1 www.EducationalDesigns.com © 2018
The Periodontic/Orthodontic Connection: Maximizing Success with the Orthodontic Patient Kristy Menage Bernie, RDH, MS, RYT • [email protected]
- Orthodontic therapies are no longer confined to the adolescent population and as such the role of the dental team members in patient education has grown significantly in recent years. This course will include the latest in tooth movement sciences as well as the periodontic/orthodontic connection. Methods to maximize oral health during therapy, including CAMBRA (Caries Management by Risk Assessment) and periodontal considerations will be included in this interactive, fast paced seminar! Our Opportunities:
• Understand the role of the orthodontic team and education for referring practices. • Review the periodontic/orthodontic connection. • List current options in orthodontic therapies and related science. • Implement client-centered daily care options and opportunities.
Orthodontic Therapy: Current & Future Need Estimated % of patients who would benefit from orthodontic therapy = The Periodontal Orthodontic Connection: Biological & Synergistic Tooth Movement Identifying the Orthodontic Patient Occlusal Assessments: “Occlusal therapy is an integral part of periodontal therapy. Patients should be informed about the occlusal problem, therapeutic alternatives, potential complications, expected results, and their responsibility in treatment. Consequences of no treatment should be explained. Failure to treat occlusal traumatism appropriately in patients with chronic periodontitis may result in progressive loss of bone and an adverse change in prognosis, and could result in tooth loss. Given this information, patients should then be able to make informed decisions regarding their periodontal therapy.” J Periodontol 2000; 71:873-875. Orthodontic Six-Point Quick Check System: Begin by examining each arch separetly and evaluating the following categoris:
1. Arch width (molar-to-molar transpalatal width of 36 mm is average). 2. Excessive spacing or crowding present. 3. Missing or ankylosed teeth.
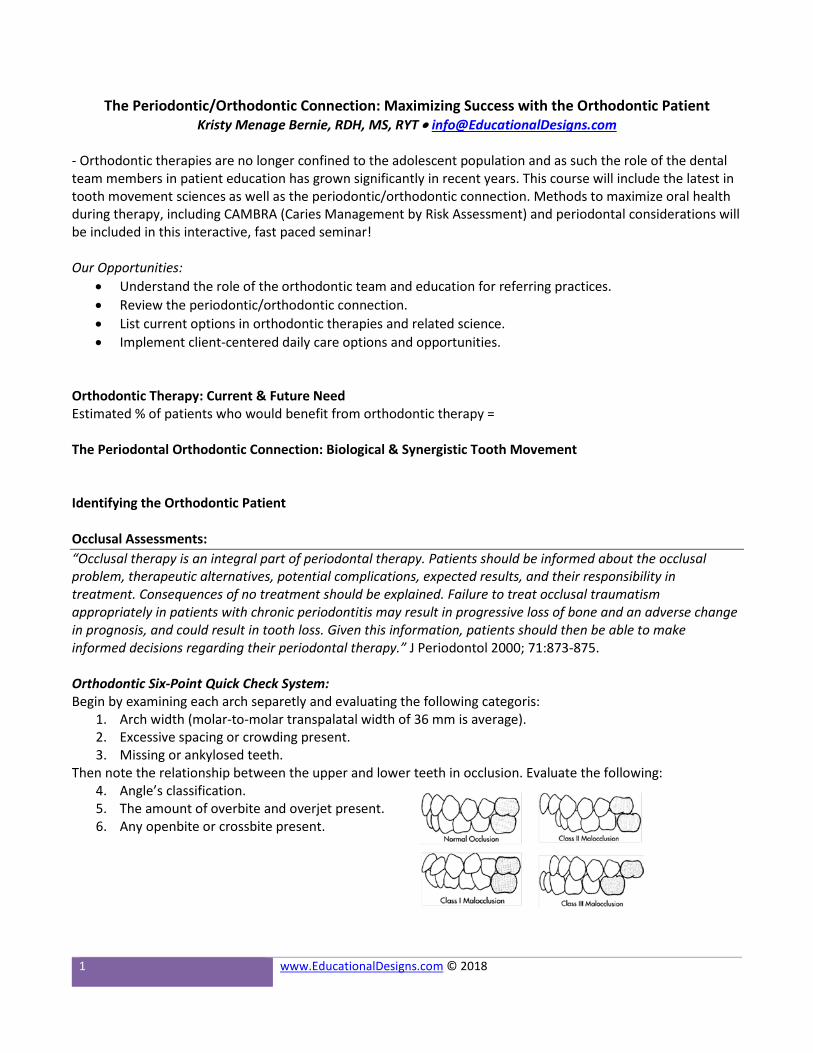
Then note the relationship between the upper and lower teeth in occlusion. Evaluate the following: 4. Angle’s classification. 5. The amount of overbite and overjet present. 6. Any openbite or crossbite present.
2 www.EducationalDesigns.com © 2018
Seven Signs & Symptoms of Occlusal Disease: 1. Pathological occlusal wear and fractures of teeth/restorations. 2. Cervical dentin hypersensitivity. 3. Tooth hypermobility. 4. Fremitus. 5. Abfractions. 6. Vertical bone loss or localized bone destruction (secondary to periodontal disease). 7. Pain and tired facial and masticatory muscles or TMJ pain.
Facial Type: Mesocephalic – Jaw bones are in harmony with the rest of the face & with each other; teeth may be malposed & therefore need orthodontic treatment; most common facial type. Brachycephalic – Jaw bones, usually the mandible, are too large in proportion to the face; the face appears short & wide; mandible is usually strong, angular, and possibly prognathic; tendency to brux & grind teeth leading to excessive wear to incisal & occlusal surfaces; when smiling very little tooth structure shows; strong muscles of mastication; from profile perspective the mouth area appears concave; extractions are rarely performed; older in appearance than age suggests. Dolichocephalic – Jaw bones, usually the mandible, are too small in proportion to the face; the face appears long; mandible is usually retrognathic depicting a deficient horizontal growth; teeth can be long or appear large with a ‘gummy’ smile; weak muscles of mastication; from the profile perspective the mouth area appears convex; extractions are common in this facial type; appear younger than age would suggest; hereditary, thumb sucking, & mouth breathing are associated with this facial type; extractions are more commonly recommended with this facial type along with orthognathic surgery; considered more difficult to treat than other facial types.
Caries Risk Management by Assessment (CAMBRA) – Active orthodontic patients are automatically considered moderate risk for caries. Periodontal Assessment – Visit www.perio.org for a patient self-assessment. Orthodontic Therapy Options:
Traditional orthodontic fixed appliances, with ligation Two-Phase therapy includes early intervention and fixed traditional appliances Bio-Adaptive therapy considers tissue and bone while accelerating the tooth movement process, gaining
arch width and generating oxygenation during tooth movement (self-ligated systems) Aligner technologies include a series of custom aligners worn sequentially over time Accelerated osteogenic orthodontics includes a combination of periodontal surgery and fixed appliances
to accelerate the tooth movement process by removing alveolar bone and using bone regenerative materials

3 www.EducationalDesigns.com © 2018
Active Orthodontic Considerations: Hard Tissue
Clinical:
1. 5% NaF Varnish 2. Chlorhexidine ‘varnish’ 3. De-plaquing
(power scalers; airpolishing, tongue cleaning, etc.)
Daily care:
1. 5,000 ppm fluoride 2. Calcium/phosphate 3. Antibacterial agents 4. Use of power toothbrush technologies 5. Appropriate interdental devices & tongue cleaning tools

4 www.EducationalDesigns.com © 2018
CAMBRA – Remineralization/Antimicrobial Considerations: REMINERALIZATION: 5% Sodium Fluoride Varnish – Consider products containing xylitol and/or calcium phosphate; can replace fluoride tray treatments (see ADA Professional Fluoride Utilization)/ various products. 38% Silver Diamine Fluoride – utilize for active lesions, will stain demineralized areas and reverse decay process (Advantage Arrest by Elevate). Calcium Phosphate Systems
• Tri-Calcium Phosphate (TCP): During the manufacturing process, a protective barrier is created around the calcium allowing it to coexist with the fluoride ions. As the toothpaste comes in contact with saliva during brushing, the barrier breaks down and makes the calcium, phosphate and fluoride readily available.
o Clinical Application: Vanish Varnish 5% NaF & Vanish XT Varnish • 3M ESPE o Daily Care Products: Clinpro 5000 (5,000 ppm NaF & TCP) Toothpaste • 3M ESPE & Prevident
Booster Plus (5,000 ppm NaF & TCP) • Colgate • Casein Phosphopeptide Amorphous Calcium Phosphate (CPP-ACP): Recaldent - casein (milk protein)
enclosed system that binds to oral tissues, plaque, etc. and then releases ACP at an acidic pH. o Clinical Application: MI Varnish 5% NaF (Not available in Canada) • GC America o Daily Care Products: MI Paste, MI Paste Plus (950 ppm NaF) & MI Paste One (950 ppm NaF) • GC
America • Calcium Sodium Phosphosilicate (CSP): Novamin® - bioactive glass assists in sustained release of calcium
& phosphate while neutralizing the pH. o Clinical Application: Nupro Prophy Paste • Dentsply & Pro Sylc Air polishing Powder • Velopex,
International o Daily Care Products: Burt’s Bees Toothpaste
• Amorphous Calcium Phosphate (ACP): ADA Foundation Technology - Immediate release of CP upon contact with oral cavity, without dependency on pH or other oral factors.
o Clinical Application: Enamel Pro Varnish (5% NaF & ACP); Enamel Pro Prophy Paste & Enamel Pro APF (1.23% non-acidulated fluoride & ACP) • Premier Dental
o Daily Application: Enamelon (970 SnF2, ACP & Sypilanthes) • Premier Dental; Relief Oral Care Gel (1,000 ppm NaF, KNO3 & ACP) • Philips Oral Healthcare
• Other: Varnishes containing xylitol and calcium phosphate o Clinical Application: Embrace Varnish (5% NaF & calcium/xylitol phosphate) • Pulpdent
ANTIMICROBIAL: Chlorhexidine
• 0.12% CHX rinses – Various (including alcohol-free by Sunstar) • CHX In-Office Application: Cervitec Plus • Ivoclar (10% CHX and 10% thymol once solvent dissipates) and
Cervitec F (with fluoride, CHX) Xylitol - Various products, including mints, chewing gum, lollipops, etc.

5 www.EducationalDesigns.com © 2018
Active Orthodontic Considerations Soft Tissue:
Full Mouth vs. Quadrant (Partial Mouth) Periodontal Therapy Full-mouth disinfection (FMD) was introduced in 1995 and was designed to target intraoral niches and periodontal pockets and reduce the likelihood of reinfection of previously treated areas. Partial Mouth Protocol: Traditional quadrant scaling and root planing over a 6 week period of time at 2 week
intervals 4 – 6 consecutive sessions Quadrant or sextant therapy Reinfection potential? Patient/ Client centered approach?
Research Protocol - FMD: Scaling and root planing 4 quads in 24 hours with hand instruments Application of chlorhexidine to all intra-oral niches Tongue disinfection 2x a day rinse and/or spray of buccal mucosa and tonsil area combined with daily
tongue disinfection
Research on the efficacy of FMD has proven that this protocol: • Improves probing depth and increases clinical attachment for up to 8 months. • Reduces oral malodor • Decreases spirochetes and motile organisms in subgingival flora • Eliminates P. gingivalis
FMD provides the following additional benefits:
• Fast-tracking of aesthetic treatment • Rapid healing and/or assessment for surgical intervention • Facilitates client-centered approach • Minimizes time spent in Phase I therapy by facilitating control of treatment planning and
patient compliance Contemporary research on adjunctive therapies always begins with full-mouth therapy that is completed in one to two weeks using both hand and powered instrumentation.
This substantial body of research utilizing this process of care provides the full rationale to accelerate periodontal instrumentation in daily practice.
Optimal Oral Health - A standard of health of the oral and related tissues which enable an individual to eat, speak, or socialize without active disease, discomfort or embarrassment and which contributes to general well-being and overall health – ADHA, 1999.

6 www.EducationalDesigns.com © 2018
PROPOSED ACCELERATED INSTRUMENTATION PROTOCOL: 2 appointments of appropriate length scheduled within 24 hours – to 2 weeks • ½ mouth per appointment
1. Pre-procedural antimicrobial rinse for 30 seconds 2. Anesthesia administration/ pain control procedures 3. Instrumentation
a. Powered instrumentation with self-contained water / medicament reservoir and antimicrobial irrigant
b. Hand instrumentation 4. Laser Therapy
a. Bacterial decontamination of pocket sites (prior and post instrumentation) b. Removal of diseased epitheal lining (post instrumentation in sites greater than 5mm)
5. Placement of locally delivery/ control release medicaments 6. Tongue deplaquing/ scraping with antimicrobial/VSC neutralizing agent 7. Post-procedural rinse for 30 seconds with antimicrobial/VSC neutralizing agent 8. Professional fluoride treatment and/or CHX varnish application (Ivoclar/Vivadent) 9. 2 to 3 month evaluation
a. Utilization of diagnostic devices to assess clinical outcome b. Placement of local delivery / controlled release agent for nonresponsive sites / or
prescription for subgingival dosage doxycycline: i. 2.5 mg chlorhexidine chip ii. 10% doxycycline gel iii. 1 mg minocycline microsphere power iv. 20 mg systemic/ subgingival dosage doxycycline bid
c. Appropriate recare schedule 10. Re-evaluation at appropriate time with referral for non-responsive cases.
• Daily oral hygiene should include toothbrushing; interdental cleansing and tongue deplaquing along with appropriate adjunctive chemotherapy for caries prevention, sensitivity control and antimicrobial benefits.
IMPLEMENTING & INTEGRATION:
• Full-mouth disinfection, or accelerated instrumentation, accounts for a client- and clinician centered approach to periodontal therapy that maximizes clinical outcomes while providing immediate benefits.
• Utilization of ultrasonics in FMD protocols will greater increase the likelihood of success and provide patients with the high-tech therapy they appreciate and deserve.
• Completing periodontal instrumentation within 1 to 2 weeks is an easy factor to control that will lend to fast-tracking aesthetic treatment plans, healing, and referral.

7 www.EducationalDesigns.com © 2018
Post Orthodontic Therapy Considerations:
Additional Considerations: • Collaborate with referring practices to determine protocols, recommendations and patient needs • Provide education on orthodontic options for adults as well as children/teens with referring practices • Offer to monitor periodontal response & health with adult patients • Host or speak at local/regional dental and dental hygiene continuing education events
Additional Action Plans/Considerations: Products - Need to purchase: GP/RDHs to contact: Updates to Assessment Phase: Updates to Clinical Phase: Updates to Post-treatment Phase:

c d a j o u r n a l , v o l 3 9 , n º 1 0
o c t o b e r 2 0 1 1 711
table 1
caries risk Assessment form — children Age 6 and over/Adults
Patient Name: ___________________________________________________________________________________Chart #:________________________________Date:________________________________________________________
Assessment date: is this (please circle) baseline or recall
disease indicators (Any one “yes” signifies likely “high risk” and to do a bacteria test**)
yes = circle yes = circle yes = circle
Visible cavities or radiographic penetration of the dentin yes
Radiographic approximal enamel lesions (not in dentin) yes
White spots on smooth surfaces yes
Restorations last 3 years yes
risk factors (Biological predisposing factors) yes
MS and LB both medium or high (by culture**) yes
Visible heavy plaque on teeth yes
Frequent snack (> 3x daily between meals) yes
Deep pits and fissures yes
Recreational drug use yes
Inadequate saliva flow by observation or measurement (**If measured, note the flow rate below)
yes
Saliva reducing factors (medications/radiation/systemic) yes
Exposed roots yes
Orthodontic appliances yes
Protective factors
Lives/work/school fluoridated community yes
Fluoride toothpaste at least once daily yes
Fluoride toothpaste at least 2x daily yes
Fluoride mouthrinse (0.05% NaF) daily yes
5,000 ppm F fluoride toothpaste daily yes
Fluoride varnish in last 6 months yes
Office F topical in last 6 months yes
Chlorhexidine prescribed/used one week each of last 6 months yes
Xylitol gum/lozenges 4x daily last 6 months yes
Calcium and phosphate paste during last 6 months yes
Adequate saliva flow (> 1 ml/min stimulated) yes
**Bacteria/saliva test results: Ms: lB: flow rate: ml/min. date:
VISUALIZE CARIES BALANCE(Use circled indicators/factors above)(EXTREME RISK = HIGH RISK + SEVERE SALIVARY GLAND HYPOFUNCTION)CARIES RISK ASSESSMENT (CIRCLE): EXTREME HIGH MODERATE LOW
Doctor signature/#: _______________________________________________________________________________________________________________________ Date:_________________________________________________________
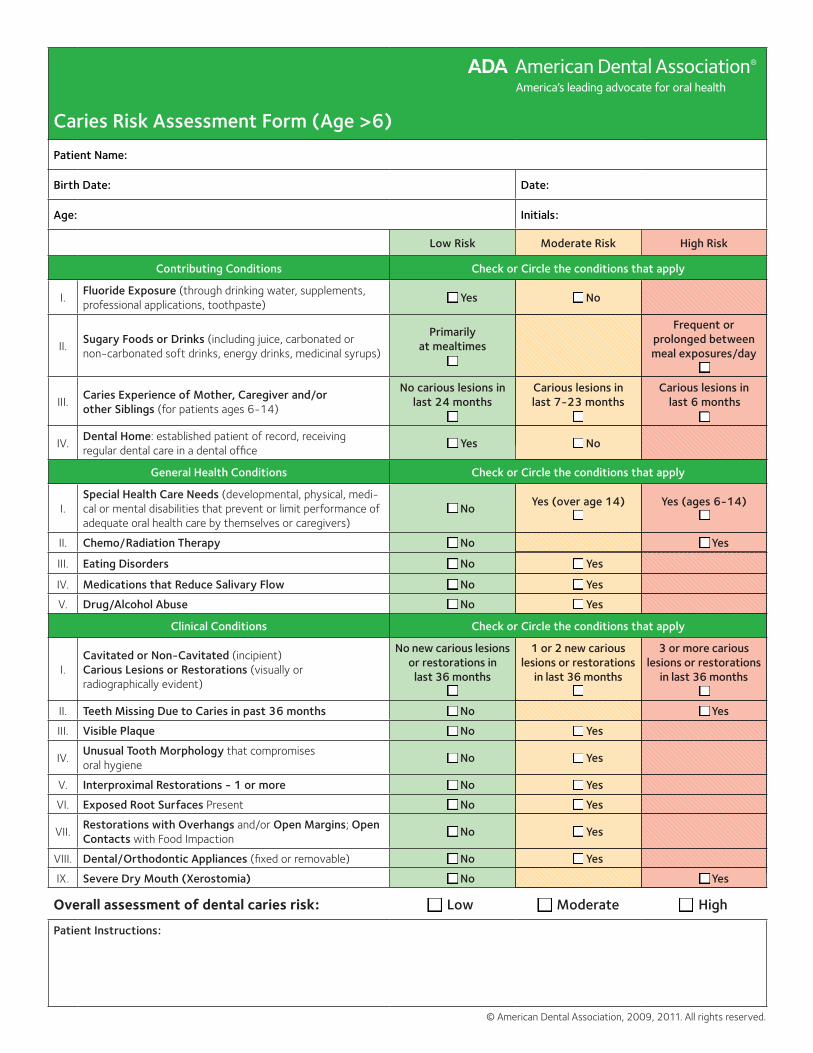
Caries Risk Assessment Form (Age >6)
Patient Name:
Birth Date: Date:
Age: Initials:
Low Risk Moderate Risk High Risk
Contributing Conditions Check or Circle the conditions that apply
I.Fluoride Exposure (through drinking water, supplements,
professional applications, toothpaste) Yes No
II.Sugary Foods or Drinks (including juice, carbonated or
non-carbonated soft drinks, energy drinks, medicinal syrups)
Primarily at mealtimes
Frequent or prolonged between meal exposures/day
III.Caries Experience of Mother, Caregiver and/or other Siblings (for patients ages 6-14)
No carious lesions in last 24 months
Carious lesions in last 7-23 months
Carious lesions in last 6 months
IV. Dental Home: established patient of record, receiving
regular dental care in a dental office Yes No
General Health Conditions Check or Circle the conditions that apply
I.
Special Health Care Needs (developmental, physical, medi-
cal or mental disabilities that prevent or limit performance of
adequate oral health care by themselves or caregivers)
NoYes (over age 14) Yes (ages 6-14)
II. Chemo/Radiation Therapy No Yes
III. Eating Disorders No Yes
IV. Medications that Reduce Salivary Flow No Yes
V. Drug/Alcohol Abuse No Yes
Clinical Conditions Check or Circle the conditions that apply
I.
Cavitated or Non-Cavitated (incipient)
Carious Lesions or Restorations (visually or
radiographically evident)
No new carious lesions or restorations in
last 36 months
1 or 2 new carious lesions or restorations
in last 36 months
3 or more carious lesions or restorations
in last 36 months
II. Teeth Missing Due to Caries in past 36 months No Yes
III. Visible Plaque No Yes
IV.Unusual Tooth Morphology that compromises
oral hygiene No Yes
V. Interproximal Restorations - 1 or more No Yes
VI. Exposed Root Surfaces Present No Yes
VII.Restorations with Overhangs and/or Open Margins; Open
Contacts with Food Impaction No Yes
VIII. Dental/Orthodontic Appliances (fixed or removable) No Yes
IX. Severe Dry Mouth (Xerostomia) No Yes
Overall assessment of dental caries risk: Low Moderate High
Patient Instructions:
© American Dental Association, 2009, 2011. All rights reserved.

Circle or check the boxes of the conditions that apply. Low Risk = only conditions in “Low Risk” column present;
Moderate Risk = only conditions in “Low” and/or “Moderate Risk” columns present; High Risk = one or more
conditions in the “High Risk” column present.
The clinical judgment of the dentist may justify a change of the patient’s risk level (increased or decreased) based
on review of this form and other pertinent information. For example, missing teeth may not be regarded as high
risk for a follow up patient; or other risk factors not listed may be present.
The assessment cannot address every aspect of a patient’s health, and should not be used as a replacement for
the dentist’s inquiry and judgment. Additional or more focused assessment may be appropriate for patients with
specific health concerns. As with other forms, this assessment may be only a starting point for evaluating the
patient’s health status.
This is a tool provided for the use of ADA members. It is based on the opinion of experts who utilized the most
up-to-date scientific information available. The ADA plans to periodically update this tool based on: 1) member
feedback regarding its usefulness, and; 2) advances in science. ADA member-users are encouraged to share their
opinions regarding this tool with the Council on Dental Practice.
Caries Risk Assessment Form (Age >6)

716 O C T O B E R 2 0 0 7
C D A J O U R N A L , V O L 3 5 , N º 1 0TA
BLE
1
Risk
Lev
el##
#**
*
Freq
uenc
y of
Ra
diog
raph
sFr
eque
ncy
ofCa
ries
Reca
ll Ex
ams
Saliv
a Te
st(S
aliv
a Fl
ow &
Bact
eria
l Cul
ture
)
Antib
acte
rials
Chlo
rhex
idin
e X
ylito
l**
**
Fluo
ride
pH C
ontr
olCa
lciu
m
Phos
phat
eTo
pica
l Su
pple
men
ts
Seal
ants
(Res
in-b
ased
or
Glas
s Io
nom
er)
Low
risk
Bite
win
g ra
dio-
grap
hs e
very
24-
36 m
onth
s
Ever
y 6-
12
mon
ths
to re
-ev
alua
te c
arie
s ris
k
May
be
done
as
a ba
se li
ne re
fer-
ence
for n
ew
patie
nts
Per s
aliv
a te
st if
don
eO
TC fl
uorid
e-co
ntai
ning
to
othp
aste
twic
e da
ily,
afte
r bre
akfa
st a
nd a
t be
dtim
e. O
ptio
nal: N
aF
varn
ish
if ex
cess
ive
root
ex
posu
re o
r sen
sitiv
ity
Not
requ
ired
Not
requ
ired
Opt
iona
l: for
ex
cess
ive
root
ex
posu
re o
r sen
-si
tivity
Opt
iona
l or a
s pe
r ICD
AS s
eal-
ant p
roto
col
(TAB
LE 2
)
Mod
erat
e ris
kBi
tew
ing
radi
o-gr
aphs
eve
ry 18
-24
mon
ths
Ever
y 4-
6 m
onth
s to
re-
eval
uate
car
ies
risk
May
be
done
as
a ba
se li
ne re
fer-
ence
for n
ew
patie
nts
or if
th
ere
is s
uspi
cion
of
hig
h ba
cter
ial
chal
leng
e an
d to
as
sess
eff
icac
y an
d pa
tient
coo
p-er
atio
n
Per s
aliv
a te
st if
don
e Xy
litol
(6-1
0 gr
ams/
day)
gu
m o
r can
dies
. Tw
o ta
bs
of g
um o
r tw
o ca
ndie
s fo
ur ti
mes
dai
ly
OTC
fluo
ride-
cont
aini
ng
toot
hpas
te tw
ice
daily
pl
us: 0
.05%
NaF
rins
e da
ily. I
nitia
lly, 1
-2 a
pp o
f N
aF v
arni
sh; 1
app
at 4
-6
mon
th re
call
Not
requ
ired
Not
requ
ired
Opt
iona
l: for
ex
cess
ive
root
ex
posu
re o
r sen
-si
tivity
As p
er IC
DAS
seal
ant p
roto
col
( TAB
LE 2
)
Hig
h ris
k*Bi
tew
ing
radi
o-gr
aphs
eve
ry 6
-18
mon
ths
or u
ntil
no
cavi
tate
d le
sion
s ar
e ev
iden
t
Ever
y 3-
4 m
onth
s to
re-
eval
uate
car
ies
risk
and
appl
y flu
orid
e va
rnis
h
Saliv
a flo
w te
st
and
bact
eria
l cu
lture
initi
ally
an
d at
eve
ry c
ar-
ies
reca
ll ap
pt. t
o as
sess
eff
icac
y an
d pa
tient
coo
p-er
atio
n
Chlo
rhex
idin
e gl
ucon
ate
0.12
%
10 m
l rin
se fo
r one
min
-ut
e da
ily fo
r one
wee
k ea
ch m
onth
. Xyl
itol (
6-10
gr
ams/
day)
gum
or c
an-
dies
. Tw
o ta
bs o
f gum
or
two
cand
ies
four
tim
es
daily
1.1%
NaF
toot
hpas
te
twic
e da
ily in
stea
d of
re
gula
r flu
orid
e to
oth-
past
e. O
ptio
nal: 0
.2%
N
aF ri
nse
daily
(1 b
ottle
) th
en O
TC 0
.05%
NaF
rin
se 2
X da
ily. I
nitia
lly, 1
-3
app
of N
aF v
arni
sh; 1
app
at
3-4
mon
th re
call
Not
requ
ired
Opt
iona
l:Ap
ply
calc
ium
/ ph
osph
ate
past
ese
vera
l tim
es
daily
As p
er IC
DAS
seal
ant p
roto
col
( TAB
LE 2
)
Extr
eme
risk*
*(H
igh
risk
plus
dr
y m
outh
or
spec
ial n
eeds
)
Bite
win
g ra
dio-
grap
hs e
very
6
mon
ths
or u
ntil
no
cavi
tate
d le
sion
s ar
e ev
iden
t
Ever
y 3
mon
ths
to re
-eva
luat
e ca
ries
risk
and
appl
y flu
orid
e va
rnis
h.
Saliv
a flo
w te
st
and
bact
eria
l cu
lture
initi
ally
an
d at
eve
ry c
ar-
ies
reca
ll ap
pt. t
o as
sess
eff
icac
y an
d pa
tient
coo
p-er
atio
n
Chlo
rhex
idin
e 0.
12%
(p
refe
rabl
y CH
X in
wat
er
base
rins
e) 10
ml r
inse
fo
r one
min
ute
daily
for
one
wee
k ea
ch m
onth
. Xy
litol
(6-1
0 gr
ams/
day)
gu
m o
r can
dies
. Tw
o ta
bs
of g
um o
r tw
o ca
ndie
s fo
ur ti
mes
dai
ly
1.1%
NaF
toot
hpas
te
twic
e da
ily in
stea
d of
re
gula
r flu
orid
e to
oth-
past
e. O
TC 0
.05%
NaF
rin
se w
hen
mou
th fe
els
dry,
afte
r sna
ckin
g,
brea
kfas
t, an
d lu
nch.
In
itial
ly, 1
-3 a
pp. N
aF
varn
ish;
1 ap
p at
3 m
onth
re
call.
Acid
-neu
tral
izin
g rin
ses
as n
eede
d if
mou
th fe
els
dry,
afte
r sna
ckin
g,
bedt
ime
and
afte
r br
eakf
ast.
Baki
ng
soda
gum
as
need
ed
Requ
ired
Appl
y ca
lciu
m/ p
hos-
phat
e pa
ste
twic
e da
ily
As p
er IC
DAS
seal
ant p
roto
col
( TAB
LE 2
)
* Pat
ient
s w
ith o
ne (o
r mor
e) c
avita
ted
lesi
on(s
) are
hig
h-ris
k pa
tient
s. **
Pat
ient
s w
ith o
ne (o
r mor
e) c
avita
ted
lesi
on(s
) and
sev
ere
hypo
saliv
atio
n ar
e ex
trem
e-ris
k pa
tient
s. **
* All
rest
orat
ive
wor
k to
be
done
with
th
e m
inim
ally
inva
sive
phi
loso
phy
in m
ind.
Exi
stin
g sm
ooth
sur
face
lesi
ons
that
do
not p
enet
rate
the
DEJ
and
are
not
cav
itate
d sh
ould
be
trea
ted
chem
ical
ly, n
ot s
urgi
cally
. For
ext
rem
e-ris
k pa
tient
s, u
se h
oldi
ng c
are
with
gla
ss io
nom
er m
ater
ials
unt
il ca
ries
prog
ress
ion
is c
ontr
olle
d. P
atie
nts
with
app
lianc
es (R
PDs,
pro
stho
dont
ics)
requ
ire e
xcel
lent
ora
l hyg
iene
toge
ther
with
inte
nsiv
e flu
orid
e th
erap
y e.
g., h
igh
fluor
ide
toot
h-pa
ste
and
fluor
ide
varn
ish
ever
y th
ree
mon
ths.
Whe
re in
dica
ted,
ant
ibac
teria
l the
rapy
to b
e do
ne in
con
junc
tion
with
rest
orat
ive
wor
k. #
## F
or a
ll ris
k le
vels
: Pat
ient
s m
ust m
aint
ain
good
ora
l hyg
iene
and
a d
iet l
ow in
fr
eque
ncy
of fe
rmen
tabl
e ca
rboh
ydra
tes.
****
Xyl
itol i
s no
t goo
d fo
r pet
s (e
spec
ially
dog
s).
Carie
s M
anag
emen
t by
Risk
Ass
essm
ent
Clin
ical
Gui
delin
es fo
r Pat
ient
s Ag
e 6
and
Old
er
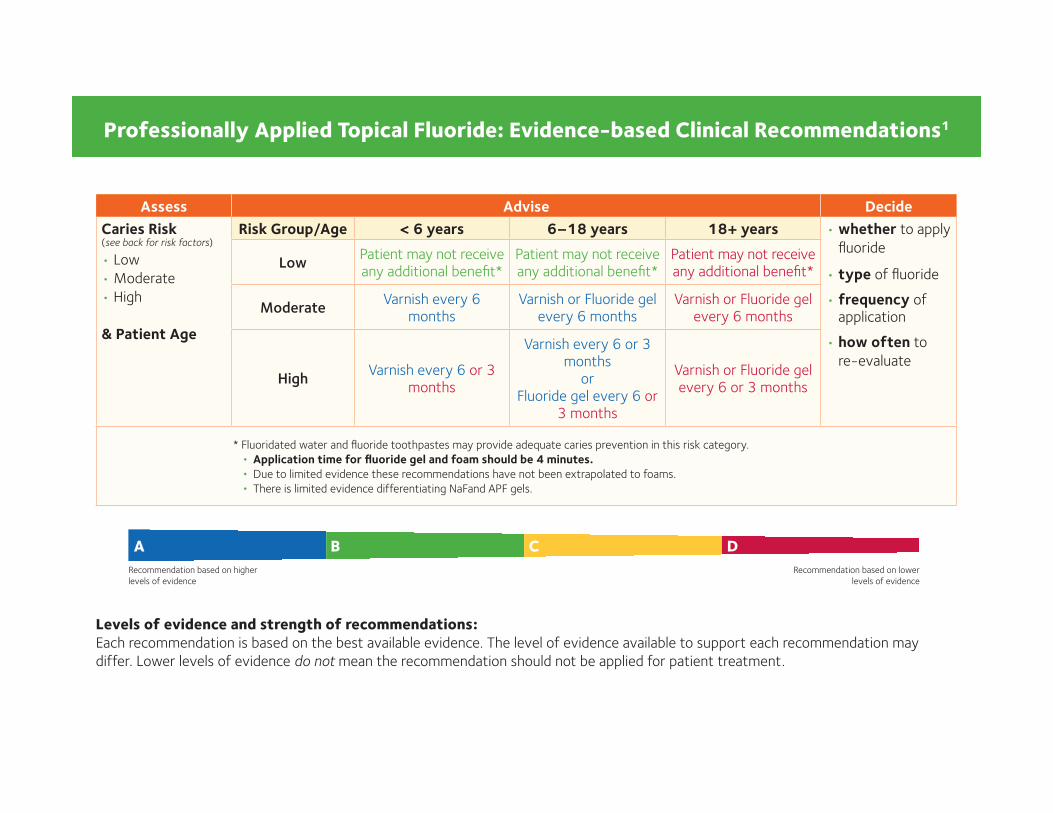
Professionally Applied Topical Fluoride: Evidence-based Clinical Recommendations1
Levels of evidence and strength of recommendations:Each recommendation is based on the best available evidence. The level of evidence available to support each recommendation may
differ. Lower levels of evidence do not mean the recommendation should not be applied for patient treatment.
Assess Advise DecideCaries Risk(see back for risk factors)
• Low
• Moderate
• High
& Patient Age
Risk Group/Age < 6 years 6–18 years 18+ years • whether to apply
fl uoride
• type of fl uoride
• frequency of application
• how often to
re-evaluate
LowPatient may not receive any additional benefi t*
Patient may not receive any additional benefi t*
Patient may not receive any additional benefi t*
ModerateVarnish every 6
monthsVarnish or Fluoride gel
every 6 monthsVarnish or Fluoride gel
every 6 months
HighVarnish every 6 or 3
months
Varnish every 6 or 3 months
orFluoride gel every 6 or
3 months
Varnish or Fluoride gel every 6 or 3 months
* Fluoridated water and fl uoride toothpastes may provide adequate caries prevention in this risk category.
• Application time for fl uoride gel and foam should be 4 minutes. • Due to limited evidence these recommendations have not been extrapolated to foams.
• There is limited evidence differentiating NaFand APF gels.
A B C DRecommendation based on higher
levels of evidence
Recommendation based on lower
levels of evidence
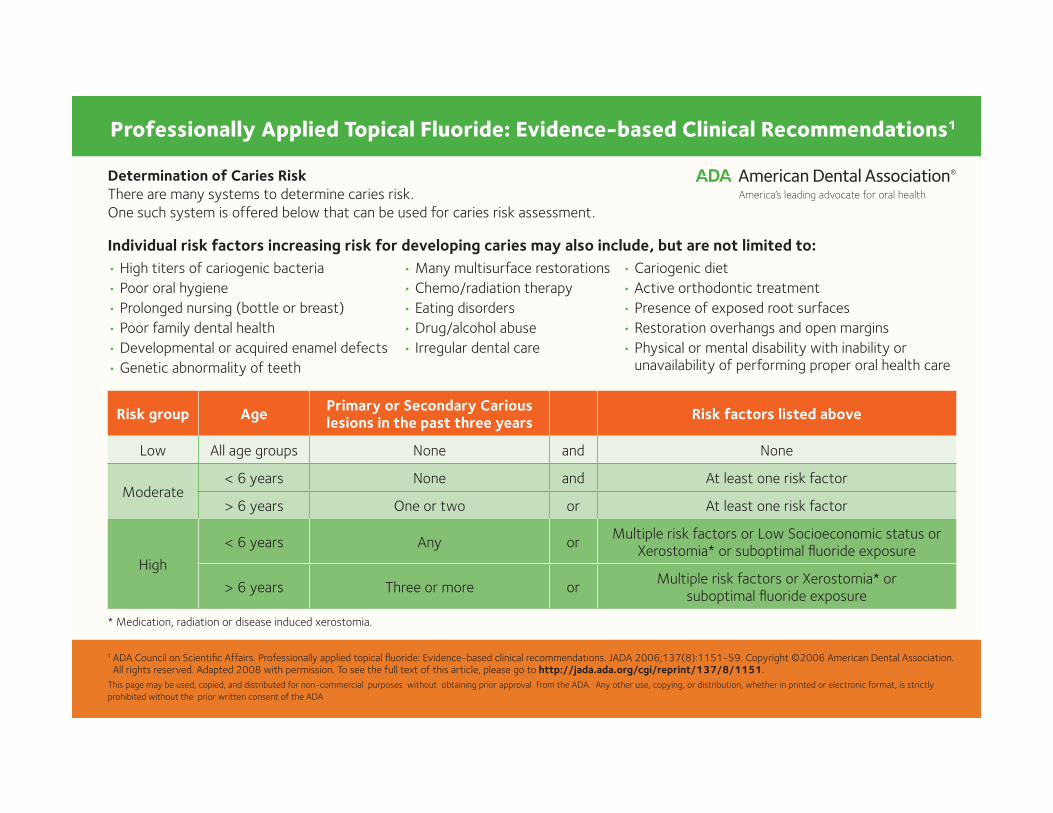
Determination of Caries Risk
There are many systems to determine caries risk.
One such system is offered below that can be used for caries risk assessment.
* Medication, radiation or disease induced xerostomia.
1 ADA Council on Scientifi c Affairs. Professionally applied topical fl uoride: Evidence-based clinical recommendations. JADA 2006;137(8):1151-59. Copyright ©2006 American Dental Association. All rights reserved. Adapted 2008 with permission. To see the full text of this article, please go to http://jada.ada.org/cgi/reprint/137/8/1151.
This page may be used, copied, and distributed for non-commercial purposes without obtaining prior approval from the ADA. Any other use, copying, or distribution, whether in printed or electronic format, is strictly
prohibited without the prior written consent of the ADA
Professionally Applied Topical Fluoride: Evidence-based Clinical Recommendations1
Individual risk factors increasing risk for developing caries may also include, but are not limited to:• High titers of cariogenic bacteria
• Poor oral hygiene
• Prolonged nursing (bottle or breast)
• Poor family dental health
• Developmental or acquired enamel defects
• Genetic abnormality of teeth
• Many multisurface restorations
• Chemo/radiation therapy
• Eating disorders
• Drug/alcohol abuse
• Irregular dental care
• Cariogenic diet
• Active orthodontic treatment
• Presence of exposed root surfaces
• Restoration overhangs and open margins
• Physical or mental disability with inability or unavailability of performing proper oral health care
Risk group Age Primary or Secondary Carious lesions in the past three years Risk factors listed above
Low All age groups None and None
Moderate< 6 years None and At least one risk factor
> 6 years One or two or At least one risk factor
High
< 6 years Any orMultiple risk factors or Low Socioeconomic status or
Xerostomia* or suboptimal fl uoride exposure
> 6 years Three or more orMultiple risk factors or Xerostomia* or
suboptimal fl uoride exposure

Comprehensive Periodontal Therapy: A Statement by theAmerican Academy of Periodontology*
The American Academy of Periodontology (AAP)periodically publishes reports, statements, and guide-lines on a variety of topics relevant to periodontics.These papers are developed by an appointed commit-tee of experts, and the documents are reviewed andapproved by the AAP Board of Trustees.
The American Academy of Periodontology offersthe following statement that sets forth thescope, objective, and procedures that consti-
tute periodontal therapy. This statement is providedto assist all members of the dental team who provideperiodontal care and should be considered in itsentirety. This statement may also be useful to thosewho supervise, teach, or regulate the provision ofperiodontal therapy.
SCOPE OF PERIODONTALTHERAPY
As a result of advances in knowledge and therapy, themajority of patients can retain their dentition over theirlifetime with proper treatment, reasonable plaque/bi-ofilm control, and continuing care. Periodontics is thespecialty of dentistry that encompasses prevention,diagnosis, and treatment of diseases of the supportingand surrounding tissues of teeth and dental implants.
Thescopeofthespecialtyofperiodonticsalsoencom-passesmaintenanceofthehealth, function,comfort,andesthetics of all supporting structures and tissues in themouth.Thegoalsof periodontal therapyare topreserve,improve, and maintain the natural dentition, dental im-plants, periodontium, and peri-implant tissues in orderto achieve health, comfort, esthetics, and function. Ahealthy periodontium is characterized by the absenceof inflammation,whichmayappearclinicallyasredness,swelling, suppuration, and bleeding on probing.
PERIODONTAL EVALUATION
A comprehensive assessment of a patient’s currenthealth status, history of disease, and risk characteris-
tics is essential to determine the periodontal diagnosisand prognosis of the dentition and/or the suitability ofdental implants.Patientsshould receiveacomprehen-sive periodontal evaluation and their risk factorsshould be identified at least on an annual basis. Suchan evaluation includes discussion with the patient re-garding his/her chief complaint, medical and dentalhistory review, clinical examination, and radiographicanalysis. Microbiologic, genetic, biochemical, or otherdiagnostic tests may also be useful, on an individ-ual basis, for assessing the periodontal status of se-lected individuals or sites. The following proceduresshould be included in a comprehensive periodontalevaluation:
1. Extra- and intraoral examination to detect non-periodontal oral diseases or conditions.
2. Examination of teeth and dental implants toevaluate the topography of the gingiva and relatedstructures; to measure probing depths, the width ofkeratinized tissue, gingival recession, and attachmentlevel; to evaluate the health of the subgingival areawith measures such as bleeding on probing andsuppuration; to assess clinical furcation status; andto detect endodontic–periodontal lesions.
3. Assessment of the presence, degree, and/or dis-tribution of plaque/biofilm, calculus, and gingival in-flammation.
4. Dental examination including caries assessment,proximal contact relationships, the status of dentalrestorations and prosthetic appliances, and othertooth- or implant-related problems.
5. An occlusal examination that includes, but maynot be limited to, determining the degree ofmobility ofteeth and dental implants, occlusal patterns and dis-crepancy, and determination of fremitus.
6. Interpretation of current and comprehensive di-agnostic-quality radiographs to visualize each toothand/or implant in its entirety and assess the quality/quantity of bone and establish bone loss patterns.
7. Evaluation of potential periodontal–systemicinterrelationships.
8. Assessment of the need for and suitability ofdental implants.
9. Determination and assessment of patient riskfactors such as age, diabetes, smoking, cardiovascu-lar disease, and other systemic conditions associated
*This statement was developed under the direction of the Task Force toUpdate the Guidelines for Periodontal Therapy and approved by the Boardof Trustees of the American Academy of Periodontology in November 2010.
DISCLAIMER: This statement represents the views of the Academyregarding periodontal therapy and related procedures. It must be recog-nized, however, that decisions with respect to the treatment of patients mustbe made by the individual practitioner in light of the condition and needs ofeach specific patient. Such decisions should be made in the best judgmentof the practitioner, taking into account all relevant circumstances.
NOTE: The Academy updates guidelines and statements on a periodicbasis. All previous publications should be considered in light of theirhistorical context with regard to current knowledge and practices. doi: 10.1902/jop.2011.117001
J Periodontol • July 2011
943

with development and/or progression of periodontaldisease.
ESTABLISHING A DIAGNOSIS, PROGNOSIS,AND TREATMENT PLAN
Clinical findings together with a diagnosis and prog-nosis should be used to develop a logical plan of treat-ment to eliminate or alleviate the signs and symptomsof periodontal diseases, thereby arresting or slowingfurther disease progression. The treatment plan shouldbe used to establish the methods and sequence of de-livering appropriate periodontal treatment, which mayinclude non-surgical, surgical, regenerative, and cos-metic periodontal therapy or dental implant place-ment. When indicated, the plan should include:
1. Medical and dental consultation or referral fortreatment, when appropriate.
2. Surgical and non-surgical periodontal and im-plant procedures to be performed.
3. Consideration of adjunctive restorative, pros-thetic, orthodontic, and/or endodontic consultation ortreatment.
4. Provision for ongoing reevaluation during peri-odontal or dental implant therapy and throughout themaintenance phase of treatment.
5. Consideration of diagnostic testing that may in-clude microbiologic, genetic, or biochemical assess-ment or monitoring during the course of periodontaltherapy.
6. Consideration of risk factors including, but notlimited to, diabetes and smoking, which play a rolein development, progression, and management ofperiodontal diseases.
7. Periodontal maintenance program including on-going evaluation and reevaluation for treatment.
INFORMED CONSENTAND PATIENT RECORDS
Informed consent should be obtained prior to thecommencement of therapy. Complete records ofthe periodontal examination (including full charting),diagnosis, treatment, and recommended follow-upare essential and should be maintained according tostate law. Information given to the patient should in-clude the following:
1. The diagnosis, etiology, proposed therapy, pos-sible alternative treatment(s), and the prognosis withand without the proposed therapy or possible alterna-tives.
2. Recommendations for treatment to be per-formed by other dentists or physicians.
3. The reasonably foreseeable inherent risks andpotential complications associated with the proposedtherapy, including failure with the ultimate loss ofteeth or dental implants.
4. The need for periodontalmaintenance treatmentafter active therapy due to the potential for disease re-currence.
TREATMENT PROCEDURES
When indicated, treatment should include:
1. Patient education, training in oral hygiene, andcounseling on control of risk factors (e.g., stress,medical status, smoking, etc.) with appropriate refer-ral if needed.
2. Management of periodontal–systemic interrela-tionships, when appropriate.
3. Removal of supra- and subgingival bacterialplaque/biofilm and calculus by comprehensive, me-ticulous periodontal scaling and root planing. In someinstances, these proceduresmay be incorporated intothe surgical treatment.
4. Chemotherapeutic agents may be used as ap-propriate to reduce, eliminate, or change the qualityof microbial pathogens, or to alter the host responsethrough local or systemic delivery.
5. Resective procedures to reduce or eliminateperiodontal pockets and create an acceptable gingi-val form that facilitates oral hygiene and periodontalmaintenance. Soft tissue procedures include gingi-vectomy, gingivoplasty, and various mucogingivalflap procedures. Osseous procedures include ostec-tomy and osteoplasty. Dental tissue proceduresinclude root resection, tooth hemisection, and odon-toplasty. Combined dental tissue and osseous proce-dures may be required.
6. Periodontal regenerative procedures includingbone replacement grafts, use of biologics, root biomo-dification, guided tissue regeneration, and combina-tions of these procedures for osseous, furcation, andgingival recession defects. Periodontal/oral recon-structive procedures include guided bone regenera-tion, ridge augmentation, ridge preservation, implantsite development, and sinus grafting.
7. Periodontal plastic surgery for gingival augmen-tation, correction of recession or soft tissue defor-mities, or enhancement of oral esthetics.
8. Occlusal therapy that may include tooth move-ment, occlusal adjustment, splinting, periodontally ac-celeratedosteogenicorthodontics, or biteguard therapyas a means to establish and maintain occlusal health.
9. Preprosthetic periodontal procedures includingexploratory flap surgery, resective procedures, regen-erativeprocedures,mucogingival procedures, or crownlengthening.
10. Selective extraction of teeth, roots, or implants.11. Surgical placement of dental implants andman-
agement of peri-implant disease.12. Procedures to facilitate orthodontic treatment
including tooth exposure, frenulectomy, fiberotomy,
Comprehensive Periodontal Therapy Volume 82 • Number 7
944
temporary anchorage devices, and gingival augmen-tation.
13. Finishing procedures, which include post-treatment evaluation with review and reinforcementof daily oral hygiene when appropriate.
EVALUATION OF THERAPY
Upon completion of planned periodontal therapy, therecord should document that:
1. The patient has been counseled on why and howto perform an effective daily personal oral hygieneprogram including managing their own personal riskfactors associated with development and/or progres-sion of periodontal diseases.
2. All indicated therapeutic procedures have beenperformed.
3. The patient’s response to therapy has been eval-uated, and treatment objectives have been met.
4. A recommendation has been made for the cor-rection of any tooth form, tooth position, restoration,or prosthesis considered to be contributing to the peri-odontal disease process.
5. An appropriate professional periodontalmainte-nance program, specific to individual circumstances,has been recommended to the patient for long-termcontrol of his/her condition, as well as for the mainte-nance of dental implants, if present. This should in-clude professional management of those risk factorsassociated with development and/or progression ofperiodontal diseases including, but not limited to,smoking and diabetes.
FACTORS MODIFYING RESULTS
The results of periodontal therapy may be adverselyaffected by factors that include systemic diseases; in-adequate plaque/biofilm control; unknown or unde-terminable etiologies; pulpal–periodontal problems;inability or failure of thepatient to follow the suggestedtreatment or maintenance program; adverse envi-ronmental influences such as smoking and stress;occlusal dysfunction; and uncorrectable anatomic,structural, or iatrogenic causalities.
Patients with medical compromises, those who re-fuse or delay treatment, or those who present withother limitations may be unable to undergo recom-mended procedures required to establish a completelyhealthy periodontium. In those situations, appropriatetherapy to establish the best possible periodontalhealth is indicated.
PERIODONTAL MAINTENANCE THERAPY
Upon completion of active periodontal therapy, peri-odontal maintenance visits should include:
1. Update of medical and dental histories.
2. Evaluation of current extra- and intraoral peri-odontal and peri-implant soft tissues as well as dentalhard tissues and referral when indicated (e.g., fortreatment of carious lesions, pulpal pathoses, or otherconditions) and diagnostic-quality radiographs whenappropriate.
3. Assessment of the oral hygiene status with rein-struction when indicated.
4. Mechanical tooth cleaning to disrupt/removedental plaque, biofilms, stain, and calculus. Local de-livery or systemic chemotherapeutic agents may beused as adjunctive treatment for recurrent or refrac-tory disease.
5. Ongoing assessment of risk factors to identify anindividual who may be more highly susceptible to on-going breakdown of the periodontal or peri-implanttissues, with elimination ormitigation of newor persis-tent risk and etiologic factors with appropriate treat-ment.
6. Identification and treatment of new, recurrent, orrefractory areas of periodontal and peri-implant pa-thoses.
7. Establishment of an appropriate interval for peri-odontal maintenance.
The patient should be kept informed of:
1. Areasofpersistent, recurrent, refractory, ornewlyoccurring periodontal or peri-implant disease.
2. Changes in the periodontal prognosis and riskfactors associated with periodontal diseases.
3. Advisability of further periodontal treatment orretreatment of indicated sites.
4. Status of dental implants.5. Other oral health problems thatmay include car-
ies, defective restorations, and non-periodontal mu-cosal diseases or conditions.
6. Changes that would warrant referral to, or con-sultation with, other dental or medical specialists.
BIBLIOGRAPHYAas JA, Paster BJ, Stokes LN, Olsen I, Dewhirst FE.
Defining the normal bacterial flora of the oral cavity. JClin Microbiol 2005;43:5721-5732.
Abdellatif HM, Burt BA. An epidemiological investigationinto the relative importance of age and oral hygienestatus as determinants of periodontitis. J Dent Res1987;66:13-18.
Albandar JM, Brunelle JA, Kingman A. Destructive peri-odontal disease in adults 30 years of age and older inthe United States, 1988-1994 [published correction ap-pears in J Periodontol 1999;70:351]. J Periodontol 1999;70:13-29.
Albandar JM, Kingman A. Gingival recession, gingivalbleeding, and dental calculus in adults 30 years of ageand older in the United States, 1988-1994. J Periodontol1999;70:30-43.
Albandar JM, Rams TE. Global epidemiology of periodon-tal diseases: An overview. Periodontol 2000 2002;29:7-10.
J Periodontol • July 2011 Comprehensive Periodontal Therapy
945

Patient Name: ________________________________________
Clinician: _____________________________________
Date of Evaluation: ________ / _____ / __________
Initials Specific Considerations Notes
pocket depths
width of keratinized tissue
gingival recession
attachment level
bleeding on probing
furcation status
presence of inflammation
Initials Specific Considerations Notes
presence, degree, and/or distribution of plaque/biofilm
presence, degree, and/or distribution of calculus
Initials Specific Considerations Notes
caries
proximal contact relationships
endodontic/periodontal lesions
status of dental restorations and prosthetic appliances
other tooth or implant related problems
Initials Specific Considerations (but not be limited to) Notes
degree of mobility of teeth and dental implants
occlusal patterns
fremitus
Initials Specific Considerations Notes
quality/quantity of bone
bone loss patterns
Initials Specific Considerations Notes
age
diabetes
smoking
cardiovascular disease
other
COMPREHENSIVE PERIODONTAL EVALUATION
1. TEETH, DENTAL IMPLANTS AND SUBGINGIVAL AREA
2. PLAQUE/BIOFILM
5. DIAGNOSTIC QUALITY RADIOGRAPHS
I
6. DISCUSSION OF PATIENT RISK FACTORS
CHECKLIST
Instructions:
- Review each of the six elements listed below
- Mark your initial by each "Specific Consideration"
- Refer to other patient information, radiographs etc. in the "Notes" section
3. DENTITION
4. OCCLUSION







