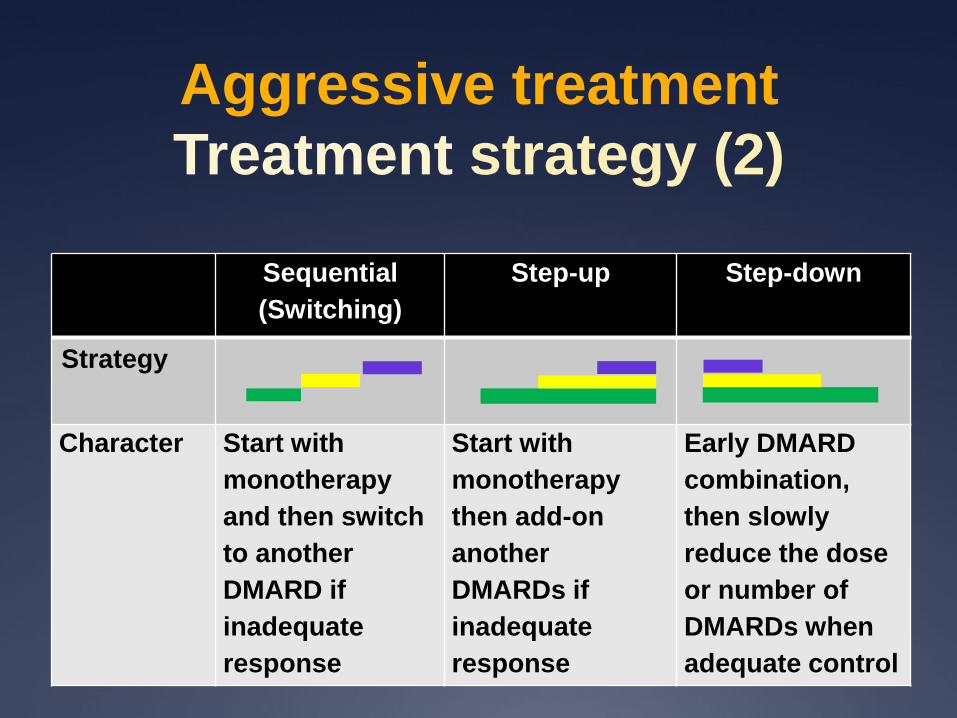
Aggressive treatment
Treatment strategy (2)
Sequential
(Switching)
Step-up Step-down
Strategy
Character Start with
monotherapy
and then switch
to another
DMARD if
inadequate
response
Start with
monotherapy
then add-on
another
DMARDs if
inadequate
response
Early DMARD
combination,
then slowly
reduce the dose
or number of
DMARDs when
adequate control

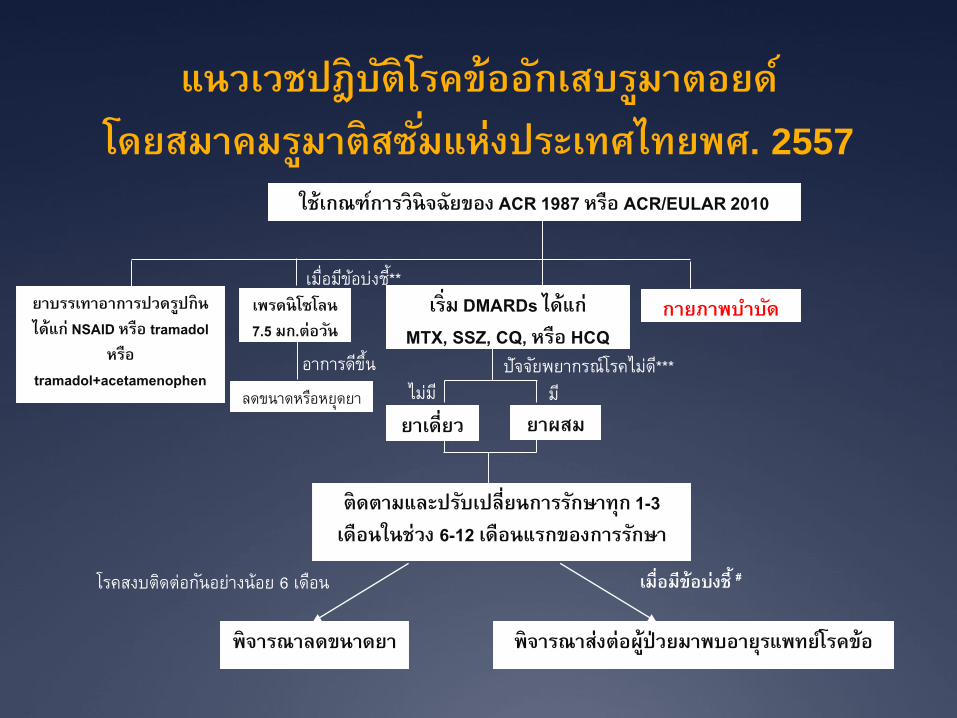
แนวเวชปฎิบติัโรคข้ออกัเสบรมูาตอยด์โดยสมาคมรมูาติสซัม่แห่งประเทศไทยพศ. 2557
อาการดขีึน้
เมื่อมขีอ้บง่ชี*้*
เม่ือมีข้อบง่ช้ี #
มี
โรคสงบตดิต่อกนัอยา่งน้อย 6 เดอืน
ไมม่ี
ใช้เกณฑก์ารวินิจฉัยของ ACR 1987 หรือ ACR/EULAR 2010
เร่ิม DMARDs ได้แก่MTX, SSZ, CQ, หรือ HCQ
ยาบรรเทาอาการปวดรปูกินได้แก่ NSAID หรือ tramadol
หรือ tramadol+acetamenophen
กายภาพบ าบดั
ยาผสมยาเด่ียว
ติดตามและปรบัเปล่ียนการรกัษาทุก 1-3 เดือนในช่วง 6-12 เดือนแรกของการรกัษา
พิจารณาลดขนาดยา พิจารณาส่งต่อผู้ป่วยมาพบอายรุแพทยโ์รคข้อ
เพรดนิโซโลน 7.5 มก.ต่อวนั
ลดขนาดหรอืหยดุยา
ปัจจยัพยากรณ์โรคไมด่*ี**

Indication for steroid
พิจารณาให้สเตียรอยด์ เมื่อมีข้อบง่ช้ีดงัต่อไปน้ี มีข้ออกัเสบรนุแรง กล่าวคือ ผูป่้วยมีภาวะทพุพลภาพจนไม่สามารถประกอบกิจวตัรประจ าวนัหรอืประกอบอาชีพได้
ผูป่้วยไม่ตอบสนองต่อ NSAIDs
ผูป่้วยมีข้อห้ามของการใช้ NSAIDs เช่น ไตเส่ือม ตบัเส่ือมเป็นต้น

Poor prognostic factors
Functional limitation
Extra-articular disease
Presence of rheumatoid factor
Presence of ACPA
Bony erosions by radiography

ข้อบง่ช้ีในการพิจารณาส่งต่อผูป่้วย
แพทยไ์ม่แน่ใจในการวินิจฉัยโรค ผูป่้วยท่ีมีภาวะแทรกซ้อนจากตวัโรคหรือมีอาการนอกข้อท่ีรนุแรง ผูป่้วยท่ีมีโรคร่วมอ่ืน ๆ ผูป่้วยท่ีไม่ตอบสนองหรือตอบสนองไม่ดีต่อการรกัษาด้วย DMARDs
ขนาดสงูเป็นเวลาอย่างน้อย 3-6 เดือน ผูป่้วยท่ีไม่สามารถหยดุคอรติ์โคสเตียรอยดไ์ด้ภายใน 6-12 เดือน ผูป่้วยท่ีมีภาวะแทรกซ้อนจากการรกัษา ผูป่้วยท่ีตัง้ครรภห์รือให้นมบตุร
แนวเวชปฎิบติัโรคข้ออกัเสบรมูาตอยด์โดยสมาคมรมูาติสซัม่แห่งประเทศไทยพศ. 2557
อาการดขีึน้
เมื่อมขีอ้บง่ชี*้*
เม่ือมีข้อบง่ช้ี #
มี
โรคสงบตดิต่อกนัอยา่งน้อย 6 เดอืน
ไมม่ี
ใช้เกณฑก์ารวินิจฉัยของ ACR 1987 หรือ ACR/EULAR 2010
เร่ิม DMARDs ได้แก่MTX, SSZ, CQ, หรือ HCQ
ยาบรรเทาอาการปวดรปูกินได้แก่ NSAID หรือ tramadol
หรือ tramadol+acetamenophen
กายภาพบ าบดั
ยาผสมยาเด่ียว
ติดตามและปรบัเปล่ียนการรกัษาทุก 1-3 เดือนในช่วง 6-12 เดือนแรกของการรกัษา
พิจารณาลดขนาดยา พิจารณาส่งต่อผู้ป่วยมาพบอายรุแพทยโ์รคข้อ
เพรดนิโซโลน 7.5 มก.ต่อวนั
ลดขนาดหรอืหยดุยา
ปัจจยัพยากรณ์โรคไมด่*ี**

Treatment
Aim and strategies
Goal Strategy
Pain relief • NSAIDS
• Analgesics
• Corticosteroid (low dose)
Prevent irreversible
structural damage and
functional disability
• Early diagnosis
• Aggressive treatment
• Tight control strategy
Preserve function and
maintain patient normal
life style
• Physiotherapy
• Surgery








