THE 2015 WHO CLASSIFICATION OF LUNG TUMORS
Updates since the 2004 WHO classification
Gail Amir

THE MAIN CHANGES
• Greater role for immunohistochemistry
• Emphasis on genetic studies
• New classification for small biopsy specimens
• New approach to adenocarcinoma (2011)
• Diagnosis of large cell CA restricted to resected specimens
• Reclassification of squamous cell carcinoma

Grouping of neuroendocrine tumors
Addition of NUT carcinoma
Sclerosing hemangioma becomes sclerosing pneumocytoma
Hamartoma becomes pulmonary hamartoma

Created PEComatous tumors group: LAM, PEComa benign, PEComa malignant
New entity: pulmonary myxoid sarcoma EWSR1-CREB1 translocation
Adding myoepithelioma, myoepithelial carcinoma – can show EWSR1 gene rearrangement
Usefulness of WWTR1-CAMTA1 fusions in diagnosis of epithelioid hemagioendothelioma

Erdheim-Chester disease added to lymphoproliferative category
New group of ectopic tumors eg germ cell tumors, intrapulmonary thymoma, melanoma, meningioma

DIAGNOSIS OF LUNG CA IN SMALL BIOPSY SPECIMENS AND CYTOLOGY
• First WHO Classification to provide criteria for lung cancer diagnosis on small biopsy specimens
• In + 2/3 cases the tumor is advanced stage so this is usually the only material available for diagnosis
• Immunohistochemical stains are required for accurate diagnosis but tissue should be spared for molecular testing (don’t waste!)

GREATER ROLE FORIMMUNOHISTOCHEMISTRY
• The 2004 WHO classification was based primarily on morphology (small cell/non small cell)
Immunohistochemistry was advised in the following situations:
- Sarcomatoid carcinoma
- Neuroendocrine tumors
- DD of mesothelioma

In the 2015 WHO Classification immuno-histochemistry has additional roles:
- Undifferentiated NSCLC – solid adenoca vs non keratinizing SCC
- Diagnosis of large cell carcinoma NOS
HOW TO SAVE TISSUE
Clear cut adenoCA or keratinizing squamous cell CA
do not require additional stains (except TTF-1 to confirm
primary adenoCA)

In poorly differentiated NSCLC egsolid adenoCA, non-keratinizing SCC, a limited optimal panel should be chosen for accurate diagnosis
Tissue should be spared for molecular testing (don’t waste!)

THE BEST LIMITED PANEL
• TTF-1 (+ mucin)
• p40

INTERPRETATION OF STAINS
mucin +: adenoCA (>5 +ve cells in 2 HPF)
TTF-1/napsinA +: NSCLC favor adenoCA
p40/p63 +: NSCLC favor SCC
Solid, non-NE, -ve stains NSSC NOS – consider doing a limited immuno panel to confirm CA and r/o metastasis eg CK, MART-1/LCA
Note: +ve staining for TTF-1 &/or napsinA is considered adenoCA irrespective of p40/p63

SOLID ADENOCARCINOMA - MUCIN STAIN

• p40 and p63 have similar sensitivity but p40has superior specificity for SCC (99-100% vs 90%)
• Note: You can suggest but not make a definite diagnosis of adenosquamous CA on small biopsy specimen

ROLE FOR IMMUNOHISTOCHEMISTRY IN PERSONALIZED/PRECISION MEDICINE
Antibodies for 3 EGFR mutations are specific but not sensitive (av. 58%)
VENTANA ALK was approved by FDA in 2015 as a companion marker together with FISH
PDL-1 – 4 drugs each with its own PDL-1 antibody

NSCC IN SMALL SPECIMENS
ADENOCARCINOMA
Describe patterns (papillary, acinic, lepidic, micropapillary, solid) and features (eg colloid features, fetal features, enteric features)

PAPILLARY PATTERN

ACINAR PATTERN
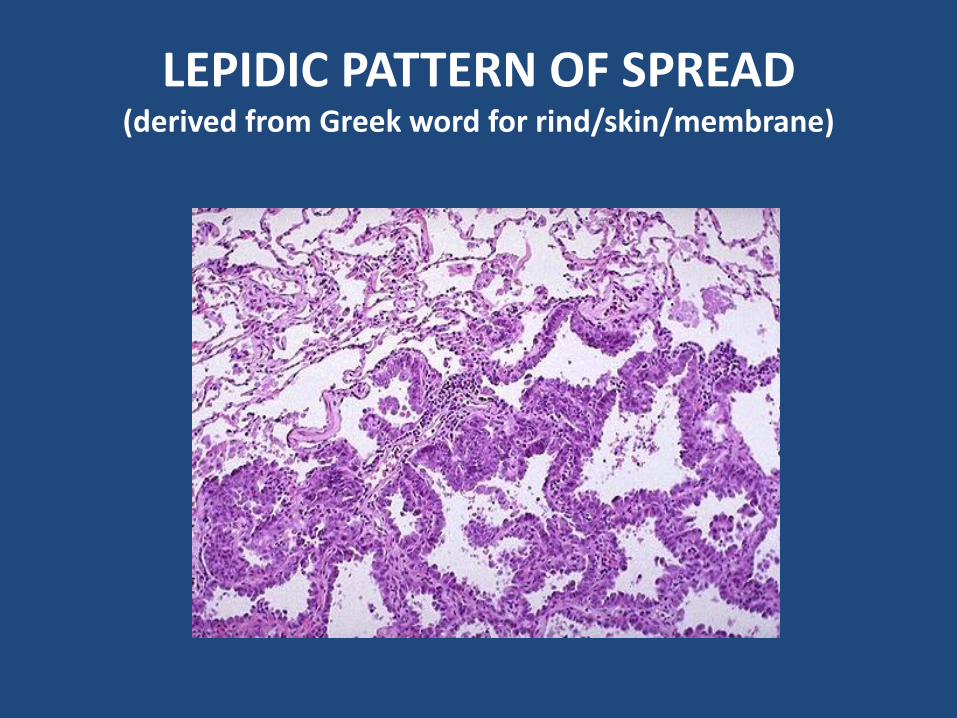
LEPIDIC PATTERN OF SPREAD(derived from Greek word for rind/skin/membrane)

If you see LEPIDIC pattern only on a small biopsy specimen add a note that invasive adenoCA cannot be excluded
Mucinous adenocarcinoma is usually lepidic and almost always invasive

ADENOCARCINOMA MICROPAPILLARY PATTERN

ADENOCARCINOMA SOLID PATTERN

SQUAMOUS CELL CARCINOMA
2004 WHO ClassificationPapillary – rareClear cell – rare, feature, not a subtypeSmall cell – rare, confusing; the term has been dropped
2015 WHO ClassificationKeratinizingNon-keratinizingBasaloid (large cell CA in 2004 WHO Classification)

SQUAMOUS CELL CARCINOMA
Keratinizing squamous cell carcinoma can be diagnosed without stains
The non-keratinizing and basaloid types need stains – p40/p63
Note: - AdenoCAs may appear to be “squamoid”- Basaloid SCC may express NE markers

SCC – BASALOIDperipheral palisading, abrupt keratinization

SCC – BASALOID prominent necrosisP40 +ve

CLASSIFICATION IN RESECTED SPECIMENS
Major changes in classification of adenocarcinoma
• Terms bronchioloalveolar carcinoma and mixed adenocarcinoma are out
• Addition of adenoCA in situ - AIS (joins atypical adenomatous hyperplasia as a pre-invasive lesion)
• Addition of minimally invasive adenocarcinoma - MIA
• Classify adenoCA by major subtype (papillary, acinar, lepidic, micropapillary, solid)

The term lepidic used for non-invasive component
Invasive mucinous adenoCA (instead of mucinous BAC) – usually lepidic with minor invasive component – r/o AIS, MIA on resection specimen
colloid adenoCA (instead of mucinous cystadenoCA)
clear cell and signet ring are features, not subtypes

ADENOCARCINOMA WHO 2015
• Pre-invasive lesions
• -Atypical adenomatous hyperplasia (<5mm)
• - Adenocarcinoma in situ (<3cm)
• Minimally invasive adenocarcinoma
• (lesion <3cm with <5mm invasion)
• Invasive adenocarcinoma
• Lepidic, acinar, papillary, micropapillary, solid
• Variants

ADENOCARCINOMA IN SITUDIAGNOSTIC CRITERIA
• Small - not >3cm• Solitary• Pure lepidic growth• No stromal, vascular, pleural invasion• No invasive histologic pattern eg acinar, papillary,
micropapillary, solid, colloid • No spread through air spaces (STAS)• Non-mucinous• Minimal or absent nuclear atypia• Septal widening with sclerosis, elastosis common• 100% disease free survival if resected

ADENOCARCINOMA IN SITU (not > 3cm)

LEPIDIC COMPONENT
• Lepidic pattern on a small biopsy could represent AIS, MIA, lepidic adenoCA, adenoCA with a lepidic component or even metastatic adenoCA (eg ovary, colon, pancreas) – don’t commit!

MINIMALLY INVASIVE ADENOCARCINOMA
• Small – up to 3cm
• Solitary
• Predominantly lepidic
• Invasive component not >0.5cm
• NO: lymphovascular, airspace, pleural invasion, tumor necrosis
• Non-mucinous
• 100% disease free survival if resected
•

MINIMALLY INVASIVE ADENOCARCINOMA

INVASIVE ADENOCARCINOMA
• Adenocarcinoma should be classified according the predominant pattern (papillary, acinar, lepidic, micropapillary, solid ) and a semi-quantitative assessment of other patterns
Reproducability among experts is not great!

HISTOLOGIC GRADING
• No established system
• Lepidic low grade
• Acinar, papillary intermediate grade
• Solid, micropapillary high grade

SPREAD THROUGH AIRSPACES - STAS
• Additional pattern of spread is now being recognized as a prognostic factor
• Presence of STAS is considered to be invasionand excludes a diagnosis of AIS, MIA
• Thought to be responsible for recurrence after limited resection (small low stage tumors)

SPREAD THROUGH AIRSPACES (STAS)

SPREAD THROUGH AIR SPACESthe lining cells are not malignant

INVASIVE MUCINOUS ADENOCARCINOMA

INVASIVE MUCINOUS ADENOCARCINOMA
• Usually predominantly lepidic with minor invasive component
• Adenocarcinoma in situ and minimally invasive adenocarcinoma of this variant are rare; can only be diagnosed/ruled out on resection specimen
• R/o metastatic mucinous carcinoma eg pancreas ovary

INVASIVE MUCINOUS ADENOCARCINOMA
• Has a different immunophenotype:
• TTF-1, napsin A negative
• CK7, CK20 positive

APPROACH TO MULTIPLE ADENOCARCINOMASmultiple primaries or intrapulmonary metastases?
• 1. Morphology may be helpful – compare growth patterns
•2. Multidisciplinary approach (clinical, radiologic, molecular, pathology) (the role of molecular studies remains to be established)

LARGE CELL CARCINOMA
• Can only be diagnosed on a resected specimen
• Exclude solid adenoCA, non-keratinizing/basaloid SCC , NEC - immunohistochemistry
• Changes from 2004 classification:
• LCNEC is now classified with other neuroendocrine tumors
• Basaloid CA is now considered a subtype of SCC
• Clear cell/rhabdoid are features rather than subtypes
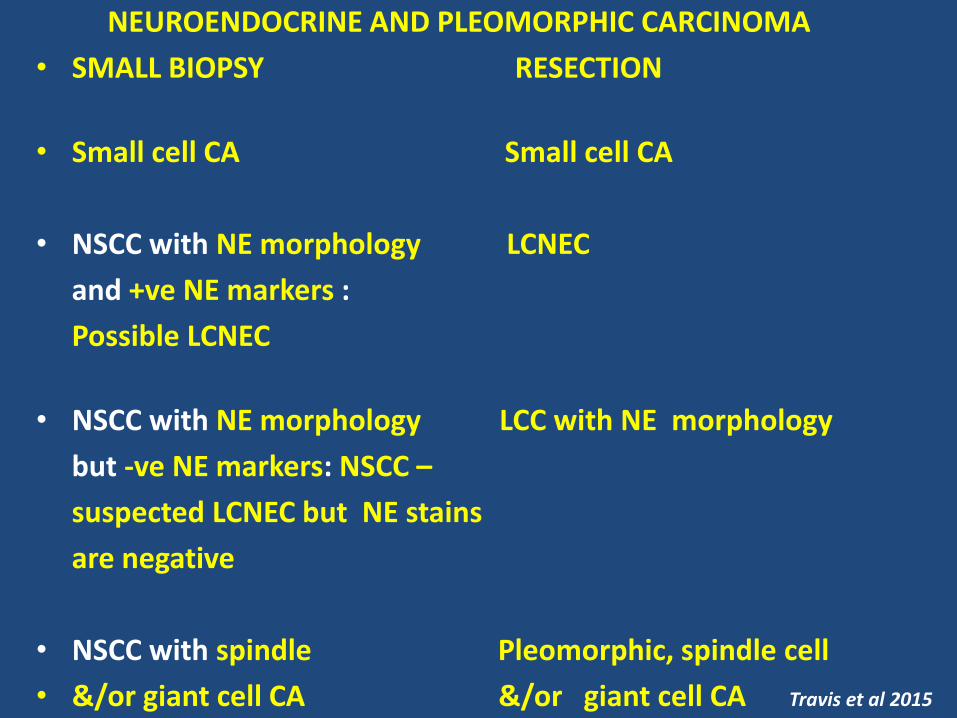
NEUROENDOCRINE AND PLEOMORPHIC CARCINOMA
• SMALL BIOPSY RESECTION
• Small cell CA Small cell CA
• NSCC with NE morphology LCNEC
and +ve NE markers :
Possible LCNEC
• NSCC with NE morphology LCC with NE morphology
but -ve NE markers: NSCC –
suspected LCNEC but NE stains
are negative
• NSCC with spindle Pleomorphic, spindle cell
• &/or giant cell CA &/or giant cell CA Travis et al 2015
•








