dr fatimah @ hartina hussin radiologist queen elizabeth ...hqe.moh.gov.my/radiologi/16. imaging of...
TRANSCRIPT

DR FATIMAH @ HARTINA HUSSIN
RADIOLOGIST
QUEEN ELIZABETH HOSPITAL
6/9/2015 KURSUS "UPDATE IN RADIOGRAPHY 2015" BAGI JURU X-
RAY KKM NEGERI SABAH & SARAWAK 8-9 JUNE 2015 1

Introduction
Prevalence of malignant renal tumours
in general population is about 0.07%
according to the American Cancer
Society.
Renal cell carcinoma (RCC) being the
most common, which accounts for
approximately 3% of adult malignancies.
The incidence of RCC is increasing at
an annual rate of approximately 2% [1]
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015" BAGI JURU X-RAY KKM
NEGERI SABAH & SARAWAK 8-9 JUNE 2015 2
Clinical presentation
Renal masses are now commonly found
as incidental lesions on imaging studies
done for other indications.
Haematuria-microscopic or gross
Loin pain with microscopic haematuria
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 3
Types of renal tumours
Cystic
Simple cyst
Complex cyst
Solid tumours
Angiomyolipoma (AML)
Adenoma
Transitional cell carcinoma
(TCC)
Renal cell carcinoma(RCC)
Oncocytoma
Metastasis
Wilm’s tumour (pediatrics)
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 4
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 5
Role of imaging
Renal tumor characteristics: Such features include size, location, gross
morphology, fat content, degree of vascularity (generally relative to the surrounding normal renal parenchyma),
nature of vascularity (i.e. rate that contrast is taken up and eliminated from the tumor),
Staging of disease – involvement of other structures e.g renal vein thrombosis IVC RA involvement, Gerota’s fascia etc.
Distant metastases-lymphadenopathy, lung, liver or bony metastases
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 6
Menu for imaging tests for renal
masses : IVU-
limited sensitivity for small renal masses
only 67% for RCC less than 3cm
Ultrasound kidneys reliable in identifying renal cysts
Multiphase renal CT Currently the gold standard for renal mass
evaluation
MRI kidney Patient with contrast allergy or impaired renal
function
Hyperdense renal cyst
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 7
Renal Ultrasound
Pro cons
Cheap , cost effective
Readily available
Free form ionizing radiation
No IV contrast
administration
The strength of
ultrasonography is its ability
to differentiate solid versus
cystic renal structures
Operator dependent
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 8

Ultrasound kidney Cystic lesion
Solid lesion
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 9
angiomyolipoma Simple cyst
Complex cyst Solid mass
Advances in ultrasound
Contrast enhanced ultrasound kidney
Ultrasound contrast agents (gas filled microbubbles covered by a stabilizing shell) are injected intravenously as liquids, and then manifest as a gas when in the bloodstream.
Therefore it will improves the detection of Doppler signals and helps better reveal both normal and abnormal vascularity.
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 10
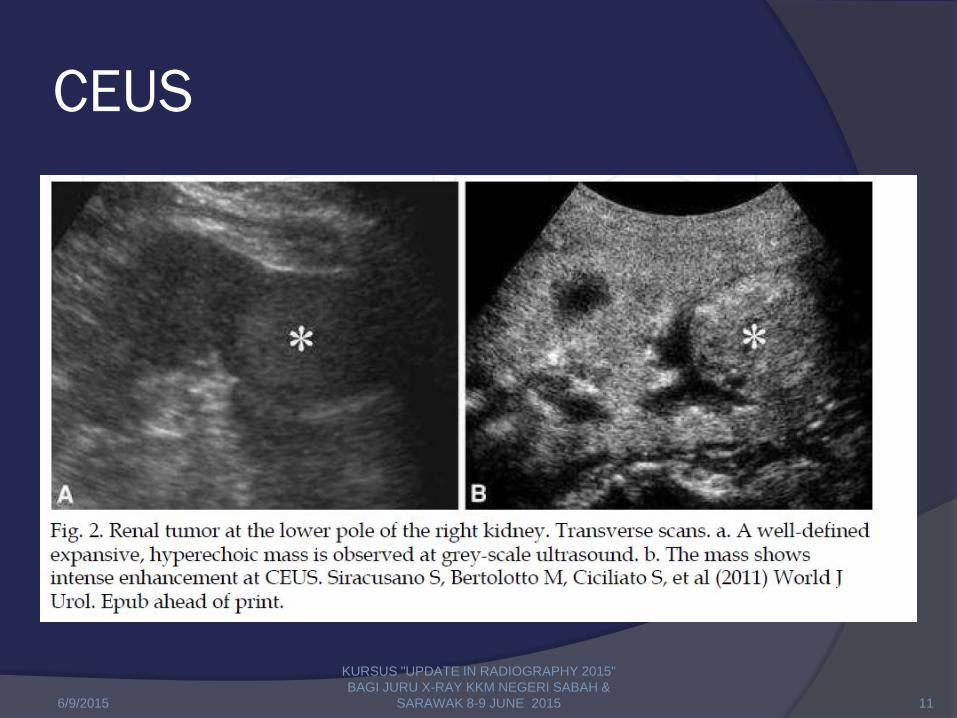
CEUS
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 11
Computed tomography (CT) pros Cons
Excellent anatomic detail for retroperitoneal structures.
Can be as well used to stage the disease
Non operator dependent
Used as primary investigation tool for suspicious renal masses
Multiplanar reconstruction for more advanced CT machines
Ionizing radiation
IV contrast
administration
More expansive
Not readily available
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 12
CT scan
Distinct phases have been clearly
identified for patients undergoing
intravenous contrast enhanced renal
imaging.
Multiphase renal CT (Standard four-
phase) has been recommended and
widely used in many clinical centers for
detection and staging of renal tumors
[2–4].
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 13
MULTIPHASE RENAL CT
It includes:
Arterial phase :15-25 s
corticomedullary phase (CMP): 25-70s
Nephrographic phase:80 -120 sec
Excretory phase (EP): 180s at post
intravenous (iv) contrast
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 14
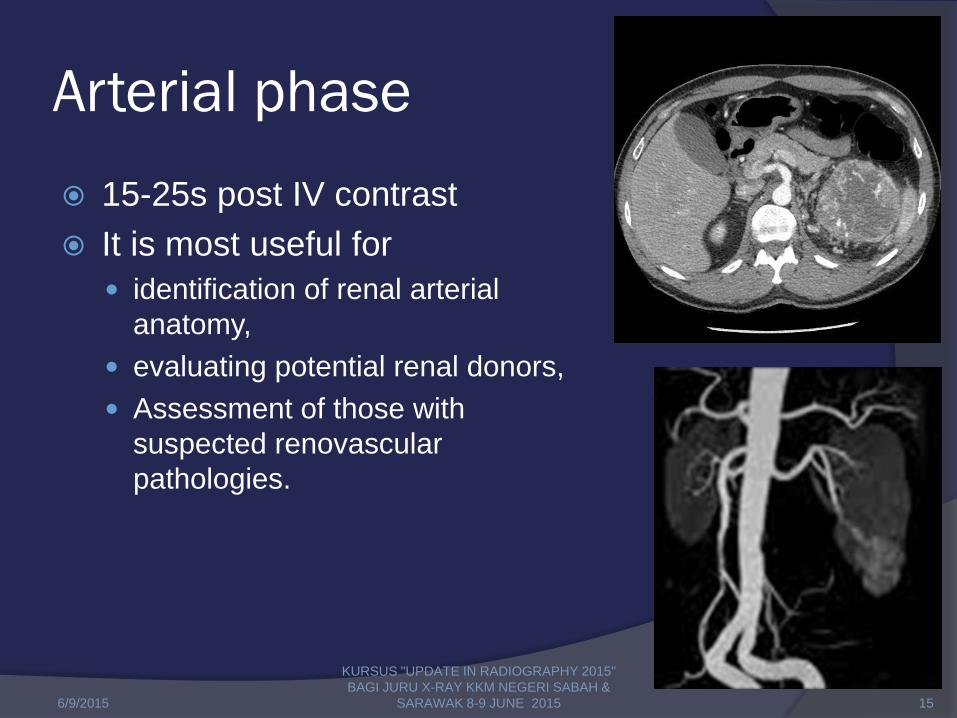
Arterial phase
15-25s post IV contrast
It is most useful for
identification of renal arterial
anatomy,
evaluating potential renal donors,
Assessment of those with
suspected renovascular
pathologies.
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 15
Corticomedullary phase (CMP)
25-70 seconds after injection.
During this phase the renal cortex has intense enhancement, as glomerular filtration of the contrast material begins to take place.
This phase is useful for the identification of hypervascular renal tumors, notably clear cell renal cell carcinomas.
The renal veins can also be seen well
during this phase.
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 16
Nephrogenic phase (NP)
80-120s after contrast
During this phase contrast has been
filtered through the glomeruli and has
made its way to the collecting ducts.
During this phase the renal parenchyma
appears homogenous.
It is at this time that subtle renal
parenchymal masses are best detected.
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 17
Excretory phase (EP)
180s after contrast administration.
During this phase the renal calyces,
pelvis, and ureters are opacified.
Further delayed imaging may be
necessary to ensure that all portions of
the ureter have been opacified.
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 18
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 19
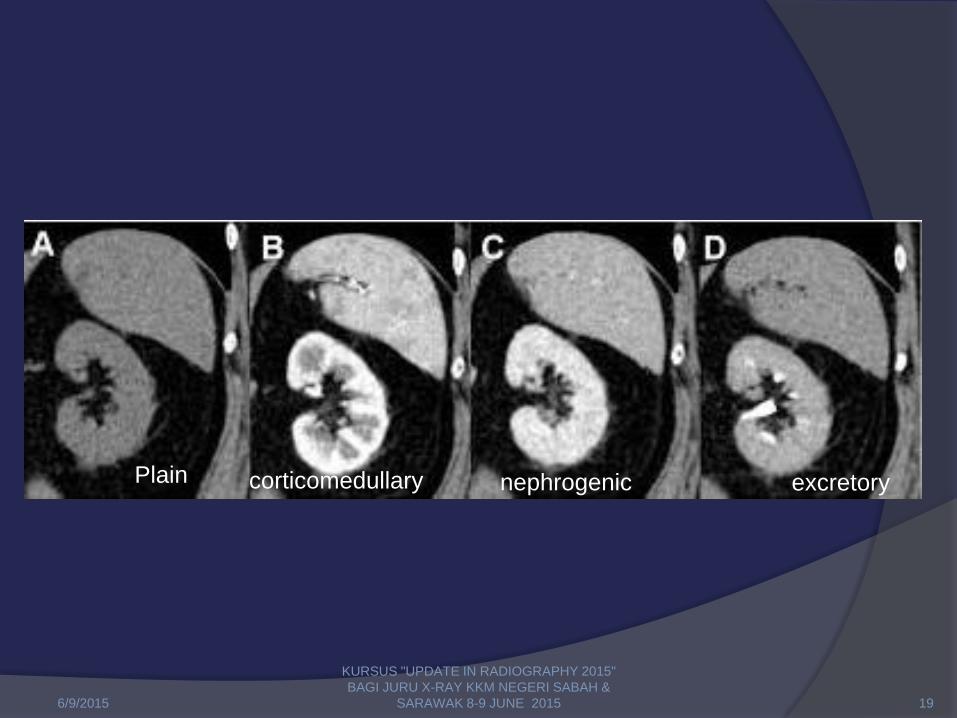
Plain corticomedullary nephrogenic excretory
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 20

In QEH Multiphase renal CT includes :
Pre contrast – diaphragm to symphysis pubis (SP)
Arterial phase : ○ 20-30s post contrast
○ ( Kidney areas only )
○ usually covers the corticomedullary phase
Venous phase: ○ 50-60s
○ (diaphragm to sp)
○ usually covers the nephrographic phase
Delayed phase : ○ 5 minutes
○ (diaphragm to sp)
○ usually cover the delayed phase including the ureters and bladder
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 21

4 PHASE CT KUB
6/9/2015 22
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015
PLAIN
ARTERIAL PHASE
VENOUS PHASE
DELAYED PHASE

MRI
MR of the kidneys is generally performed on 1.5 or 3 Tesla magnets.
The standard sequences (evaluation of a renal mass) include : T1WI imaging (in and out of phase sequences),
T2WI images in two planes,
T1WI FS before contrast administration
Multiphase T1FS post contrast at : ○ arterial,
○ corticomedullary,
○ nephrographic,
○ urographic phases.
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 23
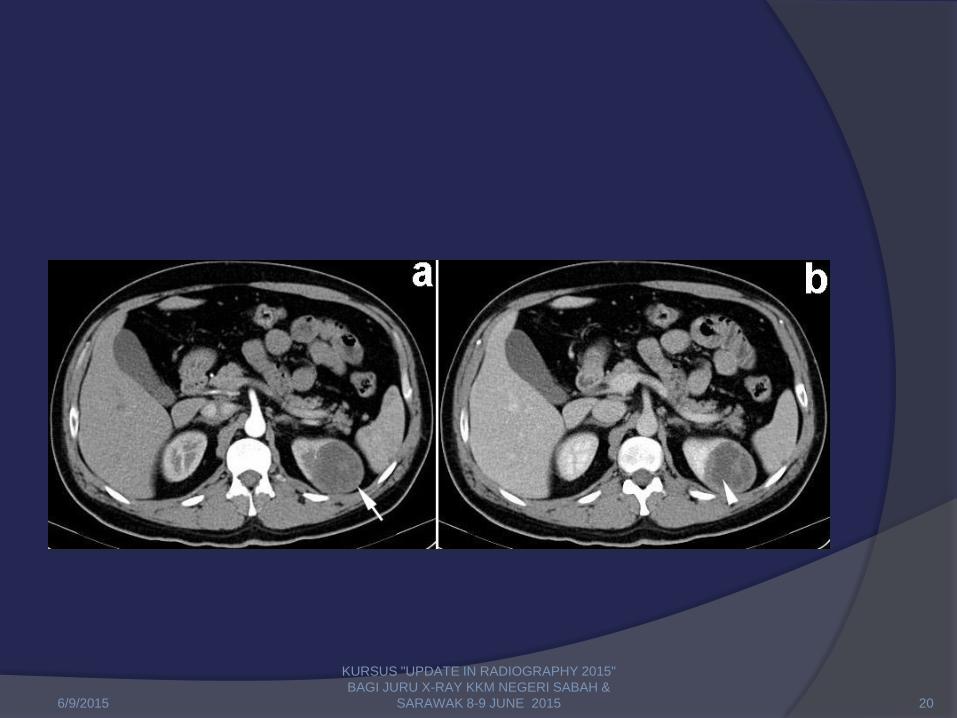
MRI substraction technique
Subtracting pre contrast image from post contrast
images.
This technique aids in detection of enhancement.
In such analyses, areas of high signal appear
only in areas of enhancement. Kang SK, Kim D, and Chandara H.
(2011). Contemporary imaging of the renal mass. Cur Urol Rep; 12:11-17.[148]
In a comparison, for identification of renal
malignancy subtraction imaging was more
sensitive (99%) when compared to
quantitative (quantitative enhancement ratio
calculation) evaluation (95%). EM, Israel GM, Krinsky GA, et al.
(2004). Renal Masses: Quantitative Analysis of enhancement with signal intensity measurements
versus qualitative analysis ofenhancement with imag]
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 24
Advances in MRI
DWI
○ Malignant masses appear to have lower
○ ADC than benign ones.
○ This is thought to be due to the high
cellularity/complex architecture of neoplastic
lesions.
Taouli B, Thakur RK, Mannelli L, et al. (2009). Renal lesions: characterization with diffusion-weighted imaging versus
contrast enhanced contrast enhanced MR imaging. Radiology, 251:398–407.
Zhang J, Tehrani YM, Wang L, et al. (2008). Renal masses: characterization with diffusion-weighted MR Imaging: a
preliminary experience. Radiology, 247:458–464.
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 25
Higher Fuhrman grade of RCC have
lower ADC than lower grade lesions.
Solid vs cystic lesion on DWI:
solid lesions have very low ADC, whereas
cysts have higher ADC, Bosniak type 1 cysts
had the highest ADC.
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 26
Nuclear Imaging
The general premise of nuclear imaging
involves the administration of radionuclide
labeled molecules for a specific purpose for
assessment of both physiologic and
anatomic details that is not obtainable with
other radiologic imaging modalities.
Nuclear imaging is more often used to
assess extent of disease rather than the
specific characteristics of primary renal
tumor.
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 27
Sestamibi Scan
Evidently retained in mitochondria, with
reported increased uptake in
oncocytomas compared with RCC, AML,
and renal cysts.
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 28
Conclusion
Renal tumours are commonly found as an incendental findings during abdominal scan.
Ultrasound is better in distinguishing cystic form solid lesion.
Multiphase renal CT is commonly used to evaluate complex cysts (Bosniak 3-4 lesions) and currently is the gold standard.
MRI has growing role in imaging of renal tumours due to its better soft tissue resolution although it is more scanning time and long waiting list.
6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 29

6/9/2015
KURSUS "UPDATE IN RADIOGRAPHY 2015"
BAGI JURU X-RAY KKM NEGERI SABAH &
SARAWAK 8-9 JUNE 2015 30