Searching for Evidence
Task 1
Find a full text document from a referenceThe ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group . Major outcomes in moderately hypercholesterolemic, hypertensive patients randomized to pravastatin vs usual care: the antihypertensive and lipid- lowering treatment to prevent heart attack trial (ALLHAT-LLT). JAMA. 2002;288:2998-3007.
Task 2
Find the best evidence concerning the use of aspirin for the primary prevention of cardiovascular disease in people with diabetes

ATHENS ACCOUNT
• To get a NHS Athens account, username and password. Register for free at: https://register.athensams.net/nhs/nhseng/
Task 3 NNT - Revision
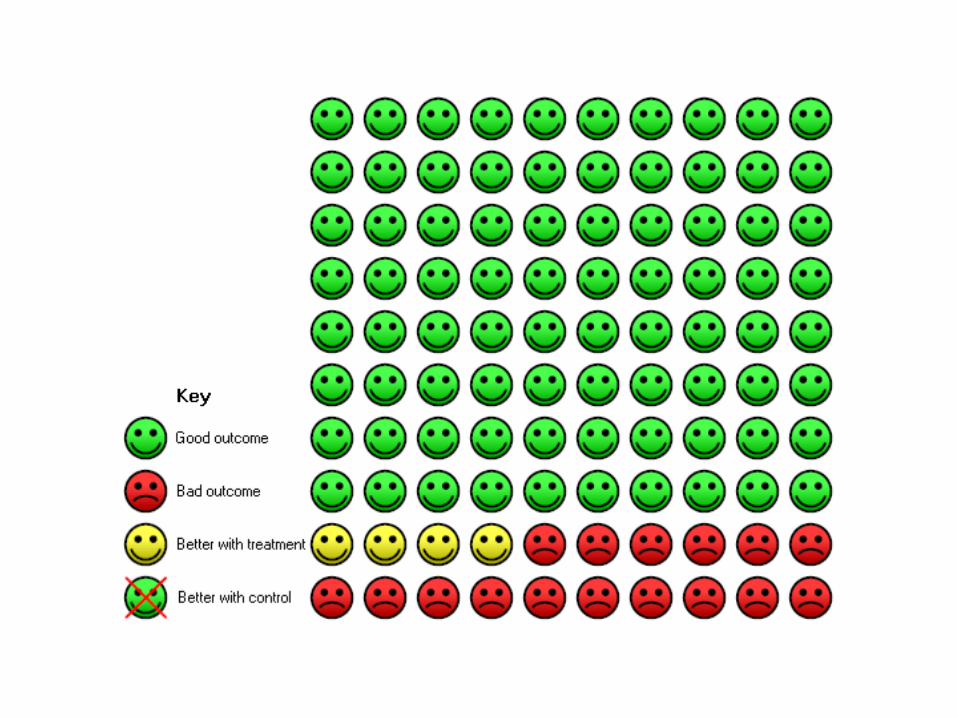
From the diagram on the next slideCalculate:
•Relative Risk•Absolute Risk Reduction•Numbers Needed to Treat

Task 4 NNT Calculation
In the Statins Metaanalysis over a mean 4.3 years:Baseline risk of a major coronary event = 5.7%Relative Risk Reduction is 29.2%Calculate Absolute Risk Reduction andNumbers Needed to Treat (for 4.3 years)
Task 5
From the NNT found in the previous taskCalculate the drug cost to prevent one coronary
event using Simvastatin (£1.37 for 28 tablets)

Task 6
The JUPITER trial of Rosuvastatin 20mg vs placebo (in 17802 healthy men & women LDL<3.4 mmol/l, high sensitivtiy CRP 2.0+ mg/l)
reported:0.77 vs 1.36 events per 100 person-years HR 0.56 (0.46-0.69) p<0.00001Rosuvastatin 20mg costs £26.02 for 28 tabs What was the drug cost to prevent 1 event in this trial?
Systematic Reviews & Guidelines
Chris Lewis Apr 2009
Types of “paper” research evidence• Primary studies
– Case studies– Experiments– Surveys– Clinical Trials
• Secondary studies– Non-systematic reviews– Systematic reviews
• Meta-analyses • Guidelines • Decision analyses
• Economic analyses

Advantages DisadvantagesEvidence-based Guideline
Summarises all relevant research about all possible interventions for a clinical problem. Explores benefits and harms.
May become out-of-date quickly.Expert opinion often fills gaps in evidence.
Systematic Review Summarises all research about an intervention.
Usually only one of several possible interventions is considered. May not explore benefits vs harms.
Primary Study Very specific information Not comprehensive
Types of evidence
Systematic Review• A systematic review is a literature review • focused on a single question • that tries to identify, appraise, select and
synthesize • all high quality research evidence relevant to that
question.

Meta-analysis
A systematic review in which the data from the primary studies is sufficiently similar that they can be analyzed as if they were the same trial.
They provide higher statistical power to detect an effect and a more powerful estimate of true effect size than individual studies.
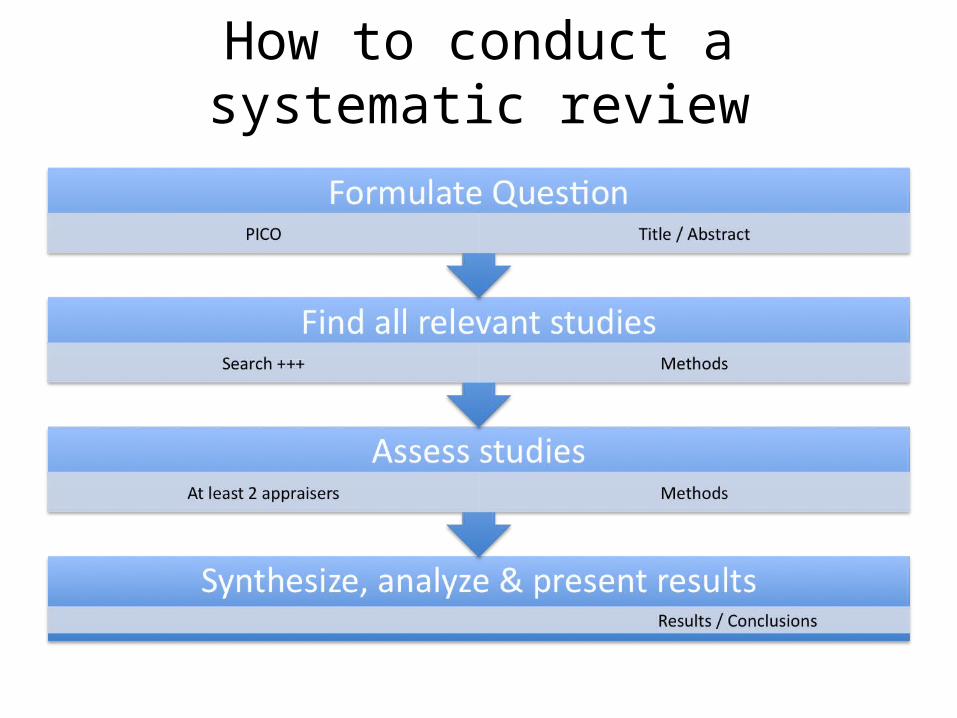
How to conduct a systematic review

FAST critical appraisal
4 FAST Questions for appraising systematic reviews:• Finding: Did they find all relevant studies?• Appraisal: Did they select good studies?• Synthesis: When the studies are put together
what do they mean?• Transferability: Are the conclusions applicable
to my patient?
Critical Appraisal Q1 – Formulate Question
Did the study address a focused clinical question?
• Population• Intervention • Comparator• Outcome
Should be found in the title, abstract or introduction
Critical Appraisal Q2 – Find all relevant studies
Were the inclusion/exclusion criteria appropriate?
• Clearly defined before the literature search• Should specify PICO• May specify type of study (eg RCT)
Should be found in the methods section
Critical Appraisal Q3 – Find all relevant studies
Is it unlikely that important relevant studies were missed?
Search strategy should include:• Major databases: Medline, EMBASE, Cochrane• Reference lists from relevant studies• Inquiry into unpublished studies• Foreign language publications• MESH terms and text words
Methods section should describe search strategyResults section should state number of studies retrieved
and number of studies excluded with reasons

Copyright restrictions may apply.
Thavendiranathan, P. et al. Arch Intern Med 2006;166:2307-2313.
Literature review flowchart
Publication Bias
• ‘Negative’ studies less likely to be published than ‘ positive’ studies
• In a follow-up of 737 studies submitted to the ethics committee at the Johns Hopkins hospital positive studies were 2.5 times more likely to be SUBMITTED than negative studies (Dickersin, JAMA, 1992)
• All trials registered at inception• Unethical not to make results available
Critical Appraisal Q4 – Assess studies
Were the included studies valid?• Should describe how quality of included studies was
assessed• Criteria for quality assessment should be pre-
determined• Criteria for quality assessment should be appropriate
to the question asked
Methods section should describe assessment process and quality criteria
Results section should give information on quality of the individual studies
Critical Appraisal Q5 – Assess studies
Were assessments of studies reproducible?
• Assessed independently by 2+ reviewers• Level of agreement between reviewers• Procedure for dealing with disagreement
Methods should describe how and by who assessments were done
Results should show level of agreements
Critical Appraisal Q6 – Analysis/Results
Were the results similar from study to study?
• Ideally results should be similar (homogeneous)
• Significance of heterogeneity may be assessed• Reasons for heterogeneity should be explored
Results section.Forest plot should show chi2 test for heterogeneity
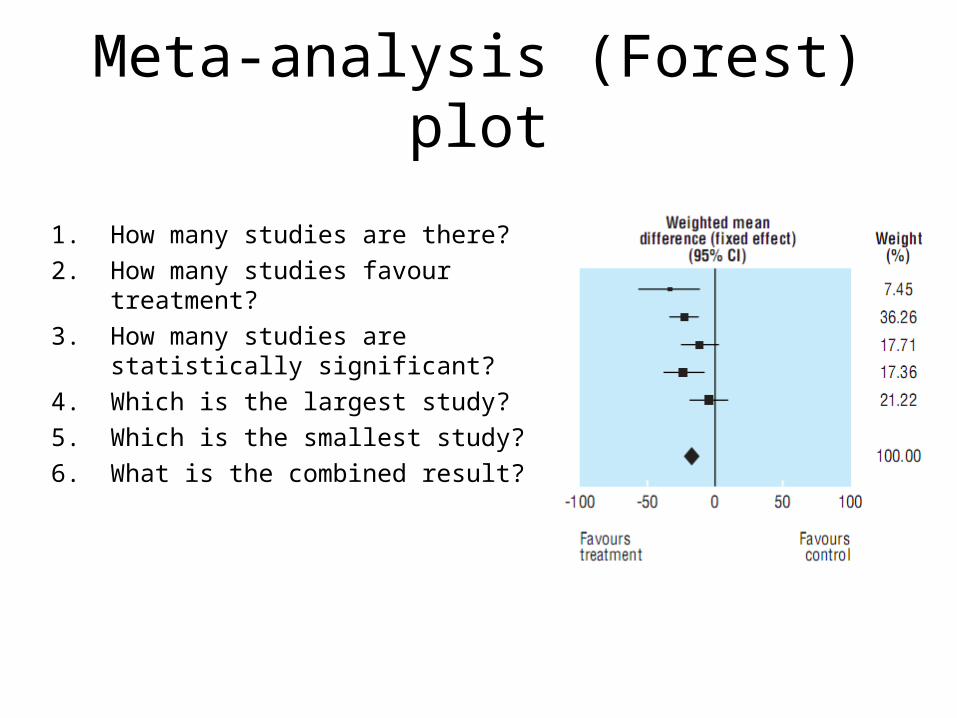
Meta-analysis (Forest) plot
1. How many studies are there?2. How many studies favour treatment?3. How many studies are statistically
significant?4. Which is the largest study?5. Which is the smallest study?6. What is the combined result?
Assessing heterogeneity
“Eyeball” test: In the Forest plot a vertical line running through the combined OR should cross the horizontal lines (95% CI) of all the individual studies

Assessing heterogeneity
Chi2 test or Cochran Q:• If chi2 is statistically significant (p<0.1) there is
definite heterogeneity• If chi2 not statistically significant (p>0.1) and
Q/df >1 there is possible heterogeneity• If chi2 not statistically significant (p>0.1) and
Q/df >1 heterogeneity is very unlikely
Explaining heterogeneity
• Variation in population studied• Variation in intervention• Variation in outcome measures• Variation in study methods

Copyright restrictions may apply.
Thavendiranathan, P. et al. Arch Intern Med 2006;166:2307-2313.
Plotted relative risk ratios (RRs) (95% confidence intervals [CIs]) for major coronary events
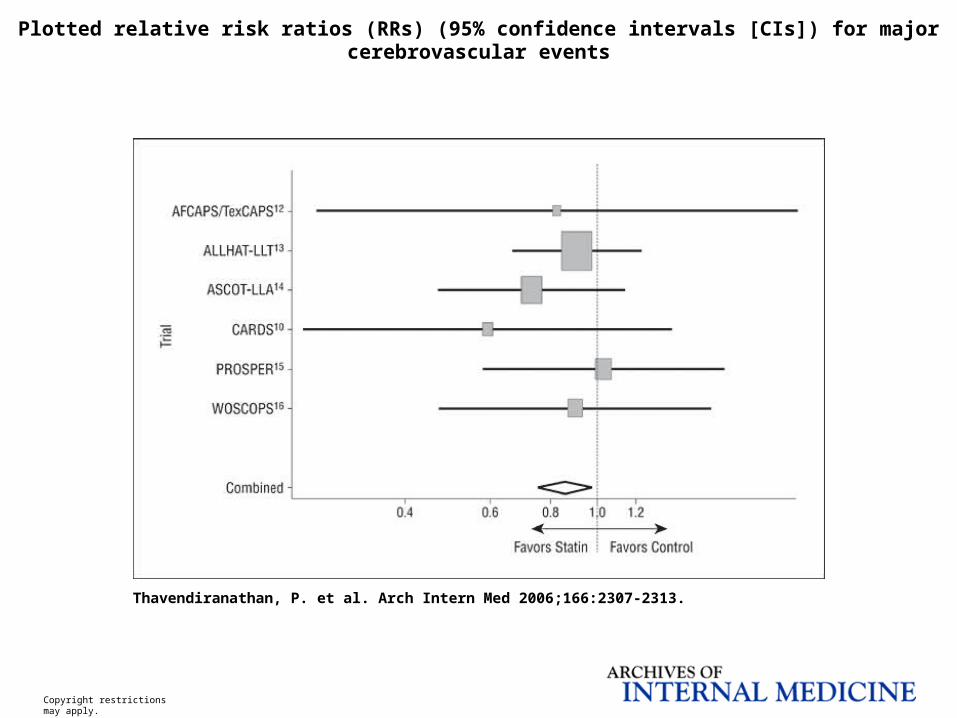
Copyright restrictions may apply.
Thavendiranathan, P. et al. Arch Intern Med 2006;166:2307-2313.
Plotted relative risk ratios (RRs) (95% confidence intervals [CIs]) for major cerebrovascular events
Critical appraisal – Question 7
Are conclusions supported by data?
Biased interpretation or emphasis of results is surprisingly common
Best to form your own conclusions from the data before reading authors conclusions
Then consider the reasons for any differences between your conclusions and the authors’

Critical Appraisal Q8
Are the results clinically relevant?
Assuming we have a statistically significant benefit from treatment:
• Is the size of the benefit worthwhile?• Are the results applicable to my patient?

Funding Bias?
• Funding / employment of authors• Drug company sponsorship
Results
Statins reduce risks by:• Coronary events 29.2% (16.7-39.8%) p<.001• Cerebrovascular events 14.4% (2.8-24.6%)
p0.02• Revascularisations 33.8% (19.6-45.5%) p<.001• Cardiovascular death 22.6% (0.56-1.08) p.13• All deaths 0.92(0.84-1.01) p.09
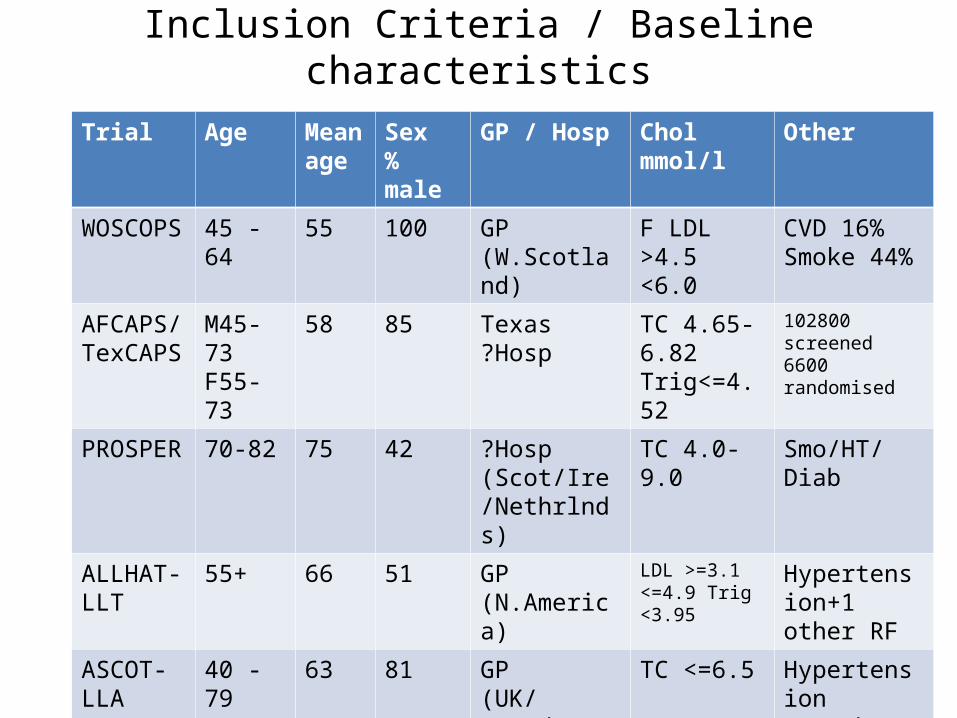
Inclusion Criteria / Baseline characteristics
Trial Age Mean age
Sex% male
GP / Hosp Chol mmol/l Other
WOSCOPS 45 - 64 55 100 GP (W.Scotland)
F LDL >4.5 <6.0
CVD 16%Smoke 44%
AFCAPS/TexCAPS
M45-73F55-73
58 85 Texas?Hosp
TC 4.65-6.82Trig<=4.52
102800 screened6600 randomised
PROSPER 70-82 75 42 ?Hosp (Scot/Ire/Nethrlnds)
TC 4.0-9.0 Smo/HT/Diab
ALLHAT-LLT
55+ 66 51 GP(N.America)
LDL >=3.1 <=4.9 Trig <3.95
Hypertension+1 other RF
ASCOT-LLA
40 - 79 63 81 GP (UK/Scand)
TC <=6.5 Hypertension+3 other RF’s
HPS 40 - 80 NA NA Hosp (UK) F TC >=3.5 Diabetes
CARDS 40 - 75 61 68 GP & Hosp (UK/Ireland)
LDL <=4.14 F Trig <=6.78
Diabetes
CARDS required at least 1 of retinopathy, albuminuria, smoking, hypertension

Influence of DiabetesTrial RR Major Coronary Events % Diabetic
WOSCOPS 1995 0.70 (0.58-0.85) 1.0
AFCAPS/TexCAPS 1998 0.60 (0.43-0.83) 3.8
PROSPER 2002 0.91 (0.71-1.15) 12.2
ALLHAT-LLT 2002 0.91 (0.79-1.04) 34.4
ASCOT-LLA 2003 0.65 (0.50-0.83) 24.3
HPS 2003 0.57 (0.41-0.79) 100
CARDS 2004 0.53 (0.35-0.82) 100

Systematic Reviews
Advantages:• Larger numbers with greater statistical power• Robustness across differing trial populations,
drugs within a classDisadvantages:• Small, but consistent, biases may produce an
invalid conclusion of real effect

Resources
• Oxford Centre for Evidence-based Medicine http://www.cebm.net/
• The Cochrane Collaboration http://www.cochrane.org/

Formula for caluclating NNT from OR if Patient Expected Event Rate is known
GUIDELINES
The AGREE InstrumentAppraisal of Guidelines for REsearch & EvaluationThe AGREE Collaboration – June 2001www.agreecollaboration.org
The AGREE Instrument
23 items organised in six domainsEach item is rated on a 4-point score scale1. Strongly disagree2. Disagree3. Agree4. Strongly agree
Overall assessment• Strongly recommend• Recommend (with provisos/alterations)• Would not recommend• Unsure
Domain 1: Scope & Purpose
1. Overall objective(s)2. Clinical question(s)3. Target population
should all be specifically described

Domain 2: Stakeholder Involvement
4. Guideline development group includes individuals from all relevant professional groups
5. Patients’ views & preferences sought6. Target users clearly defined7. Piloted by end users
Domain 3: Rigour of development
8. Systematic search for evidence9. Criteria for selecting evidence described10.Methods for formulating recommendations
described11.Health benefits, unwanted effects and risks
considered in formulating recommendations12.Explicit link between recommendations and
evidence13.External review by experts before publication14.Procedure for update provided
Domain 4: Clarity & Presentation
15.Recommendations specific & unambiguous16.Management options clearly presented17.Key recommendations easily identifiable18.Guideline supported by tools for application
Domain 5: Applicability
19.Potential organisational barriers in applying the recommendations discussed
20.Cost implications considered21.Key review criteria for monitoring/audit
presented
Domain 6: Editorial Independence
22.Editorially independent from funding body23.Conflicts of interest of guideline
development members recorded







