Strokes (Ischemic) in Childrenby
Dr. Azher ShahAssociate Professor
Department of Paediatric MedicineAzra Naheed Medical College, Lahore
Introduction
Stroke is the acute neurologic injury that occurs as a result of either Brain Ischemia or Brain Haemorrhage
Approximately 80 percent of strokes are due to Ischemic Cerebral Infarction and 20 percent due to Brain Haemorrhage
Introduction
More common in older adults, stroke also occurs in neonates, infants, children, and young adults, resulting in significant morbidity and mortality
Annual incidence rates of arterial ischemic stroke (AIS) in infants and children range from 0.6 to 7.9/100,000 children per year
Paediatric ischemic stroke is more common in boys than in girls
Etiology
Etiologies and risk factors for arterial ischemic stroke (AIS) in children differ from those in older adults • Congenital and acquired heart problems• Hematologic conditions• Vasculopathies• Metabolic disorders• Drug ingestion
Children
Etiology (Cont…)
Older Adults
• Hypertension• Smoking• Diabetes• Hypercholesterolemia
Risk Factors in ChildrenCardiac abnormalities
Vascular lesions
Hematologic abnormalities
Infection
Head and neck trauma
Genetic conditions
Clinical Features
Infants
• Focal weakness• Seizures• Altered mental status
Clinical Features (Cont…)
Older Children
• Hemiparesis• Focal neurologic signs such as aphasia, visual
disturbance• Cerebellar signs• Seizures, headache and lethargy• Neck pain (with cervical artery dissection)• Horner's syndrome (carotid dissection)
Differential Diagnoses
Vascular Abnormalities
• Intracranial haemorrhage• Aneurysm• Arteriovenous malformation• Cerebral venous sinus thrombosis
Differential Diagnoses (Cont…)
Nonvascular Conditions
• Intracranial infection (brain abscess or meningoencephalitis)• Demyelinating conditions (such as acute disseminated
encephalomyelitis)• Tumours and other structural brain lesions• Prolonged postictal paresis (Todd's paralysis)• Complicated migraine• Familial alternating hemiplegia• Reversible posterior leukoencephalopathy syndrome• Metabolic stroke• Drug toxicity• Postinfectious cerebellitis• Psychogenic conditions
Evaluation
Urgent Neuro-imaging
• Cardiac• Vascular• Hematologic risk factors
Thorough investigation for
Evaluation (Cont…)
Neuroimaging • Brain CT is generally considered inadequate to diagnose stroke• MRI may be required to reliably exclude stroke mimics• Brain MRI is more sensitive for acute ischemia than CT• Brain MRI provides better visualization of the posterior fossa
MRI Brain or CT Brain
Magnetic resonance angiography (MRA) of the head
MRA of the neck to evaluate the extracranial large arteries
Evaluation (Cont…)
Laboratory studies
• Complete blood count including platelets • Prothrombin time (PT) and international normalized ratio (INR) • Partial thromboplastin time (PTT) • Electrolytes, urea nitrogen, creatinine • Liver function tests• Serum glucose • Hemoglobin electrophoresis in patients with possible sickle cell disease
Evaluation (Cont…)
Laboratory studies
• Electrocardiogram (ECG)• Oxygen saturation • Transthoracic echocardiography • Holter monitoring - if there is suspicion for cardiac arrhythmia, particularly atrial fibrillation • Electroencephalogram (EEG) - if seizures are suspected• Lumbar puncture – if infection is suspected• Toxicology screen – if drug ingestion is suspected
Evaluation (Cont…)
Laboratory studies
• Hypercoagulable evaluation • Protein C functional • Protein S free and total or protein S functional • Antithrombin III activity • Lipoprotein (a) • Homocysteine • Prothrombin gene mutations • Factor V Leiden gene mutation • Anticardiolipin antibodies (IgG and IgM) • Beta2-glycoprotein I antibodies (IgG and IgM) • Lupus anticoagulant tests, including dilute Russell viper venom time and dilute activated PTT • Factor VIII activity • D-dimer

Evaluation (Cont…)
Laboratory studies
• Evaluation for the Vasculitis • Erythrocyte sedimentation rate• C-reactive protein level • Antinuclear antibody assay • Varicella titers • Cerebral digital subtraction angiography
Initial Management
Supportive Measures
• Maintain airway, breathing, and circulation (ABCs) • Maintain normoglycemia and normothermia; start
normal saline intravenously at maintenance rate • Allow modest hypertension • Perform frequent neurologic checks • Begin respiratory and oxygen saturation monitoring-
keep oxygen saturation >95 percent • Utilize cardiac monitoring for the first 24 hours• Patient should be positioned as flat as possible in bed
for at least the first 24 hours from stroke onset, ideally with head-of-bed elevation kept between 0 and 15 degrees
Initial Management (Cont…)
Thrombolysis
• Start venous thromboembolism prophylaxis for patients restricted to bed• Alteplase (rt-PA)
GuidelinesDifferences among consensus guidelines regarding the initial treatment of children with acute arterial ischemic stroke
American Academy of Chest Physicians (ACCP) recommends either unfractionated heparin or low molecular weight heparin (LMWH) or aspirin as initial therapy until dissection and embolic causes have been excludedAmerican Heart Association Stroke Council guideline states that it may be reasonable to initiate anticoagulation with LMWH or unfractionated heparin in children with arterial ischemic stroke pending completion of the diagnostic evaluation
The Royal College of Physicians recommends initial therapy with aspirin
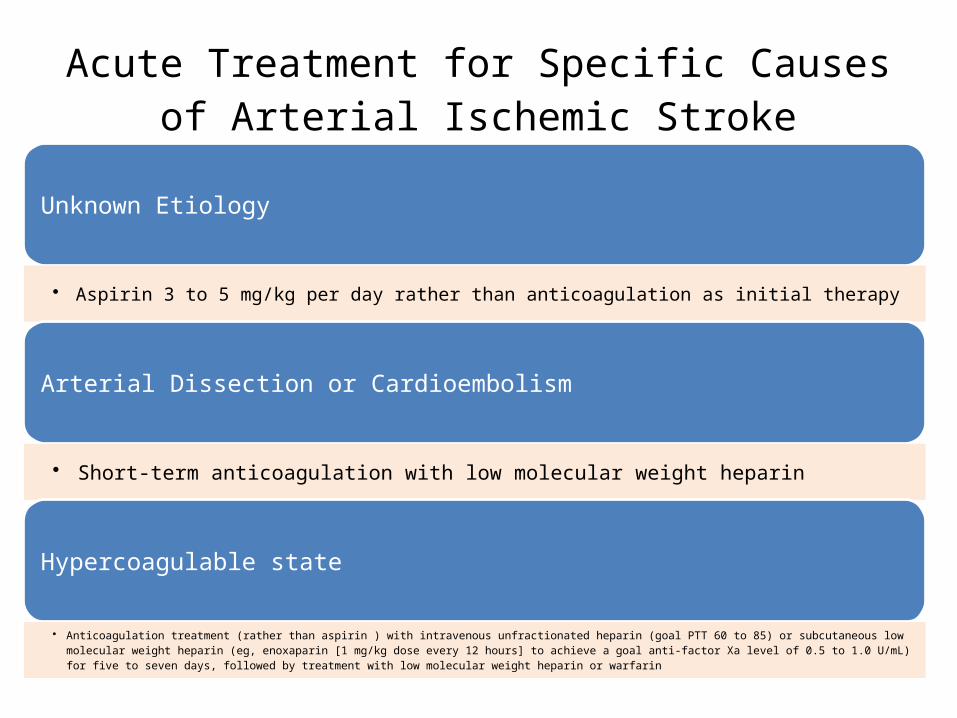
Acute Treatment for Specific Causes of Arterial Ischemic Stroke
Unknown Etiology
• Aspirin 3 to 5 mg/kg per day rather than anticoagulation as initial therapy
Arterial Dissection or Cardioembolism
• Short-term anticoagulation with low molecular weight heparin
Hypercoagulable state
• Anticoagulation treatment (rather than aspirin ) with intravenous unfractionated heparin (goal PTT 60 to 85) or subcutaneous low molecular weight heparin (eg, enoxaparin [1 mg/kg dose every 12 hours] to achieve a goal anti-factor Xa level of 0.5 to 1.0 U/mL) for five to seven days, followed by treatment with low molecular weight heparin or warfarin
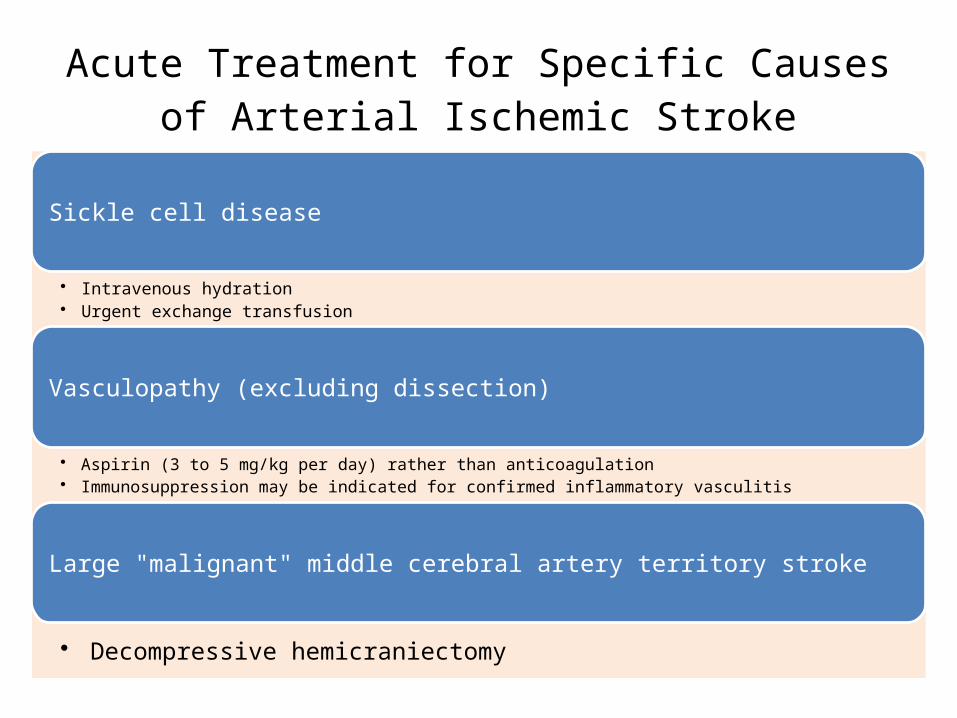
Acute Treatment for Specific Causes of Arterial Ischemic Stroke
Sickle cell disease
• Intravenous hydration• Urgent exchange transfusion
Vasculopathy (excluding dissection)
• Aspirin (3 to 5 mg/kg per day) rather than anticoagulation• Immunosuppression may be indicated for confirmed inflammatory vasculitis
Large "malignant" middle cerebral artery territory stroke
• Decompressive hemicraniectomy
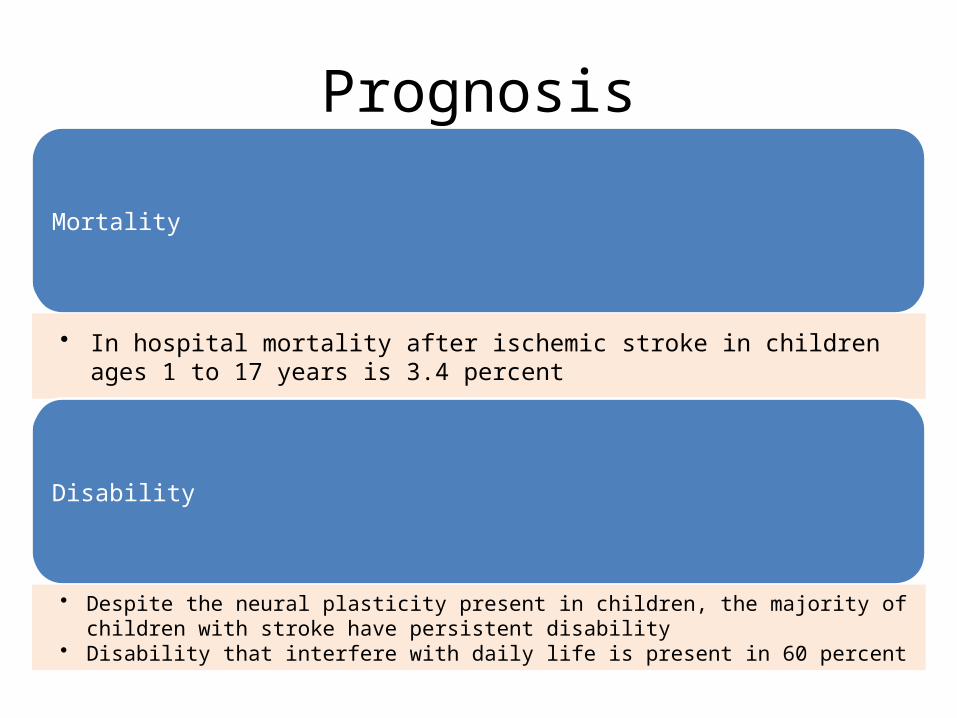
Prognosis
Mortality
• In hospital mortality after ischemic stroke in children ages 1 to 17 years is 3.4 percent
Disability
• Despite the neural plasticity present in children, the majority of children with stroke have persistent disability
• Disability that interfere with daily life is present in 60 percent
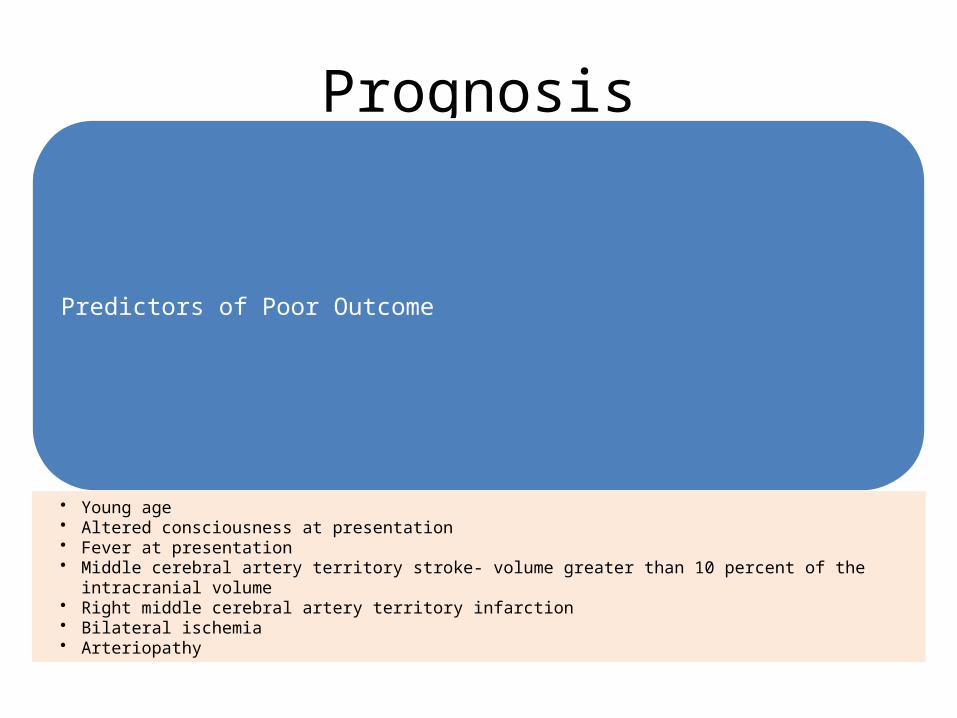
Prognosis
Predictors of Poor Outcome
• Young age • Altered consciousness at presentation • Fever at presentation • Middle cerebral artery territory stroke- volume greater than 10 percent of the intracranial volume • Right middle cerebral artery territory infarction• Bilateral ischemia• Arteriopathy
SummaryStroke in Childhood is acute neurological injury, mainly due to Brain Ischemia
Neuoimaging is the most important aspect of evaluation
Supportive measures are necessary during initial management
Thrombolytic therapy is still controversial in children
There is very high rate of disability after stroke

![Azra [broj 793, 9.5.2012]](https://cdn.vdocuments.net/doc/165x107/5536010c550346640d8b4786/azra-broj-793-952012.jpg)

![Azra [broj 699, 21.7.2010]](https://cdn.vdocuments.net/doc/165x107/5536e67e55034650678b4c00/azra-broj-699-2172010.jpg)

![Azra [broj 928, 10.12.2014]](https://cdn.vdocuments.net/doc/165x107/577cc1a81a28aba711939edc/azra-broj-928-10122014.jpg)

