The Role of Tranexamic
Acid in Patient Blood
Management
Undergoing Cardiac
Surgery
Dr Sarah Armarego
FANZCA FANZCP
Senior Staff Specialist
John Hunter Hospital
Newcastle

Declaration
Former member of a medical advisory
committee for Pfizer for Tranexamic acid
Disclaimer
This presentation discusses pharmaceutical
products and/or use of products that may
have not been approved by the TGA.
Please consult the approved Product
Information before prescribing.

Tranexamic Acid
• Patient Blood Management in Cardiac Sx
• Role of Antifibrinolytics (TxA)
– Risks/Benefits
• How should we be giving TxA ?
– Pharmacokinetics
– Dose
– Timing


PBM
• The timely application of evidence based
medical and surgical concepts designed to
– Maintain Hb concentration
– Optimise haemostasis and
– Minimise blood loss
• In an effort to improve patient outcome • Society for the Advancement of Blood
Management

Importance
• Blood usage in cardiac surgery
– Blood bank data
– Audits
– ANZCTS database
• High
– > 50% to 90%
– Depending on operation

Importance
• April 11
• 20 Cardiac, including 2 redos
• ? Elective MVR take back outlayer
PC 66 3.5 per pt
Plts 17 0.9 per pt
Novo 7 0
FFP 58 3.1 per pt
Cryo 85 4.5 per pt
Importance
• NOT IN MY UNIT
– Transfusion rate low
intraoperative
– Transfusions occurring
ICU/postop

The 3 Pillars
Antifibrinolytics
• Maintain Hb concentration
– By reducing blood loss
• Optimise Haemostasis
– Preventing secondary fibrinolysis
Evidence
• Overwhelming number of
– Observational studies
– Prospective studies
– Meta-analyses – Cochrane and otherwise
• TxA v EACA v Aprotinin v Placebo

Evidence
• Decreased blood loss
• Decreased RBC transfusion
• Decreased other blood products (?)
• Decreased take-backs

Evidence
• ? Decreased Mortality
• ? Decreased Morbidity
• ? Decreased ventilator time
• ? Decreased LOS – ICU
• ? Decreased LOS - Hospital

Evidence
• BENEFITS
– Aprotinin > TXA ~ EACA
– MOA – antifibrinolytic and anti-inflammatory
• RISKS
– Aprotinin > TXA ~ EACA
– Non-cardiac mortality
– ? Why

BALL PARK FIGURES
• Cochrane Analysis
2011
– 252 RCT
– 25 000 participants

Blood Loss
Aprotinin Tranexamic acid EACA
CI CI CI
RBC Tx ↓ 34%
RR 0.66
0.60-0.72 ↓ 39%
RR 0.61
0.53-0.70 ↓19%
RR 0.81
0.67-0.99
Intraop blood
loss
↓ 192 ml 280-103 ↓121 mls
180-63 ↓157 ml 277-36
Postop blood
loss
↓ 346 ml 383-308 ↓246 ml
295-199 ↓ 207 276-138
Total blood
loss
↓ 416 ml 520-311 ↓414
525-303 Not enough data
Blood Loss
• Aprotinin Vs TxA
– Cardiac Sx
• ↓ Blood Tx RR 0.87 CI 0.76-0.99
– Combined Sx
• NS RR 0.9 CI 0.81-1.01
– Post op bleeding (cardiac)
• More effective MD -145.81 mls CI -209.99 to –
81.62

Re-op for Bleeding
RR CI 95%
Aprotinin ↓54% 0.46 0.34 – 0.62
Absolute risk reduction of 2% or NNT of 50
TxA No ↓ 0.80 0.55 – 1.17
EACA Trend to ↓ 0.32 0.11 – 0.99
Aprotinin V
TxA
↓ 0.69 0.51 – 0.93
Heavily weighted by BART (63%)
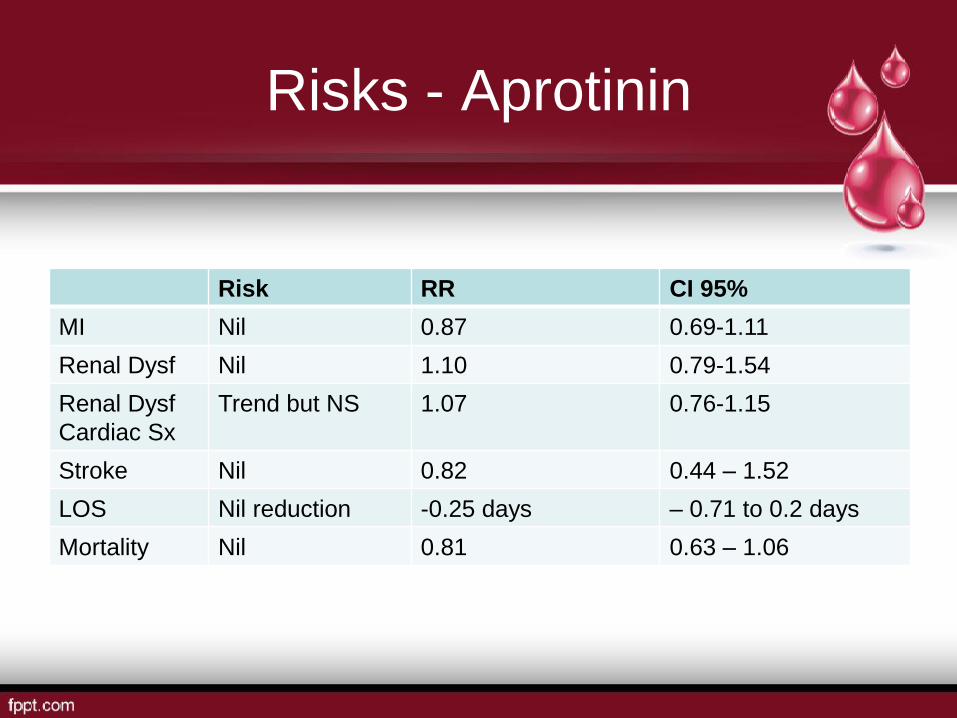
Risks - Aprotinin
Risk RR CI 95%
MI Nil 0.87 0.69-1.11
Renal Dysf Nil 1.10 0.79-1.54
Renal Dysf
Cardiac Sx
Trend but NS 1.07 0.76-1.15
Stroke Nil 0.82 0.44 – 1.52
LOS Nil reduction -0.25 days – 0.71 to 0.2 days
Mortality Nil 0.81 0.63 – 1.06
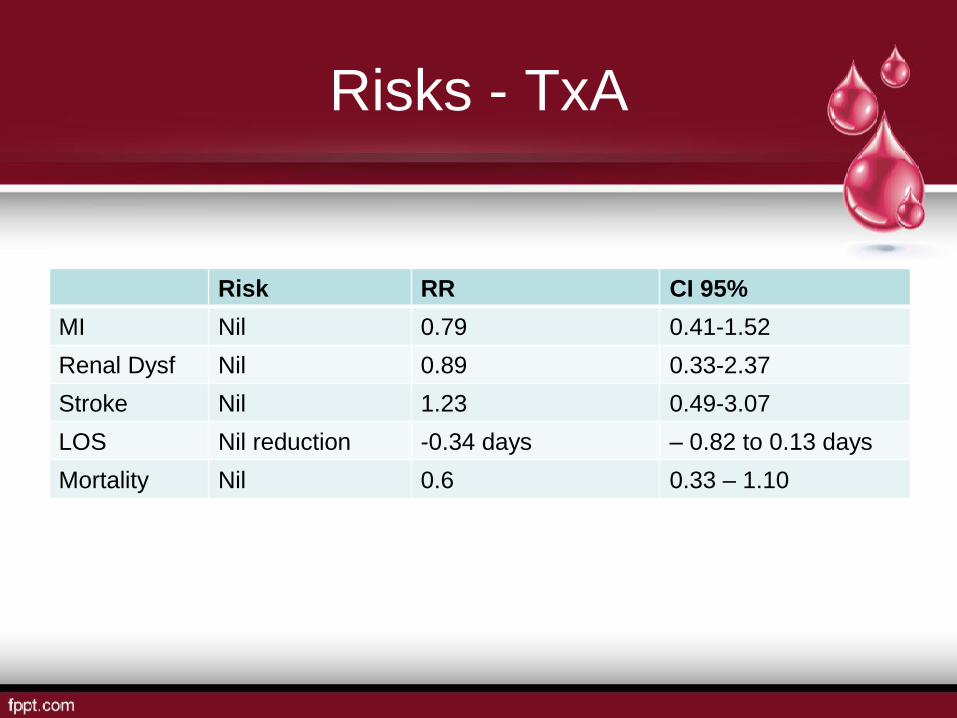
Risks - TxA
Risk RR CI 95%
MI Nil 0.79 0.41-1.52
Renal Dysf Nil 0.89 0.33-2.37
Stroke Nil 1.23 0.49-3.07
LOS Nil reduction -0.34 days – 0.82 to 0.13 days
Mortality Nil 0.6 0.33 – 1.10

Risks - EACA
Risk RR CI 95%
MI Nil 0.88 0.48 -1.63
Renal Dysf Nil 0.41 0.14-1.22
Stroke Nil 0.62 0.16-2.36
LOS Nil reduction 0.58 days – 3.17 to 4.33 d
Mortality Nil 0.6 0.33 – 1.10

Risks
• Aprotinin vs TxA and EACA
– MI - ↑NS
• RR 1.11, CI 0.82-1.50
– Mortality – ↑
• RR 0.1.39, CI 1.02-1.89
• Most data comes from BART

STUDY PROBLEMS
• Different dosing regimes
– Bolus +/- Infusion
– Pump prime +/-
– Adjustment for eGFR
– Length of infusion (up to
12h)

STUDY PROBLEMS
• PBM
– Cell savers
– Pleural drainage
reinfusion
– Transfusion triggers
– Pump volume
especially paeds
– Re-sternotomy def
– Change in PBM

STUDY PROBLEMS
• Look at benefits but not risks
– Prothrombotic risks
• MI
• Stroke
• DVT/PE
– Renal function
– Seizures
• Small numbers

Seizures
N Pre Post TxA dose
Murkin
2010
669 Papworth
London Health Sciences
Centre Canada
1.3% 3.8% 61- 259 mg/kg
71-258 mg/kg
Manji
2012
5958 Manitoba 0.2% 1.47% 80mg/kg
Koster
2013
4883 North Rhine-Westphalia 1.2% 2.5% 25 mg/kg
Sharma
2014
11529
Toronto General
Hospital
0.58% 1.44% 100 mg/kg
Kalavro
uziotis
2012
8929 Quebec Heart and Lung
Institute
0.73% 1.97% > 100 mg/kg

Seizures
N OR 95% CI
Manji
2012
5958 7.4 2.8-19.3 P<0.001
Koster
2013
4883 2.10 1.29-3.41 P=0.003
Sharma
2014
11529
14.3 5.5-36.7 P<0.001
Kalavrouziotis
2012
8929 2.6 1.7-3.8 P < 0.0001
Seizure Characteristics
• Patient characteristics
– High and moderate dose TxA
– Most open heart
• (CPB)(more complicated ops)
– Older pts
– Renal dysf (dose adjustment/HF)
– More atheroma – Ao, PVD

Seizure Characteristics
• Seizures
– Grand Mal
– Occurring in ICU (observation effect)
– Coincident with sedation weaning
– No ass with new or old infarcts on CT/MRI

Seizure outcome
• ↑ Ventilation time
• ↑ICU stay
• ↑ Hospital stay
• ↑ Mort
– Koster 19% in open heart
– Sharma 2.5 x in hospital
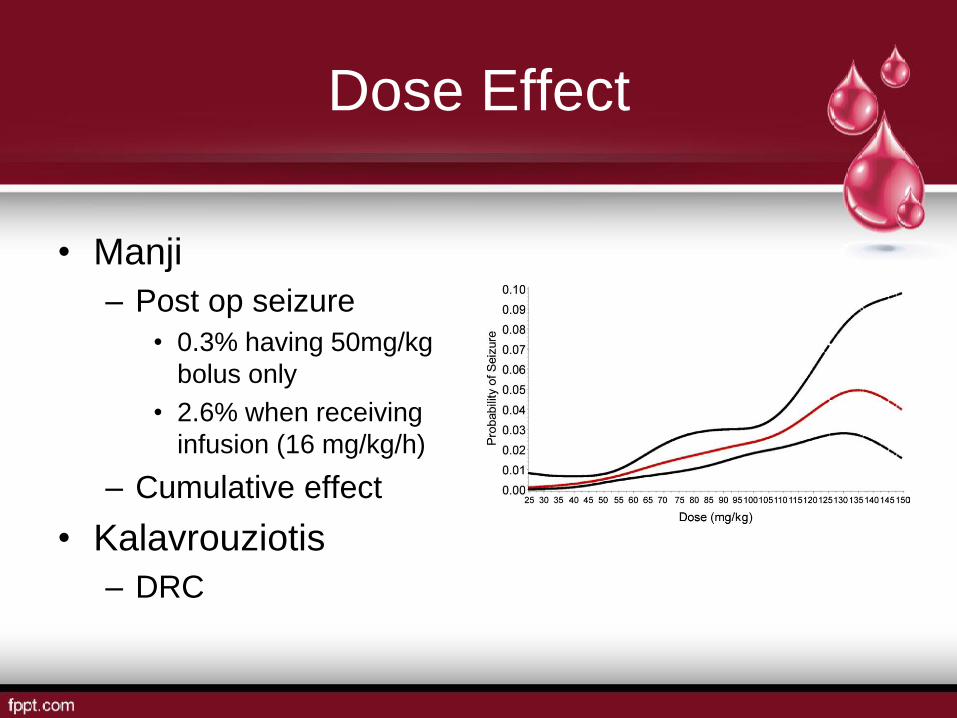
Dose Effect
• Manji
– Post op seizure
• 0.3% having 50mg/kg
bolus only
• 2.6% when receiving
infusion (16 mg/kg/h)
– Cumulative effect
• Kalavrouziotis
– DRC

SEIZURE - Mechanism
• Structural analogue of
glycine
– A major inhibitory NTM
in brain and SC
• Competitively inhibit
glycine R
Pro-convulsant effect
• Topical application to
neural tissue and high
iv doses

Lecker Studies
• TxA inhibits glycine currents when both
pre and co-applied with glycine
• TxA applied alone does not cause currents
and is therefore not a glycine R agonist
• TxA does not modulate glycine R
• TxA moves the glycine response curve to
the right without changing max response

Lecker Studies
• Onset of TxA inhibition was not channel
use dependent
• Recovery from blockade was reversed
immediately after TxA washout
• TxA inhibits GABAA R in brain and SC
• Propofol and isoflurane but not midazolam
attenuated TxA inhibition
• Propofol dose required is 3 x normal

Lecker Studies
• TxA applied to cortical slices evoke
epilepiform activity due to both glycine
inhibition and GABAA inhibition
• Serum and CSF TxA levels from pts
undergoing thoracoabdominal Ao repairs are
within range of causing seizures
• CSF peak levels occur after infusion
cessation
• Subunit variability

Seizures
Why some more than others
• Increased incidence in open heart =
breakdown of BBB
• Microemboli
• Increased permeability for TXA and toxic
cerebral TXA concentrations

GUIDELINES - ABA
RECOMMENDATIONS – medications (tranexamic acid)
• R17
• In adult patients undergoing cardiac surgery, the use
of intravenous tranexamic acid is recommended
(Grade A)
• Body of evidence can be trusted to guide practice
GUIDELINES Society of Thoracic Surgeons and Society of Cardiovascular Anesthesiologists
• Drugs used for intraoperative blood Mx
– Lysine analogues – epsilon aminocaproic acid
(Amicar) and tranexamic acid (Cyklokapron) –
reduce total blood loss and decrease the
number of patients who require blood
transfusion during cardiac procedures and are
indicated for blood conservation
– Level I (A)
GUIDELINES European Society of Anesthesiology
• We recommend that Tranexamic acid or EACA
should be considered before CABG surgery 1A
• We recommend that intraoperative Tranexamic
acid or EACA administration should be
considered to reduce perioperative bleeding in
high-, medium – and low risk cardiovascular
surgery 1A
• We recommend the consideration of Tranexamic
acid (20-25 mg/kg) 1A
THE QUESTION IS NOT WHETHER TO GIVE
TxA BUT HOW MUCH?

BACKGROUND
Australia
• Synthesised by Okamoto in late 50’s
• First regulatory approval Jan 1966 Austria
• TGA approved oral formulation (72,84,87) • Hereditary angioneurotic odema
• Short term use for hyphaema
• Pts with established coagulopathies undergoing
minor Sx
• Menorrhagia

BACKGROUND
Australia
• Aprotinin removed from market by Bayer
in Nov 2007
• SAS use of IV Tranexamic acid increased
• TGA approached Pfizer for approval of IV
form Sept 2010

Background
• Adults
– For the reduction of peri- and post-operative
blood loss and the need for blood transfusion
in patients undergoing cardiac surgery or total
knee arthroplasty or total hip arthroplasty
• Children
– For the reduction of peri- and post-operative
blood loss and the need for blood transfusion
in patients undergoing cardiac surgery

BACKGROUND
• Problems
– A lot changes 50 years (bureaucracy)
– Animal data
– In vitro data
– Minimal PK studies in humans
– No after market surveillance

Dose - PI
• Adults
– 15 mg/kg bolus followed by 4.5mg/kg/h +/- 0.6
mg/kg of the infusion dose added to prime
• Paeds
• 10 mg/kg bolus followed by a rpt bolus of 10
mg/kg during surgery or as an infusion

BART TRAIL DOSE
• Dowd 2002
– 30 adults (CABG, Valve and ASD) divided into
50 mg/kg bolus, 100 mg/kg bolus and 10
mg/kg bolus followed by infusion of 1 mg/kg/h
for 10 hours
• Plasma concentration Vs time curves
• 2 compartmental model
Dowd
• Dosing regimes were
then calculated using
the PK data obtained
and assumptions
about required
plasma concentration
for inhibition of
fibrinolysis (in vitro)
Dowd
• In vitro tissue extracts (Andersson)
– Cp 100 mcg/ml (636 μM) reduce fibrinolytic
activity in tissue extracts by 98 – 100%
– Cp 10 mcg/ml (64 μM) reduce fibrinolytic
activity by 80%
– Cp 16 μg/ml suppresses plasmin-induced plt
activation
– Suggested target 20 - 150 μg/ml

Dowd
Load
Over 30 min
Infusion Prime Cp Inhibition
12 mg/kg 6.5 mg/kg/h 1 mg/kg > 345 μM > 80%
30 mg/kg 16 mg/kg/h 2 mg/kg > 800 μM > 90%

Harrow
• 1995 Pennsylvania
Load
mg/kg
Infusion
Mg/kg/h
N
RBC
5 d
Mean
Blood loss g
0 0 27 26% 552
2.5 0.25 24 38% 504
5 0.50 22 36% 386
10 1.0 21 29% 365
20 2.0 27 26% 344
40 4.0 27 26% 369

Harrow
• Placebo gp showed significant increase in
D dimers
• Dose-response wrt blood lost but not with
blood transfused
• Recommend 10 mg/kg bolus followed by 1
mg/kg/h

ADULTS
• Grassin-Delyle 2013 France
N Cp
Low dose 30 10 mg/kg bolus
1 mg/kg/h infusion
1 mg/kg CPB
(Harrow)
28-55 μg /ml
High dose 31 30 mg/kg
16 mg/kg/h
2 mg/kg CPB
(Dowd)
114-209 μg/ml Increasing
levels
(90%)

ADULTS
• Based on maintaining a plasma conc of
150 to 190 μg/ml
– 46 mg/kg given in one hour followed by an
infusion of
– 11 mg/kg/h in pts 50-75 kg
– 10 mg/kg/h in pts 75-100 kg
– 9 mg/kg/h in pts 100-125 kg

Adults
• Sigaut 2013
N Tx up
to 7 d
FFP Plt Blood loss Rpt
sternotomy
Low
dose
2
8
4
10 mg/kg bolus
1 mg/kg/h
infusion
1 mg/kg CPB
63% 26% 23% 820 +/-
50.7
6%
High
dose
2
8
5
30 mg/kg
16 mg/kg/h
2 mg/kg CPB
60% 18% 15% 590 +/-
50.4
2.5%
P=0.3 P=0.03 P=0.02 P=0.01 P=0.01

Children
• Grassin-Delyle 2013
• 12 M – 12 Y
• Stratified into 3 gps according to weight
– 10-15 kg
– 15-20 kg
– 20-30 kg
• No UF
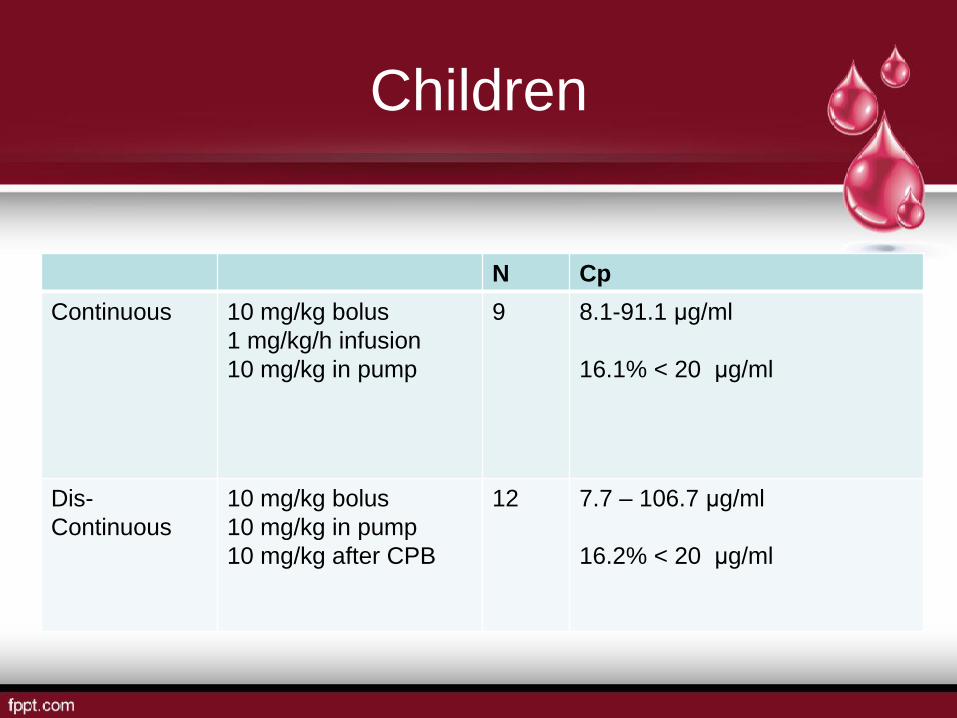
Children
N Cp
Continuous 10 mg/kg bolus
1 mg/kg/h infusion
10 mg/kg in pump
9 8.1-91.1 μg/ml
16.1% < 20 μg/ml
Dis-
Continuous
10 mg/kg bolus
10 mg/kg in pump
10 mg/kg after CPB
12 7.7 – 106.7 μg/ml
16.2% < 20 μg/ml

Children
• Larger portion pump prime cf blood vol
• CPB had a large impact on PK
• Using PK data for Cp 20-30 μg/ml
– Loading dose of 6.5 mg/kg
– Followed by a weight adjusted infusion
– 3.1 mg/kg/h for 5 kg
– 2.0 mg/kg/h for 40 kg

Children
• TxA clearance is approx 3 x lower in
children
• 2 x increase in Central volume
• 4 x increase in peripheral volume
• Increased Vd
• Affect of MUF and hypothermia not
explored

Neonates
• Wesley 2015 Boston Children’s Hospital
• 55 pts aged 2 d to 4 y
• Stratified into 3 gps
– < 2 M
– 2 M-1 y
– >1y and weighing up to 20 kg
• 100 mg/kg bolus followed by 10 mg/kg/h
plus 100 mg/kg in prime

Neonates
N Weight
kg
< 2M 15 2.5-3.8 UF/MUF Hypothermia/
DHCA (8)
2M-1Y 20 3.5-7.6 UF/MUF Hypothermia (19) Re-do (6)
> 1 Y 20 7.7-18 UF only Hypothermia (19) Re-do (16)

Neonates
Age Dose 20 μg/ml 60 μg/ml 150 μg/ml
0-2 M Load mg/kg 15 50 120
Infusion mg/kg/h 2.5 7 17
Prime μg/ml 20 60 150
2-12 M Load mg/kg 9 26 65
Infusion mg/kg/h 2 6 14
Prime μg/ml 20 60 150
> 12 M Load mg/kg 4 13 31
Infusion mg/kg/h 2 5.5 14
Prime μg/ml 20 60 150

Neonates
• NN dosing different to > 1 year
• 2 monthers require higher loading dose
than 12 monthers
• Developmental changes better captured
by age (rather than weight)
• MUF dose not impact significantly on dose
• Dose prime on volume not patient weight

Neonates
• Neonatal cord blood require lower TxA
concentrations to completely prevent
hyperfibrinolysis (Yee 2013)
• 6.54 μg/ml (95% CI 5.19-7.91)
cf 17.5 μg/ml (95% CI 14.59-20.41)
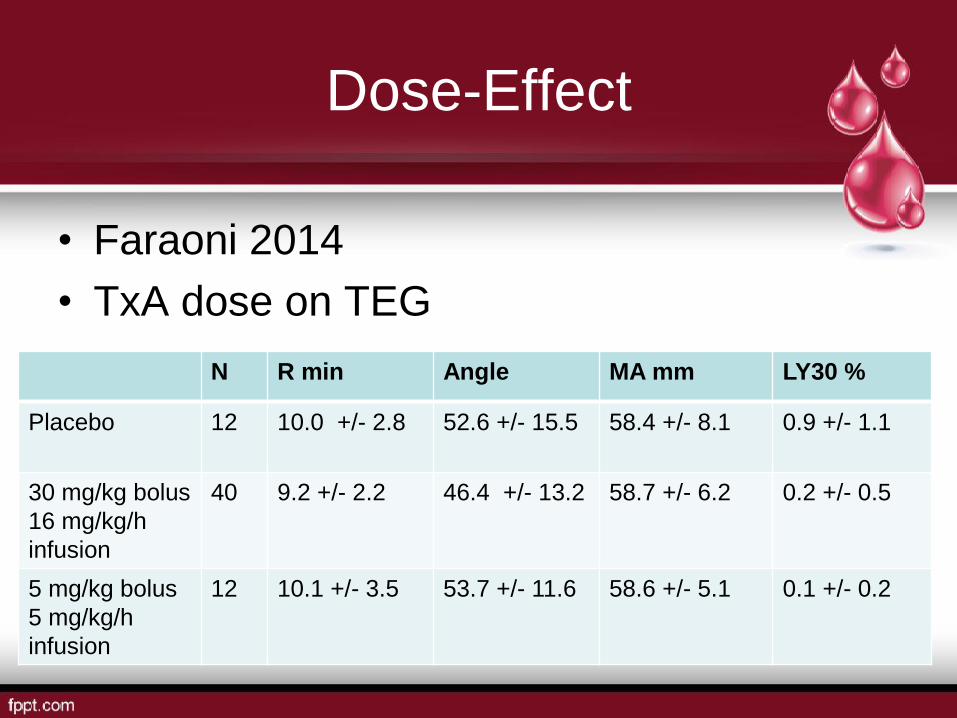
Dose-Effect
• Faraoni 2014
• TxA dose on TEG
N R min Angle MA mm LY30 %
Placebo 12 10.0 +/- 2.8 52.6 +/- 15.5 58.4 +/- 8.1 0.9 +/- 1.1
30 mg/kg bolus
16 mg/kg/h
infusion
40 9.2 +/- 2.2 46.4 +/- 13.2 58.7 +/- 6.2 0.2 +/- 0.5
5 mg/kg bolus
5 mg/kg/h
infusion
12 10.1 +/- 3.5 53.7 +/- 11.6 58.6 +/- 5.1 0.1 +/- 0.2

Where from here?
• Confirmation of PK in
different pt populations
esp paediatrics
• Dose adjustment
requirement for eGFR
• Obesity PK
(hypothermia/UF)

Timing?
• Cumulative dose
effects (infusions in
long cases)
• Total dose limits
• Timing (?12 hours)
– Max secondary
fibrinolysis
• In Vivo dose-effect

THE END







