
Contact Investigation Flagstaff, Arizona October 25, 2006
Tuberculosis Screening and Treatment of Latent TB Infection
L. Masae Kawamura, MD October 25, 2006
Tuberculosis Screening and Treatment of Latent TB Infection
2006
L. Masae Kawamura, M.D. Director, TB Control Section, San Francisco
Department of Public Health
Francis J. Curry National Tuberculosis Center University of California, San Francisco
1

Diagnosing TB infection and disease is aDiagnosing TB infection and disease is a primary care issueprimary care issue …..
Overview
• Review the basis of TB screening and populationsmore likely to have been infected with Mycobacterium tuberculosis
• Review medical conditions and factors associated with higher TB disease progression
• To discuss recent developments in diagnosis andtreatment of latent tuberculosis infection
• Briefly discuss prioritizing patients for evaluation,treatment, and completion
2
Transmission of Tuberculosis
CASE CONTACT
Site of TB Ventilation Closeness and Cough Filtration duration of contact Bacillary load U.V. light Immune status Treatment Previous infection
Active TB: Risk of Contagion Determined by bacillary load and sx’s � TB nodule: 100 - 1000 organisms � Cavity: millions to billions � Presence of cough � Positive sputum smears
Other factors Environment/site of exposure Respiratory protection On treatment Aerosolizing procedures (bronchoscopy)
3

Transmission and Pathogenesis of TB
Children <5% and immunocompromised adults
Exposure
Continued containment (90%)
No infection (70%)
Adequate
Non-immunologic defenses
Inadequate
Infection (30%)
Inadequate
Immunologic defenses
Adequate
Containment (95%)
Early progression* (5%)
Late progression(5%)
Inadequate
Immunologic defenses
Adequate
*Risk of progression much higher in
Flowchart: Evaluation to Treatment of LTBI
At-risk person
Tuberculin test + symptom review
Negative Positive
Chest x-ray
Normal Abnormal
Treatment Candidate for Rx Evaluate for not indicated of latent TB active TB
4

Symptoms and Signs of Active TB
Pulmonary Systemic • Chronic cough 40-80% • Fever – 65-80% • Sputum production • Chills/sweats • Pleuritic chest pain • Fatigue/malaise • Hemoptysis • Anorexia/weight loss
• No symptoms 10-20%
Goals of screening
� Identify active cases � Identify infected persons likely to benefit from
treatment of latent TB infection (LTBI) � Surveillance
1) Detect transmission: eg. evaluate efficacy of institutional control measures
2) Prevalence of TB infection in a population: surrogate marker of TB case rate
5

Who should be screened NOT the general population. Screening should be targeted to those at higher risk of TB.
� Populations with increased rates of TB infection and documented cases of transmission
� Persons with increased risk of progression to active TB
if infected
Program prioritization should be based on local epidemiologic data and the number of risk factors present in a given population or individual (eg. Shelters with high HIV rate, etc)
TB Screening: Determining risk by your assessment
� Risk of infection -prior exposure TB -current/recent exposure to TB -ongoing/chronic exposure
� Risk of disease progression -Medical risk factors -history of prior TB
6
Risk of infection
� Contacts of infectious TB cases
Risk associated with disease burden and presence of cough of the source case
� Foreign-born persons from TB endemic countries � Healthcare workers � Correctional facilities (inmates and staff) � Nursing homes � Long-term care facilities � Renal dialysis units
Risk of infection (2)
Medically underserved/low-income groups: � Homeless � Migrant workers � Low-cost hotel dwellers or crowded
impoverished living conditions
� Street drug users � Racial and ethnic minorities � Children with parents that have TB risk factors
7

Risk of progression
� HIV infection and other medical conditions
� Individuals with abnormal chest x-ray compatible with past TB
� Infants and children <5 yrs of age (sentinels of transmission)
Risk of progression (2)
Recent infection (contacts and converters):
� 4-5% risk of developing active disease within the first 1-2 years
� Risk may double if contact is <4 years old
� 40% progression to disease in infants younger than 12 months
� HIV co-infected progression much higher than 7-10 per year%!!!!
8

Risk of progression (3)
Medical conditions: Immunosuppressive agents � Immunosuppression � Chronic steroids � Lymphoma, leukemia
� Cancer chemotherapy � Injection drug use
� Cyclosporine� Diabetes � Malnutrition � New: TNFα blockade � Renal failure -Etanercept (Enbrel®) � Silicosis -Infliximab (Remicade®) � Alcoholism -Adalimumab (HumiraTM)
� Gastrectomy/ Jejunoilealbypass � Head and neck cancer
Frequency of screening
� Retesting: dependent on ongoing risk of TB exposure � Frequency: dependent on degree of chronic TB
exposure (use local epidemiology) – Annual testing* : HCWs, long term-care residents,
shelter or homeless CBO or substance recovery program staff
– Q 6 month testing* : TB clinic frontline staff, ER workers, pulmonologists performing bronchoscopy
– Periodic testing * : extended travel to high risk area *Need to correlate with local epidemiologic data
9

Diagnosis of tuberculosis infection
TB Skin Test (TST) QuantiFERON Blood Test
(QFT)
Mantoux Tuberculin Skin Test - Key Points
• TST should not be performed on someone with documented history of a positive test
• TST should be read and interpreted by a trained health care professional
• TB disease must be ruled out before initiating treatment for LTBI
10
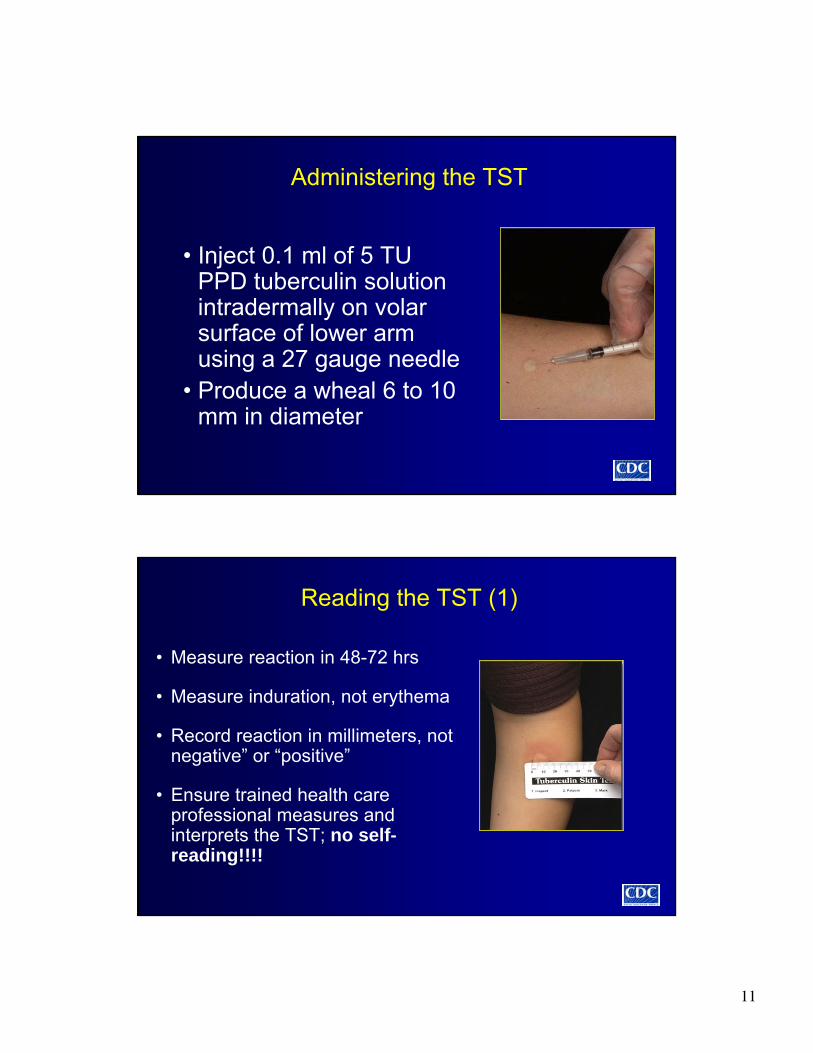
Administering the TST
• Inject 0.1 ml of 5 TU PPD tuberculin solution intradermally on volarsurface of lower arm using a 27 gauge needle
• Produce a wheal 6 to 10 mm in diameter
•
Reading the TST (1)
• Measure reaction in 48-72 hrs
• Measure induration, not erythema
• Record reaction in millimeters, not negative” or “positive”
• Ensure trained health care professional measures andinterprets the TST; no self-reading!!!!
11

Reading the TST (2)
• Positive TST reactions can be measured accurately for up to 7 days
• Negative reactions can be read accurately for only 72 hours
Tuberculin Skin Test Interpretation: CDC/ATS/AAP Cut Points
> 5 mm > 10 mm
� HIV co-infection � Foreign-born from a HR country � Immune compromise � Drug –users � Recent contact to TB � Living in HR congregate setting � Suspected disease � Specific HR groups
� Children < 4 yrs old (AAP)
>15 mm
All others (low risk groups) Why did you test?
12
Tuberculin skin test interpretation: tuberculin skin test conversion
� Signifies new infection
� CDC definition: >10 mm increase within 2 year period
� Problems with interpretation: conversions may actually represent BOOSTED reactions in some individuals
Tuberculin skin test interpretation: false-negative results
Host factors Technical factors � HIV
� The tuberculin used (i.e., � Recent TB infection (<3 improper storage,
months) contamination) � Infections (viral, fungal,
bacterial) � Improper method of administration, reading � Other illness affecting and/or recording of results lymphoid organs
� Live virus vaccination � Immunosuppressive drugs � Overwhelming TB
� Age (newborn, elderly)
13

Tuberculin Skin Testing “Boosting”
14 mm 11 mm 12 mm
Years
0 5 10 15 20 30 31
Infection TST TST TST TST
20
15
10
5
0
TST: False-positive Results
Causes
� Cross-reactions and boosted reactions from atypical mycobacterial infections and BCG
� Recent (<1 yr) or multiple BCG vaccination
� Misinterpretation of immediate hypersensitivity to tuberculin
� Switching tuberculin products (tubersol with applisol)
Indu
ratio
n(m
m)
14

Tuberculin skin test interpretation: the booster phenomenon (2)
Who needs two-step testing for boosterresponse?
� Individuals who will be tested on a regular basis (i.e., yearly)
� Elderly in high risk groups (>55 years)
The booster dose is usually administered 1-4 weeks after initial PPD and read in 48-72 hours
Screening individuals who are likely to have false negative TST results (young infants, HIV+s, immunosuppressed)
� Chest x-ray – look for evidence of TB infection (e.g., hilar calcification, upper lobe fibrosis, calcified granuloma)
� Symptom review
� Assess TB risk factors
� Decision to provide LTBI treatment in the absence of a positive TB test should be based on risk of true infection and public health implications
15
A new blood test for TB: Interferon-γ Release Assays
1. QuantiFERON-TB Gold (Cellestis Ltd., Carnegie, Australia) approved for use by the FDA approved-12/04
2. T SPOT-TB (Oxford Immunotec, Oxford, UK)
� Measures T-cell reactivity to M.tb specific M.tb antigens ESAT-6 and CFP-10
� Improved specificity: able to distinguish between TB and NTM, BCG infection
� Studies in contacts, HIV infected and children promising
QFT-G CDC guidelines: MMWR. December 16, 2004 / Vol. 54 / No. 49
� Recommends use of the test in all situations where the skin test is currently being used
-includes contact investigation, immigrant
evaluation and serial testing of HCWs
� Use caution when interpreting negative QFT results in children, immunocompromised, and HIV infected adults because of limited data
16

-
‘ ’
-
-
QFT-G CDC guidelines: MMWR. December 16, 2005 / Vol. 54 / No. 49
� Contact investigation: repeat test as you would the TST if initial QFT-G is negative at 8-10 wks
� If initial indeterminate results: repeat QFT-G or place TST or do nothing
� CDC guidelines for preventing the transmission of TB in health-care settings (MMWR 54 (No. RR-17, 1-141, 2005) also suggests that QFT-G can be used for surveillance and conversion: defined as change from negative to positive result
How QuantiFeron™ is performed
Culture overnight at 37Culture overnight at 37ooCC TB infected individuals respondTB infected individuals respond
by secreting IFNby secreting IFN-γγ
5 cc5 cc HeparinizedHeparinized whole bloodwhole blood
AntigensAntigens MitogenMitogen ControlControl
Transfer undiluted whole bloodTransfer undiluted whole blood into wells of a culture plateinto wells of a culture plate
and add antigensand add antigens
Harvest plasma from aboveHarvest plasma from above settled cells and incubate 60settled cells and incubate 60
min inmin in ‘SandwichSandwich’ ELISAELISA
Wash, add substrate,Wash, add substrate, incubate 30 minincubate 30 min
then stop reactionthen stop reaction
TMBTMB
COLORCOLOR
IFN-γ IU/mlOD
450
nmO
D 4
50nmStandard CurveStandard Curve
Measure OD,Measure OD, determine IFNdetermine IFN-γγ levelslevels
and interpret testand interpret test
Stage 2 IFNStage 2 IFN-gamma ELISAgamma ELISA
NilNil ControlControl
Stage 1 Blood CultureStage 1 Blood Culture
17
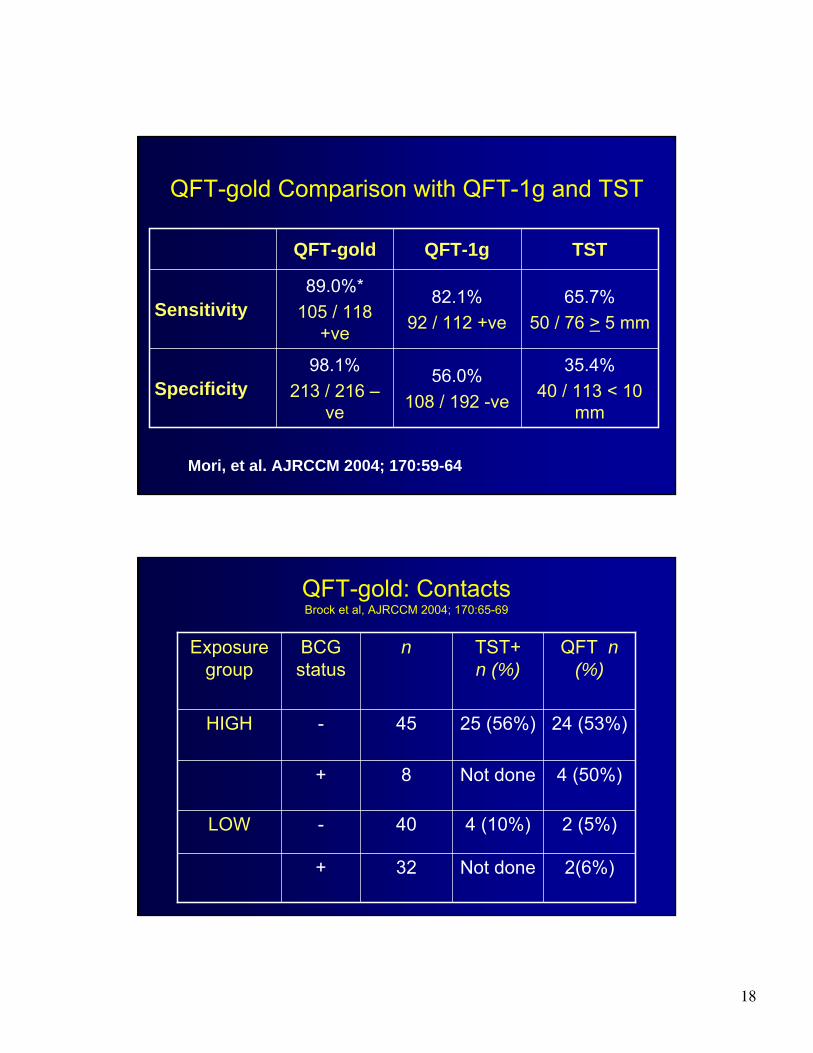
QFT-gold Comparison with QFT-1g and TST
QFT-1g QFT-gold TST
89.0%* 82.1% 65.7%Sensitivity 105 / 118 92 / 112 +ve 50 / 76 > 5 mm+ve
98.1% 35.4%56.0%Specificity 213 / 216 – 40 / 113 < 10 108 / 192 -veve mm
Mori, et al. AJRCCM 2004; 170:59-64
Exposure group
QFT-gold: Contacts Brock et al, AJRCCM 2004; 170:65-69
TST+ n (%)
nBCG status
QFT n (%)
HIGH - 45 25 (56%) 24 (53%)
+ 8 Not done 4 (50%)
LOW - 40 4 (10%) 2 (5%)
+ 32 Not done 2(6%)
18

QFT-gold: Contacts Brock et al, AJRCCM 2004; 170:65-69
• Study used recombinant ESAT-6 and CFP10 antigens (FDA approved QFT-G uses overlappingpeptides)
• Showed 94% agreement between TST and QFT-G in unvaccinated individuals
• QFT-G was not affected by BCG
Current IGRA studies on contacts: QFT-G and T-spot correlate better with exposure than TST
QFT-G vs TST QFT TST
Boosting No Yes Placement variability No Yes Reading variability No Yes Cross reactivity with BCG and NTMs No Yes Patient Visits > 1 > 2 Wait time for results (days) > 1 2-3
19
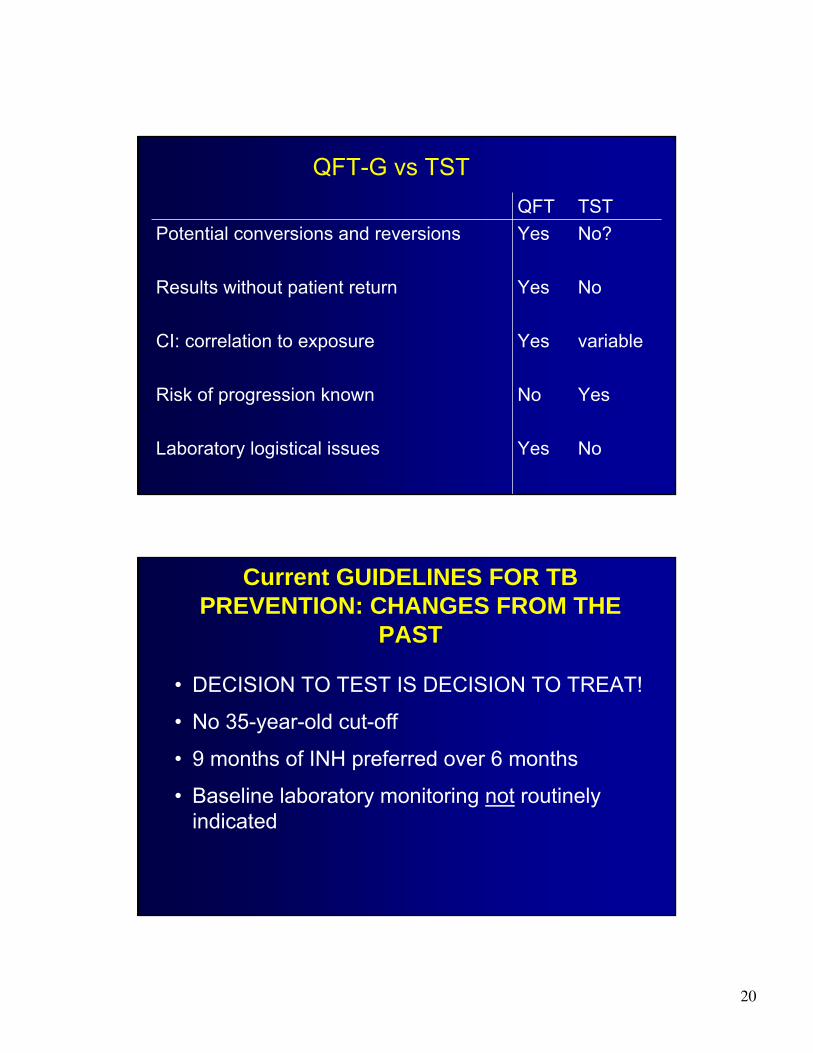
QFT-G vs TST QFT TST
Potential conversions and reversions Yes No?
Results without patient return Yes No
CI: correlation to exposure Yes variable
Risk of progression known No Yes
Laboratory logistical issues Yes No
Current GUIDELINES FOR TB PREVENTION: CHANGES FROM THE
PAST
• DECISION TO TEST IS DECISION TO TREAT!
• No 35-year-old cut-off
• 9 months of INH preferred over 6 months
• Baseline laboratory monitoring not routinely indicated
20

TREATMENT OF LATENT TB INFECTION How long is enough?
0 6 12 18 24
Months of Treatment
Cases per 100
5
4
3
2
1
0
Observed values
Calculated curve Calculated values
Comstock Int J Tuberc Lung Dis. 1999;10:847
• Lower TB rates among those who took 0-9 mo
• No extra increase among those who took >9 mo
NEW TB GUIDELINES FOR INH A Numbers Game
9
HIV Co-Infection Children
Prior TB on CXR (TB-4) Regular Folks
21

CURRENT OPTIONS FOR TREATMENT OF LATENT TB INFECTION
• Isoniazid for 9 months – either daily or twice weekly (6 months acceptable for programmaticreasons)
• Rifampin for 4 months (+/- INH) ATS/CDC AFRCCM 2000;161:s221
NOTE: Rifampin/pyrazinamide 2 months regimen isno longer recommended due to severe liverinjury and deaths (CDC revision 8/03)
Window Prophylaxis: LTBI treatment of TB exposed individuals with negative TB test results
Who should get window prophylaxis? • High risk TB contacts (young children and
immunocompromised/HIV+) who have initial negative TB test results AND significant TB exposure
When can window treatment be discontinued? • HIV-negative children: 8-10 weeks after contact broken to
untreated case and repeat TB test negative • Immunocompromised/HIV: Repeat testing may not be helpful
because of false negative results Use discretion of your TB program (some programs will treat for 9 months, while others may use CD-4 counts, hours of exposure, bacillary burden of index case and environmental factors)
22
TREATMENT OF LATENT TUBERCULOSIS IN SPECIAL SITUATIONS
• HIV-infected patients: Use rifabutin when rifampin is contraindicated with concurrent use of certain antiretroviral agents
• For persons intolerant of INH, use 4 months of rifampin
• Pregnancy is not a contraindication to LTBI treatment unless the source case is MDR Balance likelihood of true MDR infection, risk of progression, maternal resistance to taking meds with waiting until after delivery
What About LTBI and Drug-Resistance?
• Contacts of INH-resistant TB: 4-6 months of rifampin (longer for children and immunocompromised)
• Contacts of MDR-TB: consult an expert
If treatment is not available, refused or not tolerated: • Thorough patient education of TB signs and sxs • Close clinical monitoring for 2 years is recommended
for contacts and converters
23
Initiating Treatment
Before initiating treatment for LTBI • Rule out TB disease (CXR; sputum
samples; wait for culture result if sputum samples obtained)
• Determine prior history of treatment for LTBI or TB disease
• Assess risks and benefits of treatment
Isoniazid Regimens (1)
• 9-month regimen of isoniazid (INH) is the preferred regimen
• 6-month regimen is less effective but may be used if unable to complete 9 months
• May be given daily or intermittently (twice weekly) – Use directly observed therapy (DOT) for
intermittent regimen
24

Isoniazid Regimens (2)
• INH daily for 9 months (270 doses within 12 months)
• INH twice/week for 9 months (76 doses within 12 months)
• INH daily for 6 months (180 doses within 9 months)
• INH twice/week for 6 months (52 doses within 9 months)
Adverse Reactions - INH
Possible adverse effects – • Asymptomatic elevation of serum liver
enzymes • Clinical hepatitis • Peripheral neuropathy • Allergic rash
25
INH and Peripheral Neuropathy
• Occurs in < 0.2% of people taking INH at conventional doses
• More likely in diabetes, HIV, renal failure, and alcoholism
• Give pyridoxine supplementation (B6) 25-50 mg daily with above conditions
• B6 also recommended for pregnant and breastfeeding women (50 mg)
Rifampin Regimens (1)
• Rifampin (RIF) given daily for 4 months is an acceptable alternative when treatment with INH is not feasible
• RIF daily for 6 months is recommended for children and HIV infected patients
• In situations where RIF cannot be used (e.g., HIV-infected persons receiving protease inhibitors), rifabutin may be substituted
26

Rifampin Regimens (2)
• RIF daily for 4 months (120 doses within 6 months)
• RIF and PZA for 2 months should generally not be given due to risk of severe liver injury and deaths*
*MMWR August 8, 2003; 52 (31): 735-739
Rifampin: Adverse Reactions
• Hepatotoxicity • Drug rash • Many drug-drug interactions • Contraindicated in HIV-infected individuals
taking certain protease inhibitors or nonnucleoside reverse transcriptase inhibitors
Don’t forget to warn patients about orangediscoloration of body fluids!
27

Management of Patient Who Missed Doses
• Extend or re-start treatment if interruptions were frequent or prolonged enough to preclude completion
• When treatment has been interrupted for > 2 months, patient should be examined to rule out TB disease
• Recommend and arrange for DOT as needed
MONITORING PATIENTS
• Baseline laboratory testing not needed except for: 1) HIV infection 2) pregnancy 3) Hx of liver disease/heavy EtOH use 4) Patient on other liver toxic medication
• Monthly clinical monitoring : 1) adherence 2) side effects
28

INH HEPATOTOXICITY IN THE MODERN ERA
• 11,141 patients treated with INH from 1989-1995
• 11 had hepatitis (defined by symptoms, ↑ AST, resolution after stopping INH), no deaths
• Overall rate was 1 per 1,000!
Nolan JAMA 1999;281:1014
Asymptomatic Elevation of Serum Liver Enzymes
• Seen in 10%-20% of people taking INH – Levels usually return to normal after completion of
treatment
• Withhold INH if SGOT (AST) or SGPT (ALT) level exceeds 3 times the upper limit of normal if patient has symptoms of hepatotoxicity and 5 times the upper limit of normal if patient is asymptomatic
MMWR June 9, 2000; 49(No. RR-6): 39
29

Clinical Monitoring (1)
Instruct patient to report signs or symptoms of adverse drug reactions
• Rash
• Anorexia, nausea, vomiting, or abdominal pain in right upper quadrant
• Fatigue or weakness
• Dark urine
• Persistent numbness in hands or feet
Clinical Monitoring (2)
Monthly face-to-face visits should include a review of the following:
• Rationale for treatment • Adherence with therapy • Symptoms of adverse drug reactions • Plans to continue treatment
30

RE-TREATMENT OF LATENT TB INFECTION
• Re-infection can occur • Serious issue for immunocompromised
individuals
• Recommended for those who have HIV infection, other diseases causing chronicimmune suppression, and <21-years-old whohave been in contact with a smear-positive case
Counseling A Patient With LTBI
NEVER SAY: You’ve been “exposed” so you need to be treated.
INSTEAD: You have been exposed AND infected with the TB bacteria. But don’t worry…
Good news: you do not have the disease and you are not contagious to anyone.
Bad news: It is sleeping in your body and can wake up later, make you very ill and contagious to others
31
Counseling A Patient With LTBI (2)
Why get treated? Treatment will prevent future disease and protect you and those close to you.
Warning: • Taking medication for 6-9 months is a long time but
it takes that long to kill all or most of the TB germs. • “TOUGH bugs”… so take your medicine correctly
and completely
Summary
For every patient • Assess TB risk factors • If risk is present, perform TST or
QFT-G • If TST or QFT-G is positive, rule out
active TB disease • If active TB disease is ruled out,
initiate treatment for LTBI • If treatment is initiated, ensure
completion!
32

Resources for TB Medical Consultation
� Francis J Curry National TB Center: TB Warmline (415) 502-4700 � Your local TB program
Acknowledgement: Karen Steingart MD
3 kinds of infected contacts: 20 y/o immigrant from China, an HIV+ US-born homeless man,
and a 3 y/o US-born Hispanic child • Each with 20 hours of exposure to smear positive
cases in similar indoor environments
• All 3 have 1st time positive TSTs –12 mm 1. Which most likely represents recent transmission? 2. Who will most likely to develop disease? 3. Who needs to be evaluated most urgently? 4. What other factors will influence your decision? 5. Will you use DOT?
33

34
Thank you!







