
TOP PAPERS IN PEDIATRIC INFECTIOUS DISEASES
Susanna EspositoPediatric Highly Intensive Care Unit,
University of Milan, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico
Milan, Italy

AGENDA
• Viral infections
• Bacterial infections
• Hot topics in antinfective treatment

VIRAL INFECTIONS
• Ebola virus
• Enterovirus D68
• Rhinovirus
• Parechovirus
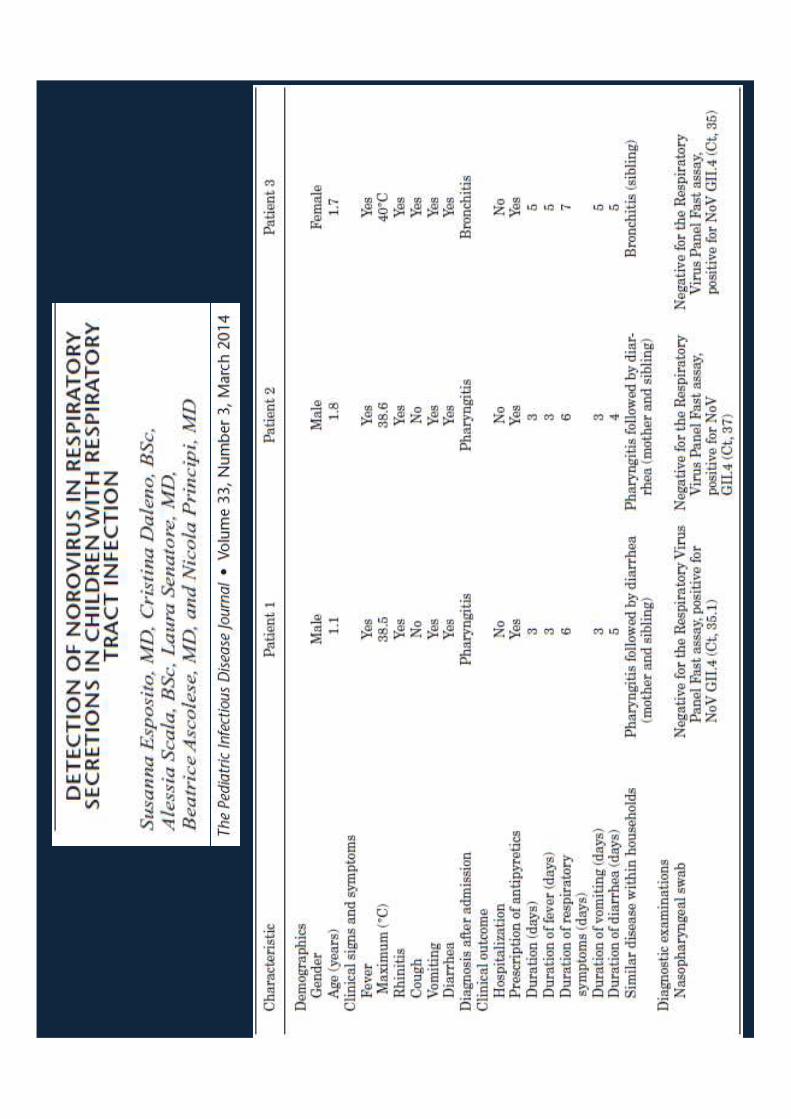
• Norovirus


Pediatric cases of Ebola virus infection(From Agua-Agum J et al., NEJM 2015)
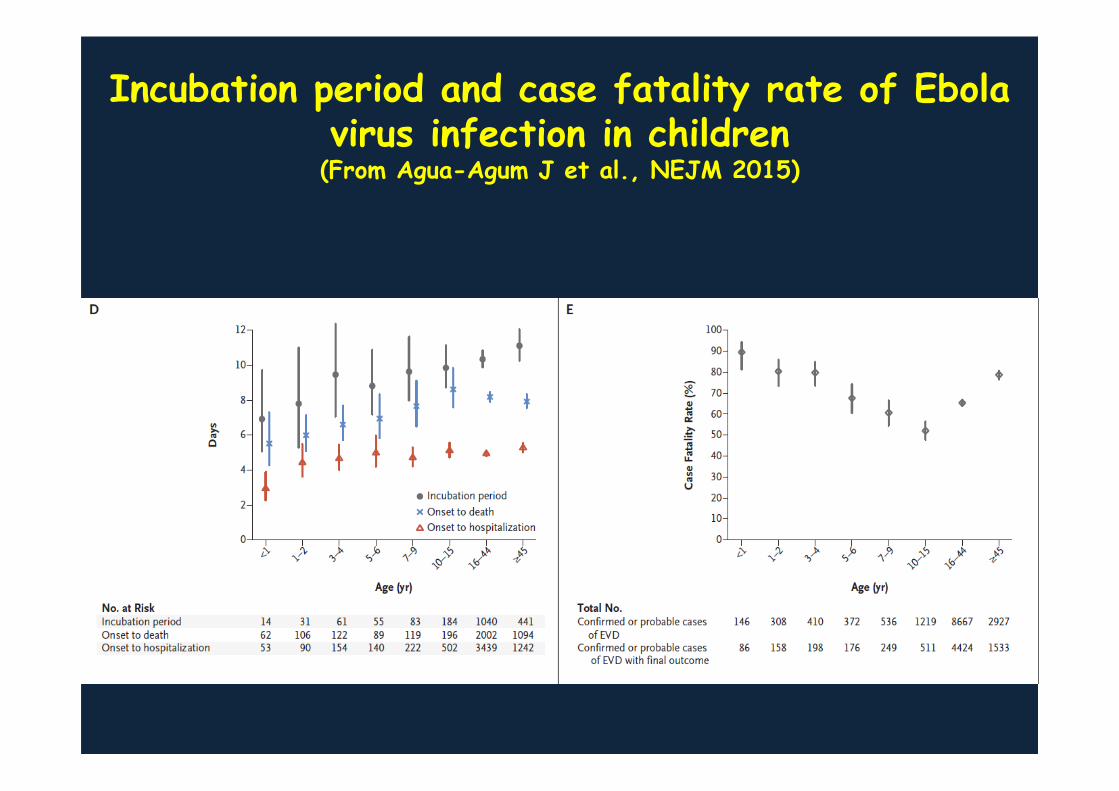
Incubation period and case fatality rate of Ebola virus infection in children(From Agua-Agum J et al., NEJM 2015)


DESCRIPTION OF THE PATIENTS WITH EVD68 INFECTION ASSOCIATED WITH ACUTE FLACCID MYELITIS
(Greninger et al., Lancet Infect Dis 2015)

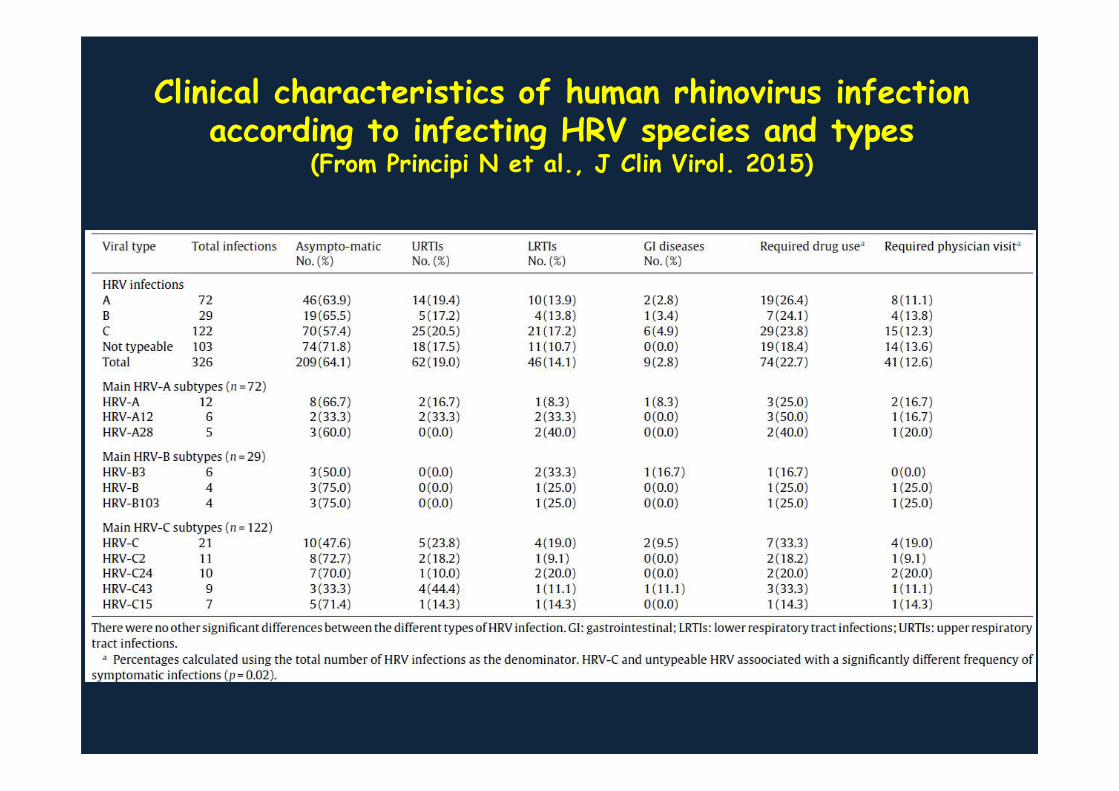
Clinical characteristics of human rhinovirus infectionaccording to infecting HRV species and types
(From Principi N et al., J Clin Virol. 2015)

Median shedding time by type of human rhinovirus(From Principi N et al. , J Clin Virol 2015)

Cases oh human rhinovirus infection with viralshedding of the same viral type ≥3 weeks
(From Principi N et al., J Clin Virol 2015)


Number of confirmed HPeV cases admitted to 5 hospitals in New South Wales each week between
October 2013 to January 2014


Main studies regarding norovirus infection in Europe
(From Kowalzik F et al., Pediatr Infect Dis J 2015)

BACTERIAL INFECTIONS
• MRSA
• Streptococcus pneumoniae• Neisseria meningitidis• ESBL producing Enterobacteriaceae• XDR TB


Proportion of households contaminated with an environmental strain type of Staphylococcus aureus
correlating with the participants’ baseline colonizing or infecting strains type, by household surface
(From Fritz SA et al., JAMA Pediatr 2014)


Predominant organismsaccording to groups
(From Irwin AD et al., Pediatrics 2015)

Proportion of bacteremia episodes of eachisolate according to age group
(From Irwin AD et al., Pediatrics 2015)
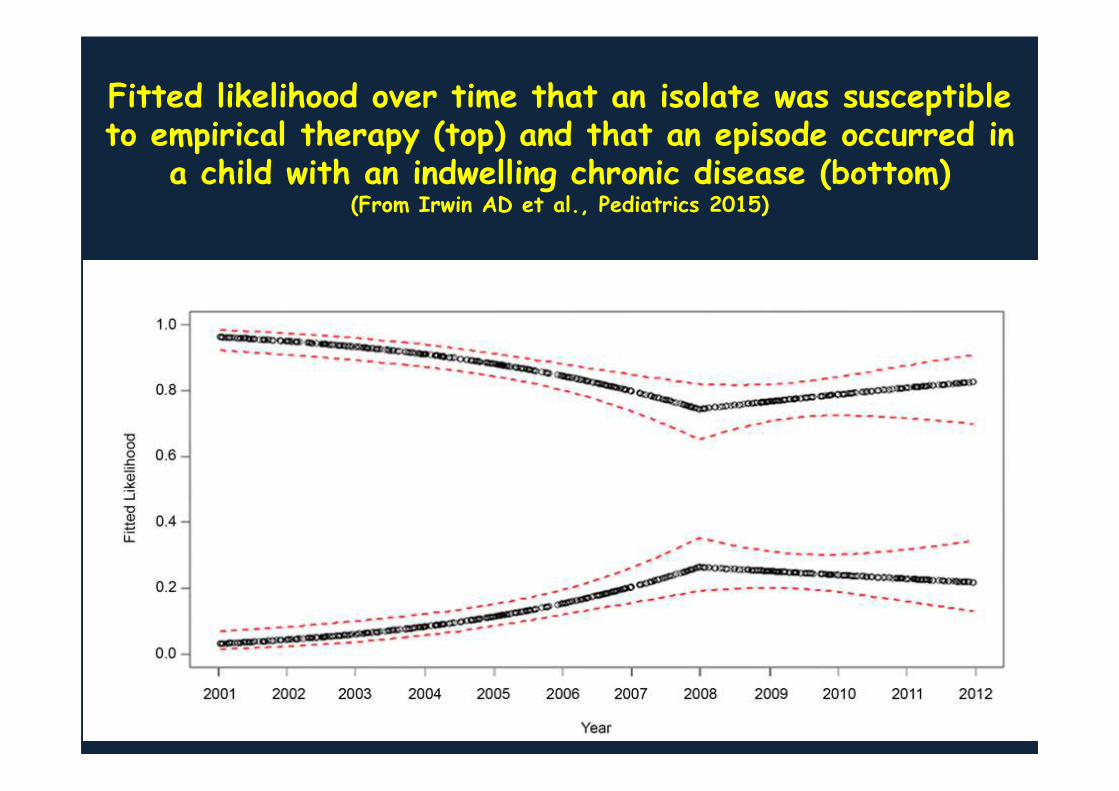
Fitted likelihood over time that an isolate was susceptibleto empirical therapy (top) and that an episode occurred in
a child with an indwelling chronic disease (bottom) (From Irwin AD et al., Pediatrics 2015)

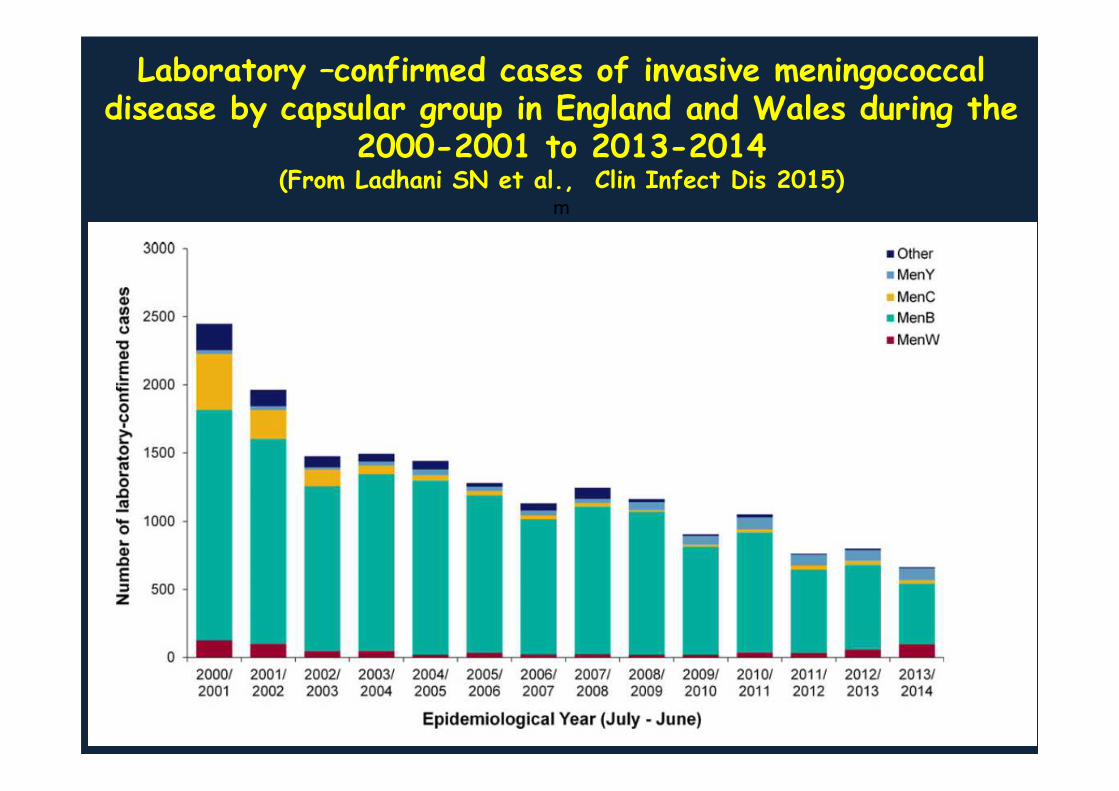
Laboratory –confirmed cases of invasive meningococcaldisease by capsular group in England and Wales during the
2000-2001 to 2013-2014(From Ladhani SN et al., Clin Infect Dis 2015)
m

Laboratory-confirmed cases of invasive meningococcalgroup W disease by phenotype, age groups, and year
of diagnosis in England and Wales (From Ladhani SN et al., Clin Infect Dis 2015)


ESBL producing Enterobacteriaceae in pediatric age(Lukac et al., Clin Infect Dis 2015)
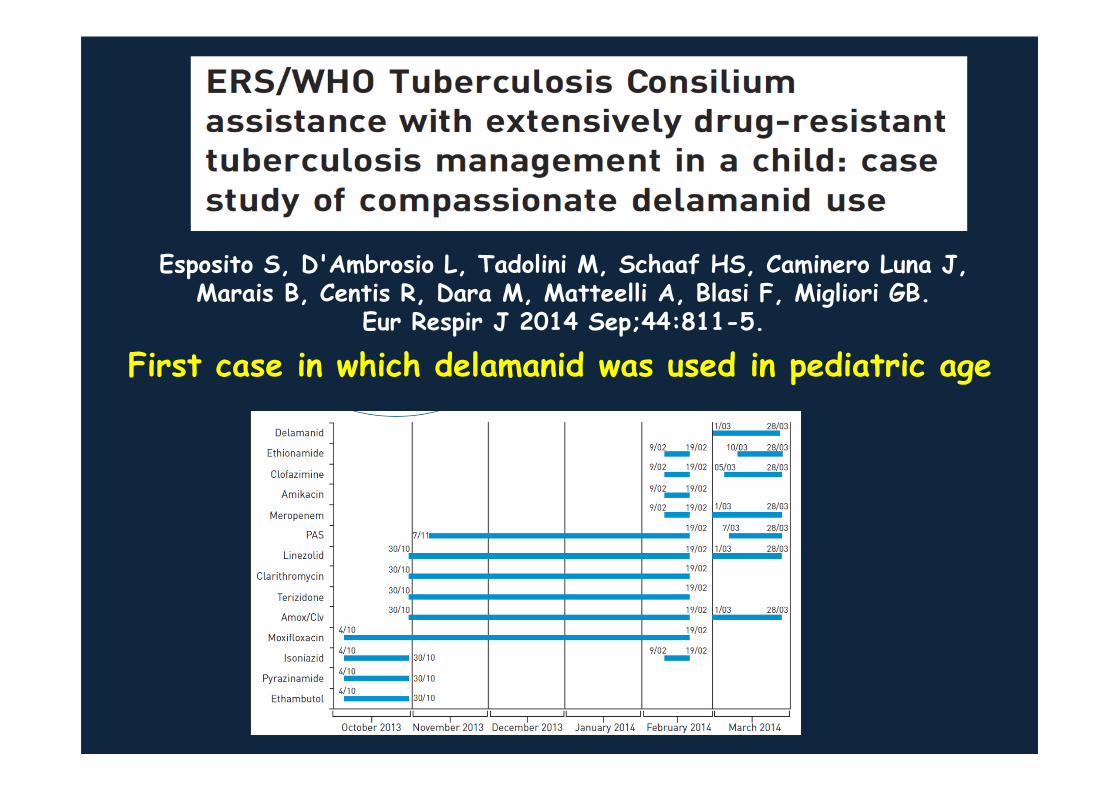
Esposito S, D'Ambrosio L, Tadolini M, Schaaf HS, Caminero Luna J, Marais B, Centis R, Dara M, Matteelli A, Blasi F, Migliori GB.
Eur Respir J 2014 Sep;44:811-5.
First case in which delamanid was used in pediatric age

Index caseFAMILY
Male, 12 yearsLaryngeal + PTBLong diagnostic delayDirect Sputun examination +++Resistant to SHREZ+FQ+Inj+EtoHaarlem strain Mother, TST+, QF+
PTB, immigrant, histopathology+, CXR improved Cat 1
21 classmates tested:1 monolateral pleurisy (immigrant)10 TST+, QF+ (7 native, 3 immigrant)
2 dental hygienists tested: 2TST+, QF+
56 playmates tested:3 TST+, QF-(BCG vaccinated)
24 students tested in parallel class performing common activities:1 TST+, QF+1TST+, QF-
57 students tested in other classes:1TST+, QF+13 TST+, QF-
TB disease TST+, QF+ TST+, QF -
18 school staff tested:4TST+, QF+5TST+, QF-
Sister 6 yrs, PTB
Brother 10 yrs, PTB
Father, TST-, QF-
19 school canteen staff tested:3 TST+, QF -
37 educators tested:1 TST+, QF-
Summer camp circle
27 tested: All TST-, QF-
Sport related circle
Catechism related circle
50 tested: 1 TST+, QF+4 TST+, QF-
Other contacts

HOT TOPICS IN ANTINFECTIVE TREATMENT
• Vancomycin serum concentrations in neonates
• Antimicrobial stewardship programmes• Use of off label antibiotics• Antifungal therapies

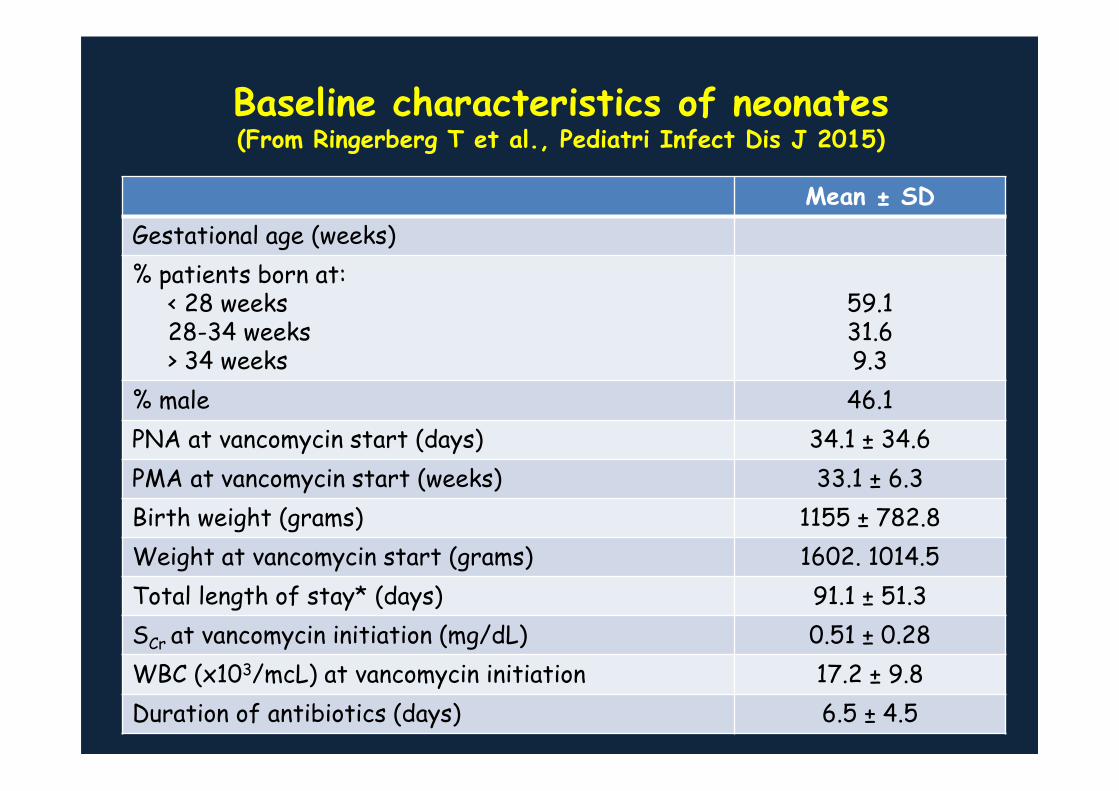
Baseline characteristics of neonates(From Ringerberg T et al., Pediatri Infect Dis J 2015)
Mean ± SD
Gestational age (weeks)
% patients born at:< 28 weeks28-34 weeks> 34 weeks
59.131.69.3
% male 46.1
PNA at vancomycin start (days) 34.1 ± 34.6
PMA at vancomycin start (weeks) 33.1 ± 6.3
Birth weight (grams) 1155 ± 782.8
Weight at vancomycin start (grams) 1602. 1014.5
Total length of stay* (days) 91.1 ± 51.3
SCr at vancomycin initiation (mg/dL) 0.51 ± 0.28
WBC (x103/mcL) at vancomycin initiation 17.2 ± 9.8
Duration of antibiotics (days) 6.5 ± 4.5

Achievement of vancomycin trough concentrations(From Ringerberg T et al., Pediatric Infect Dis J 2015)
Trough value Number of patients(%)
Initial trough (N = 171) 0-10 mcg/mL10-20 mcg/mL> 20 mcg/mL
123 (71.9)43 (25.1)5 (2.9)
Overall trough (N = 168)0-10 mcg/mL10-20 mcg/mL> 20 mcg/mL
92 (54.8)75 (44.6)
1 (0.6)
Dose adjustments to attain trough 10-20 mcg/mL(N = 75)
012
48 (64.0)22 (29.3)5 ( 6.7)
Duration of therapy to achieve trough 10-20 mcg/mL (mean ± SD)
2.27 ± 1.76 days
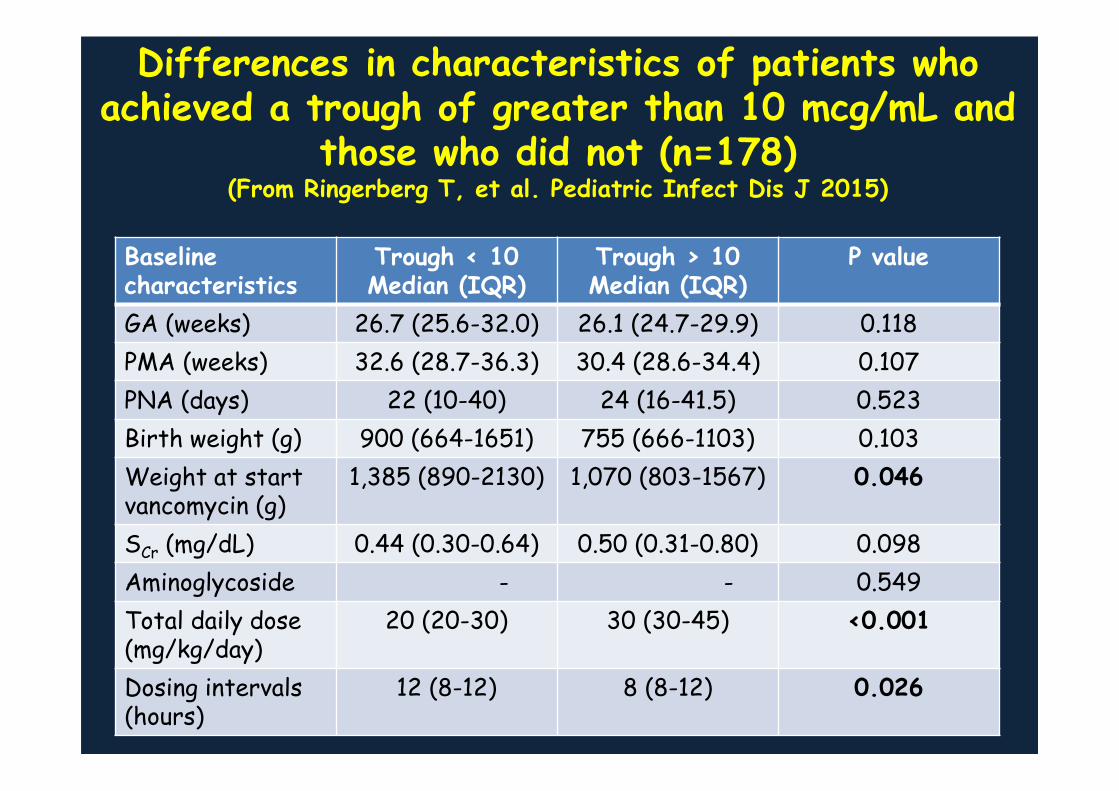
Differences in characteristics of patients whoachieved a trough of greater than 10 mcg/mL and
those who did not (n=178)(From Ringerberg T, et al. Pediatric Infect Dis J 2015)
Baseline characteristics
Trough < 10Median (IQR)
Trough > 10 Median (IQR)
P value
GA (weeks) 26.7 (25.6-32.0) 26.1 (24.7-29.9) 0.118
PMA (weeks) 32.6 (28.7-36.3) 30.4 (28.6-34.4) 0.107
PNA (days) 22 (10-40) 24 (16-41.5) 0.523
Birth weight (g) 900 (664-1651) 755 (666-1103) 0.103
Weight at start vancomycin (g)
1,385 (890-2130) 1,070 (803-1567) 0.046
SCr (mg/dL) 0.44 (0.30-0.64) 0.50 (0.31-0.80) 0.098
Aminoglycoside - - 0.549
Total daily dose(mg/kg/day)
20 (20-30) 30 (30-45) <0.001
Dosing intervals(hours)
12 (8-12) 8 (8-12) 0.026

Pediatrics 2015; January 1

DDT/1000 pts days for all and selected antibioticsfor ASP- (grey lines) and ASP+ (black lines) hospitals
(Hersh et al., Pediatrics 2015)
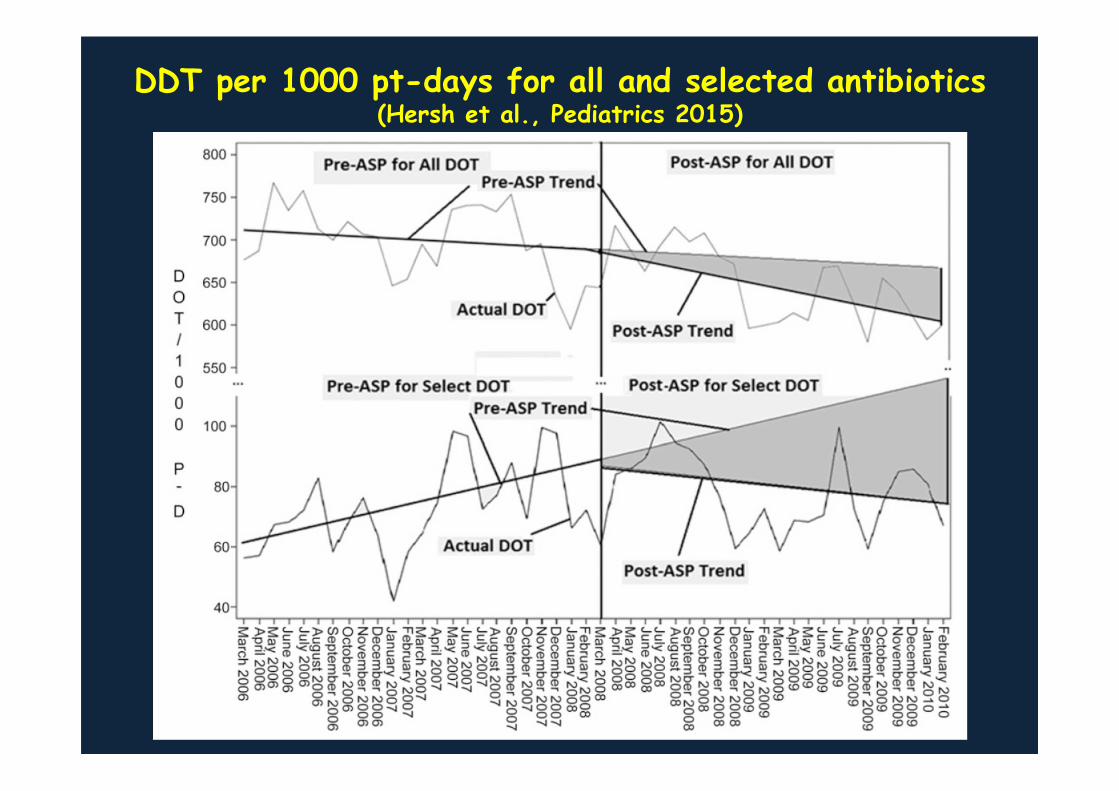
DDT per 1000 pt-days for all and selected antibiotics(Hersh et al., Pediatrics 2015)

SUGGESTED USE OF FLUOROQUINOLONES IN PEDIATRIC AGE
(Principi & Esposito, Int J Antimicrob Agents 2015)


Participantcharacteristics for
receipt of fluconazole vs
placebo
(From Benjamin DK et al.,JAMA 2015)

Safety end points and other secondary end points for receipt of fluconazole vs placebo
(From Benjamin DK et al., JAMA 2015)

Primary and secondaryendpoints and neurodevelopentalendpoints for receipt of fluconazole or placebo
(From Benjamin DK et al.,JAMA 2015)

SEE YOU IN MILAN!
THANK YOU VERY MUCH FOR
YOUR ATTENTION







