Ron E. Polk, Pharm.D., FIDSA, FSHEA
Virginia Commonwealth University
Richmond, Virginia, USA
Background EU-US Summit Declaration from 3 November 2009
called for a “transatlantic taskforce on urgent antimicrobial resistance issues…”
TATFAR report from 22 September 2012 included 17 recommendations in 3 key areas.
Recommendation # 2: Convene a joint US/EU working group to propose standards for measuring antimicrobial use in hospital settings.
TATFAR WG: Participants & PresentationsECDC, 18/19 June, 2013
Surveillance of US hospital antimicrobial consumption CDC’s NHSN: Scott Fridkin Risk adjustment strategies: Ron Polk Pediatric considerations: Jason Newland, Kevin Garey
Surveillance of EU hospital antimicrobial consumption ESAC project: Hermann Goossens ECDC surveillance: Klaus Weist, Arno Muller Review of DDDs: Hege Salvesen Blix Pediatric measurements by DDD: Mike Sharland German stewardship module: Katja de With The French Stewardship Experience: Catherine
Dumartin,
Methods for Collection of Antimicrobial Consumption Data Klaus Weist, Arno Muller (contractor to ECDC). Surveillance Section, Surveillance and Response Support Unit, Antimicrobial Resistance & Healthcare-Associated Infections (ARHAI) Programme, ECDC
“Invited experts will convene with acknowledged expertise in data collection of antimicrobial consumption in hospitals, expertise in corresponding methods and risk adjustment, and hospital stewardship, respectively.
“They should identify the steps needed to synchronisemethodology or produce comparable data and propose standards for measuring antimicrobial use in hospital settings”.
The Goals and ChallengesHow to compare EU/U.S. antimicrobial
consumption data in hospitals?
Methodologies for collection of antimicrobial consumption data
Units of measurement for antimicrobial consumption
Denominators applied for the hospital sector
Implementation of indicators for antimicrobial consumption
Klaus Weist, MD
Why Measure Hospital Antimicrobial Use?
National Healthcare Safety Network (S. Fridkin)
Which antimicrobials are being used
How much are being used
What is variability in among hospitals [Causes of Variability (eg, case mix, “inappropriate use”, etc)]
[Can “benchmarking” improve use]
What are the trends in usage over time
How does U.S. compare to other countries [Is there an common and valid metric?]
NHSN Antimicrobial Use Option Objective: Measure antimicrobial usage to provide
risk-adjusted inter- and intra-facility comparisons
Antimicrobial Metric: Antimicrobial days (DOT)/ Days present by month, patient care location.
Locations: Facility-wide npatient patient care locations & emergency department
Data Source: eMAR / BCMA
Implementation: Partner with vendors to electronically capture numerator and denominator for importation into NHSN
Fridkin S, Srinivasan A. Clinical Infectious Diseases 2014;58(3):401–6
NHSN/AU Update(Scott Fridkin, 7 Feb 2015)
Launched January 2014
Currently about 60 hospitals are reporting required data
Risk adjustment remains challenging Likely adjusted by patient location
Likely Standardized utilization ratio (observed : expected)
CDC is working with partners to identify reasonable performance measures Goal is for some federal required reporting by 2018
Metrics may be mutually exclusive groups (draft) Broad spectrum anti-gram negative
Commonly used agents for surgical prophylaxis
Anti-MRSA agents
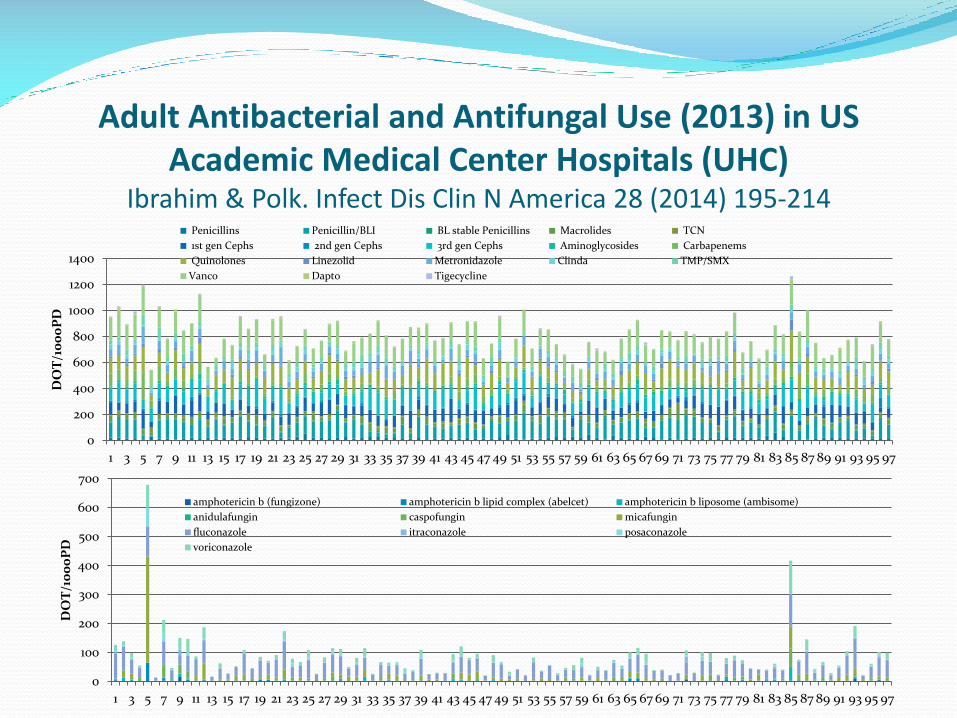
Adult Antibacterial and Antifungal Use (2013) in US Academic Medical Center Hospitals (UHC)
Ibrahim & Polk. Infect Dis Clin N America 28 (2014) 195-214
0
200
400
600
800
1000
1200
1400
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53 55 57 59 61 63 65 67 69 71 73 75 77 79 81 83 85 87 89 91 93 95 97
DO
T/1
00
0P
D
Penicillins Penicillin/BLI BL stable Penicillins Macrolides TCN
1st gen Cephs 2nd gen Cephs 3rd gen Cephs Aminoglycosides Carbapenems
Quinolones Linezolid Metronidazole Clinda TMP/SMX
Vanco Dapto Tigecycline
0
100
200
300
400
500
600
700
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53 55 57 59 61 63 65 67 69 71 73 75 77 79 81 83 85 87 89 91 93 95 97
DO
T/1
00
0P
D
amphotericin b (fungizone) amphotericin b lipid complex (abelcet) amphotericin b liposome (ambisome)
anidulafungin caspofungin micafungin
fluconazole itraconazole posaconazole
voriconazole
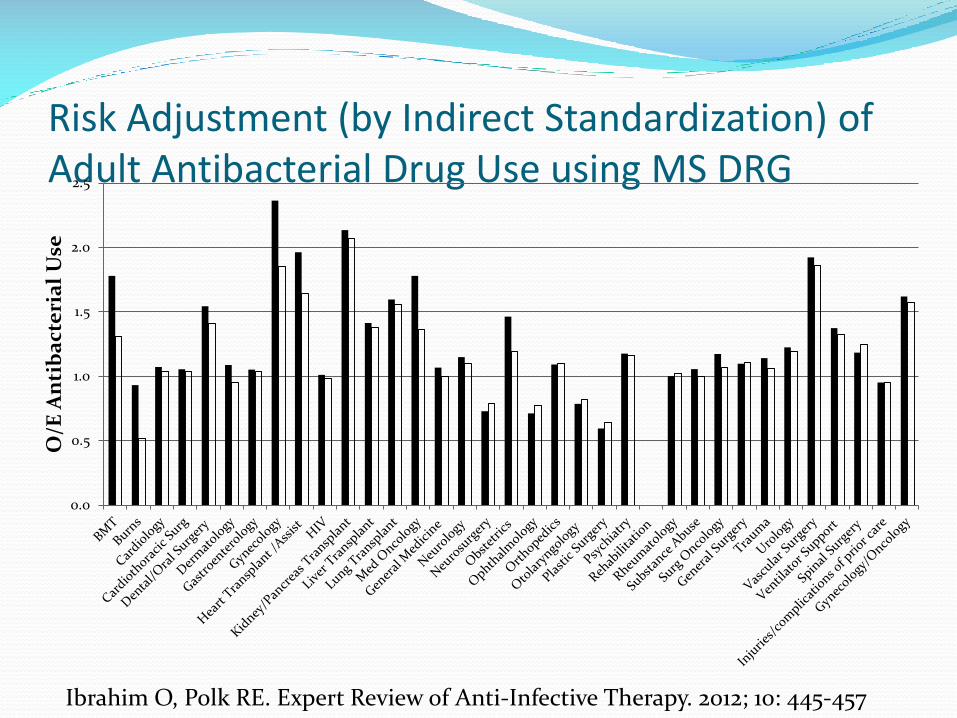
Risk Adjustment (by Indirect Standardization) of Adult Antibacterial Drug Use using MS DRG
0.0
0.5
1.0
1.5
2.0
2.5
O/E
An
tib
act
eri
al
Use
Ibrahim O, Polk RE. Expert Review of Anti-Infective Therapy. 2012; 10: 445-457
Summary of US Surveillance Measuring hospital antimicrobial consumption is
becoming possible in many/most US hospitals. Purchase data is least reliable Billing data (what the patient is charged for) Dispensing data is better yet; validation needed Administration data (e.g., BCMA, eMAR) is best, but not yet
well adapted to routine surveillance NHSN is linking proprietary pharmacy information systems
(eg, Theradoc™, Epic™) to resistance, but obstacles remain. DOT/1000PDs is current standard for US consumption, but
additional measures need evaluation (e.g., LOT ) Intensity of stewardship activities related to consumption*
* Pakyz et al. JAC, 21 Jan, 2015, Advance Access
EU Surveillance: H Goossens ESAC: European Surveillance of Antimicrobial
Consumption; Transferred to ECDC in 2011 (ESAC-Net). ESAC Longitudinal Survey (ESAC-LS):
Collect standardised pharmacy data , one hospital /country (N=18 hospitals). Apply a practical surveillance method:
To other hospitals in each country; to other countries Trends within hospitals, comparison between hospitals or
countries by appropriate stats analysis (i.e., TSA) Adjustment for clinical activity Assess metrics (DDD/occupied bed days vs. admissions)
ESAC Point Prevalence Surveys (ESAC-PPS) ARPEC: Antibiotic Resistance and Prescribing in
European Children
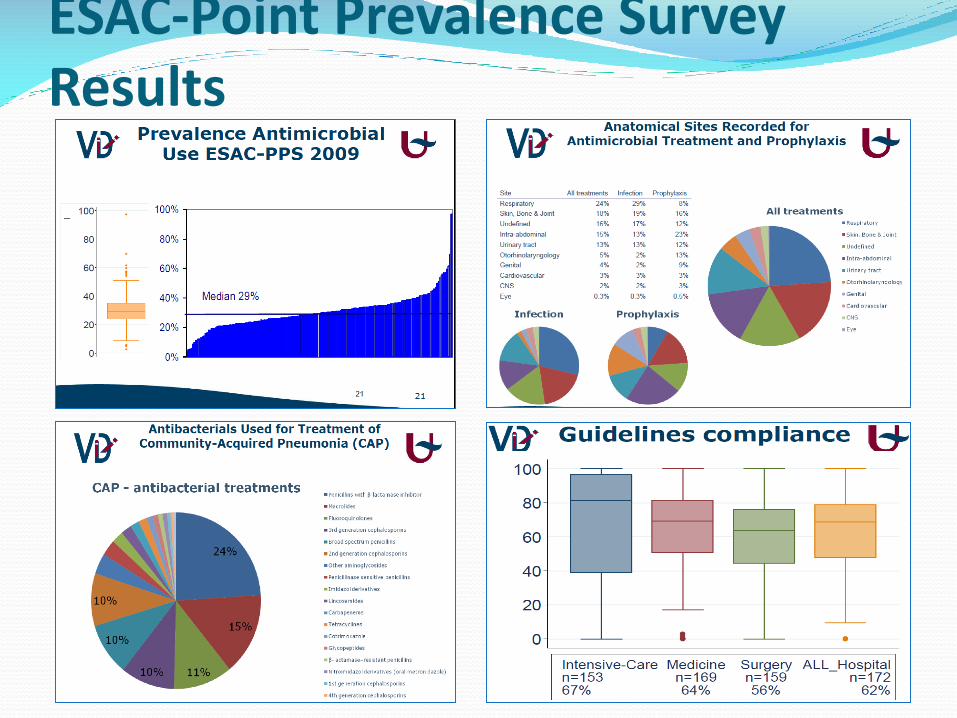
ESAC-Point Prevalence Survey Results
German training module to implement ABS (Katja de With, MD) DART (2008-13) included special training on hospital
ABS & infection control.
Clinical pharmacology, microbiology & infectious diseases, reading clinical trials, case study, therapy, pharmacoeconomics, epidemiology, AMS strategies, surveillance
Goal: produce ~350 experts by 2013
(and intensify ID physician training. )

Hospital Antimicrobial Consumption: French experience with
ATB-RAISIN (Catherine Dumartin)
Objectives
Describe France antibiotic consumption/trends
To provide a tool for benchmarking
To identify areas for improvement
Pharmacy dispensing to inpatients; DDD/PDs
1262 hospitals in 2011 (60% of all PDs in France)
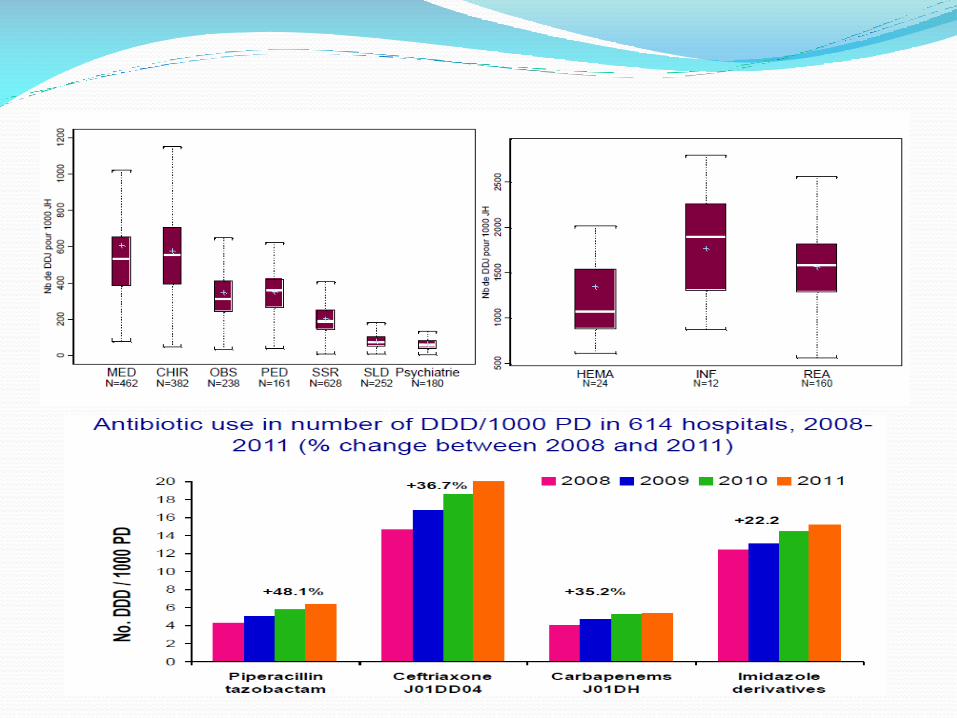
ABT-Raisin: Results
The Goals and Challenges (K. Weist)Comparison of EU/U.S. Antimicrobial Use? Methodologies for collection
Purchase, dispensing, billing, eMAR, BCAD, other?
Units of measurement DDD vs. DOT vs LOT & others yet to be identified
Denominators applied for the hospital sector Patient (bed) days vs. admissions/discharges vs ?
Implementation of indicators for antimicrobial consumption How to control for between-hospital differences ?]
[ASP activities and desired outcomes?] [How can ASPs best use these data? Most effective interventions ?
Role of technology in guiding therapy? ] [Outcomes: Cost savings, fewer adverse effects, lower rates of
resistance and CDI, improved clinical response, reduced LOS and readmissions]
[What is the role of benchmarking? Best methods to risk-adjust?] [How to develop multicenter investigations and comparable data?]
So where are we?? Is it possible to “harmonize” hospital
measurement of antibiotic consumption between EU and US?
What exactly is the goal of doing so?
How important is it to link hospital antibacterial drug use with outpatient use and non-human use? Are their common and meaningful measures?
Many possible outcomes of AS interventions. Which ones are feasible and most important?
“Don’t let the perfect be the enemy of the good.”?
19
#1) Do Less; Get More
• Measuring, severity-adjusting, and reporting institutional antibiotic use
• Reward lower institutional users with a financial bonus
• Penalize higher institutional users with a financial penalty







