
www.ias2011.org
Evaluation of point of care CD4 Testing in Ethiopia
Belete Tegbaru
National HIV Laboratory
The Ethiopian Health and Nutrition Research Institute
Addis Ababa, Ethiopia
6th IAS Conference
July 17-20, Rome Italy
www.ias2011.org
Presentation outline
• Background• Problems & questions• Objective• Plan of the evaluation• Methodology• Results• Summary• Expected Benefits of POC instruments• Anticipated Challenges for implementation

www.ias2011.org
233,361
Sites giving ART
Currently on ART
As of end of March 2011
HIV testing sites 2,309
Total Tested (2010/11) 6,592,896[+ve, 80,318 (1.2%)]
Sites giving CD4 testing service
6981. 108 Hospitals 2. 590 HCs
138All Hospitals
In Ethiopia (80 Million Population):

www.ias2011.org
Absence of on time CD4 count results (centralized and
referred)
Service
Lost follow-up
Cold chain system
Cost
Problems & questions
Distance to sites - TAT for results, HIV-DR?
transport ,storage & power interruption
Expertise, maintenance, training, referral linkage
www.ias2011.org
Objective
To evaluate a point-of-care technology (PIMATM) at different level for CD4
testing sites
• PimaTM CD4 + T cell Technology - against standard CD4 instruments
• To see the feasibility: of PIMA for CD4 testing• To see how far PimaTM CD4 + T cell Technology could help the
facilities to reach their patients on time
www.ias2011.org
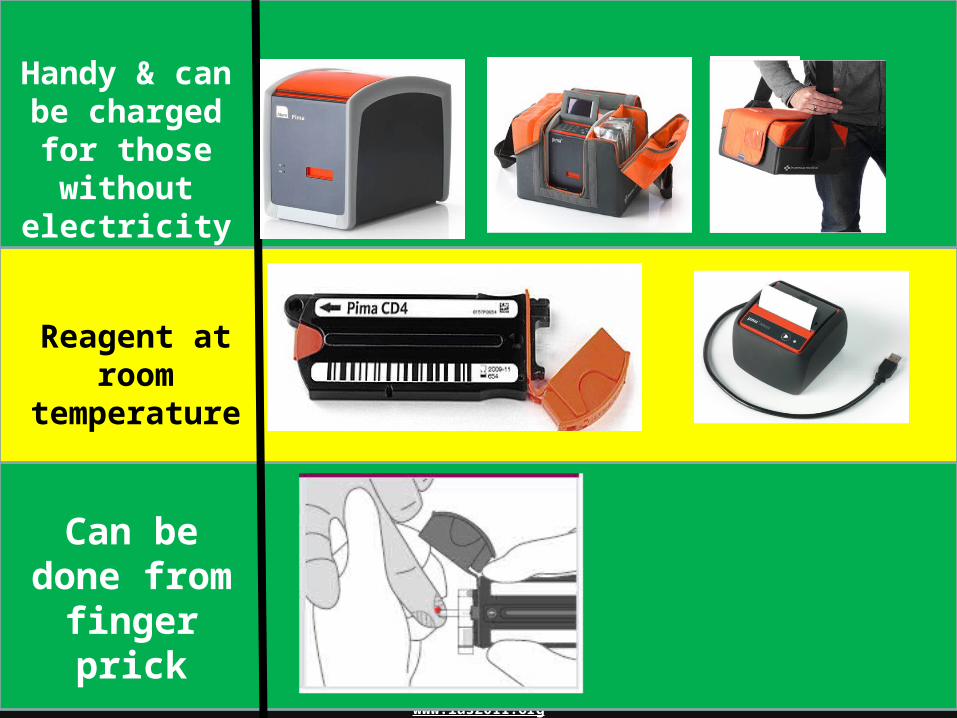
Pima™ from Inverness Medical is a revolutionary point of care analyser. The Pima analyser employs the same static image analysis and counting principles as existing CD4 enumeration technology, in a compact, portable and robust package. Designed equally to suit the needs of the healthcare professional in the field or in the laboratory the Pima analyser is an affordable, effective and valuable tool in the management of HIV patients.1. CD4 count in 20 minutes 2. Battery powered 3. Portable & Robust 4. ‘Walk Away’ testing 5. Embedded software 6. No external calibration 7. On-board data archive
The Pima CD4 cartridge is a unique and breakthrough technology in the enumeration of T-helper cells in whole blood samples. Requiring only 5μL of capillary whole blood and with all test reagents sealed within the disposable cartridge, obtaining a CD4 count is now easier than ever.1. Insertion of the Pima CD4 cartridge into the Pima analyzer
automatically begins the testing process providing you with a direct CD4 measurement in 20 minutes.
2. Capillary whole blood – 5μL 3. No manual sample handling or processing 4. All reagents sealed in disposable cartridge 5. All dried reagents – No refrigeration needed
Handy & can be charged for those without
electricity
Reagent at room temperature
Can be done from
finger prick

www.ias2011.org
Plan of the evaluation
With standard Machines at central & Hospital lab (N=2 sites, 300 samples)
At Health center level; referred samples (n=7 sites, 750 samples) + Finger prick samples (300 samples)
Finger Prick samples(n=10 sites, 500 samples)
Phase-III
Phase-II
Phase-I

www.ias2011.org
Methodology
• Evaluate against standard machines (FACSCalibur and FACSCount)
• Intra-test, inter-test, inter-instrument, interpersonal variations were determined
• Referred samples for FACSCount to referral sites and PIMA on site results were compared
• Operational parameters (failure rate, rate of additional devices for planning and training were evaluated)

www.ias2011.org
ResultsFACSCalibur FACSCount PIMA
Total Samples 316 316 316
Total tested 303 297 306
Mean CD4 (cells/l)
314.9[290.6-339.3]
323.3[298.8-347.8]
317.3[293.2-341.3]
Range 9-997 4-1039 3-970
Failure rateNo result obtained
5(1.7%) 11 (3.7%) 8 (2.6%)
Total cartidges Damaged Retesting
PIMA-Lab 333 12 (3.6%) 15 (4.9%)
PIMA –HCs 140 2(1.4%) 15(10.7%)
Lab: 27(8.1%, 5.4-11.1)Site level: 17(10.7%,7.2-18.7] for planning
9.4% extra devices
www.ias2011.org
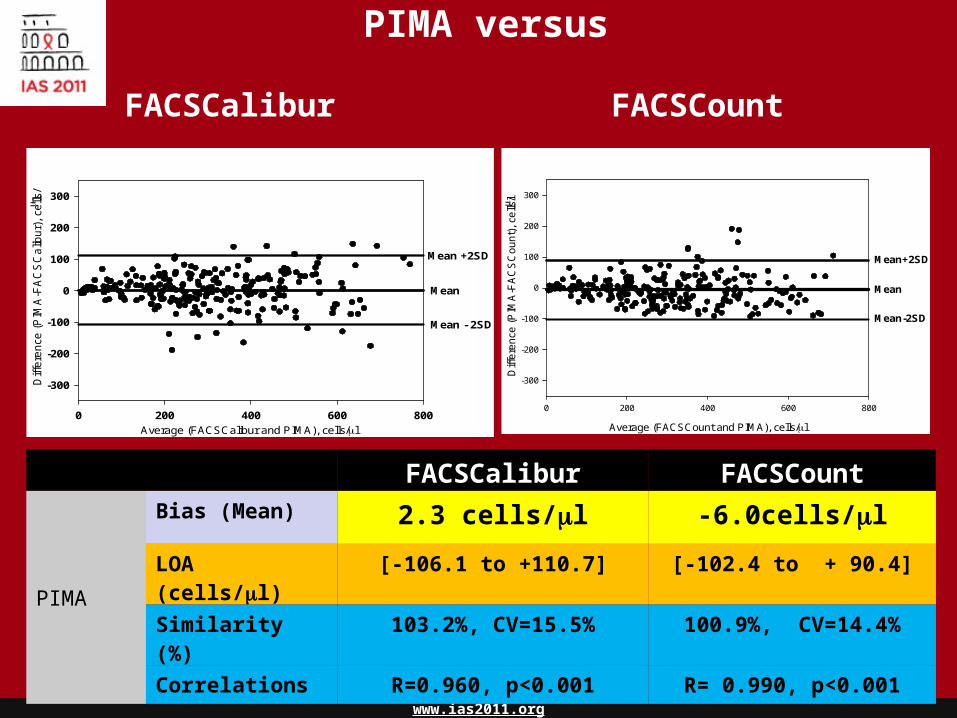
PIMA versus
Average (FACSCalibur and PIMA), cells/l
0 200 400 600 800
Diffe
ren
ce (
PIM
A-F
AC
SC
alib
ur)
, ce
lls/
l
-300
-200
-100
0
100
200
300
Mean +2SD
Mean
Mean - 2SD
Average (FACSCount and PIMA), cells/l
0 200 400 600 800
Diff
ere
nce
(P
IMA
-FA
CS
Co
un
t),
cells
/ l
-300
-200
-100
0
100
200
300
Mean+2SD
Mean
Mean-2SD
FACSCalibur FACSCount
PIMA
Bias (Mean) 2.3 cells/l -6.0cells/l
LOA (cells/l) [-106.1 to +110.7] [-102.4 to + 90.4]
Similarity (%) 103.2%, CV=15.5% 100.9%, CV=14.4%
Correlations R=0.960, p<0.001 R= 0.990, p<0.001
FACSCalibur FACSCount

www.ias2011.org
Number of patients
0 50 100 150 200 250 300
CD
4 T
ce
lls (
Ce
lls
/ l
)
0
200
400
600
800
1000
1200FACSCaliburPIMAFACSCount
Closeness of values
PIMA
0 500 1000 1500 2000 2500
FA
CS
Co
un
t
0
500
1000
1500
2000
2500
3000
CD4 Count (FACSCalibur, cells/l)
0 200 400 600 800 1000 1200 1400
CD
4 C
ou
nt
(PIM
A,
Ce
lls/
l)
0
200
400
600
800
1000
1200
1400
r= 0.960, p<0.001

www.ias2011.org
Parameters At our Lab evaluation(n=306)
Site in AA(n=141)
Within townPIMA Mean 317.3 331191FACSCount mean 323.3 349206Diff -6.0 -18
Similarity (%) 100.9 9810.6
Time to referral center and distance
5-10 min 10-15 Km, 20-30 Min
Period of referral NA 1x/week
TAT of results NA 3-4 days
PIMA versus FACSCount at health centers before and after referral

www.ias2011.org
FACSCalibur FACSCount
Phase-I(Lab based)
Total 9.2% 8.4%Downward 5.7% 6.1%Up-ward 17.3% 14.1%
Phase-II (Clinic based, N=140, Addis Ababa)
Total 1.4%Downward 0.93%Up-ward 3.1%
PIMA Misclassification rate
Taking 200 cells/µl as a cutoff

www.ias2011.org
Variability studies

www.ias2011.org
Sample
Vial-A Vial-B
TECH-A TECH-B
PIMA-1 PIMA-2 PIMA-1
TECH-A
PIMA-1
TECH-A TECH-A
Day-1
Day-2
<200: 103 cells/µl>200: 510 cells/µl
Each test= 10x

www.ias2011.org
Sample
Vial-A Vial-B
TECH-A TECH-B
PIMA-1 PIMA-2 PIMA-1
TECH-A
PIMA-1
Inter machine variation
Day-1

www.ias2011.org
Sample
Vial-A Vial-B
TECH-A TECH-B
PIMA-1 PIMA-2 PIMA-1
TECH-A
PIMA-1
Inter technician variation
Day-1

www.ias2011.org
Sample
Vial-A Vial-B
TECH-A TECH-B
PIMA-1
TECH-A
PIMA-1
Inter-assay variation
Day-1

www.ias2011.org
Sample
Vial-A Vial-B
TECH-A TECH-B
PIMA-1
TECH-A
PIMA-1
Intra-assay variation
Day-1

www.ias2011.org
Sample
Vial-A Vial-B
TECH-A TECH-B
PIMA-1 PIMA-2 PIMA-1
TECH-A
PIMA-1
PIMA-1 PIMA-1Day-2: Daily variation
Day-1
www.ias2011.org
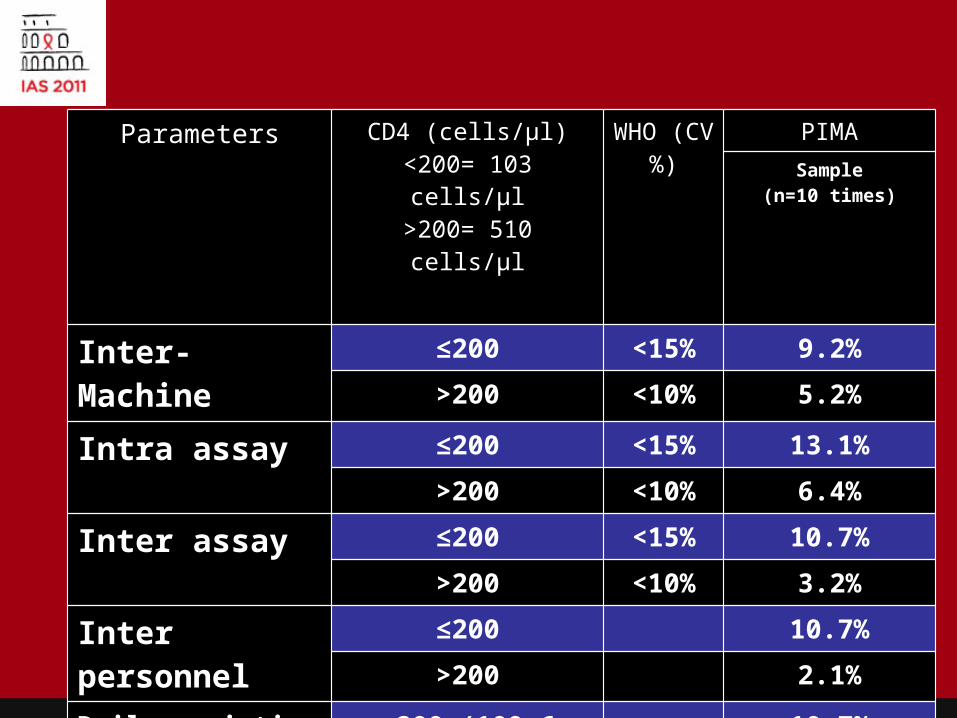
Parameters CD4 (cells/µl)<200= 103 cells/µl>200= 510 cells/µl
WHO (CV%)
PIMASample
(n=10 times)
Inter-Machine ≤200 <15% 9.2%
>200 <10% 5.2%
Intra assay ≤200 <15% 13.1%
>200 <10% 6.4%
Inter assay ≤200 <15% 10.7%
>200 <10% 3.2%
Inter personnel ≤200 10.7%
>200 2.1%
Daily variation (after 16-17 hrs test)
<200 (109.6 cells), P= 0.10
10.7%
>200 (542.1 cells), p=0.52
2.1%

www.ias2011.org
Meaning of Pont-of-care
• In phase-II: 4 HCs tested 255 patients by both PIMA and FACSCount
Results obtained by FACSCount after referral
Total tested Results returned
Lost or no result & need re-draw blood
FACSCount 255 233 12 (4.7%)**
PIMA 255 253 2(0.7%)*
**- drawing of blood for 2nd time due to lost results* Reading failure

www.ias2011.org
Expected Benefits of POC instruments

www.ias2011.org
Patient
Program
Laboratory
• Expansion of sites• Reduce the cost of referral• Reduce the cost of cold chain• Serve the patient on site• Reduce lost follow-up
• Limited training required• Storage (room temp. and space)• Sample collection (easy and safe)• Can be done at lower level
• Get service on site• Initiate ART on time• No cost for transport & others• Follow their status at any time• Increase quality of life

www.ias2011.org
Anticipated Challenges for implementation
• Supply of reagents and machines Vs expansion– Mechanism to solve – connectivity and planning
• Maintenance Vs expansion– Preventive maintenance free-– Technical service replacement strategy
• CD4% for pediatric cases– development

www.ias2011.org
Summary1. Good agreement with standard machines with low bias
and good percentage of similarity
2. On Planning: a total of 9.4% extra devices required at lab & site level
3. Failure rate on testing= 8/306= 2.6% at lab level
4. Gives extra advantage – No need to re-draw blood -point-of-care ~5% of the cases
5. Power interruption was not a problem at site level
6. The intra-, inter-tests are within WHO recommendations for ≤200 and >200 cells/l CD4 Tests

www.ias2011.org
Collaborating Individuals
Dr. Tsehaynesh Mesele EHNRIDr. Almaz Abebe EHNRIMr. Dereje Teshome
EHNRIMr. Ermias Hailu EHNRIMr. Feyissa Challa EHNRIMr Habteyes Hailu EHNRIMrs. Yodit Alemayehu EHNRIKatherine Theiss-Nyland
CHAIDr. Peter Trevor
CHAI

www.ias2011.org
Ethiopian Health and Nutrition Research Institute –Organize and lead the evaluation
CHAI: Financial, material and technical support
Alere: Training of laboratory personnel at the National HIV laboratory

www.ias2011.orgTHANK YOU!







