STRIVETM
What Is the EvidenceThat Critical Pathways Work?
UCLA Cardiac Hospitalization Atherosclerosis Management Program (CHAMP)
ACC Guidelines Applied in Practice (GAP) initiative
AHA “Get With The Guidelines” program
CRUSADE (Can Rapid Risk Stratification of Unstable Angina Patients Suppress ADverse Outcomes with Early Implementation of the ACC/AHA Guidelines)
STRIVETM
CHAMP Study: UCLA
Designed to determine whether physician/patient compliance with preventive therapies can be improved through a hospital-initiated program
Tracked initiation of aspirin, β-blocker, ACE inhibitor, statins Used preprinted orders, guidelines, lectures, discharge forms Population: patients with symptomatic atherosclerosis treated at
university-associated teaching hospital Methods: no specific algorithms used before CHAMP (1992-1993) National guidelines (ACC/AHA, NCEP ATP I and ATP II) used in
CHAMP (1994-1995) Evaluation: treatment rates and clinical outcomes pre-CHAMP
and CHAMP in patients hospitalized for acute MI
Fonarow GC, Gawlinski A. Am J Cardiol. 2000;85(3A):10A-17A.
Cardiac Hospitalization Atherosclerosis Management Program

STRIVETM
Discharge Medications at UCLA Compared With 1437 NRMI Hospitals
0
20
40
60
80
100
Aspirin β-blockers ACEI Statins
68
92 9194 96
12
6872
78
85
52
6470
75
88 8990 91
98/99 Post-CHAMP (UCLA)00/01 Post-CHAMP (UCLA)
92/93 Pre-CHAMP (UCLA)94/95 Post-CHAMP (UCLA)96/97 Post-CHAMP (UCLA)
Fonarow GC, et al. Am J Cardiol. 2001;87:819-822.
[NRMI Hospitals 00/01 (n=154,602)]Nat’l Benchmark
Uti
lizat
ion
Rat
e (%
)CHAMP Over an 8-Year Period: Rapid and Sustained
Improvement, Superior to National Benchmarks
3742
65
77
STRIVETMAdapted from Mehta RH, et al. JAMA. 2002;287:1269-1276.
0
20
40
60
80
100
At Admission At Discharge
Pre-GAPPost-GAP
Asp
irin
Usa
ge
(%)
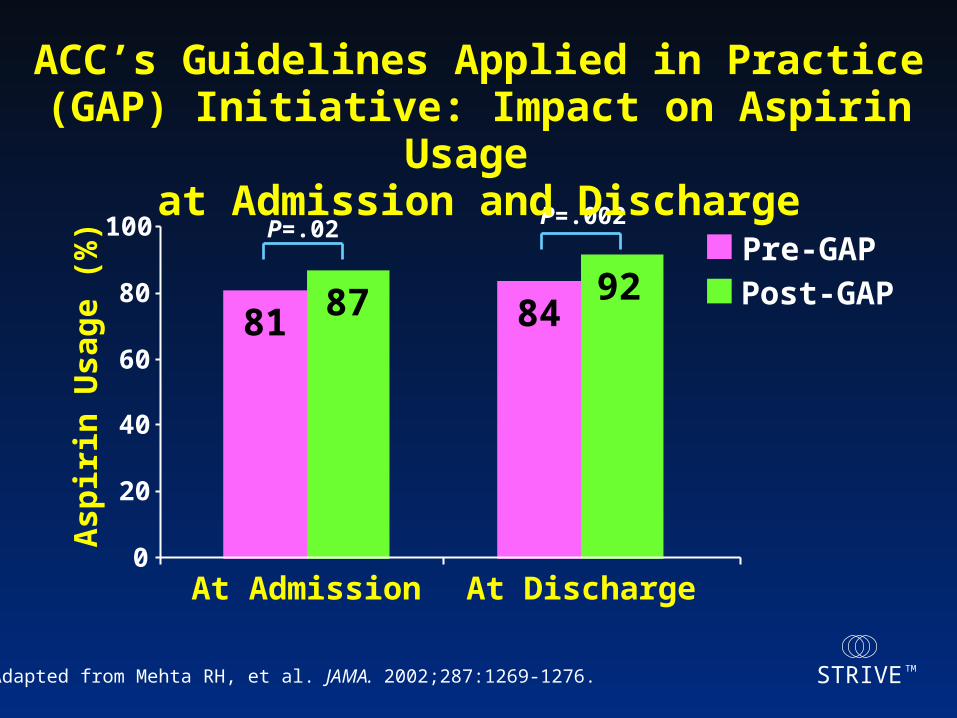
81 87 8492
P=.02 P=.002
ACC’s Guidelines Applied in Practice (GAP) Initiative: Impact on Aspirin Usage
at Admission and Discharge

STRIVETMAdapted with permission from Mehta RH, et al. JAMA. 2002;287:1269-1276.
Qu
alit
y
Ad
he
ren
ce
(%
)
Preintervention
No Tool Use
Tool Use
Postintervention
0
20
40
60
80
100
Aspirin β-Blocker LDL-CNo. of Ideal
Patients
81 8693
6573 77
64 64
82
343 308 96 213 174 71 131 165 87
P=.004P=.001
Early Quality Indicators and Standard Admission Orders
GAP Initiative: Adherence Improves With Tool Use
STRIVETM
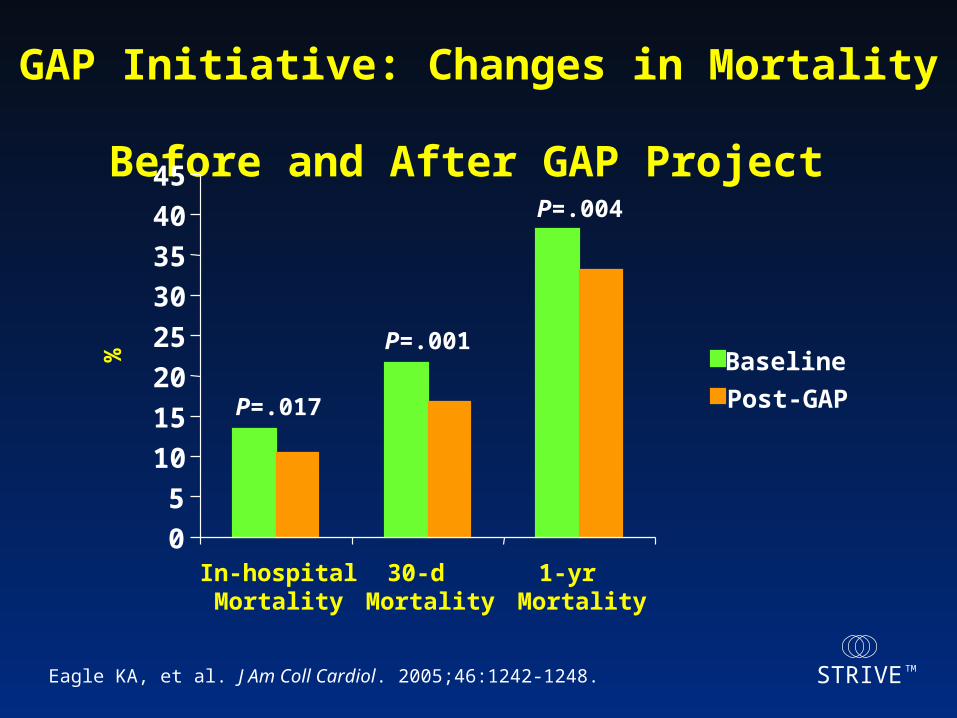
GAP Initiative: Changes in Mortality Before and After GAP Project
Eagle KA, et al. J Am Coll Cardiol. 2005;46:1242-1248.
0
5
10
15
20
25
30
35
40
45
In-hospitalMortality
30-dMortality
1-yrMortality
% Baseline
Post-GAP P=.017
P=.001
P=.004

STRIVETM
AHA “Get With The Guidelines” Program
Components Training materials for hospital staff Patient education materials Assistance in creating multidisciplinary team Secondary prevention guidelines CME workshops Sample materials (care maps, discharge
protocols, discharge forms)
American Heart Association Web site. Get With The Guidelines. Available at: http://www.americanheart.org/presenter.jhtml?identifier=1165.

STRIVETM
Clinical/Lab: 8 clicks
Clinical/Lab: 8 clicks
Interactively checks patient’s data with the AHA Guidelines
Interactively checks patient’s data with the AHA Guidelines
Discharge meds and interventions: 7 clicks
Discharge meds and interventions: 7 clicks
Demographics: 6 clicks
Demographics: 6 clicks
AHA Tool: Simple One-Page, Online Form
American Heart Association Web site. Get With The Guidelines. Available at: http://www.americanheart.org/presenter.jhtml?identifier=1165.

STRIVETM
Rehab/Exercise
Baseline 4-6 Months 9-12 Months Benchmark*
Intervention
0
20
40
60
80
100
SmokingCounsel
LDL-C BPControl
Pro
po
rtio
n o
f P
ati
ents
*Benchmarks established by CMS AND NRMI.Reprinted with permission from the American Heart Association Web site. Get With The Guidelines. Available at: http://www.americanheart.org/presenter.jhtml?identifier=1165.
Get With The Guidelines 12-Month Pilot Results: 85 New England Hospitals
N=1709
STRIVETM
CRUSADE Can Rapid Risk Stratification of Unstable Angina Patients Suppress ADverse Outcomes with Early
Implementation of the ACC/AHA Guidelines
Nationwide quality improvement (QI) initiative– Up to 600 participating hospitals
Collaborative effort between emergency medicine, cardiology, hospital QI, academia, and industry
Focused on improving the care of NSTEMI ACS patients
Adapted from CRUSADE Overview 2004. Available at: http://www.crusadeqi.com.© 2005 Duke Clinical Research Institute. Used with permission.

STRIVETM
CRUSADE: Inclusion Criteria Ischemic symptoms lasting >10 minutes within previous 24
hours and at least one of the following:
– Positive cardiac markers CK-MB or Tnl/TnT above ULN Positive bedside troponin assay
– ST-segment ECG changes ST-segment depression >0.5 mm Transient ST-segment elevation 0.6–1 mm (lasting
<10 mins)
Transfer patients (with any of the above) must arrive at CRUSADE hospital within 24 hours of symptoms
© 2005 Duke Clinical Research Institute. Used with permission. Available at http://www.crusadeqi.com.

STRIVETM
Goals for CRUSADE
Aspirin– Clopidogrel
-Blocker Heparin (UFH or LMWH) GP IIb/IIIa Inhibitor
– Cath/PCI
Aspirin Clopidogrel -Blocker ACE Inhibitor Statin/Lipid Lowering Smoking Cessation Cardiac Rehabilitation
Acute Therapy Discharge Therapy
2002 ACC/AHA Guidelines Update. Adapted from 2005 CRUSADE 2nd Quarter Results. Available at: http://www.crusadeqi.com.© 2005 Duke Clinical Research Institute. Used with permission.
Improve Adherence to ACC/AHA Guidelines Improve Patient Outcomes

STRIVETM
Hospital Presentation Characteristics in CRUSADE:
July 1, 2005–June 30, 2006 (n=31,665) Qualifying criteriaST-segment depression 28%Transient ST-segment elevation 5%Positive cardiac markers 93%
Baseline cardiac markers DrawnPositive
CK-MB 82%75%TnT/TnI 99%91%
Presenting characteristics Tachycardia 23%Hypotension 4%Signs of CHF 23%Adapted from 2006 CRUSADE Results.
Available at: http://www.crusadeqi.com.© 2006 Duke Clinical Research Institute. Used with permission.

STRIVETM
Baseline Characteristics:CRUSADE vs ACS Clinical Trials
Variable PURSUIT CURE SYNERGY CRUSADE(n = 9461) (n = 12,562) (n = 9975) (n = 180,842)
Mean age ± SD (yrs)63 ± 11 63 ± 12 67 ± 11 67 ± 14
Female sex (%) 36 39 34 40
Diabetes mellitus (%) 23 23 29 33
Prior MI (%) 32 25 28 30
Prior CHF (%) 11 8 9 18
Prior PCI (%) 13 18* 20 21
Prior CABG (%) 12 18* 17 19
ST depression (%) 50 42 55 34
N Engl J Med. 1998;339:436-43.N Engl J Med. 2001;345:494-502.JAMA. 2004:292:45-54.CRUSADE cumulative through June 30, 2006.
N Engl J Med. 1998;339:436-43.N Engl J Med. 2001;345:494-502.JAMA. 2004:292:45-54.CRUSADE cumulative through June 30, 2006.
STRIVETM
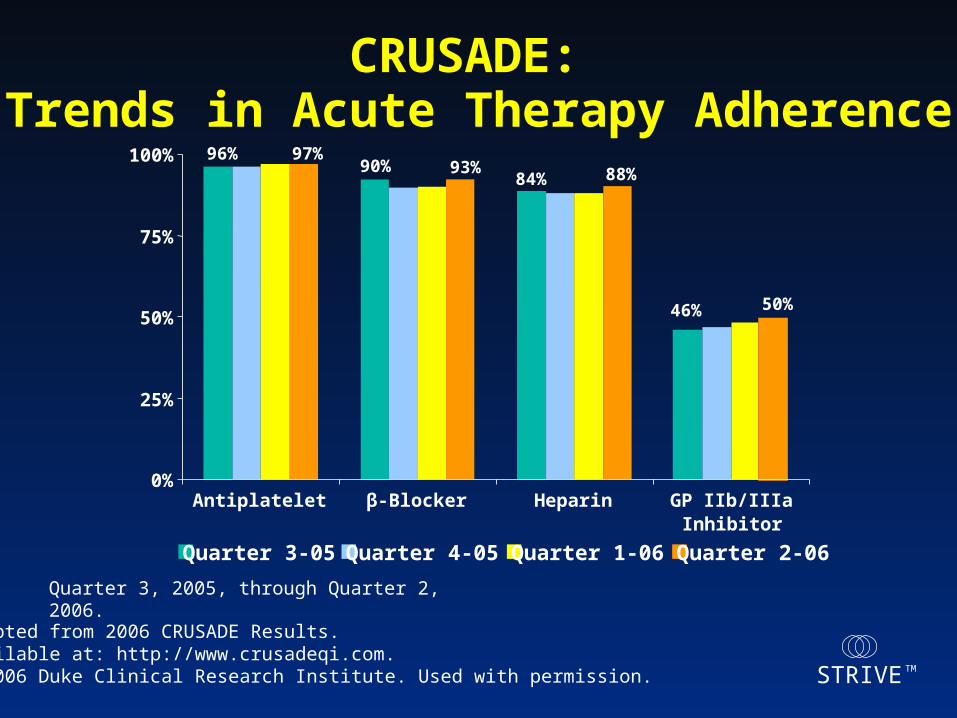
CRUSADE: Trends in Acute Therapy Adherence
Adapted from 2006 CRUSADE Results. Available at: http://www.crusadeqi.com.© 2006 Duke Clinical Research Institute. Used with permission.
96%90%
84%
46%
97%93% 88%
50%
0%
25%
50%
75%
100%
Antiplatelet β-Blocker Heparin GP IIb/IIIaInhibitor
Quarter 3-05 Quarter 4-05 Quarter 1-06 Quarter 2-06
Quarter 3, 2005, through Quarter 2, 2006.

STRIVETM
CRUSADE Data: July 1, 2005-June 30, 2006 (n=31,665)
CRUSADE: Invasive Cardiac Procedures July 1, 2005 – June 30, 2006 (n=31,665)
(Among Patients Without Contraindications to Cath)
Adapted from 2006 CRUSADE Results. Available at: http://www.crusadeqi.com.© 2006 Duke Clinical Research Institute. Used with permission.
83%
67%
53%
38%
12%
0%
20%
40%
60%
80%
100%
Cath Cath<48 hr
PCI PCI <48 hr CABG

STRIVETM
CRUSADE: Trends in Discharge Therapy Adherence
Quarter 3, 2005, through Quarter 2, 2006
Adapted from 2006 CRUSADE Results. Available at: http://www.crusadeqi.com.© 2006 Duke Clinical Research Institute. Used with permission.
94%
72%
91%
64%
89%
74%
94%
66%
88%95%
0%
25%
50%
75%
100%
Aspirin Clopidogrel β-Blocker ACE Inhibitor Lipid- Lowering
Agent
Quarter 3-05 Quarter 4-05 Quarter 1-06 Quarter 1-06

STRIVETM
CRUSADE: Trends in Discharge Recommendations Adherence
84%81%
62%
84%
62%
92%
0%
25%
50%
75%
100%
Smoking CessationCounseling
Dietary Modification Cardiac RehabilitationReferral
Quarter 3-06 Quarter 4-06 Quarter 1-06 Quarter 2-06
Quarter 3, 2005, through Quarter 2, 2006. Adapted from 2006 CRUSADE Results. Available at: http://www.crusadeqi.com.© 2006 Duke Clinical Research Institute. Used with permission.

STRIVETM
CRUSADE: Overall Guideline Adherence Trends Over Time
Available at www.crusadeqi.com © 2006 Duke Clinical Research Institute. Used with permission.
Quarter 1 2002
Quarter 12003
Quarter 12004
Quarter 12005
Quarter 22006
68.1%73.0%
78.0%80.8% 83.2%
0%
25%
50%
75%
100%

STRIVETM
Performance Matters! Association Between Hospital Guideline
Adherence and In-hospital Mortality in CRUSADE
Adapted with permission from Peterson ED, et al. JAMA.2006;295:1912-1920.
NSTE ACS = non-ST-segment elevation ACS; NSTEMI = non-ST-segment elevation MI.
8
7
6
5
4
3
2
1
01 2 3 4
In-H
osp
ital
Mo
rtal
ity
, %
Hospital Composite GuidelineAdherence Quartiles
NSTE ACS 8
7
6
5
4
3
2
1
01 2 3 4
In-H
osp
ital
Mo
rtal
ity
, %
Hospital Composite GuidelineAdherence Quartiles
NSTEMI
CRUSADE = Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes With Early Implementation of the ACC/AHA Guidelines.

STRIVETM
NRMI. Available at: http://www.nrmi.org/index.html. Get With The Guidelines. Available at: http://www.americanheart.org. ACC National Cardiovascular Data Registry. Available at: http://www.acc.org/ncdr/index.htm. GRACE. Available at: http://www.umassmed.edu/outcomes/grace. CRUSADE. Available at: http://www.crusadeqi.com.REACH. Available at: http://www.REACHregistry.org
Importance of Data-Collection Registries Track adherence to guidelines Support local quality-improvement programs Compare practice patterns/outcomes with national benchmarks Comply with regulatory requirements Provide research data Major data-collection registries
– NRMI– AHA “Get With The Guidelines” Patient Management Tool– ACC National Cardiovascular Data Registry– GRACE– CRUSADE– REACH

STRIVETM
CRUSADE: Latest Results in NSTEMI ACS in US: Conclusions
Care for NSTEMI ACS is improving:– Continued progress in adherence to ACC/AHA Guidelines for
both acute and discharge treatments
– More early cath, leading to earlier discharge
Yet opportunities for improvement persist– Largest gaps: acute GP IIb/IIIa, D/C ACE, clopidogrel
– “Right dosing” to reduce adverse events
And can lead to even better patient outcomes!
Available at www.crusadeqi.com.© 2005 Duke Clinical Research Institute. Used with permission.

STRIVETM
Conclusions Gap between knowledge of guidelines
and practice
Several studies show:– Critical pathways interventions improve
care and improve patient outcomes
Need local champions, implementation plan, and action!







