
District of Columbia Chapter Scientific Meeting – 2015
November 6 – 7, 2015
Therapy of Hypothyroidism:
New and Old Concepts
Leonard Wartofsky, M.D.
MedStar Washington Hospital Center
Georgetown University School of Medicine
Washington, DC

SUBCLINICAL THYROID DISEASE Case
• 51 y.o. WF with
high cholesterol; (-)
Hx; FHx: M --?
AITD
Bro: DM/gray
ROS:
menopause@44,
mild hypertension ;
? fatigue.
• Tchol = 245 mg%,
HDL 61, LDL 171,
hematocrit 35%,
P.E. : BP 145/93.
No palpable goiter
SUBCLINICAL THYROID DISEASE Case : Thyroid Function Tests
• Total T4 = 6.1 mcg/dl (NL 5-12)
• Free T4 = 0.99 ng/dl (NL 0.80-1.90)
• TSH = 4.978 mU/L (NL 0.4-5.5)

“SUBCLINICAL” THYROID DISEASE EARLY THYROID FAILURE
Objectives - 1
• What are the criteria for Dx ?
• What population is at risk ?
• How frequent is this entity in the population?
• If TSH is our most sensitive index of thyroid
function, how can there be thyroid failure if the
TSH is “normal” ?
“SUBCLINICAL” THYROID DISEASE EARLY THYROID FAILURE
Objectives -2
• What are the associated abnormalities?
• Should patients be followed or treated?
• What are the benefits of Rx ?

“SUBCLINICAL” HYPOTHYROIDISM
What is it ?

SUBCLINICAL HYPOTHYROIDISM DEFINITION
• Normal:
— TT4
— TT3
— FT4
— FT3
— RT3U
• TSH = 3 - 15 mIU/L
SUBCLINICAL HYPOTHYROIDISM
PATIENTS AT RISK
• Aging: Women > age 45
Men > age 60
• Hx of Rx for Graves’ disease
• Hypercholesterolemia
• +Family Hx of thyroid disease
• Infertility; menstrual irregularities
• Pregnancy; Post-partum period
Redefining the Normal Range
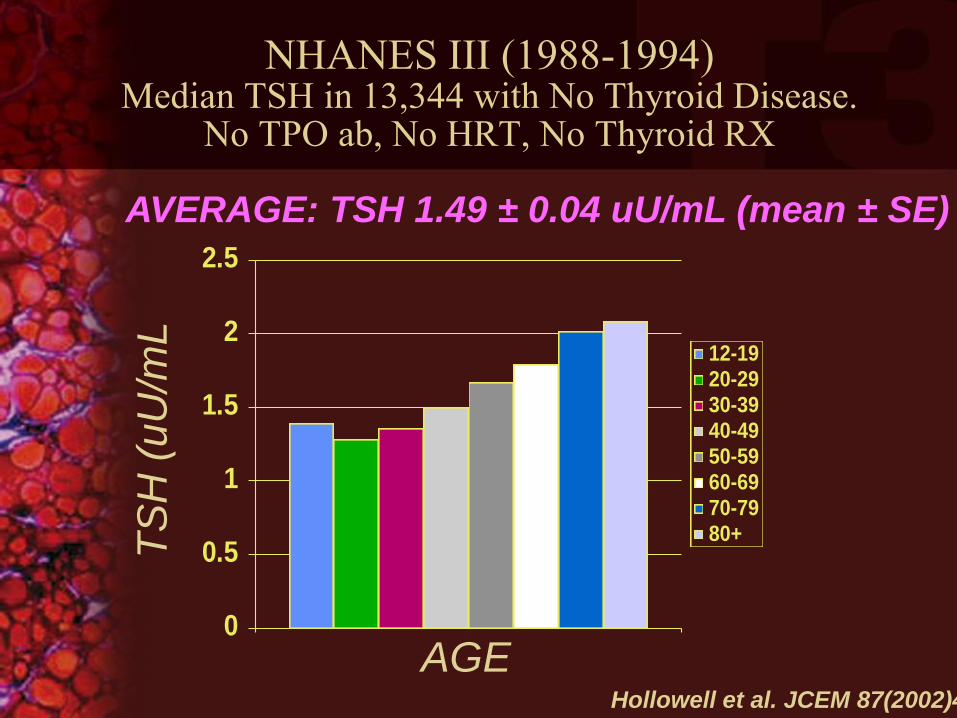
NHANES III (1988-1994) Median TSH in 13,344 with No Thyroid Disease.
No TPO ab, No HRT, No Thyroid RX T
SH
(u
U/m
L
AVERAGE: TSH 1.49 ± 0.04 uU/mL (mean ± SE)
0
0.5
1
1.5
2
2.5
12-1920-2930-3940-4950-5960-6970-7980+
AGE Hollowell et al. JCEM 87(2002)489

Individual TSH Normal Range
Participants
Mean +/- 2 SD = 1.27 (0.16 - 2.39)
Anderson S, et al. J Clin Endocrinol Metab. 2002;87:1068-1072.

Population normal TSH range may not equal
individual normal range
Person A
Normal Range
TSH = 0.9-1.5
TSH Normal Range
Person B
Normal Range
TSH = 1.2-3.0
Population vs Individual Variations in Serum TSH

Prevalence of Elevated Serum TSH by Decade of Age and Gender (n=798)
Hollowell JG, et al. J Clin Endocrinol Metab. 2002;87:489-499.
NHANES III Study (n=17,353)
% P
artic
ipan
ts w
ith E
leva
ted
TS
H
0
5
10
15
20
13-19 20-29 30-39 40-49 50-59 6-69 70-79 >80
24
Males
3.0 2.0 2.5
4.1
2.0 3.0
11.0 10.8
Females
2.0 2.2 3.0
6.5
8.5
10.5
13.8
15.8

NHANES III: Prevalence of Positive Anti-TPO Antibodies
0
5
10
15
20
25
30
35
13-19 20-29 30-39 40-49 50-59 60-69 70-79 >80
Male
Female
Pe
rce
nt
Age
Hollowell JG, et al. J Clin Endocrinol Metab. 2002;87:489-499.

• Euthyroid Outliers - inherent TSH lability
• Measurement of bioinactive isoforms
• Occult thyroid dysfunction
TSH Population Reference Ranges
Reasons for the skew of the TSH
upper limit include:
~4.0 ~0.45 1-1.5 ~2.5 ~0.45 1-1.5 ~2.5 ~4.0
95% Limits
10
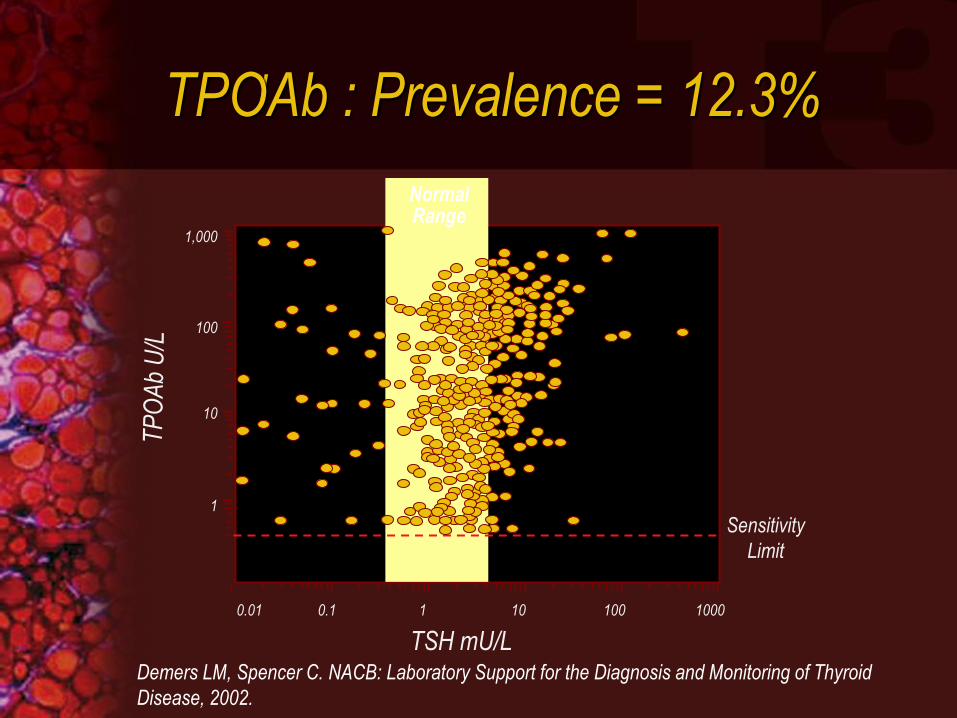
1,000
100
10
1
TSH mU/L
Sensitivity
Limit
0.01 0.1 1 10 100 1000
Normal Range
Demers LM, Spencer C. NACB: Laboratory Support for the Diagnosis and Monitoring of Thyroid
Disease, 2002.
ı TPOAb : Prevalence = 12.3%
“SUBCLINICAL” HYPOTHYROIDISM
What is the natural
history with follow-up ?

SUBCLINICAL HYPOTHYROIDISM
PROGRESSION TO OVERT DISEASE (Rosenthal et al., JAMA 1987;258:209)
• 258 healthy elderly followed x 4 yrs
• 13.2% had subclinical
hypothyroidism based on normal T4
and elevated TSH
• 4 yrs later:
• 33% overtly hypothyroid
• 80% of those with (+) Ab’s
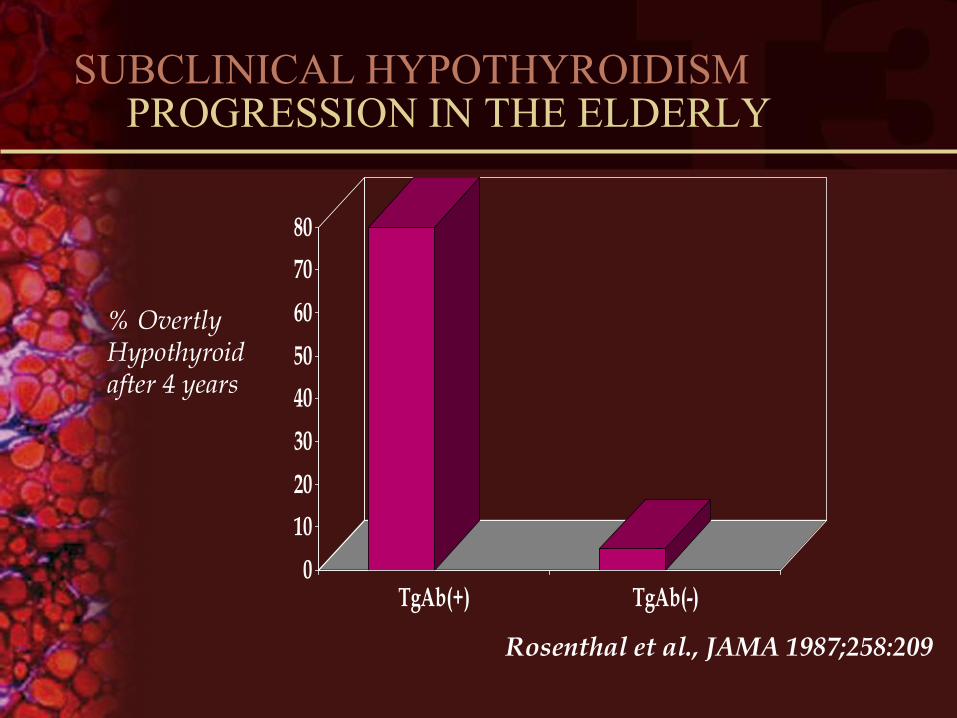
SUBCLINICAL HYPOTHYROIDISM PROGRESSION IN THE ELDERLY
0
10
20
30
40
50
60
70
80
TgAb(+) TgAb(-)
Rosenthal et al., JAMA 1987;258:209
% Overtly Hypothyroid after 4 years
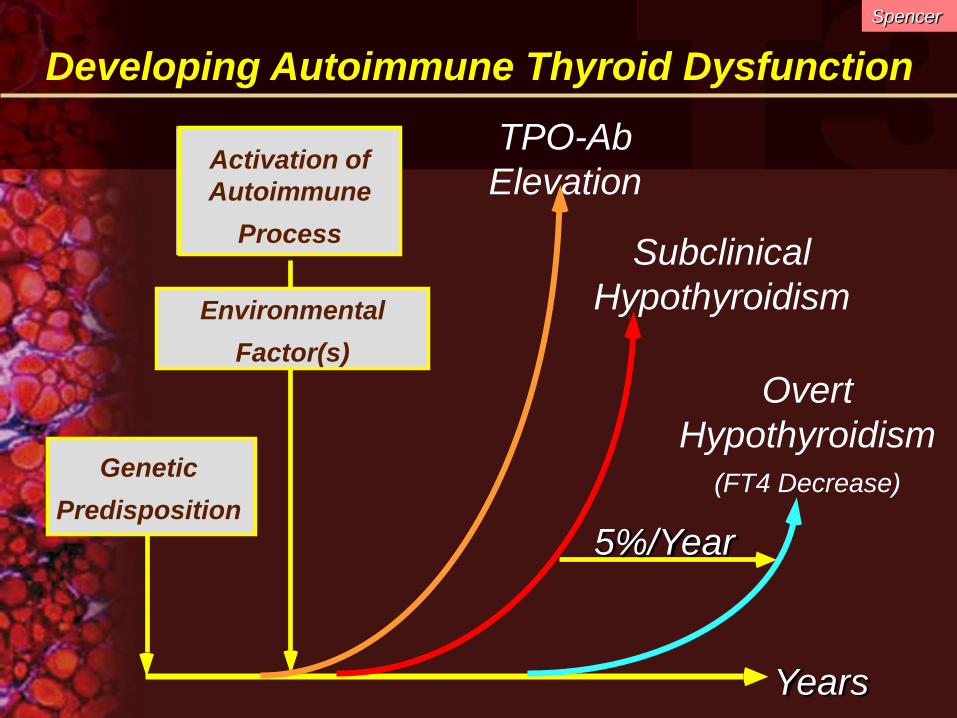
Developing Autoimmune Thyroid Dysfunction
TPO-Ab
Elevation
Subclinical
Hypothyroidism
Overt
Hypothyroidism
(FT4 Decrease)
Years
5%/Year
Activation of
Autoimmune
Process
Environmental
Factor(s)
Genetic
Predisposition
Spencer

Progression of Mild Thyroid Failure
Years
NORMAL RANGE
Overt Hypothyroidism
Mild Thyroid Failure Euthyroid
T3 T4
Adapted from Ayala AR, Wartofsky L. The Endocrinologist. 1997;7:44.
TSH

MILD THYROID FAILURE REPORTED ABNORMALITIES
• Symptoms
• Cognition; memory; psychometrics
• Neurologic function
• Muscle function; CPK
• TChol, LDL, apo(a), apo(b), TG
• PVR/systolic function; Diastolic function
• STI’s;Atherogenesis; plaque progression
• Pregnancy outcomes

Lipid Profiles in Mild Thyroid Failure

Canaris GJ, et al. Arch Intern Med. 2000;160:526-534.
Even mild Hypothyroidism is associated with increased
total Chol and LDL-Chol, both markers of CV disease
Cholesterol LDL-C HDL-C
Colorado Thyroid Disease Prevalence Study (N=25,862)
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
%

The Heart in Mild Thyroid Failure

MILD THYROID FAILURE AND RISK OF ISCHEMIC HEART DISEASE
(Imaizumi et al. JCEM 2004; 89:3365-70)
• 257 pts with TSH > 5 and NL FT4
240/257 had TSH = 5 - 10
vs. 2293 controls (TSH 0.6-5.0)
• X-sectional analysis; MTF associated with
ischemic HD (OR 2.7) independent of age,
BP, BMI, TChol, smoking, or DM
• 10 yr F/U: Increased all cause mortality
(HR 1.9-2.1) for men

MILD THYROID FAILURE AND
RISK OF ISCHEMIC
HEART DISEASE
• Risk of Ischemic
Heart disease (O.R.)
– Overall = 2.7
– Women = 1.7
– Men = 4.5
(Imaizumi et al. JCEM 2004; 89:3365-70)

Mild Thyroid Failure as a Risk Factor for Myocardial Infarction
• The Rotterdam Study
– Population study of 7983 Subjects
– Baseline Study: 1990-1993
– 1149 Women Evaluated for:
• Lipids and BMI
• TSH (Free T4 if TSH abnormal)
• Aortic Calcifications
• EKG and History of MI
– Followed-up Chart Review in 1996
Hak, et al. Ann Int Med. 2000;132:270-278

Association of MTF with risk of MI & atherosclerosis
Subclinical hypothyroid*
2.3
1.7
Od
ds
Ra
tio‡
0
0.5
1
1.5
2
2.5
3
3.5
Myocardial Infarction
Subclinical hypothyroid*
and antibodies†
3.1
1.9
Euthyroid
1.0 1.0
Aortic Atherosclerosis
* Normal T4 & TSH > 4.0 mU/L; †To thyroid peroxidase; ‡Adjusted for patient age.
Hak AE, et al. Ann Intern Med. 2000;132:270-278.
Rotterdam Study (N=1149 elderly women)

Age-adjusted RR for M.I. attributed to MTF compared to other classic
CV risk factors.
Rotterdam Study (N=1149 elderly women)
2.4
Rela
tive R
isk
0
0.5
1
1.5
2
2.5
3
3.5
Subclinical
Hypothyroidism
2.0*
2.4
1.6
2.5
1.2†
Hypercholes
-terolemia
Hyper-
tension
Smoking
(Current)
Smoking
(Past)
Diabetes
Mellitus
*Current compared with never smoked; †Past compared with never smoked.
Hak AE, et al. Ann Intern Med. 2000;132:270-278.
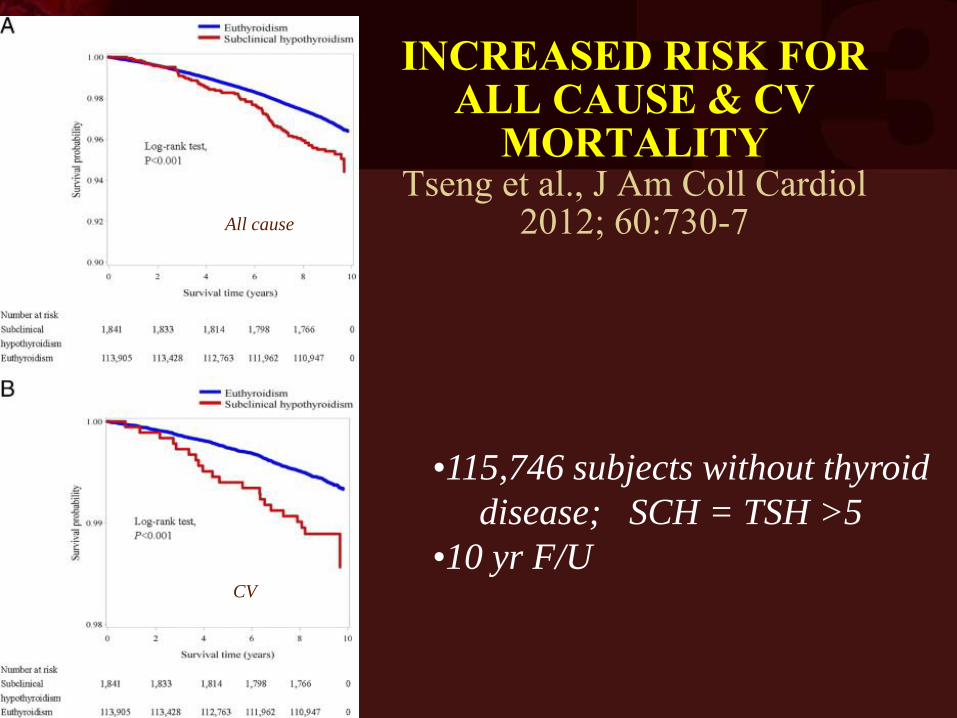
INCREASED RISK FOR ALL CAUSE & CV
MORTALITY Tseng et al., J Am Coll Cardiol
2012; 60:730-7
•115,746 subjects without thyroid
disease; SCH = TSH >5
•10 yr F/U
All cause
CV
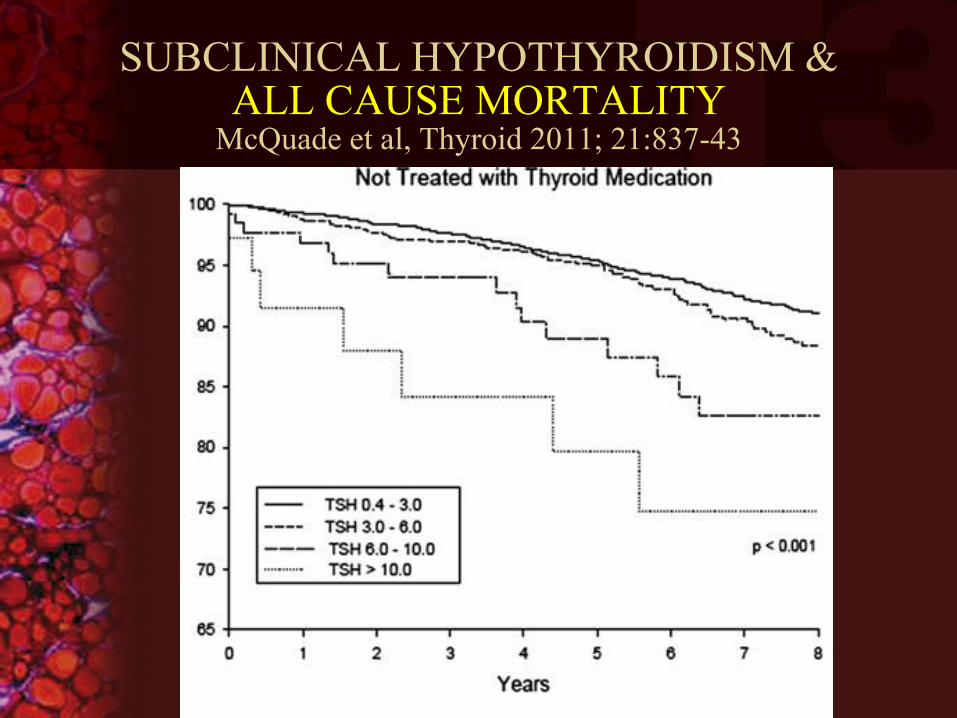
SUBCLINICAL HYPOTHYROIDISM & ALL CAUSE MORTALITY
McQuade et al, Thyroid 2011; 21:837-43

Amer J Med 2006; 119:541-51
Overall O.R. = 1.81-2.38 Subgroup Analysis: O.R. = 1.42-1.72
SUBCLINICAL HYPOTHYROIDISM
BENEFICIAL EFFECT OF L-T4 Rx ON CV RISK FACTORS & QOL (Razvi et al JCEM 2007; 92:1715)
• 100 pts in a RCT, double blind, crossover of 100 mcg LT-4 vs. placebo
• Measured TC, LDL, endothelial function, & pt. reported outcomes
• Significant improvement seen in TC, LDL-C, waist/hip ratio, flow-mediated dilatation, complaints of fatigue
• Sustained changes would yield a 10% reduction in 10 yr CV mortality

Stratified Analysis of Effect of Subclinical Hypothyroidism
on Risk of CHD
Ochs N et al, Ann Intern Med 2008;148:832-45
– <65 years RR 1.51 (1.09-2.09)
– ≥65 years RR 1.05 (0.90-1.22)
Razvi S et al, JCE&M 2008;93:2998-3007
– <65 years RR 1.68 (1.27-2.23)
– ≥65 years RR 1.02 (0.85-1.22)

SUBCLINICAL HYPOTHYROIDISM, AGE, & ISCHEMIC HEART DISEASE
Mariotti S., JCEM 2008; 93:2969-
71

MILD THYROID FAILURE REPORTED BENEFITS OF L-T4 THERAPY
• Prevent progression to overt disease
• Relieve symptoms
• Cognition; memory; psychometrics
• Neurologic function
• Muscle function; CPK
• TChol, LDL, apo(a), apo(b), TG
• PVR/systolic function; Diastolic function
• STI’s;Atherogenesis; plaque progression
• Pregnancy outcomes
SO, THE TSH IS >3 mU/L START L-T4 OR WHAT ?
• Repeat TSH in 6-8 weeks
• Measure anti-TPO antibodies
• Rx’tic trial if symptomatic or TSH => 10
• Or, first determine if Hx supports the Dx:
• ? Goiter, diastolic dysfunction, dyslipidemia
• ? Pregnancy, infertility
• ? (+) Family Hx
• ? Lithium Rx, Amiodarone, etc.
• and then treat.
T4/T3 Combination Therapy
Case Discussion • 41-year-old woman with Grave’s disease
undergoes RAI ablative therapy rendering her hypothyroid
• She is seen in follow-up 2 years later with the following thyroid function test results on levothyroxine therapy:
– TT4 10.2 (NL 5 – 12) – TT3 98 (NL 80 – 180) – TSH 0.988 (NL 0.3 – 3.5)

Case Discussion (cont.)
• Complains of fatigue, weakness and lethargy she claims have been a problem only since the RAI therapy
• Recently visited internet web sites and wants to know why you are not treating her with T3

T4/T3 COMBINATION THERAPY QUESTIONS
• Can hypothyroid patients be optimally replaced by thyroxine therapy alone?
• Are there convincing data that combined T4/T3 results in: – more physiologic tissue T4/T3 and serum TSH levels?
– improved clinical status?
• Are there new data that may provide a rationale for T4/T3 therapy?
ARGUMENTS FOR T3
SUPPLEMENTATION
1. The thyroid produces both T3 and T4
2. L-T4 therapy has no T3
3. Patients on T4 alone have higher than NL T4/T3 ratios
4. Peripheral conversion of T4 to T3 is inadequate
5. Tissues have deficient T3 levels
6. T4 monotherapy = “Tissue hypothyroidism”
Studies in rodents indicated that combined T4/T3 therapy simultaneously normalizes plasma and all tissue T4 and T3 concentrations.
T4/T3 COMBINATION THERAPY
Tissue T4 and T3 Content
Escobar-Morreale et al. J Clin Invest. 1995;96:2828.

T4/T3/rT3
T4
T3 rT3
T4 T3 rT3
30 ug/d
100 ug/d
30 ug/d
15%
85%
SOURCES OF T4 AND T3
T4/T3 = 10/1-14/1
Type 1 5’
Deiodinase

T4/T3 COMBINATION THERAPY THE “PERFECT” PILL
For the 1.78 m2 patient:
• T4 content = 112 µg
• Bioavailable T4 = 100 µg
• T3 Content = 5 µg (delayed release)
• Bioavailable T3 = 5 µg +25 µg(from T4)

T3 + T4 COMBINATION THERAPY
CONCERNS WITH PRIOR STUDIES
• Focus on QOL and psychological endpoints
• Limited data on thyroid hormone action
• Usually fixed dose/d of T3; variable T4/T3 ratio
• Studies not targeted to TSH level
• Lack of statistical power to account for genetic
polymorphisms
• Small sample size; lack of homogeneity of
patient population
• Brief duration of study period
T4/T3 Combination Therapy
The ‘Ultimate Solution’?
1. T4/T3 Tablets with correct 14:1 molar ratio 2. True slow or constant release formulation x 24 hrs 3. RCT’s showing optimal TSH levels and clinical benefit 4. Greater understanding of genetic influences on thyroid function 5. Maintenance of normal FT3/FT4 ratio

T4 Rx ALONE DOES NOT GUARANTEE EUTHYROIDISM
Gullo et al., PLoS one 6 (8):e22552; August 2011
• Measured FT4, FT3 in 1811 athyreotic pts on
LT4 with NL TSH vs. 3875 euthyroid controls
• Patients had higher FT4/lower FT3 (p = <0.001)
• Found ~ 20% of patients do not maintain FT4
and FT3 in reference range in spite of NL TSH
• Reflects inadequate peripheral T4 → T3
deiodination to compensate for missing T3
secretion
• ? Longterm effects /clinical consequences

Athyreotic patients on LT4
with normal
TSH
Gullo et al., PLoS one 6 (8):e22552; August 2011
% with higher than
Normal range FT4
% with lower
than normal
range FT3
% with lower than normal
range FT3/FT4 ratio
[2.5% of euthyroid controls]
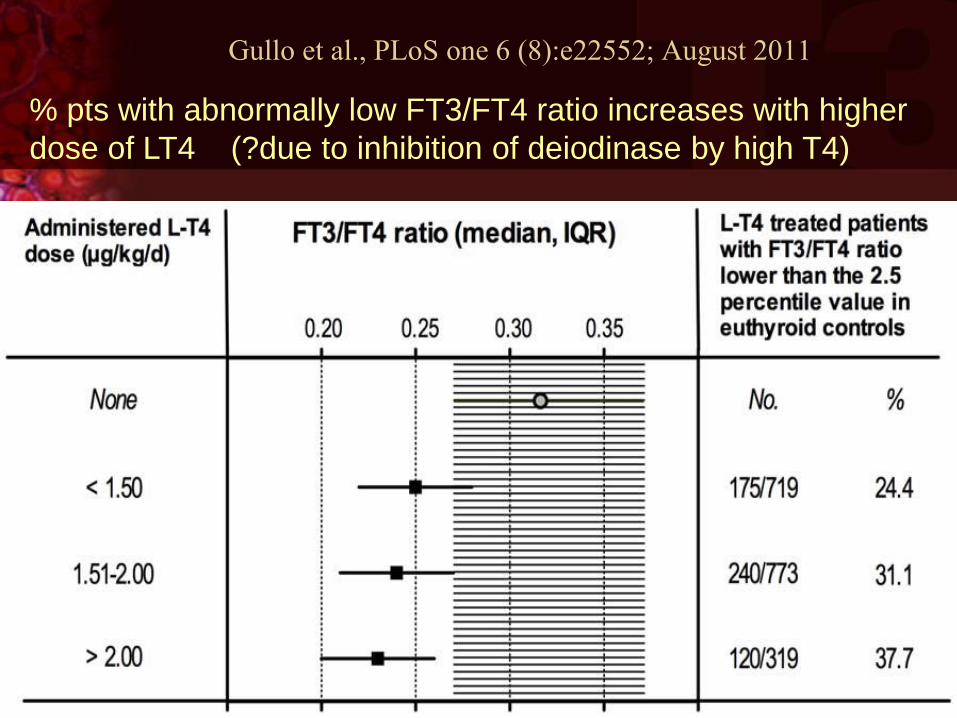
Gullo et al., PLoS one 6 (8):e22552; August 2011
% pts with abnormally low FT3/FT4 ratio increases with higher
dose of LT4 (?due to inhibition of deiodinase by high T4)
• Could variants in DIO2 gene influence well
being on T4 Rx irrespective of TSH levels?
• Analyzed common variants of 3 DIO2 genes
vs. response to T4/T3 in 552 subjects on T4
• CC genotype
• Present in 16% of population
• Had worse baseline GHQ scores on LT4
• Improved scores on T4/T3
• No change in T4, T3, TSH levels
DIO2 POLYMORPHISM AND RESPONSE TO T4/T3 Rx Panicker et al., JCEM 94:1623-29, 2009.

• With CC variant in only 16% of population,
prior studies may have been underpowered
to detect difference
• May explain why some patients on T4 do not
feel ‘back to normal’
• ? Influence of DIO2 activity in the brain and
psychological well being
• Perhaps variations in other candidate genes,
e.g., thyroid hormone transporters, might
also influence well being
DIO2 POLYMORPHISM AND RESPONSE TO T4/T3 Rx Panicker et al., JCEM 94:1623-29, 2009.

GENETIC INFLUENCES ON TSH Panicker et al., Am J Hum Gen 87:430-5, 2010
• Genome wide association study of 2.1
million single nucleotide polymorphisms
(SNP’s) in 2014 female twins
• Found significant association between TSH
and rs10917469 that was replicated in a
community based sample of 1154 people
• 29% carry the variant with TSH difference
between wild type and variant = 0.5 mIU/L
• Likely to be clinically relevant

WHICH IS BETTER - T4 or T3? Celi et al., JCEM 2011; 96:3466-74
• 14 hypothyroid pts Rx’d with either T3 or T4
• Randomized, double blind, crossover
• Rx: T4 or T3 TID to achieve target TSH
• Lipids, glucose metab assessed 6 wks after
stable at target TSH level
• NSD in heart rate, TSH, BP, HDL, exercise
tolerance, or insulin sensitivity

WHICH IS BETTER - T4 or T3? Celi et al., JCEM 2011; 96:3466-74
• While taking T3, patients had a significantly greater decrease in:
– weight loss
– total cholesterol
– LDL cholesterol
– apolipoprotein B
• Conclusion: T3, at T4 equivalent dose based
on TSH level, had greater effects on weight &
lipid metabolism without differences in CV
function or insulin sensitivity
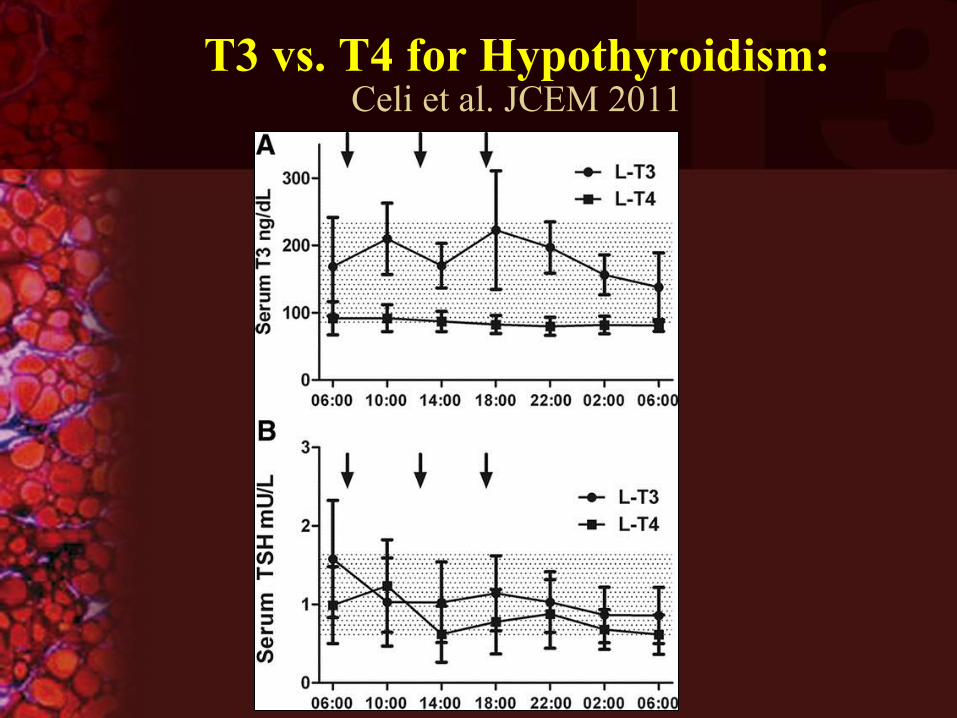
T3 vs. T4 for Hypothyroidism: Celi et al. JCEM 2011

T3 vs. T4 for Hypothyroidism: Celi et al. JCEM 2011

TREATMENT OF HYPOTHYROIDISM
AACE/ATA PRACTICE GUIDELINES 2012 Garber et al., Thyroid 22:1200-1235
• “not known whether genotyping will identify patients who will benefit from T4/T3”
• “Treatment is best accomplished using synthetic LT4”
T4/T3 COMBINATION THERAPY QUESTIONS
• Can hypothyroid patients be optimally replaced by thyroxine therapy alone?
• Are there convincing data that combined T4/T3 results in: – more physiologic tissue T4/T3 and serum TSH levels?
– improved clinical status?
• Are there new data that may provide a rationale for T4/T3 therapy?
T4/T3 COMBINATION THERAPY CONCLUSIONS
• Optimal Rx with T4 + T3 difficult due to lack of sustained release product
• No evidence of clear benefit of T3 + T4 in all patients, but patients with genetic polymorphisms may benefit
• Safest to follow ATA/AACE Guidelines
• But, in selected patients, may consider adding T3 to restore low FT3/FT4 ratio to NL while maintaining NL TSH

Back to our Case Discussion:
• 41-year-old woman who had RAI for Graves’ disease and is hypothyroid -
• Complains of fatigue and lethargy and is unhappy with her L-T4 treatment
SHOULD T3 BE ADDED TO T4 THERAPY FOR HYPOTHYROIDISM ?

SHOULD T3 BE ADDED TO T4 THERAPY FOR HYPOTHYROIDISM ?

District of Columbia Chapter Scientific Meeting – 2015
November 6 – 7, 2015
Therapy of Hypothyroidism:
New and Old Concepts
Leonard Wartofsky, M.D.
MedStar Washington Hospital Center
Georgetown University School of Medicine
Washington, DC

Review of Images Tools to assess attenuation
• Tomographic Images Location
Pattern
Does the pattern fit vascular territory
Look at individual frames
Cold defect on transaxial slices anterolateral to heart DePuey pp235 #6.







