
Therapy-Induced Encephalopathy Therapy-Induced Encephalopathy in an Allogeneic Hematopoietic in an Allogeneic Hematopoietic
Stem Cell Transplant PatientStem Cell Transplant Patient
Beverly MojicaBeverly Mojica
Pharm.D. Candidate 2011Pharm.D. Candidate 2011
Western University of Health SciencesWestern University of Health Sciences
Medicine RotationMedicine Rotation
City of HopeCity of Hope

OutlineOutline Patient casePatient case Background of encephalopathyBackground of encephalopathy Causes of encephalopathy in HSCT recipientsCauses of encephalopathy in HSCT recipients Drug-induced encephalopathyDrug-induced encephalopathy
TacrolimusTacrolimus MethotrexateMethotrexate CytarabineCytarabine RituximabRituximab
Future directionsFuture directions QuestionsQuestions

Case: N.B.Case: N.B.
N.B. is a 62 year-old male (186.2 cm, 70.7 kg) N.B. is a 62 year-old male (186.2 cm, 70.7 kg) with a history of mantle cell lymphoma with CNS with a history of mantle cell lymphoma with CNS involvement involvement
Admitted on 5/12/10 to City of Hope for an Admitted on 5/12/10 to City of Hope for an allogeneic stem cell transplant from a matched allogeneic stem cell transplant from a matched unrelated donorunrelated donor

Case: N.B.Case: N.B. Past Medical History:Past Medical History:
History of prostate cancer History of prostate cancer Refractory mantle cell lymphoma with CNS involvement Refractory mantle cell lymphoma with CNS involvement
(leptomeningeal)(leptomeningeal) Bell’s PalsyBell’s Palsy
Family History:Family History: Father had prostate cancerFather had prostate cancer Sister had an aneurysm and lives in HollandSister had an aneurysm and lives in Holland
Social History:Social History: Supported by his family including his wifeSupported by his family including his wife Engineer who is self-employed as a consultant in the Engineer who is self-employed as a consultant in the
Siemens/Diagnostic Imaging machinesSiemens/Diagnostic Imaging machines Smoked 1 pack of cigarettes for 20 years (quit in 1979)Smoked 1 pack of cigarettes for 20 years (quit in 1979) Drinks alcohol occasionallyDrinks alcohol occasionally

Case: N.B.Case: N.B.Pertinent Medications:Pertinent Medications:
Drug Dose Date
Rituximab 375 mg/m2 2002-2006
CVP + Rituximab x 8 cycles 2007
Cytarabine 4000 mg q 12 hours IV x 6 doses
4/24 to 4/27
Methotrexate 12 mg IT x 6 doses
5/03 to 5/20
Tacrolimus (1 mg/ml)
1.1 mg IV daily 5/18 to 5/31
Case: N.B.Case: N.B. Clinical HistoryClinical History
5/27:5/27: Confused overnightConfused overnight Tmax: 37 CTmax: 37 C
5/28:5/28: Hallucinations in the morningHallucinations in the morning Tmax: 37.2 CTmax: 37.2 C
5/29: 5/29: Confused overnightConfused overnight Blank staring Blank staring
Keppra 500 mg BID Keppra 500 mg BID Tmax: 37.1 CTmax: 37.1 C

Case: N.B.Case: N.B. MicrobiologyMicrobiology
6/4: 6/4: Stool: rapid CMV and HSV shell vial cultures Stool: rapid CMV and HSV shell vial cultures
negativenegative 6/5:6/5:
Aspergillus Ag negative by EIAAspergillus Ag negative by EIA Cryptococcal Ag serum negativeCryptococcal Ag serum negative Fungitell 1,3 Beta D glucan negative (65 Fungitell 1,3 Beta D glucan negative (65
pg/mL)pg/mL) Toxoplasma gondii from serum not detectedToxoplasma gondii from serum not detected

Case: N.B.Case: N.B.
Electroencephalogram (EEG)Electroencephalogram (EEG) Slow background (6 Hz) consistent with Slow background (6 Hz) consistent with
encephalopathyencephalopathy MRI HeadMRI Head
6/9: No mass effect or focal abnormality6/9: No mass effect or focal abnormality Cytology (spinal tap from omaya catheter)Cytology (spinal tap from omaya catheter)
5/20 : No lymphoma in CSF 5/20 : No lymphoma in CSF 6/15 : No lymphoma in CSF6/15 : No lymphoma in CSF

EncephalopathyEncephalopathy11
Any diffuse disease of the brain that alters brain Any diffuse disease of the brain that alters brain function or structure function or structure
Causes:Causes: Infection (bacteria, virus, or prion)Infection (bacteria, virus, or prion) Metabolic or mitochondrial dysfunctionMetabolic or mitochondrial dysfunction Brain tumor or increased intracranial pressureBrain tumor or increased intracranial pressure Exposure to toxins (i.e. solvents, drugs, alcohol, Exposure to toxins (i.e. solvents, drugs, alcohol,
paints, industrial chemicals, and certain metals)paints, industrial chemicals, and certain metals) RadiationRadiation TraumaTrauma Poor nutritionPoor nutrition IschemiaIschemia
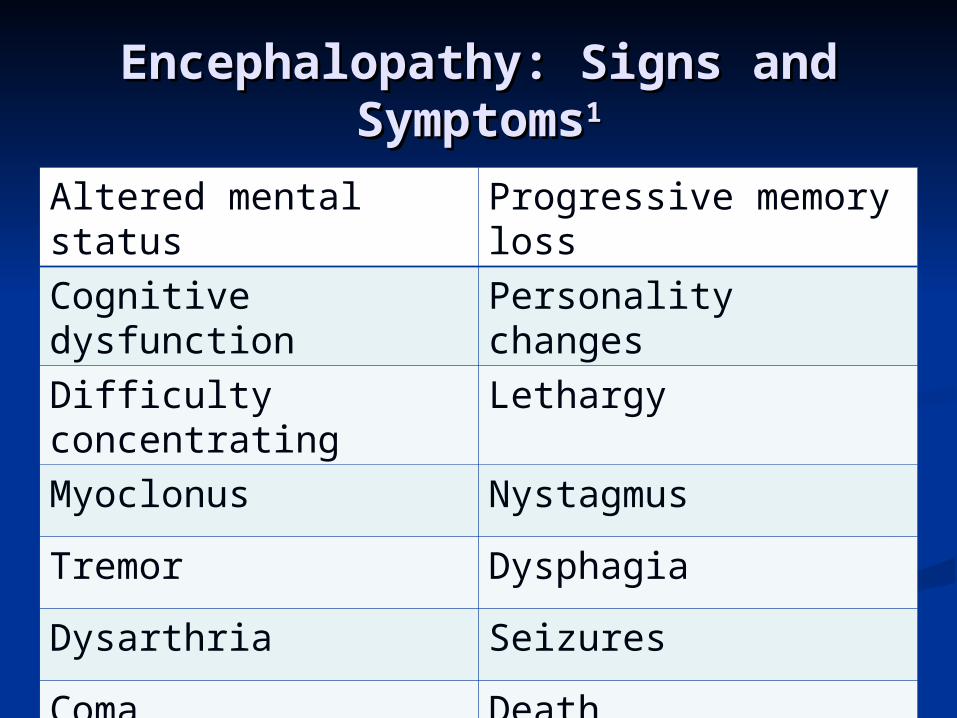
Encephalopathy: Signs and Encephalopathy: Signs and SymptomsSymptoms11
Altered mental status Progressive memory loss
Cognitive dysfunction Personality changes
Difficulty concentrating Lethargy
Myoclonus Nystagmus
Tremor Dysphagia
Dysarthria Seizures
Coma Death
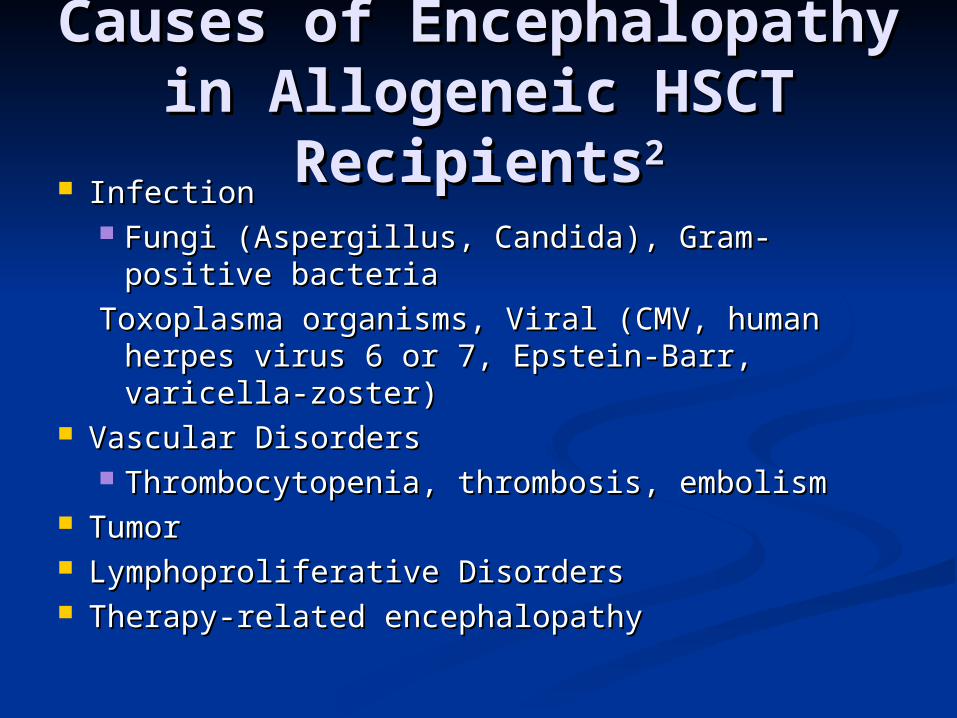
Causes of Encephalopathy in Causes of Encephalopathy in Allogeneic HSCT RecipientsAllogeneic HSCT Recipients22
InfectionInfection Fungi (Aspergillus, Candida), Gram-positive Fungi (Aspergillus, Candida), Gram-positive
bacteriabacteria
Toxoplasma organisms, Viral (CMV, human herpes Toxoplasma organisms, Viral (CMV, human herpes virus 6 or 7, Epstein-Barr, varicella-zoster)virus 6 or 7, Epstein-Barr, varicella-zoster)
Vascular DisordersVascular Disorders Thrombocytopenia, thrombosis, embolismThrombocytopenia, thrombosis, embolism
Tumor Tumor Lymphoproliferative DisordersLymphoproliferative Disorders Therapy-related encephalopathyTherapy-related encephalopathy
TacrolimusTacrolimus3,43,4
MOA: potent inhibition on T-lymphocyte MOA: potent inhibition on T-lymphocyte activation by inhibiting calcineurin phosphatase activation by inhibiting calcineurin phosphatase activity activity
TacrolimusTacrolimus3,63,6
Absorption: Oral: Incomplete and variableAbsorption: Oral: Incomplete and variable Distribution: 0.55-2.47 L/kgDistribution: 0.55-2.47 L/kg Metabolism: Extensively hepatic via CYP3A4 to Metabolism: Extensively hepatic via CYP3A4 to
eight possible metaboliteseight possible metabolites Excretion: Excretion:
Feces (~93%)Feces (~93%) Urine (<2% as unchanged drug)Urine (<2% as unchanged drug)
Biological half-life varies: 3.5-40.5 hoursBiological half-life varies: 3.5-40.5 hours33

Tacrolimus NeurotoxicityTacrolimus Neurotoxicity Incidence: ~5-30%Incidence: ~5-30%77
Posterior reversible encephalopathy syndrome Posterior reversible encephalopathy syndrome (PRES)(PRES)
Initial manifestation:Initial manifestation: Sudden altered mental status, confusion, Sudden altered mental status, confusion,
headache, diminished spontaneity and speech, headache, diminished spontaneity and speech, lethargy, unconsciousness, convulsionslethargy, unconsciousness, convulsions
Not dose-dependentNot dose-dependent2,6,7,82,6,7,8
Can occur at anytime after HSCT (usually within 1 Can occur at anytime after HSCT (usually within 1 month)month)

Tacrolimus NeurotoxicityTacrolimus Neurotoxicity2,5,62,5,6
Mechanism unclear:Mechanism unclear: Direct endothelial damage Direct endothelial damage injury to the injury to the
capillary bed capillary bed alteration of blood-brain alteration of blood-brain barrier (BBB) barrier (BBB) white matter edema white matter edema release of vasoactive peptides (endothelin, release of vasoactive peptides (endothelin, thromboxane, prostacyclin) thromboxane, prostacyclin) vasospasm or vasospasm or interruption of cerebral autoregulationinterruption of cerebral autoregulation

Tacrolimus NeurotoxicityTacrolimus Neurotoxicity5,75,7
Radiologic FindingsRadiologic Findings MRI: edema involving white matter in the MRI: edema involving white matter in the
posterior portions of the cerebral hemispheres posterior portions of the cerebral hemispheres (esp. bilaterally in the parieto-occipital (esp. bilaterally in the parieto-occipital regions); hyperintense lesions (T2 weighted)regions); hyperintense lesions (T2 weighted)
CT: low attenuation of white matterCT: low attenuation of white matter EEG: diffuse slowing or sharp epileptic EEG: diffuse slowing or sharp epileptic
dischargesdischarges

MethotrexateMethotrexate9,109,10
MOA: inhibits DNA synthesis by irreversibly MOA: inhibits DNA synthesis by irreversibly binding to dihydrofolate reductasebinding to dihydrofolate reductase

MethotrexateMethotrexate10,1110,11
Absorption: completely absorbed with parenteral Absorption: completely absorbed with parenteral routeroute
Distribution: widely distributed throughout bodyDistribution: widely distributed throughout body Metabolism: <10% with hepatic aldehydeMetabolism: <10% with hepatic aldehyde
and intestinal bacteriaoxidaseand intestinal bacteriaoxidase Excretion: renal (~90% unchanged in the urine); Excretion: renal (~90% unchanged in the urine);
small amount in fecessmall amount in feces Renal impairment: CNS half-life may reach 19-Renal impairment: CNS half-life may reach 19-
44 hours44 hours Half-life: 4.5 -14 hoursHalf-life: 4.5 -14 hours
Methotrexate Methotrexate NeurotoxicityNeurotoxicity12,13,1412,13,14
AcuteAcute Onset: during or within hours after MTXOnset: during or within hours after MTX Somnolence, confusion, fatigue, seizuresSomnolence, confusion, fatigue, seizures Usually reversibleUsually reversible
Subacute (3-15%)Subacute (3-15%) Onset: days to weeks post MTX treatmentOnset: days to weeks post MTX treatment Stroke-like syndromeStroke-like syndrome
Hemiparesis, seizures, speech disorderHemiparesis, seizures, speech disorder Usually reversibleUsually reversible
ChronicChronic Onset: months to yearsOnset: months to years LeukoencephalopathyLeukoencephalopathy
Dementia, focal seizures, quadriparesis, stuporDementia, focal seizures, quadriparesis, stupor May or may not be reversibleMay or may not be reversible

Methotrexate NeurotoxicityMethotrexate Neurotoxicity15,1615,16
IncidenceIncidence22
< 10% with high dose IV MTX< 10% with high dose IV MTX22
Up to 40% with ITUp to 40% with IT22
Risk factors:Risk factors: Dose-relatedDose-related Age >10Age >10 Cranial irradiationCranial irradiation Concomitant use of cytarabine, daunorubicin, Concomitant use of cytarabine, daunorubicin,
salicylates, sulfonamides or vinca alkaloids salicylates, sulfonamides or vinca alkaloids
Methotrexate NeurotoxicityMethotrexate Neurotoxicity12,14,15,17,1812,14,15,17,18
Mechanism not well establishedMechanism not well established Direct toxic effects on neuronsDirect toxic effects on neurons MTX inhibits dihydrofolate reductaseMTX inhibits dihydrofolate reductase
Increased levels of adenosineIncreased levels of adenosine Dilation of cerebral blood vesselsDilation of cerebral blood vessels Decreased synthesis of biogenic amine Decreased synthesis of biogenic amine
neurotransmittersneurotransmitters Elevated homocysteine:Elevated homocysteine:
Endothelial cell injuryEndothelial cell injury Cerebrovascular infarctsCerebrovascular infarcts

Methotrexate NeurotoxicityMethotrexate Neurotoxicity Route (IV, IT) and dose-dependent (cumulative Route (IV, IT) and dose-dependent (cumulative
exposure) exposure) IV IV >> 1 g/m2 (or frequent IV) 1 g/m2 (or frequent IV)12,16,1812,16,18
IT: 12-15 mg (> 100 mg)IT: 12-15 mg (> 100 mg)1919
Higher risk when IT MTX >50 mg in Higher risk when IT MTX >50 mg in combination with cranial irradiation or combination with cranial irradiation or
systemic (IV) MTX systemic (IV) MTX 1515
Recurrence rate: 10-56% upon rechallengeRecurrence rate: 10-56% upon rechallenge1818
IT MTX must be preservative-freeIT MTX must be preservative-free1818

Methotrexate NeurotoxicityMethotrexate Neurotoxicity14,1514,15
ManagementManagement Antidote for reversal of MTX neurotoxicity: Antidote for reversal of MTX neurotoxicity:
aminophylline 2-5 mg/kg every 6 hoursaminophylline 2-5 mg/kg every 6 hours14,15,1814,15,18
Displaces adenosine from the receptorDisplaces adenosine from the receptor IT MTX overdose: glucarpidase 50 units/kg IT MTX overdose: glucarpidase 50 units/kg
bolus IV injection over 5 minutes bolus IV injection over 5 minutes 1010
Rapidly decrease MTX levels by up to 98% in Rapidly decrease MTX levels by up to 98% in 30 minutes30 minutes
Not available commerciallyNot available commercially Call: 1-866-918-1731 for overnight shippingCall: 1-866-918-1731 for overnight shipping

Methotrexate NeurotoxicityMethotrexate Neurotoxicity10,1610,16
PreventionPrevention Folinic acid (leucovorin rescue)Folinic acid (leucovorin rescue)
100 mg/m2 48 hours after MTX administration q 3 hours 100 mg/m2 48 hours after MTX administration q 3 hours x8 doses followed by 200 mg/m2 x8 doses followed by 200 mg/m2
q 6 hours x4 dosesq 6 hours x4 doses1616
High dose did not compromise cureHigh dose did not compromise cure1616
HydrationHydration1010
2.5 -3.5 L/m2 per day starting 12 hours prior to MTX 2.5 -3.5 L/m2 per day starting 12 hours prior to MTX infusioninfusion
Urinary alkalinazationUrinary alkalinazation1010
50 mL of D5W containing sodium bicarbonate 1 mEq/kg 50 mL of D5W containing sodium bicarbonate 1 mEq/kg IV over 30 minutes q 4-6 hoursIV over 30 minutes q 4-6 hours
CytarabineCytarabine2020
MOA: primary action is inhibition of DNA MOA: primary action is inhibition of DNA polymerase resulting in decreased DNA polymerase resulting in decreased DNA synthesis and repair. synthesis and repair. Cytarabine is specific Cytarabine is specific for the S phase of the for the S phase of the cell cycle (blocks progression cell cycle (blocks progression from the G1 to the S phase).from the G1 to the S phase).

CytarabineCytarabine20,21,2220,21,22 Absorption: Complete with IVAbsorption: Complete with IV Distribution: Widely and rapidly in most tissuesDistribution: Widely and rapidly in most tissues
Crosses BBB with CSF levels of 40% to 50% of plasma Crosses BBB with CSF levels of 40% to 50% of plasma level level
Metabolism: Primarily hepatic; 86% to 96% of dose is Metabolism: Primarily hepatic; 86% to 96% of dose is metabolized to inactive metabolitemetabolized to inactive metabolite ITIT little conversion to inactive metabolite little conversion to inactive metabolite
Excretion: Renal (~80%; 90% as inactive metabolite) within 24 Excretion: Renal (~80%; 90% as inactive metabolite) within 24 hours hours
Half-lifeHalf-life IV: < 20 minutesIV: < 20 minutes2121
IT: 2-6 hours IT: 2-6 hours 20,2120,21

Cytarabine NeurotoxicityCytarabine Neurotoxicity13,21,2313,21,23
Route: Intrathecal, IV, liposomalRoute: Intrathecal, IV, liposomal23,1323,13
Cerebellar dysfunction (most common), generalized Cerebellar dysfunction (most common), generalized encephalopathy, peripheral neuropathy, and encephalopathy, peripheral neuropathy, and arachnoiditis, fecal and urinary incontinencearachnoiditis, fecal and urinary incontinence
Cytotoxic levels of cytarabine may be maintained for Cytotoxic levels of cytarabine may be maintained for up to 24 hours after IT administrationup to 24 hours after IT administration
IT liposomal (sustained release) may maintain IT liposomal (sustained release) may maintain cytotoxic concentrations of the drug in the CSF for up cytotoxic concentrations of the drug in the CSF for up to 14 daysto 14 days CSF exposure up to 40x that of standard Ara-CCSF exposure up to 40x that of standard Ara-C
Onset: As early as 2-5 days after treatmentOnset: As early as 2-5 days after treatment1313
May resolve spontaneously within a few days or May resolve spontaneously within a few days or may be permanentmay be permanent23,1323,13
Cytarabine NeurotoxicityCytarabine Neurotoxicity13,2313,23
Incidence: varies from 5-50%Incidence: varies from 5-50%13,2413,24
Risk factorsRisk factors13,2313,23
IV doses > 1 g/m2 IV doses > 1 g/m2 2323
Total IV dose > 30 g (Total IV dose > 30 g (>> 3g/ m2 every 12 hours) 3g/ m2 every 12 hours)33
IT dose (> 100 mg per week)IT dose (> 100 mg per week)2121
Age > 40 years of ageAge > 40 years of age1313
Prior cytarabine therapyPrior cytarabine therapy Renal dysfunctionRenal dysfunction IT, IT liposomal administrationIT, IT liposomal administration1313
Concomitant use with high-dose chemotherapy Concomitant use with high-dose chemotherapy (i.e. methotrexate)(i.e. methotrexate)13,2413,24
Cytarabine NeurotoxicityCytarabine Neurotoxicity25,2625,26
MOA of how it causes encephalopathy:MOA of how it causes encephalopathy:
-Cytotoxic effect-Cytotoxic effect2525
-Immune-mediated mechanism is hypothesized-Immune-mediated mechanism is hypothesized2626
Management:Management: Cytarabine should be discontinued immediatelyCytarabine should be discontinued immediately1313
No standard treatment is availableNo standard treatment is available Corticosteroids (methylprednisolone, Corticosteroids (methylprednisolone,
dexamethasone)dexamethasone)25,2625,26
PreventionPrevention Concurrent use of corticosteroid with IT liposomal Concurrent use of corticosteroid with IT liposomal
cytarabine reduces risk of arachnoiditiscytarabine reduces risk of arachnoiditis21,24,2521,24,25

RituximabRituximab2727
MOA: B cell lysis by binding of the Fab domain MOA: B cell lysis by binding of the Fab domain of rituximab to the CD20 antigen on B of rituximab to the CD20 antigen on B lymphocytes and by recruitment of immune lymphocytes and by recruitment of immune effector functions by the Fc domaineffector functions by the Fc domain Complement-dependent Complement-dependent
cytotoxicity (CDC)cytotoxicity (CDC) Antibody-dependent cellular Antibody-dependent cellular
cytotoxicity (ADCC)cytotoxicity (ADCC)

RituximabRituximab27,28,2927,28,29
Absorption: I.V.: Immediate and results in a rapid Absorption: I.V.: Immediate and results in a rapid and sustained depletion of circulating and and sustained depletion of circulating and tissue-based B cellstissue-based B cells
Metabolism: HepaticMetabolism: Hepatic Distribution: Lymph nodes Distribution: Lymph nodes Excretion: Uncertain; may undergo phagocytosis Excretion: Uncertain; may undergo phagocytosis
and catabolism in the reticuloendothelial system and catabolism in the reticuloendothelial system (RES)(RES)
Median terminal half-life for NHL: 22 days Median terminal half-life for NHL: 22 days (range: 6-52 days)(range: 6-52 days)
Rituximab NeurotoxicityRituximab Neurotoxicity3030
Progressive Multifocal Leukoencephalopathy Progressive Multifocal Leukoencephalopathy (PML)(PML)
Incidence: RareIncidence: Rare 2 PML cases per 8000 rituximab treated SLE 2 PML cases per 8000 rituximab treated SLE
patientspatients Need to conduct more epidemiological studiesNeed to conduct more epidemiological studies
Risk factors:Risk factors: Need more studiesNeed more studies Possibly low CD4 counts and low IgG levelsPossibly low CD4 counts and low IgG levels

Rituximab NeurotoxicityRituximab Neurotoxicity27,3027,30
Clinical presentationClinical presentation Confusion/disorientationConfusion/disorientation Motor weakness/hemiparesisMotor weakness/hemiparesis Altered vision/speechAltered vision/speech Poor motor coordination Poor motor coordination Symptoms progress over weeks to monthsSymptoms progress over weeks to months
MOA of how it causes encephalopathyMOA of how it causes encephalopathy1,21,2
Unclear, but rituximab can decrease the immune Unclear, but rituximab can decrease the immune system and cause reactivation of the Jakob-system and cause reactivation of the Jakob-Creuzfeld (JC) virusCreuzfeld (JC) virus
Rituximab NeurotoxicityRituximab Neurotoxicity3030
A retrospective analysis of patients diagnosed with PML A retrospective analysis of patients diagnosed with PML after rituximab treatmentafter rituximab treatment Cases from cancer centers or academic hospitals (22), Cases from cancer centers or academic hospitals (22),
FDA reports (11), manufacturers database (30), FDA reports (11), manufacturers database (30), publications (18)publications (18)
Inclusion: rituximab therapy prior to PML, PML Inclusion: rituximab therapy prior to PML, PML confirmation with brain histology or MRI, no HIV infectionconfirmation with brain histology or MRI, no HIV infection
Patient Population (n=57)Patient Population (n=57) B-cell lymphoproliferative disorder (52)B-cell lymphoproliferative disorder (52) Systemic Lupus Erythmetous (2)Systemic Lupus Erythmetous (2) Autoimmune pancytopenia (2)Autoimmune pancytopenia (2) Immune thrombocytopenia purpura (1)Immune thrombocytopenia purpura (1)
Rituximab NeurotoxicityRituximab Neurotoxicity3030
Onset:Onset: Median of 16 months (following rituximab Median of 16 months (following rituximab
initiation)initiation) 5.5 months (following last rituximab dose)5.5 months (following last rituximab dose) 6 rituximab doses preceded PML diagnosis6 rituximab doses preceded PML diagnosis
In the absence of immune reconstitution, case In the absence of immune reconstitution, case fatality rate was 90%fatality rate was 90% Survival rates up to 38% after hematopoietic Survival rates up to 38% after hematopoietic
stem cell transplantationstem cell transplantation

Rituximab NeurotoxicityRituximab Neurotoxicity27,3027,30
Promptly evaluate any patient presenting with Promptly evaluate any patient presenting with neurological changesneurological changes
Consider neurology consultation, brain MRI Consider neurology consultation, brain MRI and lumbar puncture for suspected PMand lumbar puncture for suspected PM LL
Discontinue rituximab in patients who Discontinue rituximab in patients who develop PMLdevelop PML
Consider reduction/discontinuation of Consider reduction/discontinuation of concurrent chemotherapy or concurrent chemotherapy or immunosuppressantsimmunosuppressants
Risks versus benefitsRisks versus benefits
Back to N.B.Back to N.B.
Clinical HistoryClinical History 6/16: confusion is clinically improving6/16: confusion is clinically improving 6/17: mental status seems to be slowly 6/17: mental status seems to be slowly
improvingimproving 6/20: confusion clinically stable6/20: confusion clinically stable
Acute altered mental status attributed to Acute altered mental status attributed to tacrolimus CNS toxicitytacrolimus CNS toxicity

Future DirectionsFuture Directions
Need of biological markers or markers for Need of biological markers or markers for quantification of medication-induced quantification of medication-induced neurotoxicityneurotoxicity AdenosineAdenosine Choline (higher levels correlated with Choline (higher levels correlated with
demyelination)demyelination) PatternsPatterns
MRI, CT, EEGMRI, CT, EEG
ReferencesReferences1. Author unknown. NINDS Encephalopathy Information Page. National Institute of 1. Author unknown. NINDS Encephalopathy Information Page. National Institute of
Neurological Disorders and Stroke. http://www.ninds.nih.gov/disorders/encephalopathy/ Neurological Disorders and Stroke. http://www.ninds.nih.gov/disorders/encephalopathy/ encephalopathy.htm Last updated: 0212/2007. Date accessed: 06/17/2010encephalopathy.htm Last updated: 0212/2007. Date accessed: 06/17/2010
2. Nishiguchi T, Mochizuki K, Shakudo M, et al. CNS complications of Hematopoietic Stem 2. Nishiguchi T, Mochizuki K, Shakudo M, et al. CNS complications of Hematopoietic Stem Cell Transplantation. AJR 2009; 192: 1002-1011Cell Transplantation. AJR 2009; 192: 1002-1011
3. Prograf® (tacrolimus) injection package insert. Astellas Pharma.Deerfield, IL. Last 3. Prograf® (tacrolimus) injection package insert. Astellas Pharma.Deerfield, IL. Last Revised: August 2009Revised: August 2009
5. Hinchey J, Chaves C, Appignani B, et al. A Reversible Posterior Leukoencephalopathy 5. Hinchey J, Chaves C, Appignani B, et al. A Reversible Posterior Leukoencephalopathy Syndrome. NJEM (1996) 334:494-500. Syndrome. NJEM (1996) 334:494-500.
6.Oliverio P, Restrepo L, Mitchell S, et al. Reversible Tacrolimus-induced Neurotoxicity 6.Oliverio P, Restrepo L, Mitchell S, et al. Reversible Tacrolimus-induced Neurotoxicity Isolated to the Brain Stem. Am J Neuroradiol (2000) 21: 1252-1254Isolated to the Brain Stem. Am J Neuroradiol (2000) 21: 1252-1254
7. Grimbert P., Azema C., Pastural M., et al. Tacrolimus (FK506)-induced severe and late 7. Grimbert P., Azema C., Pastural M., et al. Tacrolimus (FK506)-induced severe and late encephalopathy in a renal transplant recipient. Nephrol Dial Transplant (1999) 14: 2489-encephalopathy in a renal transplant recipient. Nephrol Dial Transplant (1999) 14: 2489-2491.2491.
8. Chegounchi M, Hanna M, Neild G. 8. Chegounchi M, Hanna M, Neild G. Progressive neurological disease induced by Progressive neurological disease induced by tacrolimus in a renal transplant recipient: Case presentation. BMC Nephrology 2006 Vol tacrolimus in a renal transplant recipient: Case presentation. BMC Nephrology 2006 Vol 7:1-37:1-3
9. Methotrexate for injection, USP package insert. Bedford Laboratories. Bedford, OH. Last 9. Methotrexate for injection, USP package insert. Bedford Laboratories. Bedford, OH. Last Revised: April 2005. Revised: April 2005.
ReferencesReferences10. LaCasce A. 10. LaCasce A. Therapeutic use of high-dose methotrexate. UpToDate. http://uptodate.com.proxy. Therapeutic use of high-dose methotrexate. UpToDate. http://uptodate.com.proxy.
westernu.edu/online/content/ topic.do?topicKey=chemge. Last updated: 02/23/2009 Date westernu.edu/online/content/ topic.do?topicKey=chemge. Last updated: 02/23/2009 Date Accessed: 06/16/2010Accessed: 06/16/2010
11. Lexi-Comp online, Lexi-Drugs Online. Hudson, Ohio Lexi-Comp, Inc. Methotrexate. Last updated 11. Lexi-Comp online, Lexi-Drugs Online. Hudson, Ohio Lexi-Comp, Inc. Methotrexate. Last updated 6/18/10. Accessed 6/18/10.6/18/10. Accessed 6/18/10.
12. Vazmar S, Schusseler P, Becker A, et al. Methotrexate-Associated Alterations of the Folate and 12. Vazmar S, Schusseler P, Becker A, et al. Methotrexate-Associated Alterations of the Folate and Methyl-transfer Pathway in the CSF of ALL Patients with and without Symptoms of Neurotoxicity. Methyl-transfer Pathway in the CSF of ALL Patients with and without Symptoms of Neurotoxicity. Pediatr Blood Cancer (2009) 52:26-32Pediatr Blood Cancer (2009) 52:26-32
13. Wen P, Plotkin S. Neurologic complications on non-platinum cancer chemotherapy. UpToDate. 13. Wen P, Plotkin S. Neurologic complications on non-platinum cancer chemotherapy. UpToDate. http://www.uptodate.com.proxy.westernu.edu http://www.uptodate.com.proxy.westernu.edu /online/contecnt/topic.do? topicKey=genl_onc/online/contecnt/topic.do? topicKey=genl_onc Last Last updated: 12/27/2009. Date accessed: 06/17/2010.updated: 12/27/2009. Date accessed: 06/17/2010.
14. Brugnoletti F, Morris EB, Laningham FH, et al. 14. Brugnoletti F, Morris EB, Laningham FH, et al. Recurrent Intrathecal Methotrexate Induced Recurrent Intrathecal Methotrexate Induced Neurotoxicity in an Adolescent with Acute Lymphoblastic Leukemia: Serial Clinical and Radiologic Neurotoxicity in an Adolescent with Acute Lymphoblastic Leukemia: Serial Clinical and Radiologic Findings. Pediatric Blood Cancer p.293-29515. Findings. Pediatric Blood Cancer p.293-29515.
15. Shuper A, Stark B, Kornreich L, et al. Methotrexate-related Neurotoxicity in the Treatment of 15. Shuper A, Stark B, Kornreich L, et al. Methotrexate-related Neurotoxicity in the Treatment of Childhood Acute Lymphoblastic Leukemia. IMAJ (2002) Vol 4 p1050-1051Childhood Acute Lymphoblastic Leukemia. IMAJ (2002) Vol 4 p1050-1051
16. 16. Hamidah A, Lope R, Latiff Z, et al. Hamidah A, Lope R, Latiff Z, et al. Prevention of Neurotoxicity by High-dose Folinic Acid Rescue Prevention of Neurotoxicity by High-dose Folinic Acid Rescue after High-dose methotrexate and Intrathecal methotrexate without Compromising Cure inspite of after High-dose methotrexate and Intrathecal methotrexate without Compromising Cure inspite of Previous Transient Leukoencephalopathy after Intrathecal Methotrexate. Annals Academy of Previous Transient Leukoencephalopathy after Intrathecal Methotrexate. Annals Academy of Medicine. p743-744Medicine. p743-744

ReferencesReferences17. Dicuonzo F, Salvati A, Palma M, et al. 17. Dicuonzo F, Salvati A, Palma M, et al. Posterior Reversible Encephalopathy Posterior Reversible Encephalopathy
Syndrome Associate with Methotrexate Neurotoxicity: Conventional Magnetic Syndrome Associate with Methotrexate Neurotoxicity: Conventional Magnetic Resonance and Diffusion-Weighted Imaging Findings. J Child Neurol (2009) Resonance and Diffusion-Weighted Imaging Findings. J Child Neurol (2009) 24;8:1013-101824;8:1013-1018
18. Inaba H, Khan RB, Laningham FH, et al. 18. Inaba H, Khan RB, Laningham FH, et al. Clinical and Radiological Characteristics of Clinical and Radiological Characteristics of Methotrexate-induced Acute Encephalopathy in Pediatric Patients with Cancer. Methotrexate-induced Acute Encephalopathy in Pediatric Patients with Cancer. Annals of Oncology (2008) 19: 178-184Annals of Oncology (2008) 19: 178-184
19. Finkelstein Y, Zevin S, Raikhlin-Eisenkraft B, Bentur Y. 19. Finkelstein Y, Zevin S, Raikhlin-Eisenkraft B, Bentur Y. Intrathecal methotrexate Intrathecal methotrexate neurotoxicity: clinical correlated and antidotal treatment. Environmental Toxicology neurotoxicity: clinical correlated and antidotal treatment. Environmental Toxicology and Pharmacology (2005) 19:721-725and Pharmacology (2005) 19:721-725
20. Cytarabine for injection, USP package insert. Bedford Laboratories. Bedford, OH. 20. Cytarabine for injection, USP package insert. Bedford Laboratories. Bedford, OH. Last Revised: September 2008Last Revised: September 2008
21. Kwong YL, Yeung D, Chan J. Intrathecal Chemotherapy for Hematologic 21. Kwong YL, Yeung D, Chan J. Intrathecal Chemotherapy for Hematologic Malignancies: Drugs and Toxicities. Ann Hematol (2009) 88: 193-201Malignancies: Drugs and Toxicities. Ann Hematol (2009) 88: 193-201
22. Lexi-Comp online, Lexi-Drugs Online. Hudson, Ohio Lexi-Comp, Inc. Cytarabine. Last 22. Lexi-Comp online, Lexi-Drugs Online. Hudson, Ohio Lexi-Comp, Inc. Cytarabine. Last updated 4/7/2010. Accessed 6/17/10. updated 4/7/2010. Accessed 6/17/10.
23. Nielsen E, Brant J. Chemotherapy-Induced Neurotoxicity. AJN Supplement (2002) 23. Nielsen E, Brant J. Chemotherapy-Induced Neurotoxicity. AJN Supplement (2002) 16-1916-19
ReferencesReferences24. Jabbour E, O’Brien S, Kantarjian H, et al. 24. Jabbour E, O’Brien S, Kantarjian H, et al. Neurologic complications associated with Neurologic complications associated with
intrathecal cytarabine given prophylatically in combination with high-dose methotrexate and intrathecal cytarabine given prophylatically in combination with high-dose methotrexate and cytarabine with acute lymphocytic leukemia. Blood (2007) Vol 109, No 8, pp 3214-3218cytarabine with acute lymphocytic leukemia. Blood (2007) Vol 109, No 8, pp 3214-3218
25. Hilgendorf I, Wolff D, Junghass C, et al. Neurological complications after Intrathecal 25. Hilgendorf I, Wolff D, Junghass C, et al. Neurological complications after Intrathecal liposomal cytarabine application in patients after allogeneic hematopoietic stem cell liposomal cytarabine application in patients after allogeneic hematopoietic stem cell transplantation. Ann Hematol (2008) 87:1009-1012transplantation. Ann Hematol (2008) 87:1009-1012
26. Malhotra P, Mahi S, Lal V, et 26. Malhotra P, Mahi S, Lal V, et al. Cytarabine-Induced Neurotoxicity Resal. Cytarabine-Induced Neurotoxicity Responding to ponding to Methylprednisolone. American Journal of Hematology 77: 416Methylprednisolone. American Journal of Hematology 77: 416
27. Rituxan® (rituximab) for injection package insert. Genentech, Inc. South San Francisco, CA. 27. Rituxan® (rituximab) for injection package insert. Genentech, Inc. South San Francisco, CA. Las Revised: 02/2010Las Revised: 02/2010
28. Lexi-Comp online, Lexi-Drugs Online. Hudson, Ohio Lexi-Comp, Inc. Rituximab. Last updated 28. Lexi-Comp online, Lexi-Drugs Online. Hudson, Ohio Lexi-Comp, Inc. Rituximab. Last updated 6/18/10. Accessed 6/18/10.6/18/10. Accessed 6/18/10.
29. Cartron G, Blasco H, Paintaud G, Watier H, Le Guellec C. Pharmacokinetics of rituximab and 29. Cartron G, Blasco H, Paintaud G, Watier H, Le Guellec C. Pharmacokinetics of rituximab and its clinical use: thought for the best use? Crit Rev Oncol Hematol 62(1):43-52 (2007 Apr).its clinical use: thought for the best use? Crit Rev Oncol Hematol 62(1):43-52 (2007 Apr).
30. Carson K, Evens AM, Richey EA. Progressive multifocal leukoencephalopathy after rituximab 30. Carson K, Evens AM, Richey EA. Progressive multifocal leukoencephalopathy after rituximab therapy in HIV-negative patients: a report of 57 cases from the Research on Adverse Drug therapy in HIV-negative patients: a report of 57 cases from the Research on Adverse Drug Events and Reports project. Events and Reports project. BLOOD 05/14/2009. Vol 113, No 20. pp4833-4840. BLOOD 05/14/2009. Vol 113, No 20. pp4833-4840.
QuestionsQuestions







