dr con kolivas staff anaesthetist box hill hospital...
TRANSCRIPT

Anaesthesia for Shoulder Surgery in the Sitting Position
Dr Con KolivasStaff AnaesthetistBox Hill Hospital
Tuesday, 27 May 2008

Introduction
● History● Variations● Physiology● Surgical Features● Advantages● Disadvantages● Technique● Personal Perspective● Conclusions

History
● Open shoulder surgery– Semi-sitting
● Arthroscopic– Lateral– Sitting
● Steep upright

Semi Sitting "Beach chair"

Semi Sitting
● 30-45°– Classic position– Used for open shoulder surgery– Airway access minimal– Physiological disturbance small– Pressure points
● Eyes● Elbows● Wrists
– Securing head– Theoretical Venous Air Embolism

Lateral
●Shoulder arthroscopic surgery– Classic lateral + Finger trap
●Least physiological disturbance●Airway access possible●Pressure points
– Elbows– Knees– Axillae
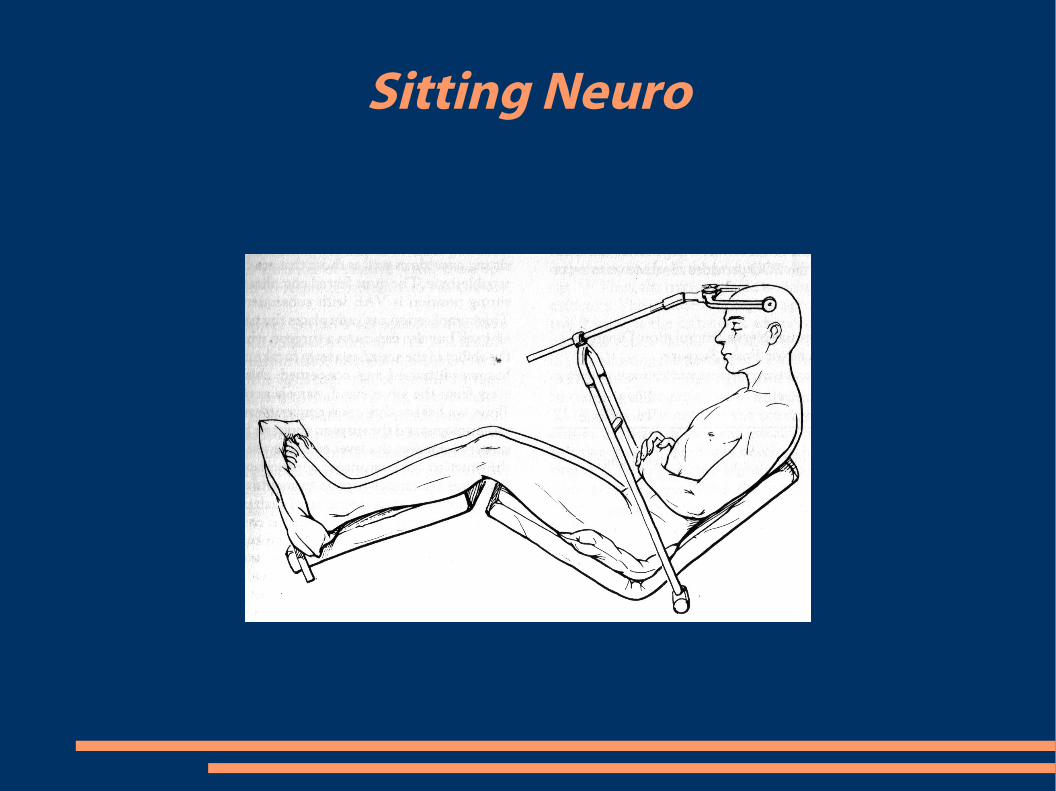
Sitting Neuro

Sitting
● Evolution of semi-sitting● Steep upright 80° more than neuro● Dedicated operating table “Spyder”● Physiological disturbance greatest● Pressure points
– Elbows– Wrists– Eyes– Sciatic n.
● Head securing● Airway Access

Sitting

Physiology
● GRAVITY– Exaggerated position cf neurosurgery– 30 cm between heart->head
● 1.3mmHg per cm water● Relative cerebral hypoperfusion
– Stroke risk?● Venous return
– Bezold-Jarish Reflex– Vaso-vagal in awake
● Blunted sympathetic nervous system response of anaesthesia
● Venous Air Embolism● PAE with PFO (Right to Left Shunt)● Airway Obstruction● Risk of Venous obstruction causing significant decrease
in CPP

Physiology 2
● Relative Contraindications to neurosurgical sitting position
● Cerebral ischaemia upright awake● Minor
– ?Cardiac instability– ?Age extremes
● Ventriculoatrial shunt in place and open● Left Atrial Pressure < right atrial pressure● Platypnoea-orthodeoxia● Preoperative demonstration of patent foramen ovale or
right-to-left shunt● Little relevance to shoulder surgery struck
through

Surgical Features
● Axillary plexus damage in lateral position– Predates finger trap
● Surgical Exposure– Arm positioning
● Less tissue retraction and damage– Arthroscopy relevance?
● Less bleeding– More hypotension?

Anaesthesia advantages 1
● Better respiratory function?

Anaesthesia advantages 2

Anaesthesia advantages 3

Anaesthesia advantages
● Respiratory function● Less bleeding● Less cranial n. damage● Head security with spyder● Pressure care● Challenge?
Anaesthesia Disadvantages
● Haemodynamic– Hypotension routine– Bradycardia 25-40%– Arrhythmias Rare– Venous Air Embolism
● No reported cases● Cerebrovascular
– Hypoperfusion● Correlation with BIS
– Paradoxical Air Embolism● Not reported

Disadvantages 2
● Airway– Access– Obstruction– Securing
● Positioning– Complexity– Pressure points
● Eyes● Elbows● Wrists● Buttocks

Technique
● Regional vs General– Regional Blockade
● Usual Generic Regional concerns● Interscalene block
– High success rate– Usually misses small section of innervation– Unpleasant surgical procedure requiring sedation
● Cardiovascular complications– Blunted but not ablated– Hypotension uncommon– Bradycardia 25%– Sedation blunts compensation further

Technique 2
● General Anaesthesia– Usual Generic issues with GA– Cardiovascular complications more common
● Hypotension almost routine● Bradycardia more common● Reflexes further blunted● Regional blockade abolishes any sympathetic response
exaggerating CVS issues

Technique 3
● Extra Management– Pre-op
● Patient suitability● ?Consent issues● Large bore IV access● Arterial Line● Regional Block if desired● Vasopressors prepared● TED stockings

Technique 4
● Monitoring– Routine + – Arterial Line– BIS– ?ECG 5 lead– Theoretical:
● Brain ischaemia monitoring● Doppler Ultrasound● Trans-Oesophageal Echo● Pulmonary Artery Catheter● Neck Tourniquet● Emergency practice drill

Technique 5
● Induction/Technique– Relaxant– ETT– Controlled Ventilation– Achieve haemodynamic stability in supine position
before sitting– Fluid loading
Technique 6
● Maintenance– ? Preemptive anticholinergics– Move arterial transducer with head position– Raise position incrementally– Adjust vasopressor as required– Observe pressure care

Personal Perspective
● Regional + General– Teaching opportunity– Reliability– Patient/Anaesthetist/Surgeon satisfaction– Trainees may go on to perform procedure under
regional once they master the block– Haemodynamic consequences of General are
greatest post induction, so avoiding block to rely on painful stimulus for BP is unhelpful.
– Single shot blockade covers vast majority of pain of the first day which is mostly due to capsular distension, then oral analgaesia satisfactory.
Personal Perspective 2
● Pre-op– Consent issue is impossible to tackle?– Full length TED stockings
● Note venous congestion– 16g IV access– No fluid loading (TED stockings and vasopressor fill
vessels and diuresis post-op common).– Premed with midazolam 40µg/kg– Interscalene block
● Reverse trendelenburg (Venous congestion)● Single shot● n. stimulator >0.2mA <0.4mA +/- Ultrasound guidance● 30ml 0.75% levobupivacaine● 75µg clonidine (note hypotensive effect)● Block lasts 16-20 hours

Personal 3
● Induction– Fentanyl 3µg/kg– Propofol 1mg/kg– Rocuronium 0.6mg/kg
● Maintenance– Air/Oxygen FiO2 0.8– Desflurane– BIS monitoring

Personal 4
● Positioning– Preempt with 0.2mg Glycopyrrolate– Start phenylephrine with induction
● 5mg/hour and titrate to effect● Use mean BP as endpoint and keep >= 75% of pre-
induction value– Move arterial transducer to ear level
● Adjust vasopressor to maintain BP minimum of 10mmHg below acceptable heart level pressures (50-150 in non-hypertensive patient).
– Elevate legs– Elevate head till 45 degrees then reassess
● Most data supports no BP changes <=45 degrees– Usually adjusting BP prior to elevation smooths
transition

Personal 5
● BIS monitor– Valuable added information– Minimise anaesthetic depth safely thereby
minimising vasopressor requirement.– Indirect monitor of perfusion
● Falls to zero when brain profoundly hypoperfused.

Pictures

Pictures 2

Pictures 3

Pictures 4

Pictures 5

Conclusions
● Risk transferred from surgical positioning to one of Anaesthesia monitoring
● Can be safely conducted with significant extra effort
● Worldwide experience confirms relative safety● Worldwide experience also confirms relative
danger when conducted without deference to physiological issues
● Familiarity with position is paramount to safety● Communication and not surprise

Conclusions 2
● Outstanding concerns– How do we consent for the relative risk of a
position?– What don't we know or can't quantify?
● Cardiovascular risk– Vasopressor use– Fluid challenges
● Cerebrovascular risk– Subtle neurological deficits
– What constitutes a contrainidication?– How would you have your shoulder operated on?