Download - surgical management of acne scars

DERMATOSURGICAL PROCEDURES FOR ACNE SCARS
DR SWATHY LEKSHMI J L
PATHOGENESIS
Inflammation
Granulation tissue formation
Matrix remodelling
• Proliferation of P.acne• Stimulation of innate immune response
• Activation of complement• Inflammation
• Inflammation extends to dermis • Degradation of dermal matrix
GRANULATION TISSUE
Shift in the balance of collagen type
Type 1 collagen- 80%

MATRIX REMODELLING
Activation of Nf-kb & Aps
Up regulation of MMPs
Procollagen synthesis

CLASSIFICATION OF ACNE SCARS
MACULAR
Erythematous
Hyperpigmented
Depressed
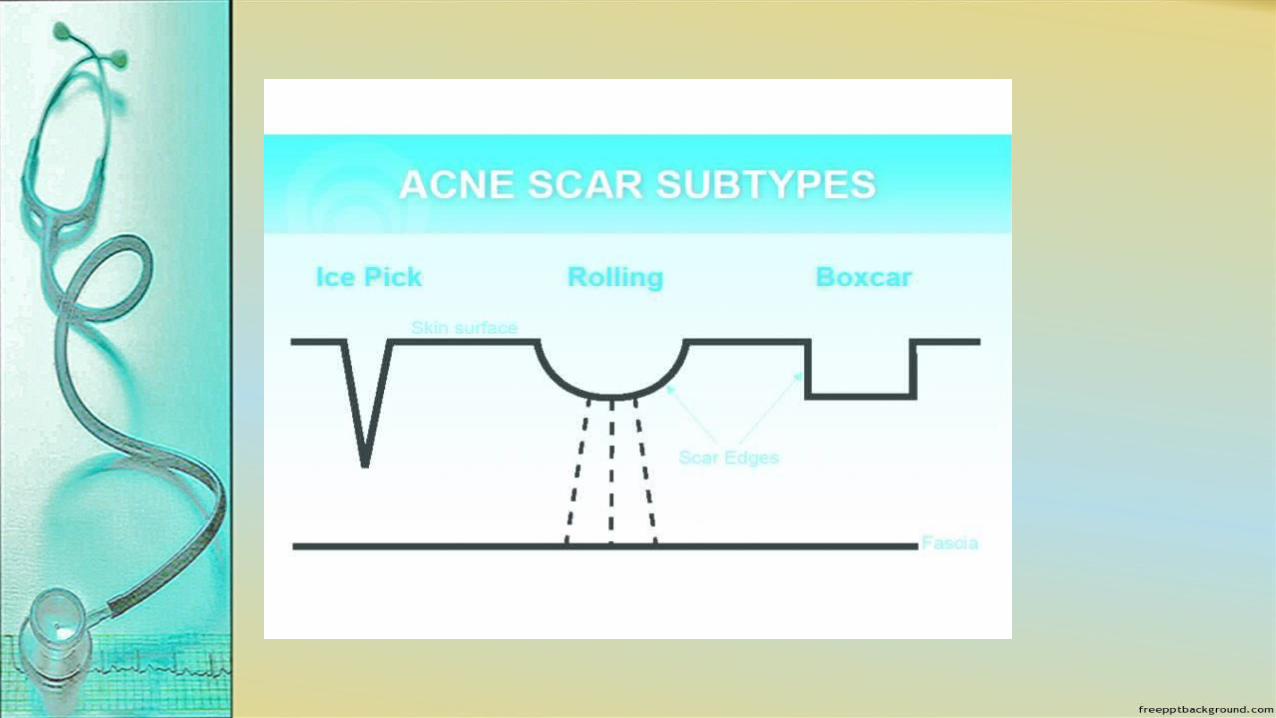
Ice pick- Depressed scars
wider at surface
narrower at base

Rolling- Distensible,
depressed scars with
sloping edges
Boxcar – Shallow or
deep, punched out
scars, wide at surface
and base

ELEVATED
Hypertrophic-Elevated fibrotic scars
Mandibular area, back

Keloidal-Back and
chest
Papular-Raised,
papular and fibrotic
Chin and nose
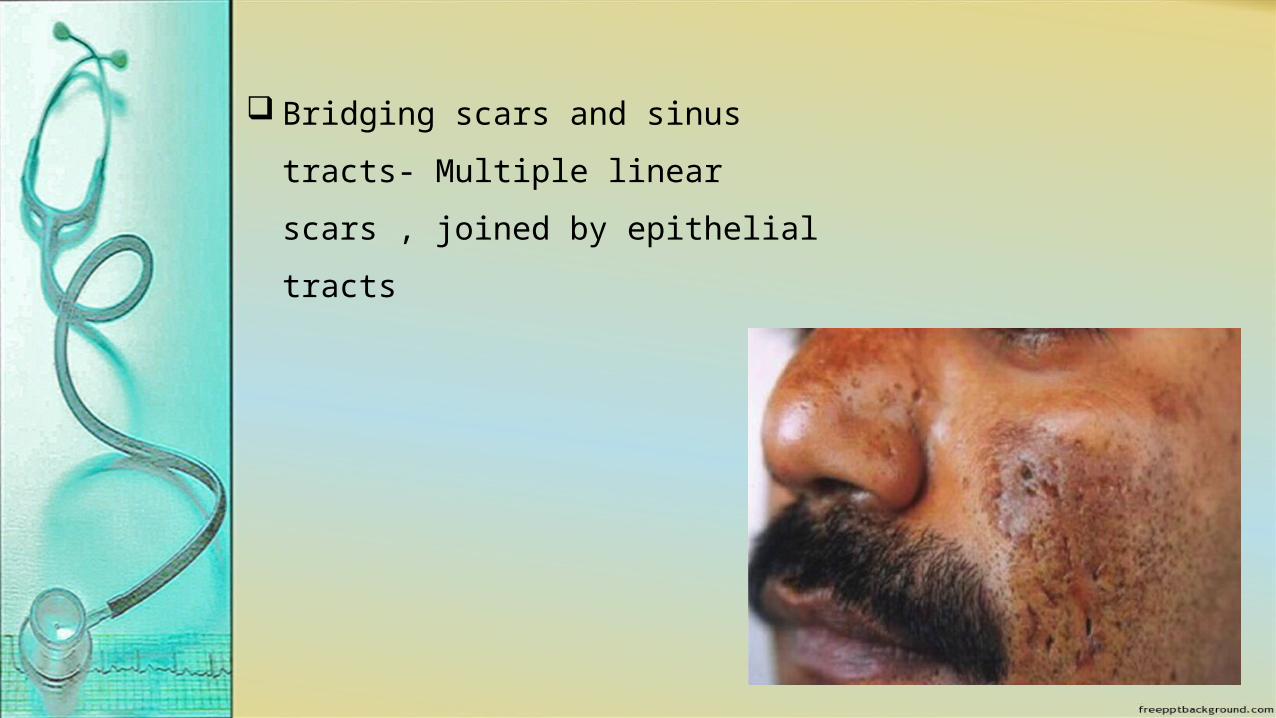
Bridging scars and sinus tracts-
Multiple linear scars , joined by
epithelial tracts
Surgical procedures

PREOPERATIVE ASSESSMENT
HISTORY
HSV infection
Recent use of Isotretinoin
Keloidal tendency
Current medication
Previous surgery
Degree of sunexpusre
Immunocompromising condition

EXAMINATION
General
Skin type
Keloid or Hypertrophic scar
Presence of infection
Activity of acne
Antiviral therapy 2 days prior and for 7-10 days after
procedure
Sun screen, HQ, Glycolic acid
Consent form
Photograph- mandatory for resurfacing with laser,
dermabrasion, chemical peels
Microneedling
Subcision
Punch technique
TCA CROSS
Dermal grafting
Indication
Rolling and Boxcar scars
MICRONEEDLING
CONTRAINDICATION
Active herpes labialis
Keloidal tendency
Isotretinoin therapy in the preceeding 6 months
Bleeding disorders
DERMAROLLER
Drum shaped roller
192 microneedles of 0.1 mm dia.
Needle length 0.5 – 2 mm
Motorised Dermastamps & Home
care dermastamps
PROCEDURE
Topical anaesthesia
Stretch the skin perpendicular to direction of movement of
derma roller
Roll the tool 4 times in 4 different directions
250-300 Pricks/cm sq.
Needle penetrates at an angle, then goes deeper, and
extracted at a converse angle
End point- uniform bleeding points over scarred area

POST PROCEDURE
Clean with NS
Oral analgesic
No need of phtoprotection
3-4 sessions at 4-8 wks intervals


SUBCISION
HISTORY
1957- Spangler
1995- David Orentreinch and Norman Orentreinch
Subcutaneous incisionless surgery

PRINCIPLE
Releasing fibrotic strands underlying scars
Organization of blood in the induced dermal
pockets
Connective tissue formation in the area

INDICATION
Rolling scars
PROCEDURE
Mark the scar
Local infiltration anaesthesia
18 G,1.5 inch Nokor Admix
needle
Insert the needle at periphery of scarred area
Move back and forth, fanlike motion
Firm pressure for 5 mts.
Avoid preauricular, temporal and mandibular areas

Repeat at 6 wkly intervals
2-3 sessions
COMPLICATIONS
Bleeding
Hematoma
Hypertrophic scarring
Scar recurrence

PUNCH EXCISION AND CLOSURE
Ind- Ice pick and Boxcar scars
PROCEDURE
Local anaesthesia
Select appropriate size punch
Traction at right angles to RSTL
Descend upto s/c fat and excise scar plug
Undermine the wound edges
Suture


PUNCH INCISION AND ELEVATION [Punch floatation]
Depressed scars with normal surface texture
Boxcar scar>3mm

PROCEDURE
Punch that match to inner dia. of crateriform scar
Rotating motion release bound down scar
Elevate the plug and free from underlying tissue
Elevate the plug and position to lie slightly higher than
surrounding skin
Secure in position by cyanoacrylate tissue adhesive
PUNCH REPLACEMENT AND GRAFTING
INDICATION
Deep irregular pits
Tethered boxcar scars with altered skin texture
PROCEDURE
Scar plug is removed and graft is transferred to the
plug site
Donor site- post auricular area and inner arm
Donor punch graft size> 0.5mm larger

CROSS
Technique using high strength TCA focally on atrophic acne
scars to induce collagenisation and cosmetic improvement
PRINCIPLE
Precipitation of proteins
Coagulative necrosis of epidermal cells and collagen
Dermal remodelling
INDICATION
Ice pick scars
PROCEDURE
Mark the scar
Clean with spirit and degrease with acetone
Patient in sitting position
Stretch the skin and apply 100% TCA focally
Avoid spillage
Keep the skin stretched until frosted
Wash the face
Photo protection
3 sessions , 4 wkly intervals
COMPLICATIONS
Transient post inflammatory hyper& hypo pigmentation
Priming skin with HQ and tretinoin for 2 wks

DERMAL GRAFTING
Placing dermal grafts into precise pockets under skin
ADVANTAGES
Not susceptible to infection
Can be tailored accurately
Creates a permanent space
Readily available
Easy to perform

PROCEDURE
Conventional
Enzymatic
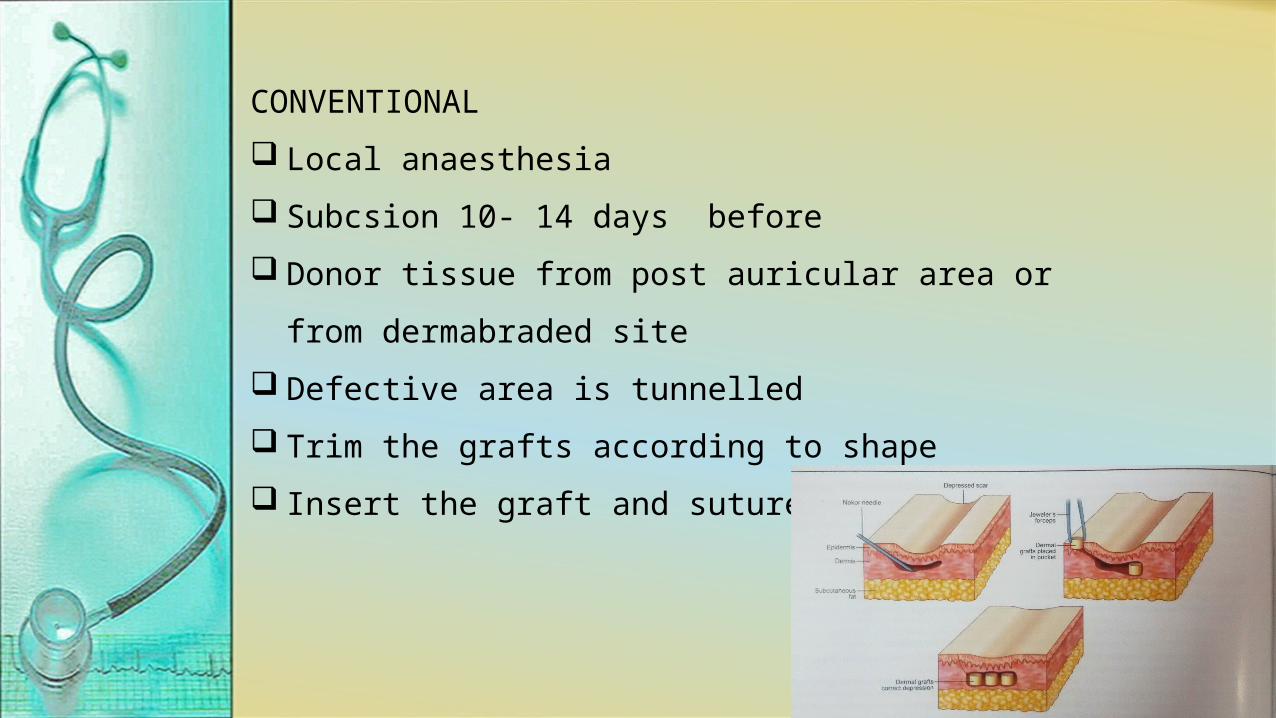
CONVENTIONAL
Local anaesthesia
Subcsion 10- 14 days before
Donor tissue from post auricular area or from
dermabraded site
Defective area is tunnelled
Trim the grafts according to shape
Insert the graft and suture slit

ENZYMATIC TECHNIQUE
Graft in 0.25% trypsin in EDTA solution
Incubate at 37⁰ C for 75 mts.
Transfer to phosphate buffered saline and remove
epidermis
Insert the graft by conventional technique
or inject using a wide bore needle
RESURFACING TECHNIQUES

CHEMICAL PEELING
Salicylic acid 20-30%- active acne and
superficial scars
TCA 10%, 15%, 25%
Glycolic acid 25-35%
Jessener’s peel
Medium depth & deep phenol peels –
effective but not recommended

ABLATIVE
DERMABRASION
Ind- superficial acne scars
Spot dermabrasion can be done in office setting
Full face dermabrasion needs an operation theatre facility
Topical or infiltrative anaesthesia
Mark scars and stretch the skin
Dermabrade till the base of scars
Maximum level- Jn of upper and mid reticular dermis
Manual dermabrader to feather the edges

Hemostasis
Non adherent dressing for 1 wk
COMPLICATIONS
Infections
Persistent dyschromia
Hypo/ hyper pigmentation
Erythema & scarring

LASER ABLATION
CO2 laser (10,600nm)
Er: YAG laser (2940nm)
RESUEFACING – NON ABLATIVE OR MINIMALLY ABLATIVE

MICRODERMABRASION
Superficial minimally invasive technique of mechanical
abrasion of skin using a pressurised stream of abrasive
particles
Aluminium oxide crystals
Disposble diamond tip
Ind- Superficial scars
CI- Active infection
Concurrent dermatoses on face
Eye protection
Set machine parameters with pr. level 10-30 mm of Hg
Stretch the skin under tension
Move the hand piece in a sweeping, outward motion
2nd pass in a direction perpendicular to first pass except in
neck
End point- erythema
Topical antibiotic
Repeated weekly
COMPLICATION
Erythema, oedema, infection, purpura,
pigmentary changes and scarring
Conjunctival congestion
Crystal adherence to cornea
SPK

DISADVANTAGES
Does not improve deep scars
Multiple sittings
Maintenance therapy

NON ABLATIVE RESURFACING LASERS
Ind- atrophic acne scars
Nd :YAG LASER(1320 nm, 1064 nm)
Diode laser(1450 nm)
Flash lamp pumped pulsed dye laser(585 nm)
Er: glass laser

SOFT TISSUE AUGMENTATION
Ind- soft atrophic scars with loss of dermal tissue
Dermal filers are placed under scars
Elevate and bring the surface of scar in level with
surrounding skin
Subcsion or microneedling can be done prior
Hyalouronic acid fillers
Autologous fat
PLLA
Calcim hydroxyapatite


INTRALESIONAL STEROIDS AND CYTOTOXICS
Ind- Hypertrophic and keloidal scars
Triamcinolone 10-20 mg/ml + 5FU

SILICONE GEL SHEETING
Useful in flattening keloid and hypertrophic scars
SCAR REVISION
Ind- Linear and extensive scarring
Z, M and Y Plasty
CRYOTHERAPY
Cryoslush
Cryopeel method

FRACTIONAL PHOTOTHERMOLYSIS
Non injured part of skin is the source of keratinocytes
Migration begins within 24 hrs
Keratinocytes facilitate removal of MENDs

NON ABLATIVE
1550nm erbium doped fibre laser
ABLATIVE
Fractional CO2laser
Direct vaporizing effect on epidermis and some part of
dermis
Free of any active acne lesions
No history of keloidal tendency
PROCEDURE
Clean the skin with 70% alcohol
LA cream for 1 hr
No. of passes and fluence depending on skin type &
severity of scarring
Cool the skin with ice packs after procedure
Non comedogenic Abs for 3-5 days +sunscreen

COMPLICATIONS
Erythema and crusting
PIH
Dryness of skin
Pruritus
Bronzing of skin
Aggravation of acne

THANK YOU







