
1
Welcome to SECO 2009
SECO 2011March 2-6, 2011
Essentials in Systemic Disease
Carlo J. Pelino, ODJoseph J. Pizzimenti, OD
DISCLOSURE STATEMENT
Please silence all mobile devices
At the conclusion of this course, please properlydispose of your trash as you leave this room
Dr. Pizzimenti is CEO of Optometryboardcertified.comDr. Pizzimenti has received honoaraia from Alcon, Reichert,Zeavision, and Carl Zeiss MeditecDr. Pelino has received honoraria from Carl Zeiss Meditec
• The Eye is an extension of the brainThe Eye is an extension of the brain
•• The anatomy of the eye is structured to serve the functions of the The anatomy of the eye is structured to serve the functions of the ““retinaretina””
•• The primary reason for dilation is to detect systemic disease The primary reason for dilation is to detect systemic disease
RPE and RPE and Choroidal Choroidal pigmentationpigmentationInner and Outer blood retinal barrierInner and Outer blood retinal barrier

2
Iris / Iris / Ciliary Ciliary Body 15%Body 15%
ChoroidChoroid 80% 80%
SympatheticSympatheticControlControl
Retina 5 %Retina 5 %
AutoregulateAutoregulate
Classification of Blood PressureClassification of Blood Pressure (Adults 18 and older) (Adults 18 and older)
CategoryCategory Systolic Blood PressureSystolic Blood Pressure Diastolic Blood PressureDiastolic Blood Pressure
•• NomalNomal < 120 mm Hg< 120 mm Hg < 80 mm Hg< 80 mm Hg
•• PrehypertensionPrehypertension 120-139 mm Hg120-139 mm Hg 80-89 mm Hg80-89 mm Hg
•• Hypertension Hypertension 140-159 mm Hg 140-159 mm Hg 90-99 mm Hg90-99 mm Hg (Stage 1) (Stage 1)
•• Hypertension Hypertension >160 mm Hg >160 mm Hg 100 mm Hg100 mm Hg (Stage 2) (Stage 2)
Source: U.S. Department of Health Services; NIH no. 03-5231 May 2003Source: U.S. Department of Health Services; NIH no. 03-5231 May 2003
Clinical Clinical Ophthalmoscopic Ophthalmoscopic findingsfindings
Grade 1Grade 1 Retinal vessels narrowedRetinal vessels narrowed > 90 and < 110 Diastolic BP> 90 and < 110 Diastolic BP
Grade 2Grade 2 Nicking of retinal vesselsNicking of retinal vessels > 90 and <110 Diastolic BP> 90 and <110 Diastolic BP
Grade 3Grade 3 CWS, CWS, HemesHemes, Lipid exudates, Lipid exudates > 110 > 110 –– 115 Diastolic BP 115 Diastolic BP
Grade 4Grade 4 Grade 3 + Optic disc swellingGrade 3 + Optic disc swelling > 130 Diastolic BP> 130 Diastolic BP
Grading of Hypertensive RetinopathyGrading of Hypertensive Retinopathy
• Grades 3 and 4 = increase risk of cerebral, heart and kidney problemsGrades 3 and 4 = increase risk of cerebral, heart and kidney problems

3
54 year old54 year old
+ Diabetes + Diabetes
+ HTN+ HTN
+ Cholesterol+ Cholesterol

4

5

6
Grade 4 Hypertensive RetinopathyGrade 4 Hypertensive Retinopathy

7
Malignant HypertensionMalignant Hypertension Malignant HypertensionMalignant Hypertension
Malignant HypertensionMalignant Hypertension

8
Malignant HypertensionMalignant Hypertension::
• Defined as Blood Pressure > 210 / 130Defined as Blood Pressure > 210 / 130
Ocular PresentationOcular Presentation: May present with the following: May present with the following
•• Disc Edema Disc Edema•• Arterio-venous Arterio-venous crossing changescrossing changes•• Nerve fiber layer infarcts (cotton wool spots) Nerve fiber layer infarcts (cotton wool spots)•• Macular edema Macular edema•• Hard exudates Hard exudates•• Flame shaped hemorrhages Flame shaped hemorrhages•• Choroidal Choroidal ischemia (usually seen in young patients)ischemia (usually seen in young patients)

9
Malignant HypertensionMalignant Hypertension: Systemic Presentation: Systemic Presentation
• Patient may be asymptomaticPatient may be asymptomatic•• Patient may have encephalopathy, headaches, vomiting or coma Patient may have encephalopathy, headaches, vomiting or coma
Treatment of Malignant Hypertension:Treatment of Malignant Hypertension:
•• Blood pressure measurement Blood pressure measurement•• Immediate referral to emergency room or primary care doctor for Immediate referral to emergency room or primary care doctor for slow loweringslow lowering of the blood pressure !!!!! of the blood pressure !!!!!
•• Visual field testing Visual field testing•• MRI MRI –– to rule out space occupying lesion to rule out space occupying lesion•• MRV- to rule out MRV- to rule out ““ venous sinus thrombosis venous sinus thrombosis ””•• Lumbar puncture if necessary Lumbar puncture if necessary
• Keith et al. found that ~ 80 % of patients with Grade 4 HypertensiveKeith et al. found that ~ 80 % of patients with Grade 4 Hypertensive Retinopathy ( malignant hypertension ) died within 1 year Retinopathy ( malignant hypertension ) died within 1 year
•• Also, over a 3 year period, there was a 95% mortality for those with Also, over a 3 year period, there was a 95% mortality for those with malignant hypertension malignant hypertension
•• HLA B15 has been associated with malignant arterial hypertension. HLA B15 has been associated with malignant arterial hypertension.
HypertensionHypertension: ~ 70 million Americans ~ 70 million Americans
•• Malignant Malignant•• Essential Essential•• Secondary HTN ( Secondary HTN ( PheochromocytomaPheochromocytoma, renal artery , renal artery stenosisstenosis, etc. ), etc. )
Essential HypertensionEssential Hypertension:: defined as a blood pressure > 140 / 90defined as a blood pressure > 140 / 90
••During young adulthood /early middle ageDuring young adulthood /early middle age……HTN is more common in malesHTN is more common in males••Elderly patientsElderly patients……HTN is more common in womenHTN is more common in women
••A family history of HTN usually exists in essential HTNA family history of HTN usually exists in essential HTN••Essential HTN is usually controlled with one or two medicationsEssential HTN is usually controlled with one or two medications••Blood pressure does not progress to higher levels over a short period of timeBlood pressure does not progress to higher levels over a short period of time
••Work Up = BUN/Cr, Lipid Profile, Glucose, CBC, EKG, Work Up = BUN/Cr, Lipid Profile, Glucose, CBC, EKG, ““Metabolic PanelMetabolic Panel””
Secondary HypertensionSecondary Hypertension::
Drugs / ToxinsDrugs / Toxins
Renal DiseaseRenal Disease GlomerulonephritisGlomerulonephritis, Diabetes, Chronic nephritis, Diabetes, Chronic nephritis
VascularVascular Coarctation Coarctation of the aortaof the aorta
NeurologicNeurologic Increased Intracranial Pressure, G-B syndromeIncreased Intracranial Pressure, G-B syndrome
EndocrineEndocrine PheochromocytomaPheochromocytoma, Hypo-Hyperthyroidism, Hypo-Hyperthyroidism
PregnancyPregnancy
StressStress Postoperative, Burns, Postoperative, Burns, Alchohol Alchohol withdrawalwithdrawal
ZoorobZoorob RJ, et al. Hypertension. Prim Care. 2000 Sep;27(3):589-614 RJ, et al. Hypertension. Prim Care. 2000 Sep;27(3):589-614

10
Always question the malignant hypertensive patientAlways question the malignant hypertensive patient
Hypertensive encephalopathyHypertensive encephalopathy•• Syncope Syncope•• Seizures Seizures•• Focal weakness Focal weakness•• ParesthesiasParesthesias•• Speech problemsSpeech problems
Hypertensive Cardiac involvementHypertensive Cardiac involvement•• Chest pain Chest pain•• PalpatationsPalpatations•• Cough Cough•• DyspneaDyspnea
Hypertensive renal problemsHypertensive renal problems•• Change in renal volume Change in renal volume•• HematuriaHematuria, abdominal pain, abdominal pain
2 Months2 Months
BP 125 / 82BP 125 / 82RASRAS
Epiretinal Epiretinal Membrane formationMembrane formation
• Hypertensive Hypertensive ChoroidopathyChoroidopathy

11
Essential HypertensionEssential Hypertension –– Long standingLong standing
Arteriosclerosis Grade 2-3Arteriosclerosis Grade 2-3
Retinal Arterial Retinal Arterial MacroaneurysmMacroaneurysm Retinal Arterial Retinal Arterial MacroaneurysmMacroaneurysm
12
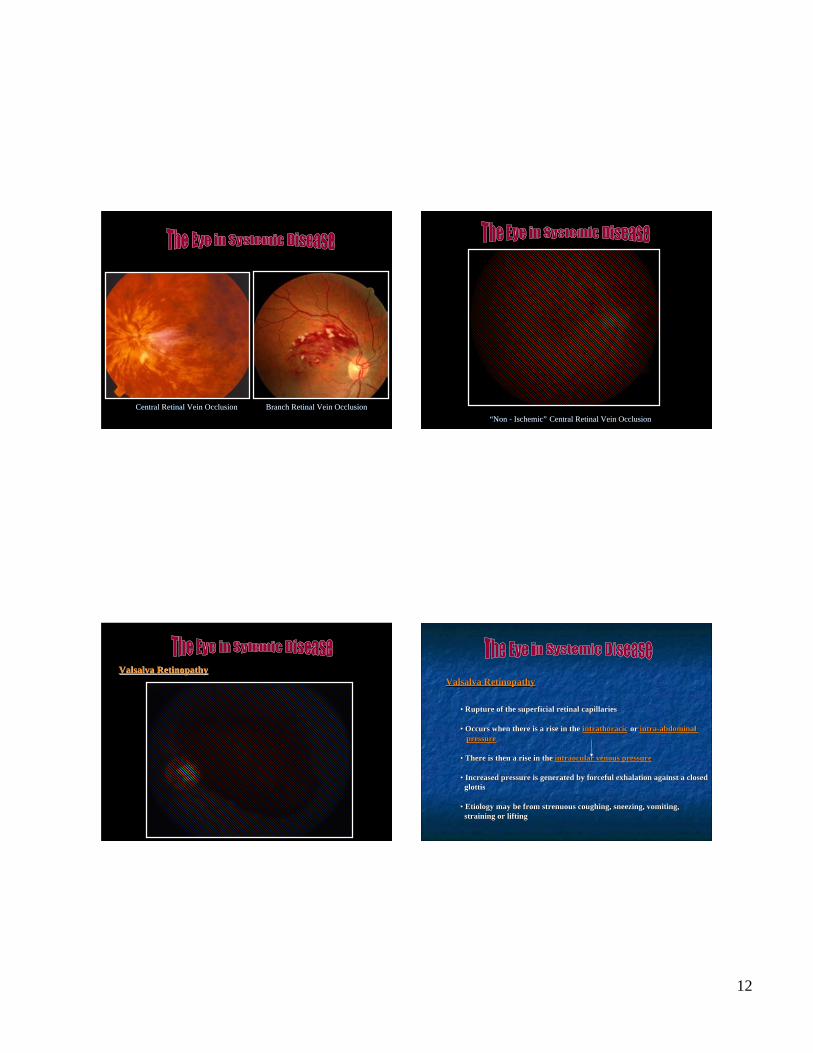
Central Retinal Vein Occlusion Branch Retinal Vein OcclusionCentral Retinal Vein Occlusion Branch Retinal Vein Occlusion““Non - IschemicNon - Ischemic”” Central Retinal Vein Occlusion Central Retinal Vein Occlusion
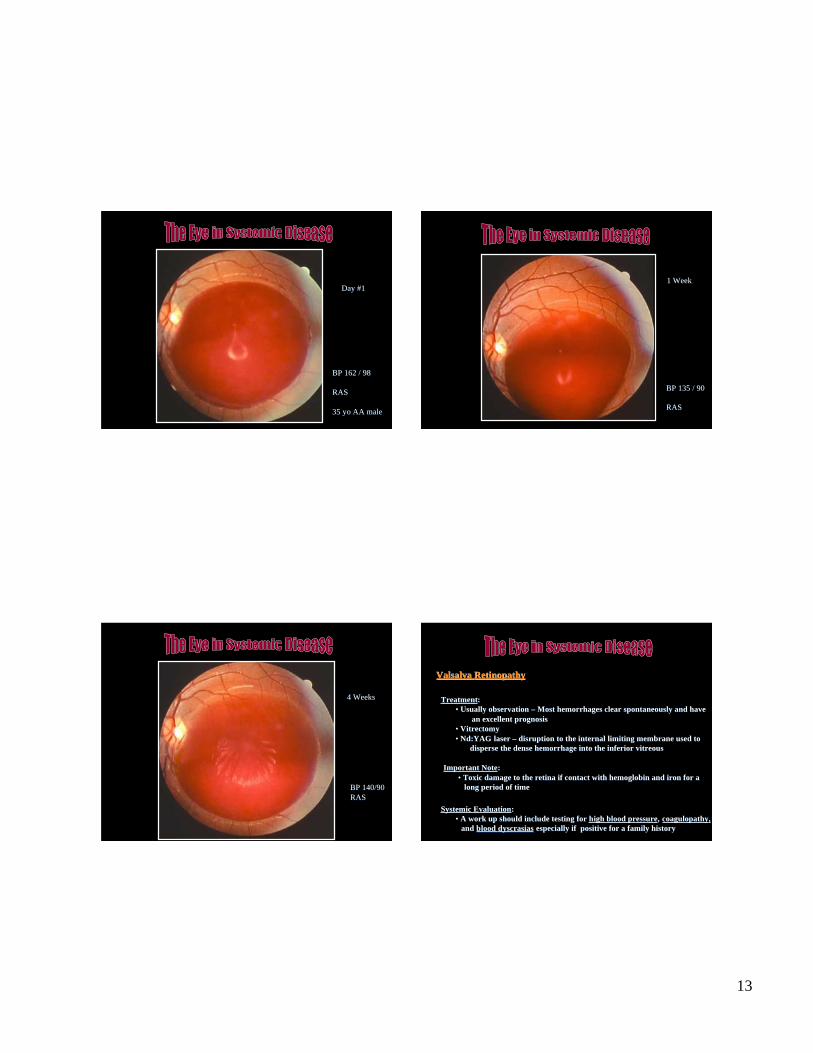
Valsalva Valsalva RetinopathyRetinopathyValsalva Valsalva RetinopathyRetinopathy
• Rupture of the superficial retinal capillariesRupture of the superficial retinal capillaries
•• Occurs when there is a rise in the Occurs when there is a rise in the intrathoracicintrathoracic or or intra-abdominal intra-abdominal pressurepressure
•• There is then a rise in the There is then a rise in the intraocular venous pressureintraocular venous pressure
•• Increased pressure is generated by forceful exhalation against a closed Increased pressure is generated by forceful exhalation against a closed glottis glottis
•• Etiology may be from strenuous coughing, sneezing, vomiting, Etiology may be from strenuous coughing, sneezing, vomiting, straining or lifting straining or lifting
13
Day #1Day #1
BP 162 / 98BP 162 / 98
RAS RAS
35 35 yo yo AA maleAA male
1 Week1 Week
BP 135 / 90BP 135 / 90
RASRAS
4 Weeks4 Weeks
BP 140/90BP 140/90 RAS RAS
Valsalva Valsalva RetinopathyRetinopathy
TreatmentTreatment::•• Usually observation Usually observation –– Most hemorrhages clear spontaneously and have Most hemorrhages clear spontaneously and have an excellent prognosis an excellent prognosis•• VitrectomyVitrectomy•• Nd:YAGNd:YAG laser laser –– disruption to the internal limiting membrane used to disruption to the internal limiting membrane used to
disperse the dense hemorrhage into the inferior vitreousdisperse the dense hemorrhage into the inferior vitreous
Systemic EvaluationSystemic Evaluation::•• A work up should include testing for A work up should include testing for high blood pressurehigh blood pressure, , coagulopathycoagulopathy,,
and and blood blood dyscrasiasdyscrasias especially if positive for a family history especially if positive for a family history
Important NoteImportant Note::•• Toxic damage to the retina if contact with hemoglobin and iron for a Toxic damage to the retina if contact with hemoglobin and iron for a long period of time long period of time

14
Hypercoaguable Hypercoaguable StateState::
• It is a risk factor for artery and venous occlusionsIt is a risk factor for artery and venous occlusions•• Has and association with coronary artery disease Has and association with coronary artery disease•• Has and association with cerebral vascular accidents (CVA) Has and association with cerebral vascular accidents (CVA)•• Hypercoaguable Hypercoaguable state is associated with peripheral vascular diseasestate is associated with peripheral vascular disease
Primary StatePrimary State:: Secondary StateSecondary State::
• Protein C deficiencyProtein C deficiency•• Protein S deficiency Protein S deficiency•• AntithrombinAntithrombin III III•• Factor V Factor V LeidenLeiden•• HyperhomocysteinemiaHyperhomocysteinemia•• ProthrombinProthrombin 20210 mutation 20210 mutation•• AntiphospholipidAntiphospholipid syndrome (Lupus anticoagulant / Anti- syndrome (Lupus anticoagulant / Anti-cardiolipincardiolipin antibody) antibody)•• CBC c differential, Platelet count and PT / PTT CBC c differential, Platelet count and PT / PTT
• PregnancyPregnancy•• Malignancy Malignancy•• Congestive Heart Failure Congestive Heart Failure•• Immobility Immobility
Coagulation PathwayCoagulation Pathway
Hypercoaguable Hypercoaguable StateState: Important Note: Important Note
• Factor V LeidenFactor V Leiden is the most common hereditary blood coagulation is the most common hereditary blood coagulation disorder in the United States ~10%disorder in the United States ~10%
•• Prothrombin Prothrombin 2021020210 mutation is the second most common inherited mutation is the second most common inheritedclotting abnormality in the United Statesclotting abnormality in the United States
Ophthalmic Presentations:Ophthalmic Presentations:
•• Central Retinal Artery Occlusion Central Retinal Artery Occlusion•• Branch Retinal Artery Occlusion Branch Retinal Artery Occlusion•• Central Retinal Vein Occlusion Central Retinal Vein Occlusion

15
““BRAOBRAO”” in a 42 in a 42 yo yo AA femaleAA female Birth-control medication Birth-control medication

16
Hypercoaguable Hypercoaguable StateState: Treatment: Treatment
••Monitor patient closely with Primary Care PhysicianMonitor patient closely with Primary Care Physician
••CoumadinCoumadin, Heparin, Aspirin therapy, Heparin, Aspirin therapy
••Treat ocular conditions accordinglyTreat ocular conditions accordingly
Dot and Blot Dot and Blot hemes hemes in mid-peripheral retinain mid-peripheral retina

17
Hypoperfusion Hypoperfusion Retinopathy / Ocular Ischemic SyndromeRetinopathy / Ocular Ischemic Syndrome::
• Usually unilateral but may be bilateral in 20% of casesUsually unilateral but may be bilateral in 20% of cases
•• Males > Females by a 2 to 1 ratio Males > Females by a 2 to 1 ratio
•• Dot and blot Dot and blot hemes hemes / / microanuerysms microanuerysms found only in the found only in the mid-mid-peripheralretina peripheralretina = = Hypoperfusion Hypoperfusion RetinopathyRetinopathy
•• When the above is associated with neovascularization of the Disc, When the above is associated with neovascularization of the Disc, Retina, Iris or Angle = Ocular Ischemic Syndrome Retina, Iris or Angle = Ocular Ischemic Syndrome

18
PathogenesisPathogenesis: Ocular Ischemic Syndrome:: Ocular Ischemic Syndrome:
• Atheromatous Atheromatous ulceration and ulceration and stenosis stenosis at the bifurcation of the at the bifurcation of the common carotid artery ( 90% occlusion has to be present ) common carotid artery ( 90% occlusion has to be present )
SymptomsSymptoms: Ocular Ischemic Syndrome: Ocular Ischemic Syndrome
• Ocular and Ocular and periorbital periorbital pain in 40% of cases = pain in 40% of cases = ““Ocular AnginaOcular Angina””
•• Prolonged recovery of vision following exposure to bright light- Prolonged recovery of vision following exposure to bright light- known as known as ““Light Induced AmaurosisLight Induced Amaurosis””
•• Amaurosis Fugax ( Transient Monocular Blindness ) in 5% of cases Amaurosis Fugax ( Transient Monocular Blindness ) in 5% of cases
•• Transient Ischemic Attacks (TIA) Transient Ischemic Attacks (TIA)
•• Vision Loss ( 90% ) Vision Loss ( 90% ) –– Short Posterior Short Posterior Ciliary Ciliary Arterial Arterial hypoperfusionhypoperfusion
Carotid DopplerCarotid Doppler Carotid BruitCarotid Bruit

19
SymptomsSymptoms: Ocular Ischemic Syndrome: Ocular Ischemic Syndrome
Ocular and Ocular and periorbital periorbital pain in 40% of cases = pain in 40% of cases = ““Ocular AnginaOcular Angina””
•• Ischemia to the ophthalmic division of Cranial Nerve 5 Ischemia to the ophthalmic division of Cranial Nerve 5
•• Anterior segment inflammation Anterior segment inflammation
•• Elevated intraocular pressure ( IOP ) from Elevated intraocular pressure ( IOP ) from neovascular neovascular glaucomaglaucoma
Ocular SignsOcular Signs: Ocular Ischemic Syndrome:: Ocular Ischemic Syndrome:
• Dilated but not tortuous retinal veinsDilated but not tortuous retinal veins•• Retinal Hemorrhages in mid-peripheral retina (80%) of patients Retinal Hemorrhages in mid-peripheral retina (80%) of patients•• Cotton Wool Spots (5%) Cotton Wool Spots (5%)•• Neovascularization of the Disc (35%) Neovascularization of the Disc (35%)•• Neovascularization of the Retina (8%) Neovascularization of the Retina (8%)•• Rubeosis Rubeosis iridis iridis (65%)(65%)•• Uveitis Uveitis –– mild anterior (20%) mild anterior (20%)•• Emboli (retinal) Emboli (retinal)•• Lower IOP - initially Lower IOP - initially

20
Ocular Ischemic SyndromeOcular Ischemic Syndrome
Cholesterol PlaquesCholesterol Plaques55 yo AA male “BRAO” OD
55 yo AA male OS

21
Cerebral Blood Supply Motor and Sensory Areas

22
Occipital Lobe InfarctOccipital Lobe Infarct
Work UpWork Up::
•• Carotid artery evaluation (Carotid Carotid artery evaluation (Carotid –– Duplex Scanning) Duplex Scanning) –– ICA, ECA, ICA, ECA,CCCC
•• Color Trans-cranial Color Trans-cranial doppler doppler (TCD) (TCD) –– ocular arteries ocular arteries
•• Possible MRA (Magnetic Resonance Angiography) Possible MRA (Magnetic Resonance Angiography)
•• Computed Tomography (CT) angiography Computed Tomography (CT) angiography
•• Cardiology work up (Echocardiogram) Cardiology work up (Echocardiogram) –– Transesophogeal Transesophogeal //TransthoracicTransthoracic
•• HTN, DM, Lipid Panel, ESR, C-reactive proteinHTN, DM, Lipid Panel, ESR, C-reactive protein
Ocular Ischemic SyndromeOcular Ischemic Syndrome
TreatmentTreatment::
•• Consider carotid surgery if warranted ( Consider carotid surgery if warranted (EndarterectomyEndarterectomy))European Carotid Surgery Trial (ECST)European Carotid Surgery Trial (ECST)North American Symptomatic Carotid End. TrialNorth American Symptomatic Carotid End. Trial
( NASCET) ( NASCET)
•• Therapeutic approach Therapeutic approach –– Aspirin ( 325 mg QD or BID ) , Aspirin ( 325 mg QD or BID ) , PlavixPlavix•• Control modifiable vascular risk factors ( HTN, DM, Control modifiable vascular risk factors ( HTN, DM, dyslipidemia dyslipidemia ))•• Stop smoking Stop smoking•• Panretinal Panretinal photocoagulation (PRP) if neovascularizationphotocoagulation (PRP) if neovascularization
Important NoteImportant Note::Leading cause of death = Ischemic heart diseaseLeading cause of death = Ischemic heart diseaseSecond leading cause of death = StrokeSecond leading cause of death = Stroke
Ocular Ischemic SyndromeOcular Ischemic Syndrome
CharacteristicsCharacteristics
•• ~ ~ 24 million American have Diabetes24 million American have Diabetes
•• Most commonMost common retinal vasculature disease retinal vasculature disease
•• Diabetes = leading cause of blindness in Americans between 20-74 Diabetes = leading cause of blindness in Americans between 20-74 years old years old
•• African Americans, Hispanics and Native Americans are high risk groups African Americans, Hispanics and Native Americans are high risk groups
• Non white females are at greatest risk for blindnessNon white females are at greatest risk for blindness
DiabetesDiabetes

23
• Hispanic population tends to have the highest prevalence rates of DRHispanic population tends to have the highest prevalence rates of DR
•• African Americans tend to have highest rates of vision threatening DR African Americans tend to have highest rates of vision threatening DR
•• No prominent difference between genders were seen in the prevalence of No prominent difference between genders were seen in the prevalence of diabetic retinopathy diabetic retinopathy
•• The prevalence of diabetic retinopathy is in older age groups The prevalence of diabetic retinopathy is in older age groups
The Prevalence of Diabetic RetinopathyThe Prevalence of Diabetic RetinopathyClassification of Diabetic RetinopathyClassification of Diabetic Retinopathy
““Non-ProliferativeNon-Proliferative”” ““ProliferativeProliferative””
•• Mild Mild EarlyEarly•• Moderate Moderate High riskHigh risk•• Severe (4-2-1 rule) Severe (4-2-1 rule)•• Very Severe Very Severe
Other Ocular Complications:Other Ocular Complications:•• Clinically Significant Macular Edema Clinically Significant Macular Edema•• Diabetic Diabetic PapillopathyPapillopathy•• Cranial Nerve Palsy 3,4,6 Cranial Nerve Palsy 3,4,6•• Cataract formation Cataract formation
DiabetesDiabetes
““SevereSevere”” Non-Proliferative Non-Proliferative Diabetic RetinopathyDiabetic Retinopathy
DiabetesDiabetes
24
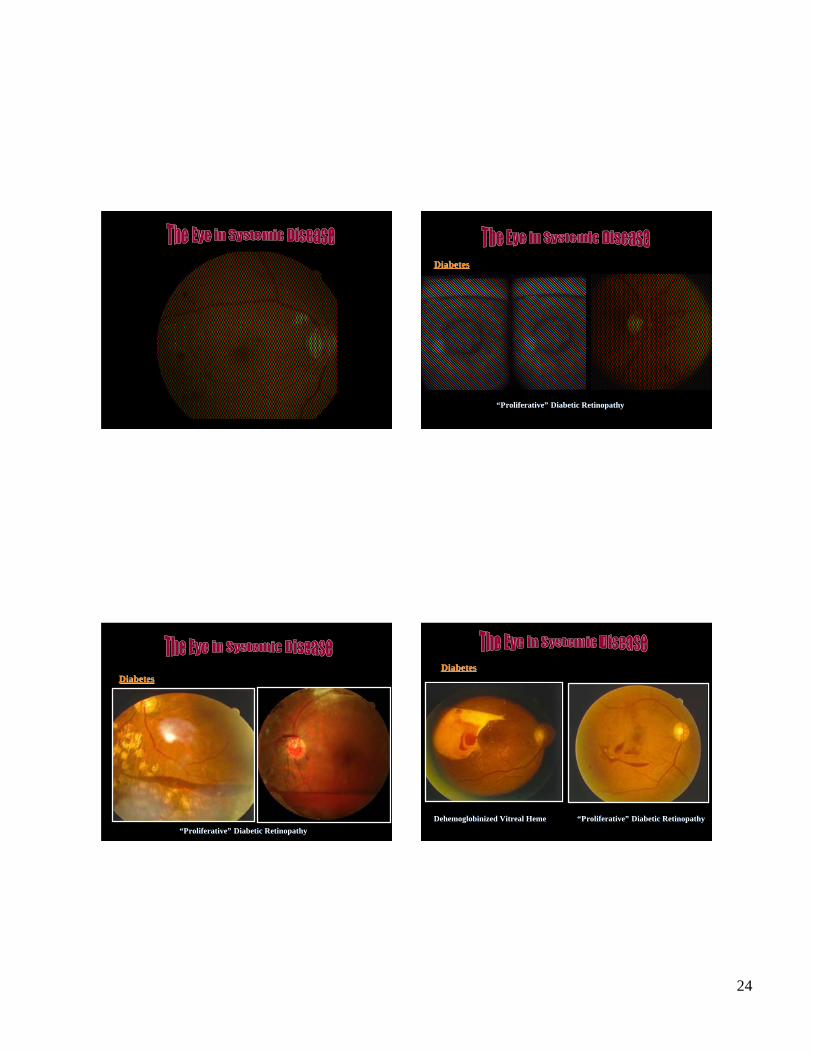
““ProliferativeProliferative”” Diabetic Retinopathy Diabetic Retinopathy
DiabetesDiabetes
DiabetesDiabetes
““ProliferativeProliferative”” Diabetic Retinopathy Diabetic Retinopathy
DiabetesDiabetes
Dehemoglobinized Vitreal HemeDehemoglobinized Vitreal Heme ““ProliferativeProliferative”” Diabetic Retinopathy Diabetic Retinopathy

25
DiabetesDiabetes
““ProliferativeProliferative”” Diabetic Retinopathy Diabetic Retinopathy
DiabetesDiabetes
Fibrous Proliferation Fibrous Proliferation –– ““ProliferativeProliferative”” Diabetic Retinopathy Diabetic Retinopathy
““CSMECSME”” –– Clinically Significant Macular Edema Clinically Significant Macular Edema
DiabetesDiabetes 4-2-1 Rule4-2-1 Rule
Severe NPDRSevere NPDR At least one of :At least one of :
intraretinalintraretinal hemorrhages in hemorrhages in fourfour quadrants quadrants
venous beading invenous beading in two two quadrants quadrants
intraretinalintraretinal microvascularmicrovascular abnormalities in abnormalities in 1 quadrant1 quadrant
Standard photographs available at:Standard photographs available at:eyephoto.ophth.wisc.edu/ResearchAreas/Diabetes/DiabSeyephoto.ophth.wisc.edu/ResearchAreas/Diabetes/DiabStds.htmtds.htm

26
IntraretinalIntraretinal hemorrhages in hemorrhages in fourfourquadrantsquadrants
Venous Beading and Venous Beading and IntraretinalIntraretinalMicrovascularMicrovascular Anomalies (IRMA) Anomalies (IRMA)
Venousbeading IRMA
DIABETIC MACULAR EDEMA
CSME DefinedCSME Defined
CSME, as defined by the ETDRS, existsCSME, as defined by the ETDRS, existswith any of the following findings:with any of the following findings: Retinal thickening within 500 mm of theRetinal thickening within 500 mm of the
center of the foveacenter of the fovea Hard exudates within 500 mm of the center ofHard exudates within 500 mm of the center of
the fovea with adjacent retinal thickeningthe fovea with adjacent retinal thickening At least 1 disc area of retinal thickening, anyAt least 1 disc area of retinal thickening, any
part of which is within 1 disc diameter of thepart of which is within 1 disc diameter of thecenter of the foveacenter of the fovea

27
Diabetic Macular EdemaDiabetic Macular Edema Management Guidelines: DMEManagement Guidelines: DME More recently, laser out-performedMore recently, laser out-performed
intravitreal Kenalogintravitreal Kenalog.. Laser + Laser + Lucentis Lucentis out-performed laserout-performed laser
alone.alone.
++
DiabetesDiabetes
Some important systemic effects of diabetes that affect Some important systemic effects of diabetes that affect retinopathy retinopathy andandincrease the risk of increase the risk of ““Heart AttackHeart Attack””::
#1 #1 ProteinuriaProteinuria•• First sign of renal diseaseFirst sign of renal disease•• As nephropathy increases As nephropathy increases……the the glomerular glomerular filtration rate fallsfiltration rate falls•• American Diabetes Association (ADA) recommends American Diabetes Association (ADA) recommends yearly urinalysisyearly urinalysis
•• Random Spot Urine or 24 hour collection Random Spot Urine or 24 hour collectionNormal <30Normal <30Microalbuminuria Microalbuminuria 30 mg 30 mg –– 299 mg 299 mgAlbuminuria Albuminuria > 300 mg> 300 mg
DiabetesDiabetes
#2 Anemia#2 Anemia•• Gets more severe as renal disease worsens Gets more severe as renal disease worsens•• Kidney production of Kidney production of ““ErythropoietinErythropoietin”” decrease, which means that less decrease, which means that less
reaches the bone marrow and less red blood cells are made reaches the bone marrow and less red blood cells are made•• Measured by Measured by Hematocrit Hematocrit (HCT) and hemoglobin levels in a CBC(HCT) and hemoglobin levels in a CBC
If hemoglobin levels are less than 11g/dl = If hemoglobin levels are less than 11g/dl = anemiaanemia
AnemiaAnemia may actually be making the retinopathy worse!!!may actually be making the retinopathy worse!!!
Treat the patient with Treat the patient with ““ProcritProcrit”” if patient is not on dialysis if patient is not on dialysis……also give ironalso give iron
KidneyKidney ErythropoietinErythropoietin Bone Marrow Bone Marrow RBCRBC’’ss

28
DiabetesDiabetes
#3 #3 HyperlipidemiaHyperlipidemia• Cholesterol and triglyceride healthy levels should be < 200 mg/dlCholesterol and triglyceride healthy levels should be < 200 mg/dl•• PCP should consider PCP should consider Lipitor Lipitor if cholesterol highif cholesterol high
#4 #4 HypertensionHypertension• Target blood pressure for diabetics with nephropathy is Target blood pressure for diabetics with nephropathy is 130 /80130 /80•• ACE inhibitors ACE inhibitors should be given if blood pressure is high should be given if blood pressure is high•• ACE inhibitors are both ACE inhibitors are both renal-protectiverenal-protective and and anti-anti-proteinuricproteinuric
#5 #5 HyperglycemiaHyperglycemia• Induces vasoconstriction = kidney ( Induces vasoconstriction = kidney ( glomerularglomerular ) damage ) damage•• The Hemoglobin A1C should be as close to 7 % as possible The Hemoglobin A1C should be as close to 7 % as possible
• Hypertension in diabetics is Hypertension in diabetics is labilelabile and only effectively and only effectively measured at home measured at home
WBCWBC’’s s adhere toadhere toand accumulateand accumulatewithin the retinalwithin the retinalvasculaturevasculatureICAMICAM
FurtherFurtherbreakdownbreakdownof the blood-of the blood-retinal barrierretinal barrier
Release of VEGFRelease of VEGFVascularVascularEndothelialEndothelialGrowthGrowthFactorFactor
REMSleep
#6. #6. Obstructive Sleep ApneaObstructive Sleep Apnea
•• Progressive relaxation of upper airway musculature in deeper stages of sleep Progressive relaxation of upper airway musculature in deeper stages of sleep• Nocturnal HypertensionNocturnal Hypertension
Continuous Positive Airway PressureContinuous Positive Airway Pressure
Nasal Mask:Nasal Mask:•• Intimidating Intimidating•• Cumbersome Cumbersome•• ? Poor Compliance ? Poor Compliance

29
• Elevated morning BP by 20 -30 mmHgElevated morning BP by 20 -30 mmHg
• Elevated, resistant BP throughout the dayElevated, resistant BP throughout the day
• Relationship: Congestive Heart Failure, Nocturnal MI / CVA, NephropathyRelationship: Congestive Heart Failure, Nocturnal MI / CVA, Nephropathy
DM + Smoking = BlindnessDM + Smoking = Blindness
#7. #7. SmokingSmoking
• Severely worsens Severely worsens microangiopathymicroangiopathy • Smoking is a risk factor for Smoking is a risk factor for proteinuria proteinuria and increased blood pressureand increased blood pressure
•• Nicotine increases blood platelet viscosity which can increase retinopathy Nicotine increases blood platelet viscosity which can increase retinopathy
•• Smoking also causes arterial wall damage and constriction Smoking also causes arterial wall damage and constriction
SmokingSmoking

30
““ModerateModerate”” Non-Proliferative Non-Proliferative Diabetic RetinopathyDiabetic Retinopathy

31

32

33
ACCORD studyACCORD study
•• Patients with tightly controlled blood glucose (HbA1C < 6%) had a 22% Patients with tightly controlled blood glucose (HbA1C < 6%) had a 22% higher risk of death vs. those patients with less HbA1C control (7-8%) higher risk of death vs. those patients with less HbA1C control (7-8%)
•• The study was halted The study was halted
ADVANCE studyADVANCE study
•• Had different results. Risk reduction by 10% in micro and Had different results. Risk reduction by 10% in micro and macrovascularmacrovascular events.events.
DPP (Diabetic Prevention Program) DPP (Diabetic Prevention Program) - - PrediabeticsPrediabetics
•• Lifestyle intervention group vs. med group (Lifestyle intervention group vs. med group (metforminmetformin) vs. placebo) vs. placebo
•• Lifestyle group showed the most decrease in diabetes risk Lifestyle group showed the most decrease in diabetes risk
Take HomeTake Home::
•• Diabetic Retinopathy is exacerbated by many concomitant conditions Diabetic Retinopathy is exacerbated by many concomitant conditions
•• Control of the systemic aspects of the disease improves the systemic Control of the systemic aspects of the disease improves the systemic and and ocular healthocular health
•• Understand how Diabetic Retinopathy relates to the overall systemic Understand how Diabetic Retinopathy relates to the overall systemic health health
DiabetesDiabetes
Cholesterol /Cholesterol /TriglyceridesTriglycerides< 200 mg/dl< 200 mg/dl
TriglyceridesTriglycerides> 2,500 mg/dl> 2,500 mg/dl
““Lipemia RetinalisLipemia Retinalis””
CholesterolCholesterol990 mg/dl990 mg/dl
TriglycerideTriglyceride7,200 mg/dl7,200 mg/dl
• Arcus SenilisArcus Senilis•• Arcus Juvenilis Arcus Juvenilis
• 50% have high cholesterol levels50% have high cholesterol levels
• In younger people may lead to MI orIn younger people may lead to MI or cardiovascular disease cardiovascular disease
•• ArcusArcus = = ““Bow likeBow like
• HyperlipoproteinemiaHyperlipoproteinemia in younger pts. in younger pts.

34
The Association of Corneal The Association of Corneal Arcus Arcus with Coronary Heart Disease andwith Coronary Heart Disease andCardiovascular Disease Mortality in the Lipid Research ClinicsCardiovascular Disease Mortality in the Lipid Research ClinicsMortality Follow-up StudyMortality Follow-up Study ( Am J Public Health 1990; 80:1200-1204 )( Am J Public Health 1990; 80:1200-1204 )
Prospective study of White men ( n = 3,930 )Prospective study of White men ( n = 3,930 )and women non-hormone users ( n = 2139 )and women non-hormone users ( n = 2139 )Followed for an average of 8.4 yearsFollowed for an average of 8.4 years
• Corneal Corneal ArcusArcus was strongly associated with CHD and CVD mortality was strongly associated with CHD and CVD mortality only in only in hyperlipidemichyperlipidemic men ages 30-49 years. men ages 30-49 years.
•• Among 30-49 year old males, corneal Among 30-49 year old males, corneal arcusarcus was a prognostic factor was a prognostic factor for CHD independent of for CHD independent of hyperlipidemiahyperlipidemia
ResultsResults::
HyperlipidemiaHyperlipidemia
• Type 2 diabetics have elevated triglyceride levelsType 2 diabetics have elevated triglyceride levels
•• Type 2 diabetics have decreased high-density lipoprotein (HDL) levels Type 2 diabetics have decreased high-density lipoprotein (HDL) levels
•• Increases cardiovascular mortality risk = Coronary Artery Disease Increases cardiovascular mortality risk = Coronary Artery Disease
Management:Management:
• Nutrition Therapy = lifestyle changeNutrition Therapy = lifestyle change
•• Exercise = lifestyle change Exercise = lifestyle change
•• Drug Therapy Drug Therapy StatinsStatins ( (akaaka) HMG-) HMG-CoACoA reductasereductaseinhibitorsinhibitors
• Aspirin use in diabetic patients is Aspirin use in diabetic patients is not associatednot associated with an with an increased risk of hemorrhage or progression of retinopathy increased risk of hemorrhage or progression of retinopathy or macular edema !!! or macular edema !!!
•• Aspirin use may actually slow the progression of diabetic retinopathy ??? Aspirin use may actually slow the progression of diabetic retinopathy ???
•• Aspirin Therapy ( 81-325 mg/day): ADA recommendations Aspirin Therapy ( 81-325 mg/day): ADA recommendations
•• Family History of coronary heart disease Family History of coronary heart disease•• Cigarette smoking Cigarette smoking•• Hypertension Hypertension•• Obesity Obesity•• AlbuminuriaAlbuminuria•• Elevated lipid levelsElevated lipid levels•• Age > 30 years Age > 30 years
Aspirin Use in DiabetesAspirin Use in Diabetes

35
29 year old AA female. Dry eye complaints29 year old AA female. Dry eye complaints
Cotton Wool Spots OUCotton Wool Spots OUHIV Retinopathy HIV Retinopathy –– CD4 count 110 CD4 count 110 Pt. not on HAART Pt. not on HAART

36
45 year old male. Diabetes history45 year old male. Diabetes history
Cytomegalo-virus (CMV)
• CD4 Count CD4 Count –– Measure of T-cell count ( 600 Measure of T-cell count ( 600 –– 1500 cell / m3 ) 1500 cell / m3 )
•• CD4 / CD 8 Ratio ( Normal is 2.0 ) CD4 / CD 8 Ratio ( Normal is 2.0 )
•• Viral Load - # of HIV 1-RNA molecules / ml blood ( 10,000 low / 100,000 high ) Viral Load - # of HIV 1-RNA molecules / ml blood ( 10,000 low / 100,000 high )
CD 4 Count and Ocular Management of the HIV Patient CD 4 Count and Ocular Management of the HIV Patient
CD4 Count Frequency of Examination
> 250 cell / mm3 1 year
150 cell / mm3 6 months
50 -150 cell / mm3 3 months
< 50 cell / mm3 1 month
Acquired Immune Deficiency Syndrome (AIDS)Acquired Immune Deficiency Syndrome (AIDS)
Course of the DiseaseCourse of the Disease
•• Initial Stage Initial Stage –– Influenza like illness ~ 4-12 weeks after becoming infected Influenza like illness ~ 4-12 weeks after becoming infected
•• Chronic Stage Chronic Stage –– Latent period ~ 10 years with minor immune dysfunction Latent period ~ 10 years with minor immune dysfunction
•• Final (Crisis) Stage Final (Crisis) Stage –– Weight loss, fever, skin rashes, opportunistic infections Weight loss, fever, skin rashes, opportunistic infections and and neoplasmsneoplasms

37
Foscarnet (Foscavir®)
Ganciclovir (Cytovene®)
Cidofovir (Vistide®)
Valganciclovir (Valcyte®)
Ganciclovir implants (Vitrasert®)
Fomivirsen (Vitravene®)
Five drugs currently available to people with CMV diseaseFive drugs currently available to people with CMV disease::
Through an IV line
Through an IV line followed by capsules
Through an IV line
Tablets that must be swallowed.
Surgically implanted directly into the eye.
A shot directly into the eye.
www.aidsmeds.com
Lupus RetinopathyLupus Retinopathy
Sheathing of Blood VesselsSheathing of Blood Vessels

38
Lupus Choroidopathy Lupus Retinopathy and Optic Neuropathy
Iritis
Systemic Lupus
Three forms of lupus are knownThree forms of lupus are known•• Systemic lupus Systemic lupus erythematosuserythematosus•• Cutaneous Cutaneous lupuslupus•• Drug-induced lupus Drug-induced lupus
A multisystem autoimmune disorderthat commonly affects women ofthat commonly affects women ofchildbearing age (women>>>men)childbearing age (women>>>men)
Common findings include Common findings include malarmalar rash rash,,arthritisarthritis,, oral ulcers, oral ulcers, renal disease,renal disease,hematologicalhematological, seizures and psychosis,, seizures and psychosis,pulmonary and GIpulmonary and GI ““Roth SpotRoth Spot””

39
Systemic Lupus Systemic Lupus ErythematosusErythematosus
• Lupus is more common in the African American, Lupus is more common in the African American, Asian and native American populations Asian and native American populations
•• Approximately 15 % of patients with Lupus will have retinal disease Approximately 15 % of patients with Lupus will have retinal disease
•• Retinopathy can be associated with central nervous system Retinopathy can be associated with central nervous system complications such as complications such as cerebritiscerebritis
Clinical Retinal FeaturesClinical Retinal Features
•• Cotton Wool Spots Cotton Wool Spots•• Retinal Hemorrhages Retinal Hemorrhages•• VasoVaso-occlusive disease-occlusive disease•• Frosted branch Frosted branch periphlebitisperiphlebitis
Laboratory Testing in Systemic Lupus Laboratory Testing in Systemic Lupus ErythematosusErythematosus
• Complete Blood Count (CBC)Complete Blood Count (CBC)
•• Platelet count Platelet count
•• Erythrocyte Sedimentation Rate (ESR) - Westergren Erythrocyte Sedimentation Rate (ESR) - Westergren
•• C-Reactive Protein (CRP) C-Reactive Protein (CRP)
•• Antinuclear antibody (ANA) Antinuclear antibody (ANA) –– screening test screening test
•• Anti-n DNA ( ordered when ANA is positive ) Anti-n DNA ( ordered when ANA is positive )
•• Urinalysis Urinalysis
•• Complement ( C3 and C4 ) serum levels Complement ( C3 and C4 ) serum levels
Scleritis

40
Scleral thinning and scleromalacia perforans
FeatureFeature EpiscleritisEpiscleritis ScleritisScleritis
Number of patientsNumber of patients 3737 9797
AgeAge 4545 5151
GenderGender 30%30% 29%29% menmen70%70% 71%71% womenwomen
RaceRace white 84%white 84% white 79%white 79%
BitlateralBitlateral 49%49% 51%51%
Systemic diseaseSystemic disease RA RA 18% RA18% RA
EpiscleritisEpiscleritis and and ScleritisScleritis: Clinical Features and Treatment Results. Doug Jabs, et al.: Clinical Features and Treatment Results. Doug Jabs, et al.Ophthalmology 2000; 130:469-476.Ophthalmology 2000; 130:469-476.
““MetastaticMetastatic”” Choroidal Choroidal TumorTumor

41
Choroidal Choroidal MetastasisMetastasis
Metastatic Metastatic TumorsTumors
• Lung cancerLung cancer - #1 cause of death in males - #1 cause of death in males•• Breast cancer Breast cancer - #1 cause of death in females - #1 cause of death in females•• Prostate cancer Prostate cancer –– most common cancer in men most common cancer in men
(More common and more aggressive in African Americans)(More common and more aggressive in African Americans)
•• Colon cancer Colon cancer –– 3 3rdrd most common in men, 2 most common in men, 2ndnd most common in women most common in women•• Melanoma Melanoma –– skin most common site of cancer development skin most common site of cancer development
(Males = trunk)(Males = trunk) (Females = extremities)(Females = extremities)
•• Ovarian cancer Ovarian cancer –– disease of postmenopausal women disease of postmenopausal women•• Pancreatic cancer Pancreatic cancer –– usually >65 years old, wt. loss, jaundice, anorexia usually >65 years old, wt. loss, jaundice, anorexia•• Uterine cancer Uterine cancer –– disease of postmenopausal women disease of postmenopausal women
(abnormal vaginal discharge or bleeding)(abnormal vaginal discharge or bleeding)

42

43
Metastatic Metastatic TumorsTumors
• Choroidal Choroidal Metastasis is the most common ocular tumorMetastasis is the most common ocular tumor•• Most metastases found in the choroid are from the breast and lung Most metastases found in the choroid are from the breast and lung•• Only Only ~ 65 %~ 65 % of patients with a of patients with a choroidal choroidal metastasis have beenmetastasis have been
diagnosed with a form of systemic cancerdiagnosed with a form of systemic cancer
Ocular Presentation:Ocular Presentation:•• Dome-shaped lesion yellow to orange in color Dome-shaped lesion yellow to orange in color•• Most often in the posterior pole but can be in iris and Most often in the posterior pole but can be in iris and ciliary ciliary bodybody•• They may be solitary or They may be solitary or multifocal multifocal •• Bilateral in Bilateral in ~ 30 %~ 30 % of cases of cases
Treatment:• Observation, external beam radiation, radioactive plaque therapyObservation, external beam radiation, radioactive plaque therapy•• The goal of treatment is to save the The goal of treatment is to save the pxpx’’ss vision for the remainder of life vision for the remainder of life
44
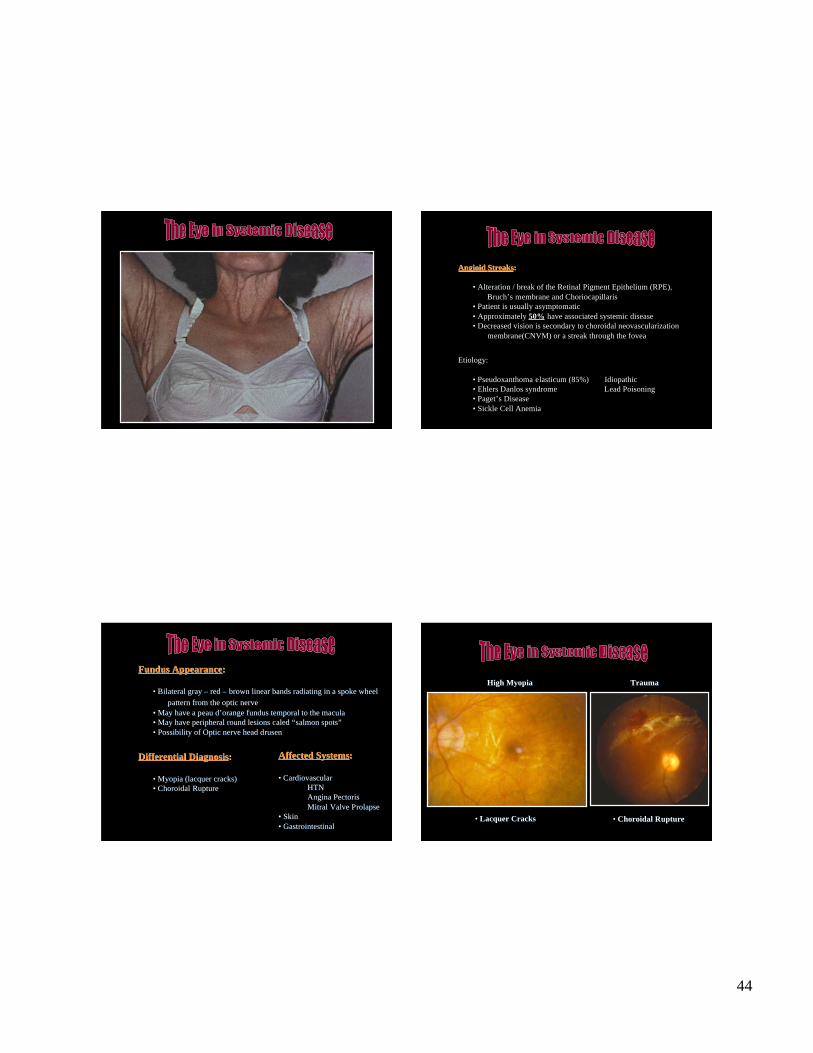
Angioid Angioid StreaksStreaks::
• Alteration / break of the Retinal Pigment Epithelium (RPE),Bruch’s membrane and Choriocapillaris
• Patient is usually asymptomatic• Approximately 50% have associated systemic disease• Decreased vision is secondary to choroidal neovascularization
membrane(CNVM) or a streak through the fovea
Etiology:
• Pseudoxanthoma elasticum (85%) Idiopathic• Ehlers Danlos syndrome Lead Poisoning• Paget’s Disease• Sickle Cell Anemia
Fundus AppearanceFundus Appearance::
• Bilateral gray Bilateral gray –– red red –– brown linear bands radiating in a spoke wheel brown linear bands radiating in a spoke wheelpattern from the optic nervepattern from the optic nerve
•• May have a May have a peau dpeau d’’orange orange fundus temporal to the maculafundus temporal to the macula•• May have peripheral round lesions May have peripheral round lesions caled caled ““salmon spotssalmon spots””•• Possibility of Optic nerve head Possibility of Optic nerve head drusendrusen
Differential DiagnosisDifferential Diagnosis::
• Myopia (lacquer cracks)Myopia (lacquer cracks)•• ChoroidalChoroidal Rupture Rupture
Affected SystemsAffected Systems::
• CardiovascularCardiovascularHTNHTNAngina PectorisAngina PectorisMitralMitral Valve Valve ProlapseProlapse
•• Skin Skin•• Gastrointestinal Gastrointestinal
• Lacquer CracksLacquer Cracks • Choroidal Choroidal RuptureRupture
High MyopiaHigh Myopia TraumaTrauma

45
• Choroidal RutureChoroidal Ruture
Initial PresentationInitial Presentation 3 weeks later3 weeks laterTreatmentTreatment:: Angioid Angioid StreaksStreaks
•• Focal laser if (CNVM) is present Focal laser if (CNVM) is present•• Management of any underlying systemic disease Management of any underlying systemic disease
Follow upFollow up::
• Twice a year with a dilated fundus examinationTwice a year with a dilated fundus examination•• AmslerAmsler Grid testing (~3 x week) Grid testing (~3 x week)
The End !!!!
Any Questions ????







