
VIRAL INFECTIONS
IHAB YOUNIS, MD
Part I

Some properties of viruses
• Possess no membranes, cytoplasm, ribosomes, or other cellular components
• They cannot move or grow
• They can only reproduce inside a host cell
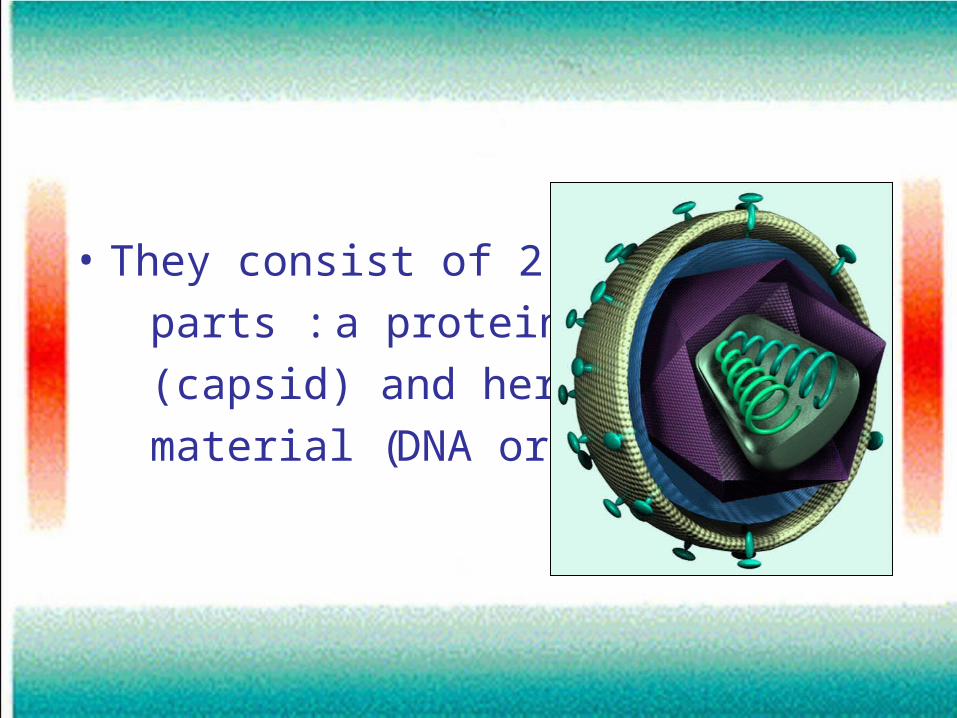
• They consist of 2 major
parts : a protein coat
(capsid) and hereditary
material (DNA or RNA)

1-virus attaches to a cell
2-Virus penetrates cell membrane&injects nucleic acid into it
3-Virus nucleic acid replicates inside the cell
4-New viral nucleic acids are packaged into viral particles&released
Viral life cycle
Related to Viruses
• Viroids : even smaller than viruses, consist of RNA strands that lack a protein coat
• Prions : infectious agents that are believed to be the cause of Mad Cow Disease, relatively newly found and much is not known about them

Viruses cause:
I-Proliferation of epidermal cells
II-Destruction leading to vesicle formation
III-Inflammatory response

Warts
(Verrucae)
Etiology• The DNA-containing human papillomavirus
(HPV)• Some believe that the number of its genotypes
has approached 130 or more • The virus enters the skin after direct contact with
recently shed viruses kept alive in warm, moist environments such as a locker room, or by direct contact with an infected person. The entry site is often an area of recent injury
• The incubation period: 1-8 months
• Contrary to popular mythology, touching a frog will not cause warts

Types
1 -Common warts (verrucae vulgaris)
• Develop anywhere but common on the hands, feet and knees
• Gray to flesh colored, raised from the skin surface & have rough, hornlike projections


2 -Plantar warts
• The only painful type
• Occur on the plantar surface, usually in high-pressure areas such as the heel and the metatarsal heads
• Usually flat because of pressure
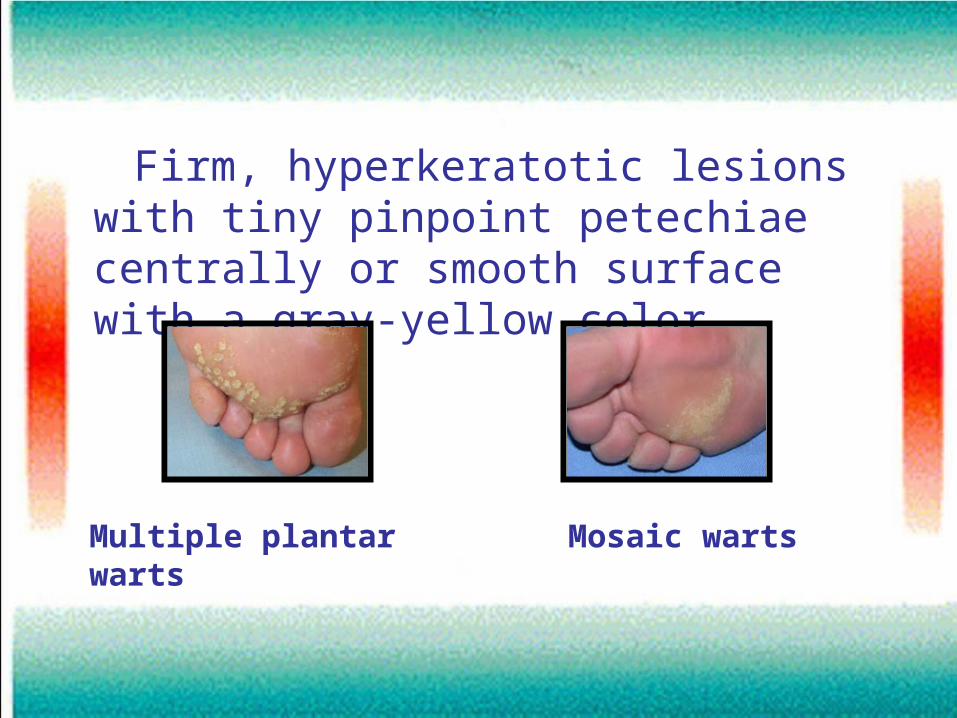
Firm, hyperkeratotic lesions with tiny pinpoint petechiae centrally or smooth surface with a gray-yellow color
Mosaic wartsMultiple plantar warts

3-Plane warts (verrucae plana)
• Most commonly seen on the face & back of hands
• Small individual papules about 5 mm in diameter

4-Digitate warts • Common on the head and neck

5 -Anogenital warts (cond.accuminata)
• Until 1907, they were believed to be a form of syphilis or gonorrhea
• Roughly, 10% of the general population in the USA have been infected by genital HPV at some time in their life
• 2 types:

Pink-to-brown
papillomatous papules
or nodules on the
genitalia, perineum,
crural folds and anus

Vary in size and can form large, exophytic, cauliflowerlike masses
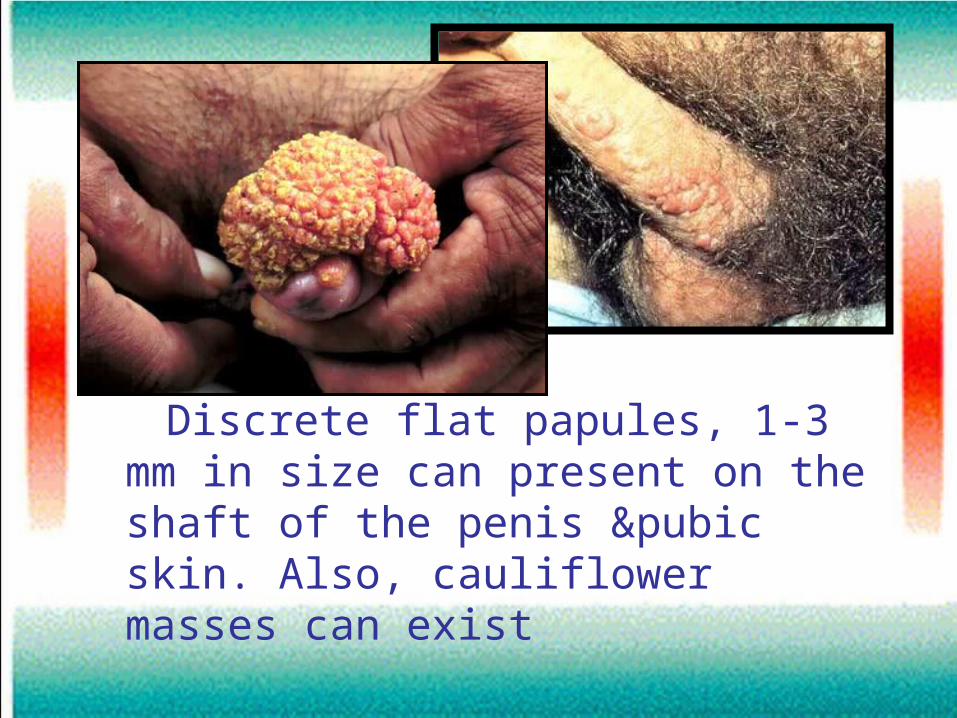
Discrete flat papules, 1-3 mm in size can present on the shaft of the penis &pubic skin. Also, cauliflower masses can exist
• 50% of homosexual men with SCC of the anus have a history of anorectal warts
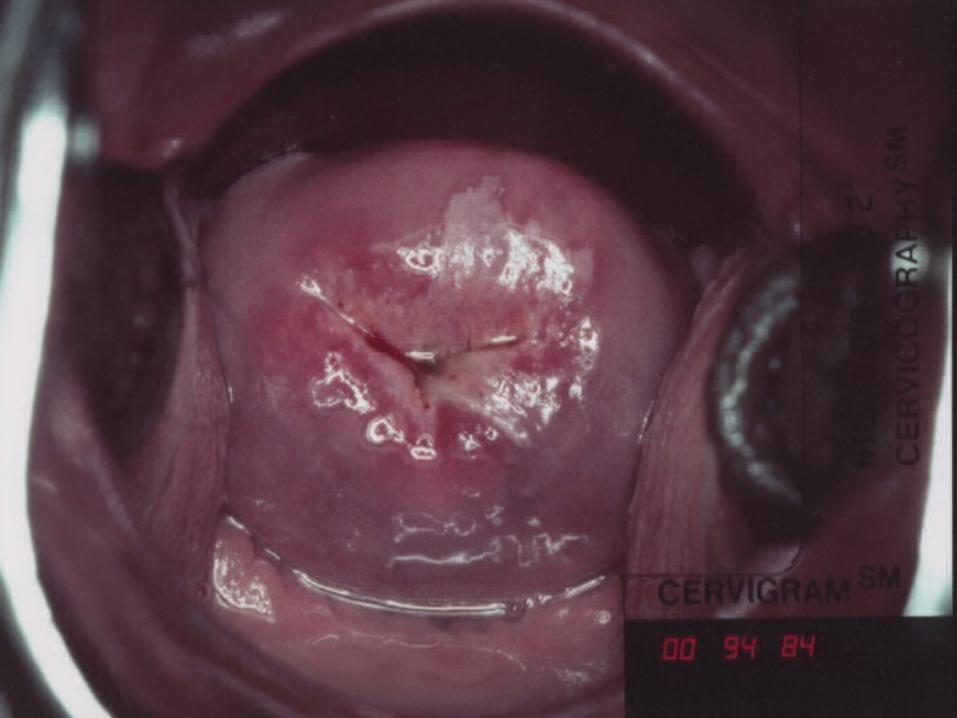
• On the cervix they are subclinical lesions
• Colposcopic examination with 3% acetic acid solution is required for identification
• Pap smear is required annually for fear of SCC
• Pap smear should be performed annually on all women once they become sexually active or when they have reached the age of 18 years if they have remained abstinent
• Once a woman has had findings within the reference range on 3 or more consecutive annual Pap smears, the Pap smear may be performed less frequently

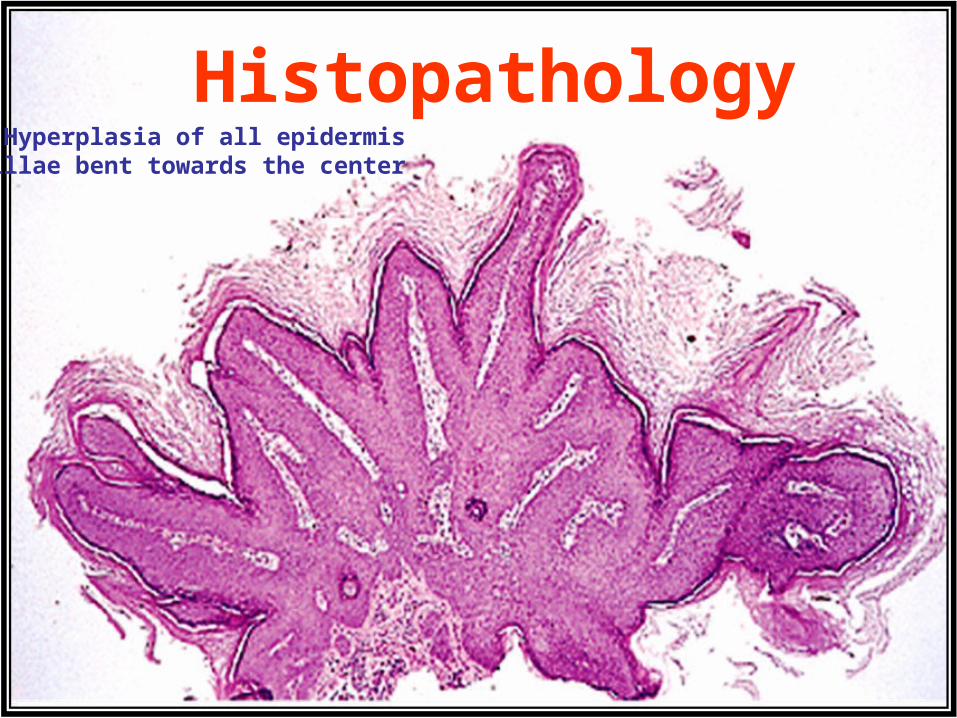
HistopathologyHyperplasia of all epidermis
Papillae bent towards the center
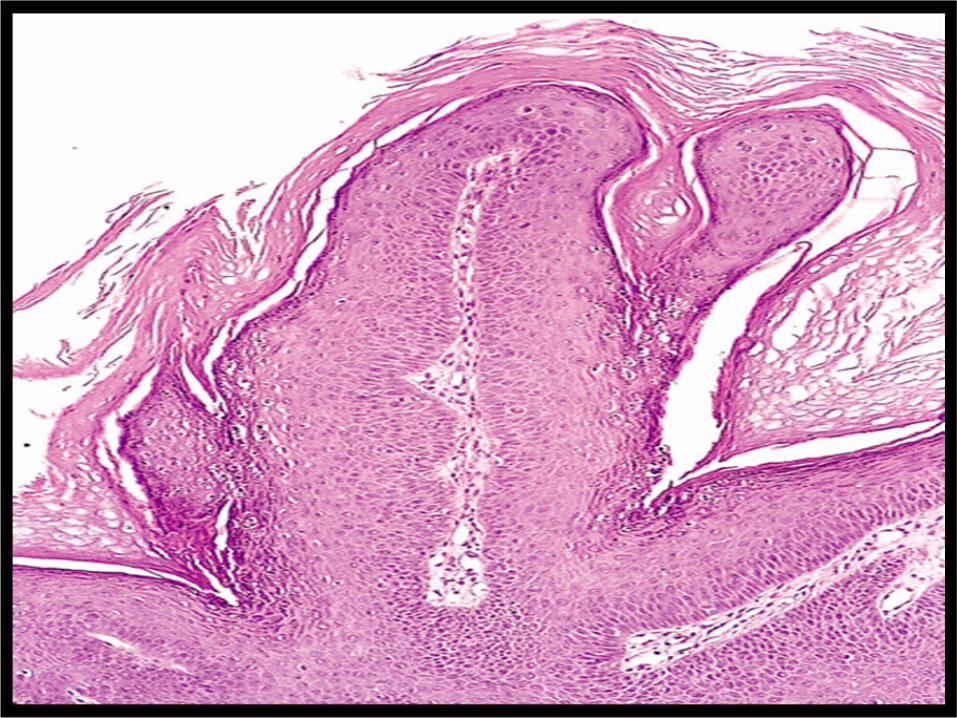

Koilocytes(altered keratinocytes) with deeply basophilic nuclei & halo

Koilocytes(altered keratinocytes) with deeply basophilic nuclei & halo
TreatmentDestruction by:
1-Chemical agents:
A- keratolytic agents
B-Cytotoxic agents
C- Immune response modifiers
D-Others
2-Physical agents

A-Keratolytic agentsTCA 25-90% sol.Salicylic acid 12-26%
Alone or with lacticVery powerful but painful Mild
Applied directly on a weekly basis. As the acid dries, a white frosting develops and should be
powdered with sodium bicarbonate to remove any
unreacted acid
Applied daily for 3 M alone or in combination with lactic acid
and collodion or in an adhesive plaster
Can be used on all types of warts
Used primarily to treat nongenital warts

B-Cytotoxic agentsPodophyllin 10-25% in
tincture benzoin5-Flurouracil 5% cream
Arrests mitosis in metaphase
Interferes with synthesis of DNA and RNA
Appllied by physician weekly for 6 weeks
Appllied by patient 1-3 times/w for as needed
Clean the skin, apply avoiding normal skin &
allow to dry for½ h. then remove. Subsequent applic.
can be for 1-4 h.
Same but remove after 3-10 h.

Effective only in anogenital warts
?Effective in all types
Contraindicated in pregnancy&on bleeding areas
Not formally indicated
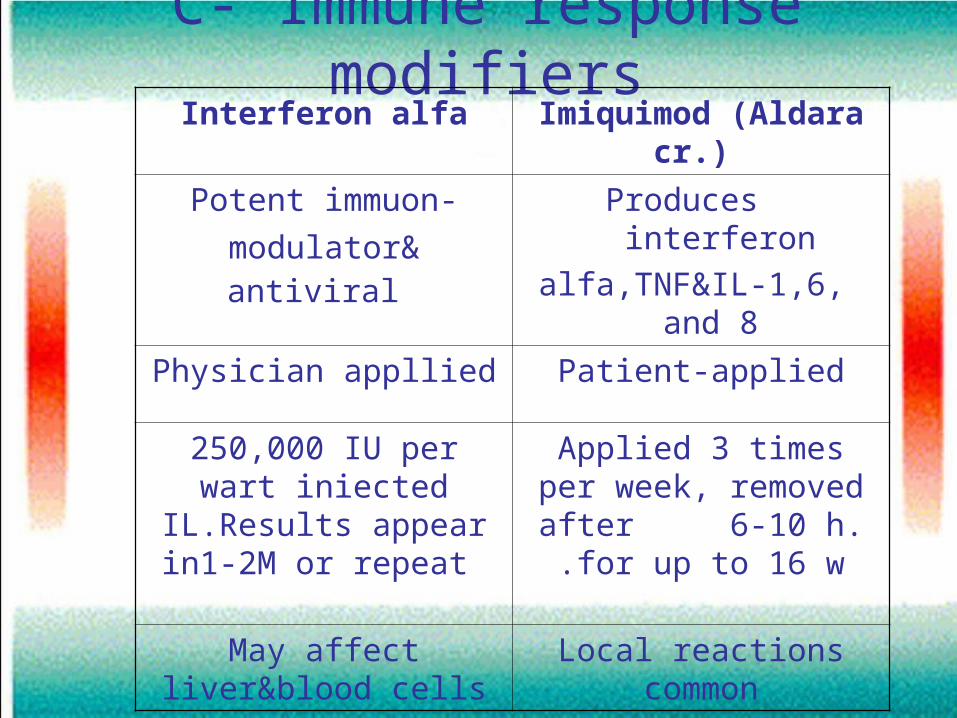
C- Immune response modifiersImiquimod (Aldara cr.) Interferon alfa
Produces interferon
alfa,TNF&IL-1,6, and 8
Potent immuon-
modulator& antiviral
Patient-appliedPhysician appllied
Applied 3 times per week, removed after 6-10 h. for up to 16 w.
250,000 IU per wart iniected IL.Results
appear in1-2M or repeat
Local reactions commonMay affect liver&blood cells
D-Other treatments
1-Retinoids
• Retinoic acid (Retin–A) topically may be usefull for plane warts
• Etretinate orally may be of some help in immunocopromised patiets

2- Formalin 2-3% solution
• May be effective for plantar warts
• Affected area is soaked for 15-20 min./day
• It is virucidal
• Time consuming&dries skin

3-Intralesional bleomycin
• 1mg/ml conc. is injected intralesionally till blanching
• A hemorrhagic eschar develops in 2-3 W.
• It is painful so, spared for refractory cases
4- Cimetidine (Tagamet)
• Orally:40mg/kg/day for3 months
• Has weak immunomodulatory effects
• Conficting results
5-Hypnosis
• Uncontroled studies

Physical methods
1-Electrosurgery • Electrosurgical equipment converts domestic alter- nating current into high frequency alternating current• When this current meets the high resistance of the skin, it produces heat

• Under local anaesthesia, the growth is curetted away and the base
burned by electrodessication
(needle in contact)or
fulgration(spark)
• The treated area appears raw immediately after surgery and develops a scab. Five to ten days later fresh skin appears which gradually blends in to the normal skin color
• 20% of warts can be expected to recur within a few months

2-Diathermy:• A-Unipolar:Current is delivered through a
unipolar needle (+ve electrode) to the point required then passes in patien’s body to a –ve electrode connected to the patient
• a burn at the –ve electrode may occur due to faulty connection
• B-Bipolar:Current is produced and collected by the 2 poles avoiding the hazards of unipolar diathermy
Advices to the patient
• Your wound may be tender 1-2 hours after the curettage when the local anaesthetic wears off
• Leave the dressing in place for 24 hours • Avoid strenuous exertion&stretching of the area• Keep the wound dry for 48 hoursIf the wound
becomes red or very painful, consult your doctor• The wound will take approximately 2-3 weeks to
heal over. The scar will initially be red and raised but usually reduces in color and size over several months

3-Cryotherapy • Liquid nitrogenis the most commonly used agent ( boiling pont -196°C)
• Many practitioners use a spray, but cotton wool-tipped sticks are still widely used and can be preferable when treating children or for warts near the eyes
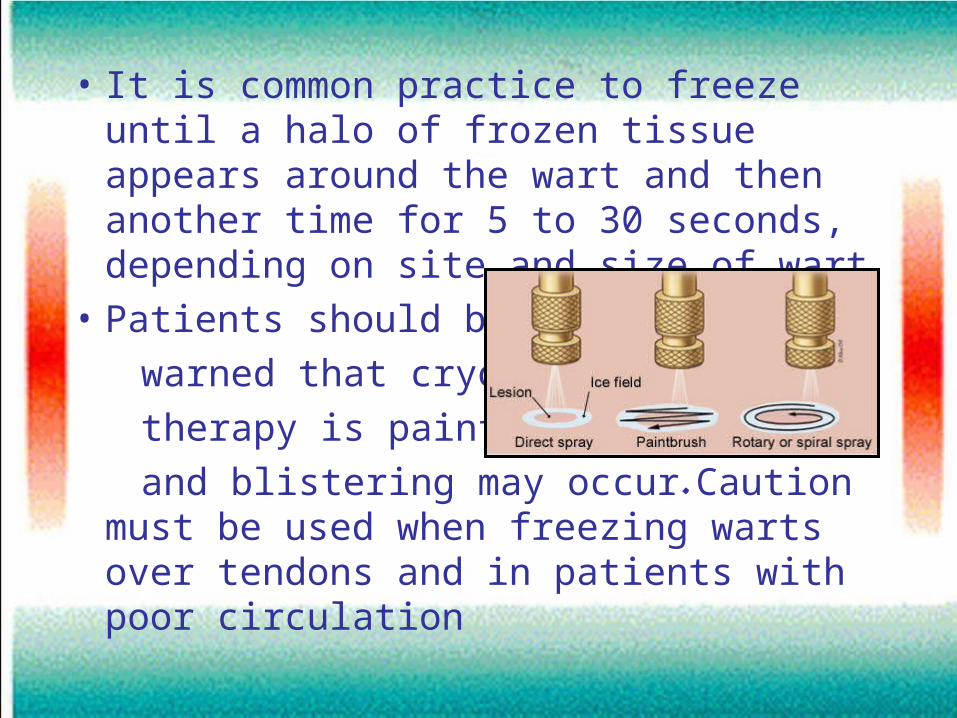
• It is common practice to freeze until a halo of frozen tissue appears around the wart and then another time for 5 to 30 seconds, depending on site and size of wart
• Patients should be
warned that cryo-
therapy is painful
and blistering may occur. Caution must be used when freezing warts over tendons and in patients with poor circulation

4-Lasers• Carbon Dioxide Laser Periungual and subungual lesions, which can be difficult to eradicate by other methods, may be particularly appropriate for this treatment• Pulsed Dye Laser -Depends upon the energy absorption within the
capillary loops of the wart and hence localized tissue necrosis- Pain and scarring are less than with the CO2laser

5-Photodynamic Therapy
• Depends upon the uptake by abnormal cells of a chemical, usually amino-laevulinic acid (Levulan), topically
• After 3-6 h photo-oxidation is invoked by irradiation of affected tissue using laser or non-laser light for 5-45 min.

Epidermodysplasia verruciformis
Etiology• Results from a genetically determined defect in
cutaneous immunity that makes them susceptible to widespread viral infection
• Patients are usually infected with more than 30 types of HPV. 90% of EV-associated skin cancers contain HPV types 5,8, and 47
• Carcinogenic cofactors, such as ultraviolet B and x-ray irradiation, are likely involved in the progression from benign warts to malignancy

Clinically• The disease usually begins in infancy or
early childhood
• Skin lesions on the face are indistinguishable from plane warts
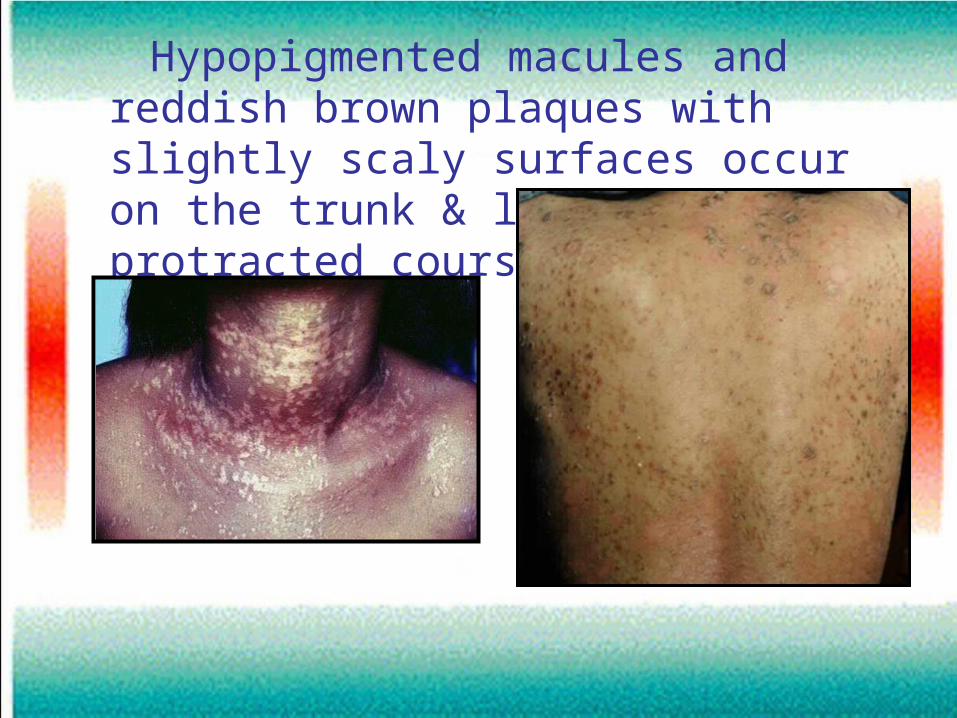
Hypopigmented macules and reddish brown plaques with slightly scaly surfaces occur on the trunk & limbs with a protracted course

• Malignant transformation of skin lesions has been observed in more than one half of the patients followed up for 20-30 years• Most cancers remain local, and metastasis is extremely uncommon

BOWENOID PAPULOSIS

• Described in 1977 by Kopf and Bart
• Induced virally by HPV
• Lesions appear to run a benign course, although a number of case reports associate BP with malignant invasive transformation (2.6%)

May be considered a transitional state between a genital wart and Bowen disease

Clinically
• Occurs in young sexually active persons• Spontaneous regression occurs within several
months• A more protracted course is believed to occur in
older patients and, possibly, with lesions consistent with certain HPV types. These lesions may last as long as 5 years, or they may never regress completely
• The lesions tend to be asymptomatic but can be inflamed, pruritic, or painful
• Presents as solitary or multiple, small, pigmented (red, brown, or flesh-colored) papules with a flat-to-verrucous surface
• The lesions can coalesce into larger plaques
• Lesions occur most commonly on the shaft of the penis or the external genitalia of females

Bowen
Bowenoid


• Circumscribed epidermal proliferation composed of pleomorphic cells with clumped nuclei and numerous
occasionally abnormal mitoses• The integrity of the dermal- epidermal border is preserved• The pattern may be identical to Bowen disease
or squamous cell carcinoma in situ, occurring on nongenital skin

Treatment
• Podophyllin 10-25% in tincture benzoin weekly
• TCA 25% every 2 weeks
• Imiquimod (Aldara) 3 nights per wk
MOLLUSCUMCONTAGIOSUM
Etymology: Latin molluscus, thin-shelled, soft.Marine invertebrates of the phylum Mollusca, typically having a soft unsegmented body.

Etiology
• MCV is a DNA ds virus (largest known virus)
• Type1 responsible for 76-97 %
• Type 2
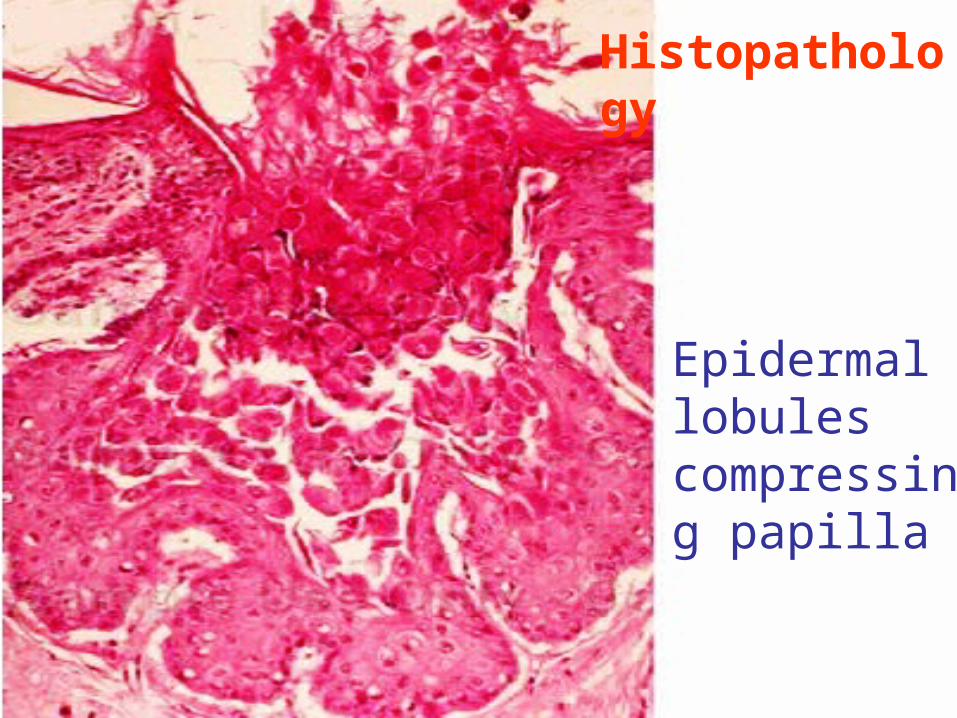
Epidermal lobules compressing papilla
Histopathology
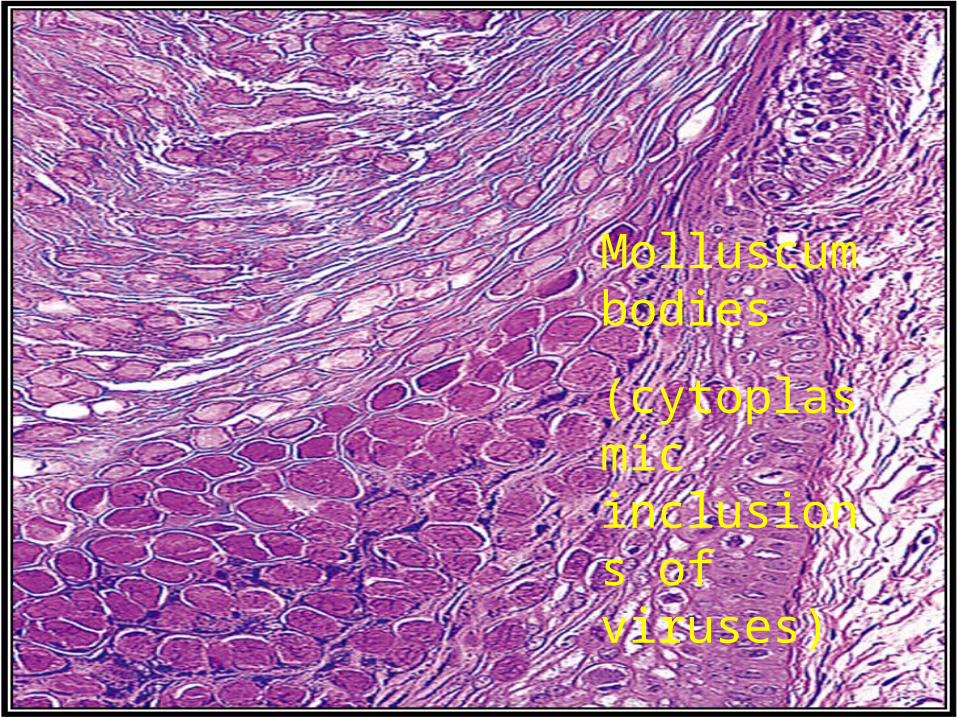
Molluscum bodies
(cytoplasmic inclusions of viruses)
Clinically• Incubation period: 2 weeks-6 months
• Distribution– In children: lesions mainly on the trunk and
extremities– In adults: lesions often are located on the
lower abdominal wall, inner thighs, pubic area, and genitalia
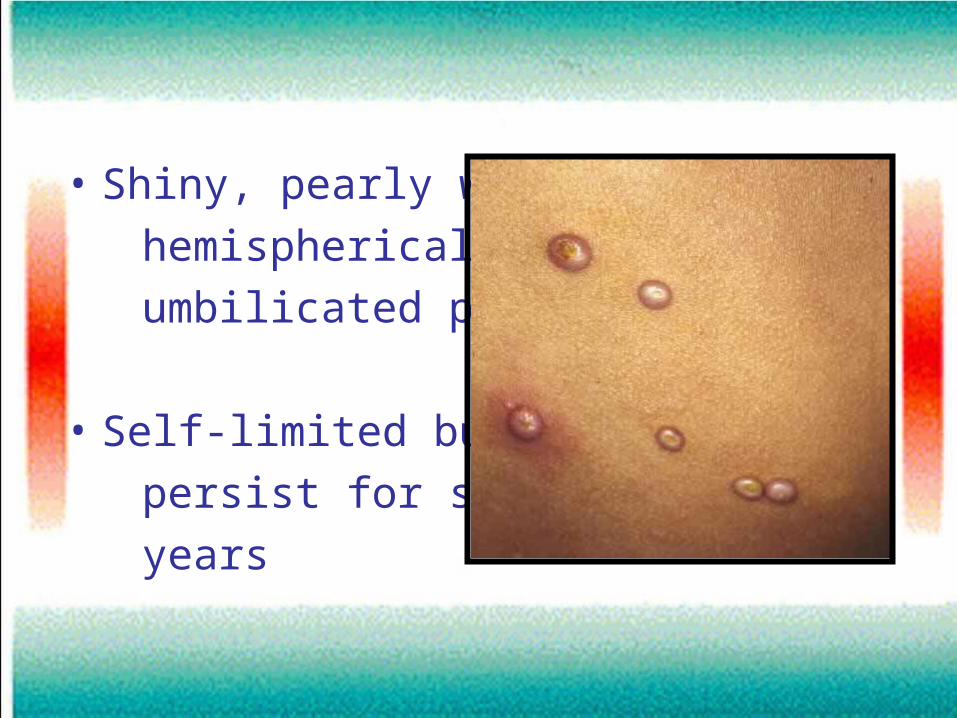
• Shiny, pearly white,
hemispherical,
umbilicated papule
• Self-limited but can
persist for several
years

Diagnosis
• Freezing accentuates umbilication
• Microscopic examination of crusshed lesion

Differential diagnosis
PyogenicGranul.
Kerato-acanth.
Epithelioma
Treatment• ? Wait for spontaneous resolution
• Destruction:
I-By physical methods:
Cryotherapy
Electrocautary
Laser
Expression by forceps
II-By topical cauterizing agents:
1-TCA
2-Silver nitrate
3-Phenol
4-Wart preparations
5-Others

1-Trichloroacetic acid• Causes less irritation&can be used in anal areas • Response:incomplete&frequent recurrences
occur• Repeat q1-2wk • Safety for use during pregnancy has not been
established• Contraindications: premalignant or malignant
lesions

2-Silver nitrate
• Applied daily for approximately 5 d
• Safety for use during pregnancy has not been established
3-Phenol
• 10-20%
• Painful

4-Wart preparations
• Salicylic acid 20%
Lactic acid 5% }Collomack
Polidocanol(topical anesth.) 2%
• Once or twice weekly
Other topical therapies:
• Tretinoin
• Podophyllin

III-Systemic drugs:
• Cimetidine (Tagamet) orally:40mg/kg/day for 2 months







