Why we need DCD Randolph Schaffer, MD
Scripps Center for Organ Transplant March 5, 2015
No Disclosures
Why we need DCD
• History of DCD
• Early hopes
• Clinical outcomes
• Risks of overuse
• Ethical issues
History of Organ Donation in the US
• 1954 – First successful US transplantation – Kidney from identical twin living donor
• 1962 – First successful deceased donor kidney transplant – Early immunosuppressive therapy era
• 1978 – Discovery of cyclosporine
History of Organ Donation in the US
• Early era: – Living donation – Donation following declaration of death based on
irreversible cessation of circulatory and respiratory function
i.e. the options were living donor and DCD – 1960s: Improved ICU care (mechanical ventilation/
medical support) – Need for better criteria for determining death
Transplantation Legislation
• 1968 Uniform Anatomical Gift Act (UAGA) • Uniform legal environment for donation across the US • Gave adults the right to donate their bodies/organs
upon their death “without subsequent veto by others.”
• 1981 Uniform Determination of Death Act • Codified existing common laws for determining death • “An individual who has sustained either irreversible
cessation of circulatory and respiratory functions, or irreversible cessation of all functions of the brain, including the brain stem is dead.”
Transplantation Legislation
• 1984 National Organ Transplant Act (NOTA) • Established the OPTN (data reporting began in 1988) • Expanded the OPO system • Prohibited commercial transactions in organs
• 1987 Amended UAGA • Provided explicit priority to the intention of donors
over that of their relatives • Prohibited the sale of body organs • Included required request provisions
Brain Death
• 1981 Uniform Determination of Death Act • “An individual who has sustained either irreversible
cessation of circulatory and respiratory functions, or irreversible cessation of all functions of the brain, including the brain stem is dead.”
• Use of neurologic criteria for determination of brain death has gained wide medical legal, ethical and public acceptance in the US.
Pivotal time in organ transplantation
• 1950-70s – Limited immunosuppressive therapy options
(steroids/azathioprine) – “DCD” donors
• 1978-81
– Cyclosporine – UDDA: Brain Death soon becomes foundation for
organ donation and benchmark for deceased donor transplant outcomes
“Narrowing the Gap”
• 2006 Institute of Medicine – Committee on Increasing
Rates of Donation – Multifaceted approach
• Systems support, consent, facilitating donation decisions, presumed consent, incentives, living donation
– “Expanding the population of potential deceased donors”
IOM Reports on DCD • 1997, 2000, 2006
• “emphasized the importance of developing the
nation’s capabilities for donation after circulatory determination of death (DCDD*)… as there is an opportunity to significantly expand the number of organ donors”
• “One set of conservative estimates suggests that at least 22,000 of out-of-hospital cardiac arrest deaths annually in the [US] could be potential donors if important ethical and practical matters could be resolved”
Terminology
• DCDD – Donation after circulatory determination of death
• NHBD – “Non-heart-beating” donor
• DCD – Donation after cardiac death – Donation after circulatory death
• DNDD / DBD – Donation after neurologic determination of death – Donation after brain death
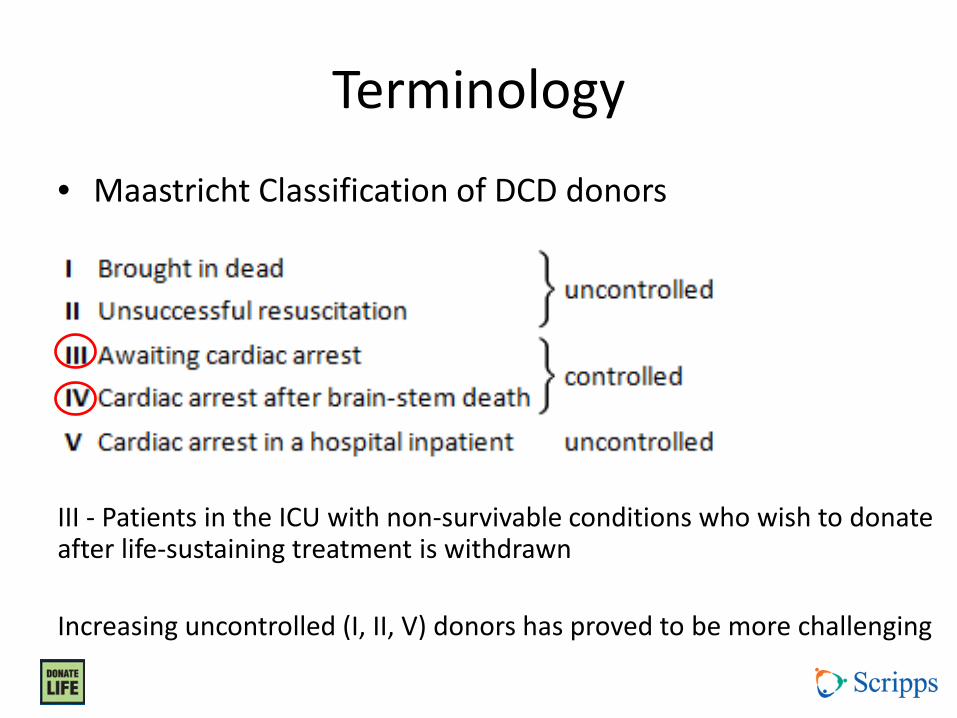
Terminology
• Maastricht Classification of DCD donors
III - Patients in the ICU with non-survivable conditions who wish to donate after life-sustaining treatment is withdrawn Increasing uncontrolled (I, II, V) donors has proved to be more challenging
Controlled DCD
• Expected withdrawal of care • Allows family time to psychologically prepare • Allows for determination of donation
potential – Potential organ(s) and potential recipient(s) – Appropriate procurement team(s)
• Facilitates procurement process – Minimizes ischemic time to organs
Recommendations from IOM
• All OPOs and hospitals should have DCD protocols in place
• DCD should be considered part of the continuum of quality end-of-life care
• Openness and public education regarding DCD to ensure public trust
• Adherence to ethical principles
Ethical Principles of DCD
• Organ donors must be dead at time of organ removal – Determination of death after circulation permanently
(irreversibly) lost • 1997/2001: 5 minute wait to ensure no auto-resuscitation • 2006: “At least 2 minutes of observation is required, and more
than 5 minutes is not recommended.”
• Active euthanasia is absolutely prohibited • Complete openness about policies and protocols • Informed consent • Respect for donor’s and family’s wishes • Enhancing rates of organ donation is of value to society • Safeguards against conflict of interest
Ensuring Success from Donation
DBD • After neurologic
determination of death: – Artificial cardiopulmonary
support continues – Maintains normal circulation
of oxygenated blood to preserve organ viability
– Maximizes utilization of organs from the donor
DCD • After circulatory
determination of death: – Lack of blood flow and
oxygenation leads to tissue ischemia / damage
– Measures to ensure organ viability must be implemented as rapidly as possible
– Duration of tolerable ischemia varies by organ
• Kidney / Lung • Pancreas • Liver • Heart
Ensuring Success from Donation
• Every protocol / maneuver to enhance the DCD process and every intervention to the organ after procurement represents an effort to minimize ischemic time and enhance organ viability (and approximate DBD donation success)
• Better definition of when organ ischemia begins
• Better definition of graft function after DCD
Maneuvers to Enhance Outcomes
• Anticoagulants / thrombolytics (heparin / TPA) • Organ perfusion solutions • Organ perfusion / surgical techniques • Re-intubation after death (lungs) • ECMO • Pulsatile organ perfusion after recovery • Minimizing cold ischemic time of organ • Proper recipient selection
– Distance, appropriate for risk, anatomy, etc.
Defining Success with DCD
• Increase number of organs transplanted?
– Should be additive (i.e. “expand the pool”)
• Maintain patient and graft survival rates?
– Compared to organs from DBD
– Compared to not getting transplanted
Defining Success with DCD
• Increase number of organs transplanted?
– Should be additive
• Maintain patient and graft survival rates?
– Compared to organs from DBD
– Compared to not getting transplanted
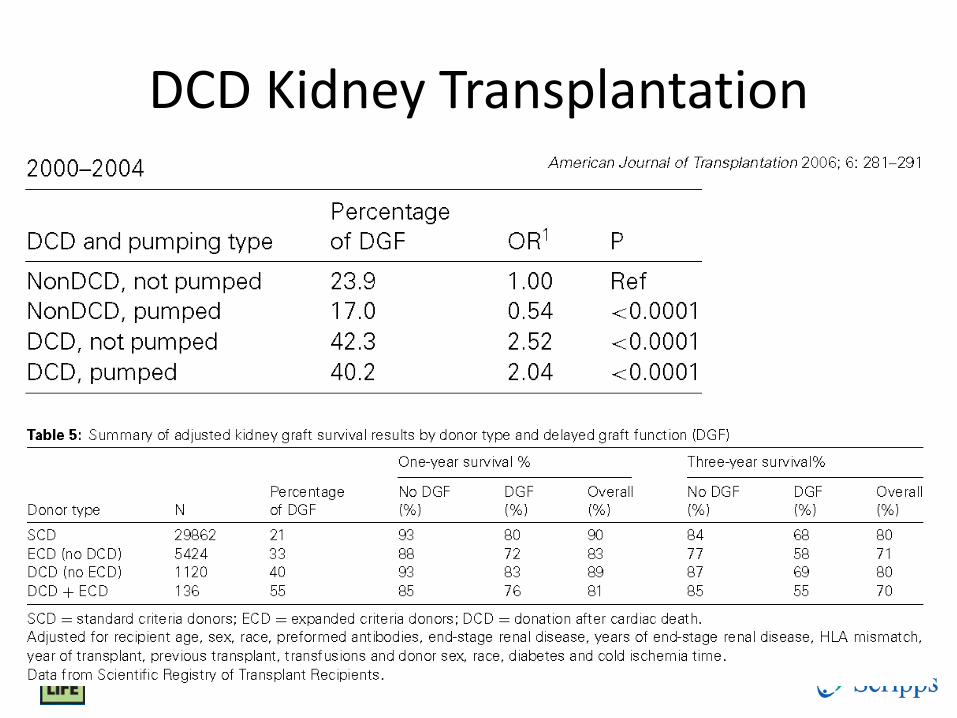
DCD Kidney Transplantation
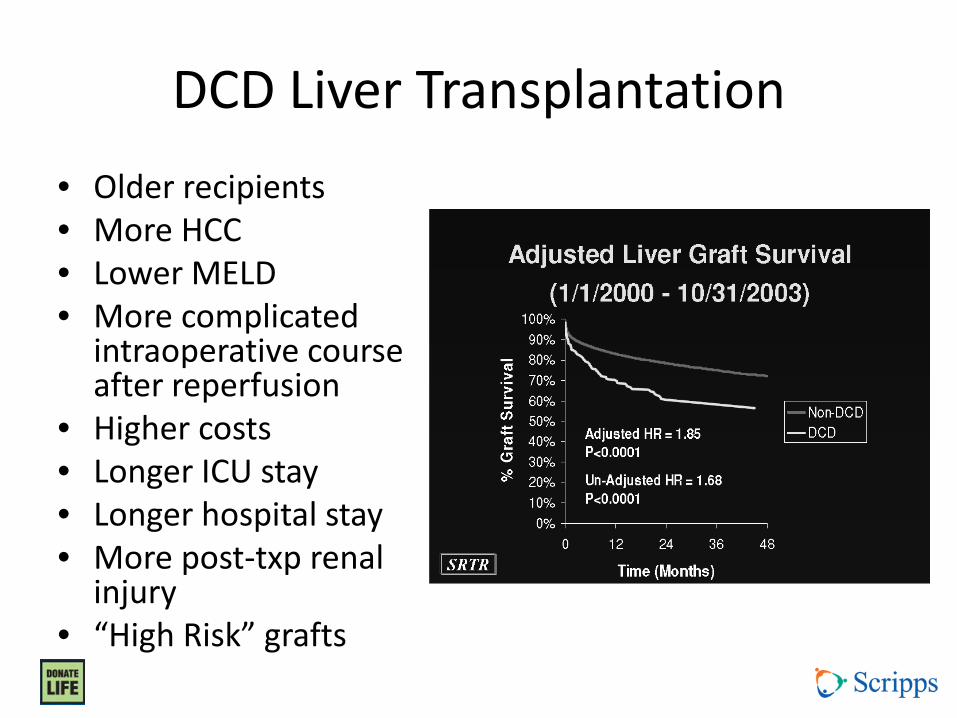
DCD Liver Transplantation • Older recipients • More HCC • Lower MELD • More complicated
intraoperative course after reperfusion
• Higher costs • Longer ICU stay • Longer hospital stay • More post-txp renal
injury • “High Risk” grafts
DCD Liver Transplantation
• Seven UK transplant centers • Recipients of DCD livers have 2x risk of graft
loss and death at 3 years • Results varied across centers
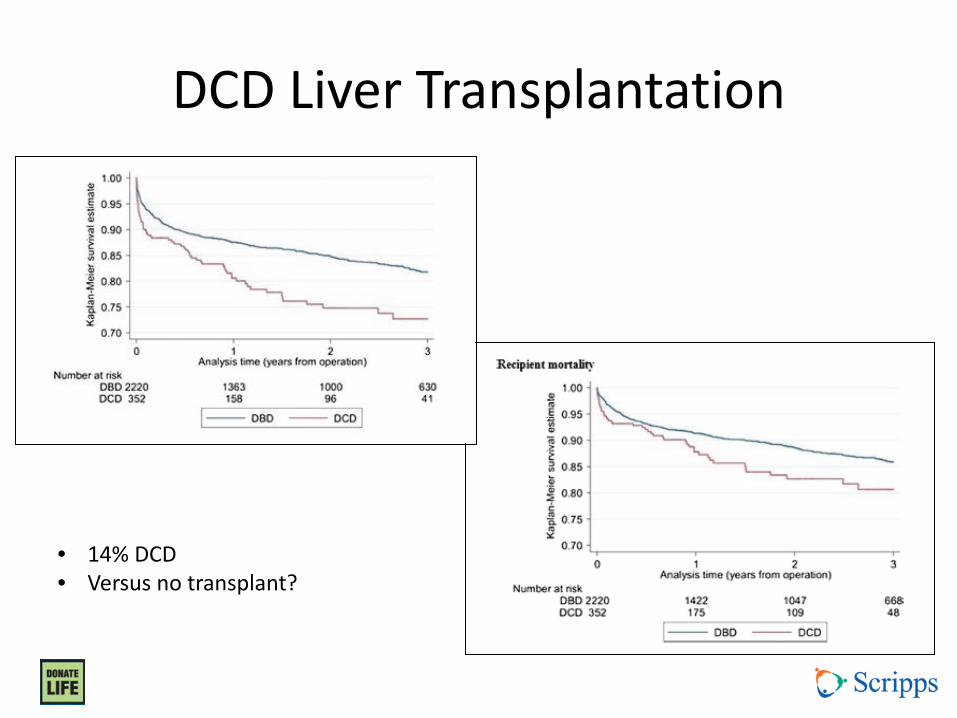
DCD Liver Transplantation
• 14% DCD • Versus no transplant?
DCD Liver Transplantation
• Modelling study – MELD <15 and HCC: greater cost and reduced
effectiveness – MELD 15-20: improved effectiveness but at increased
cost per year of benefit (QALY) – MELD >20: improved effectiveness with less cost/QALY
Potential long-term costs of DCD
• Ischemic cholangiopathy in recipients
• “Lesser graft function” but with low MELD
• Poor quality of life
• No avenue for expedited re-transplantation
• Consequences of regulatory oversight
Defining Success with DCD
• Increase number of organs transplanted?
– Should be additive
• Maintain patient and graft survival rates? – Compared to organs from DBD
– Inferior to equal results
– Compared to not getting transplanted – Better than no transplant in selected populations
Defining Success with DCD
• Increase number of organs transplanted?
– Should be additive (i.e. “expanding the pool”)
• Maintain patient and graft survival rates? – Compared to organs from DBD
– Inferior to equal
– Compared to not getting transplanted – Better than no transplant in selected populations
• The Netherlands experienced over 5 years • a 21% decrease in DBD (159 to 126; -33) • a 129% increase in DCD (41 to 94; +53)
• Not experienced across the US as a whole, but perhaps within certain OPOs—initiating DCD protocols, local/regional healthcare biases
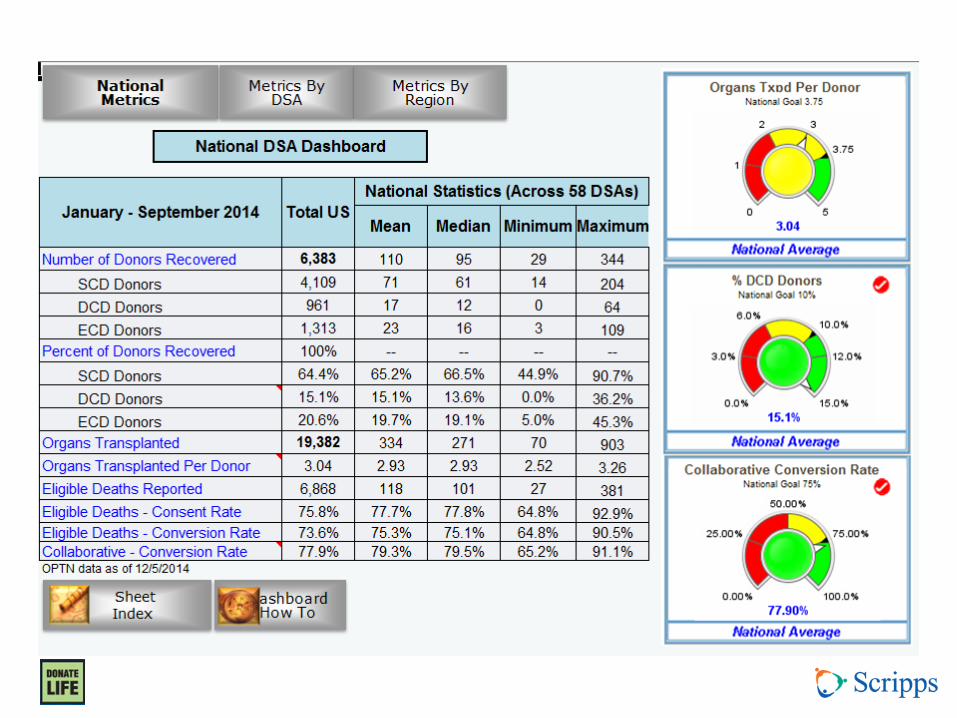
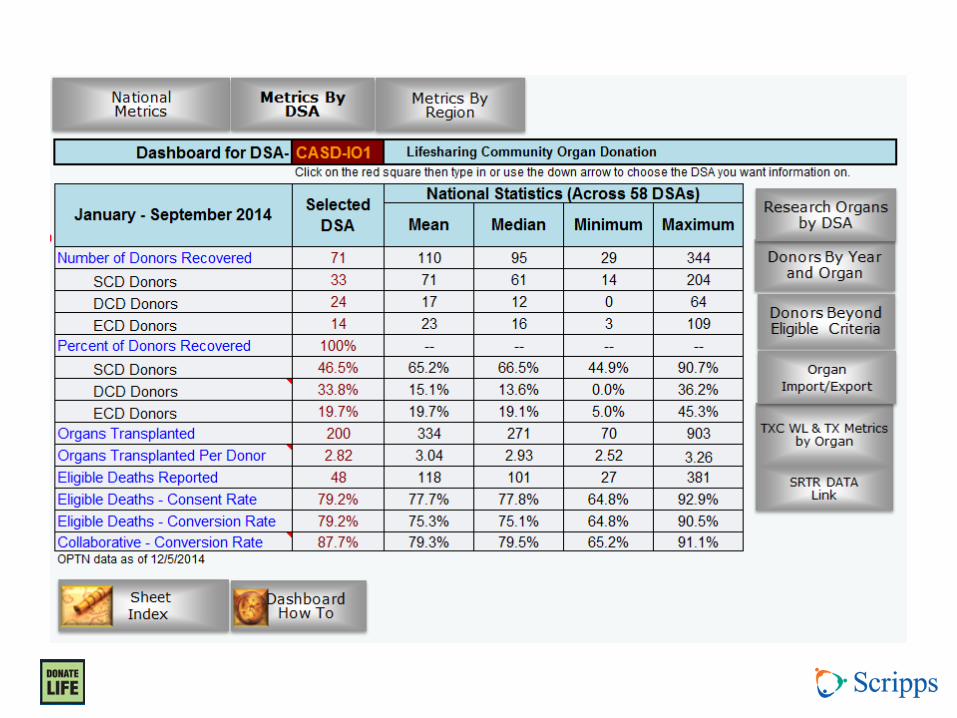
• Number of donors v. Number of organs recovered v. Number of organs/donor
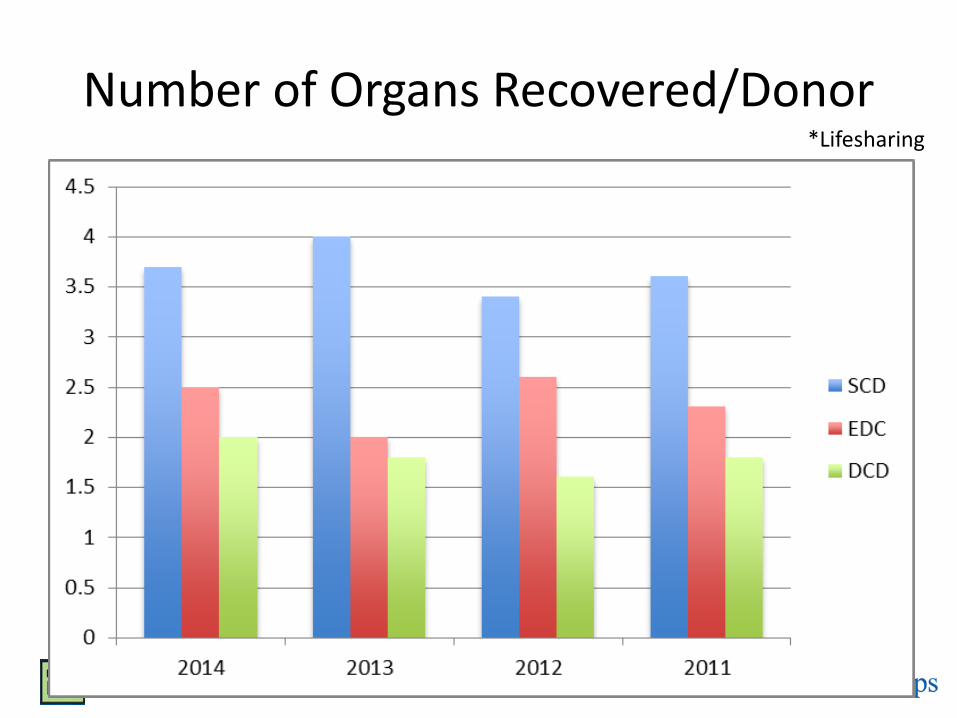
Number of Organs Recovered/Donor *Lifesharing
Pressures to Utilize DCD
• Need for more organs
• Mandated benchmark of 10% DCD donors
• Healthcare economics
Case 1
• 27 year old male, GSW to the head 1 hour ago – Non-survivable injury per Neurosurgery – Hemodynamically stable in ED – Does not currently meet brain death criteria – ICU near capacity
• What do you do? – Recommend early withdrawal of care 2o futility – Transfer to ICU to see if progresses to brain death
Conclusions (from the perspective of a transplant surgeon)
• Both DCD and DBD should be viewed as part of the continuum of end-of-life care
• The DCD organ supply is critical to addressing the ever-growing organ need
• DCD organs may bring added challenges compared to organs from DBD
• DCD should be an alternate pathway for donors who will not reach brain death, not an expedited means of getting to donation
Thank you Questions?







