dr. pamela leventis consultant rheumatologist epsom & st. helier nhs trust gout
TRANSCRIPT
Dr. Pamela Leventis
Consultant Rheumatologist
Epsom & St. Helier NHS Trust
Gout
A disease of Kings
GOUT – Outline
EpidemiologyDiagnostic difficultiesManagement (EULAR/BSR guidelines)Gout – Top tips
EpidemiologyCommonest Inflammatory Arthritis in men
Mean UK prevalence – 1.4%
Prevalence increases with age
>7% of men >75 yrs, >4% of women >75 yrs (Mikuls et al., 2005)
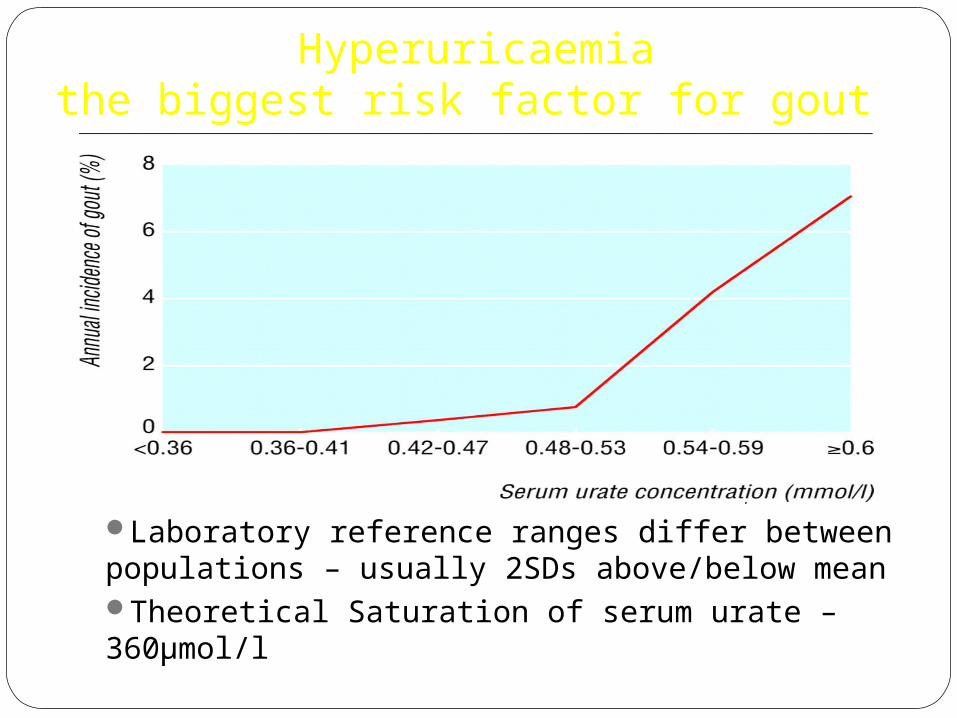
Hyperuricaemiathe biggest risk factor for gout
Underwood M BMJ 2006;332:1315-1319
Laboratory reference ranges differ between populations – usually 2SDs above/below meanTheoretical Saturation of serum urate – 360μmol/l
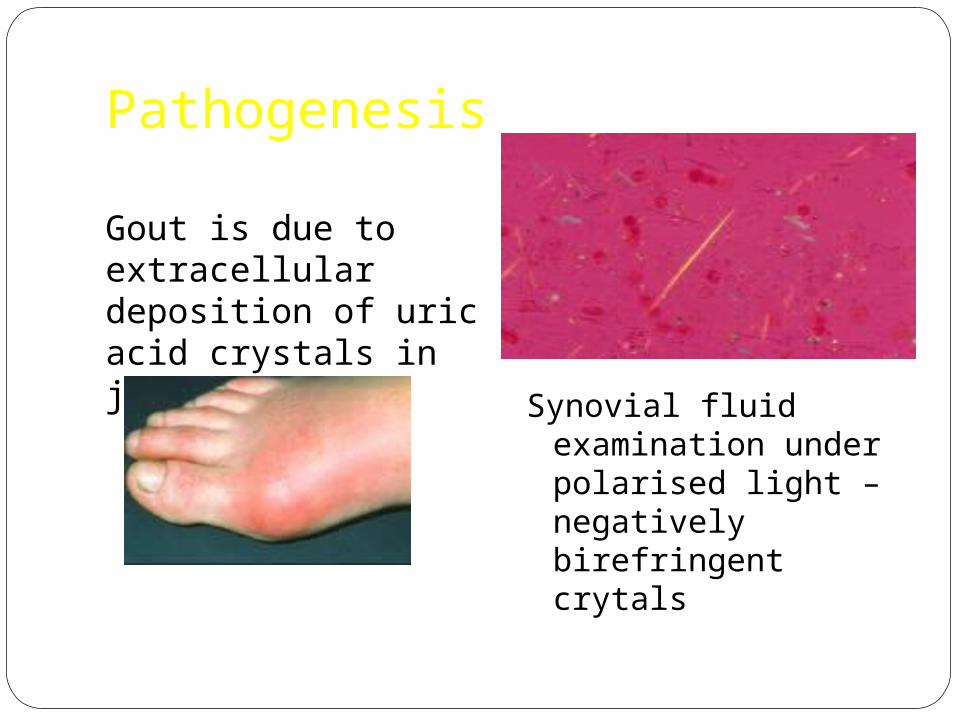
Pathogenesis
Gout is due to extracellular deposition of uric acid crystals in joints
Synovial fluid examination under polarised light – negatively birefringent crytals
Gout Diagnosis
A first hand descriptionThe victim goes to bed and sleeps in good health. About 2 o'clock in the morning, he is awakened by a severe pain in the great toe; more rarely in the heel, ankle or instep. This pain is like that of a dislocation, and yet the parts feel as if cold water were poured over them. Then follows chills and shiver and a little fever. The pain which at first moderate becomes more intense. With its intensity the chills and shivers increase. After a time this comes to a full height, accommodating itself to the bones and ligaments of the tarsus and metatarsus. Now it is a violent stretching and tearing of the ligaments-- now it is a gnawing pain and now a pressure and tightening. So exquisite and lively meanwhile is the feeling of the part affected, that it cannot bear the weight of bedclothes nor the jar of a person walking in the room.
Thomas Sydenham 1683
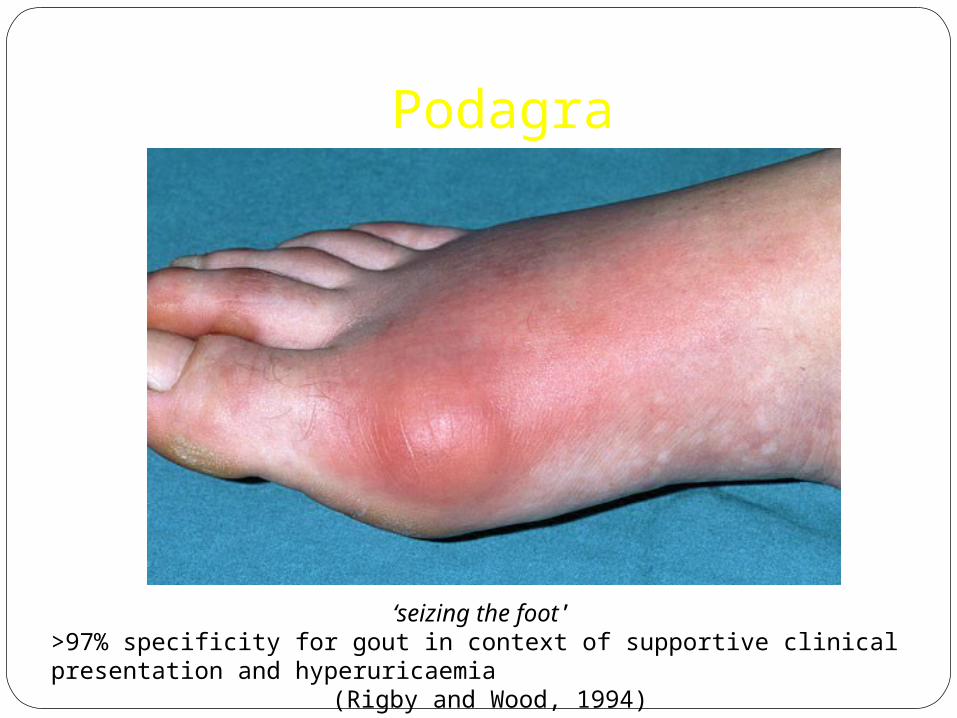
Podagra
‘seizing the foot’ >97% specificity for gout in context of supportive clinical presentation and hyperuricaemia
(Rigby and Wood, 1994)

Why can gout be difficult to diagnose?
Atypical Joint/tendon/bursa
involvement
Pre-existing joint pathology
Gout- a great mimic
Roddy E, Doherty M. Gout. In: Warburton L (ed). Musculoskeletal disorders in primary care. London: RCGP. In press 2011.Roddy E. (2011) Arthritis Research UK

Gout or Septic Arthritis?

Gout or Cellulitis?
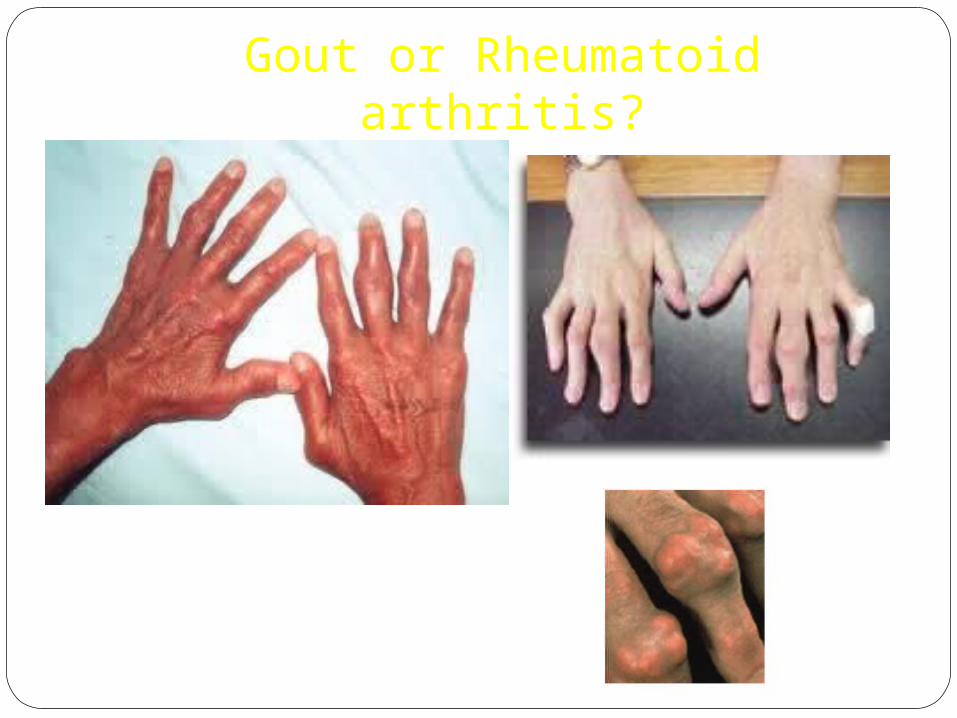
Gout or Rheumatoid arthritis?
Diagnostic ambiguity
Gout flare can be associated withNormal Serum urate (~10%)
?serum urate lowered during acute phase response (Urano et al., 2002)Gout triggered by drop in serum urate
Mild LeucocytosisLow grade feverNormal X-ray
Synovial fluid examination 63-78% sensitivity – degree of operator dependence/sample
quality (Swan et al., 2002)Crystals may co-exist with sepsis (case series 30 patients – Yu et
al. (2003))
Gout Management
Goals of Therapy
1. Minimise morbidity of acute flare
2. Prevent future flares, and thereby prevent joint damage and disability
Patient Education and Lifestyle changes Pharmacological Prophylaxis if indicated
ManagementAcute Gouty Flare
BSR Guidelines (Jordan et al., 2007)1st line
Full dose NSAID continued for 1-2 weeks – unless contraindication
If risk of peptic ulcer disease – co-prescribe Proton pump inhibitorAlternatively
Colchicine 500μg bd-qds (higher dosing associated with disproportionate toxicity)
Intra-articular corticosteroid injection for monoarticular flareOral prednisolone for severe/polyarticular flare
Urate lowering therapies should not be commenced or stopped during acute gout
ManagementLong term ProphylaxisNon – pharmacological
Diet (www.ukgoutsociety.org)Alcohol < 21 U/wk ♂, <14 U/wk ♀Obesity – aim for ideal BMIExerciseSmokingStrong association between gout and the metabolic syndrome
(Choi et al., 2007)Annual Screen- BP/Weight/fasting lipid profile/glucose
ManagementLong term Prophylaxis - Pharmacological
When to initiate urate lowering therapies?EULAR/BSR Guidelines
Uniform agreement for prompt treatment in:Severe gout with X-ray changesTophaceous depositsChronic kidney diseaseNephrolithiasisUrinary uric acid excretion exceeding 1100 mg/day (6.5 mmol)
Otherwise shared decision with patient re: risks/benefits of treatment/no treatment
BSR guidelines suggest initiation of treatment if ≥ 1 further attack within 12 months
ManagementLong term Prophylaxis - Pharmacological
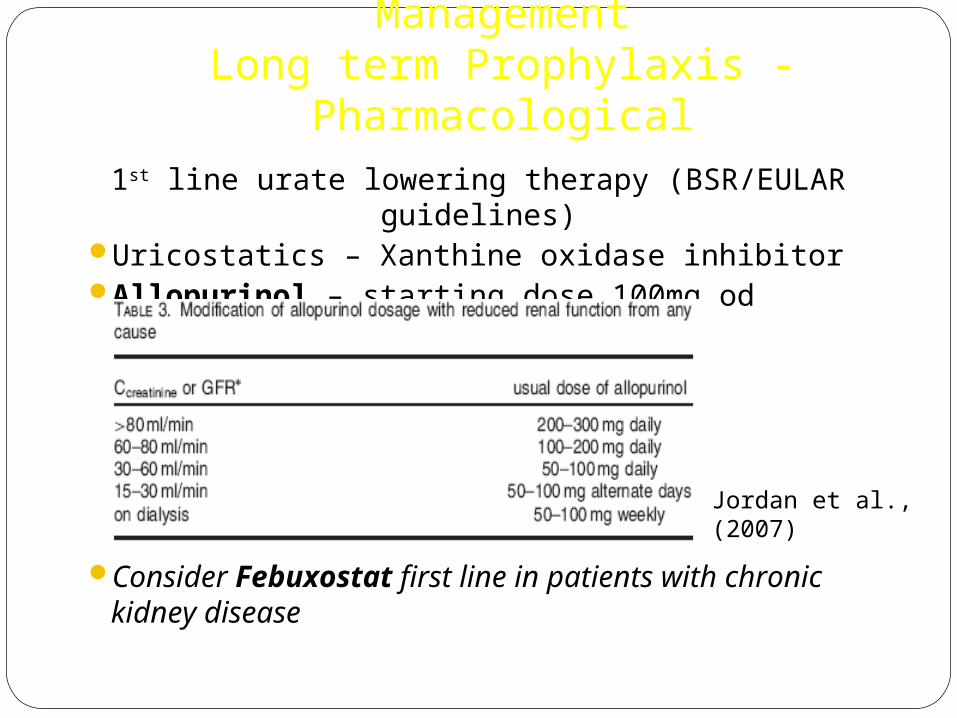
1st line urate lowering therapy (BSR/EULAR guidelines)Uricostatics – Xanthine oxidase inhibitorAllopurinol – starting dose 100mg od
Consider Febuxostat first line in patients with chronic kidney disease
Jordan et al., (2007)
ManagementLong term Prophylaxis - Pharmacological
Aim for plasma urate<300μmol/l (BSR guidelines)
median [urate] for men in UK<360 μmol/l (EULAR guidelines)
saturation point serum urate
Commence at least 2 weeks following resolution of acute attack
Consider low dose colchicine – 500μg od/bd for up to 6 months following initiation77% patients flare within 6 months of initiating allopurinol
(Borstad et al. 2004)
Allopurinol dosingIncrease every 2-4 weeks by 100mg until target
serum urate achieved. Maximum 900mg/day.
Start low – go slow approach recommended To reduce likelihood of triggering attackTo minimise risk of toxicity (AHS)Emphasis on target value
Allopurinol Hypersensitivity Syndrome1:300 patientsAt risk groups: Elderly and Renal Impairment
Erythematous desquamating rashFeverHepatitisEosinophiliaWorsening renal function
20% mortality (Lee et al., 2008)
ManagementLong term Prophylaxis - Pharmacological
2nd line – failure to reach target serum urate If normal renal function
uricosuric (Contraindicated if history of nephrolithiasis)Sulphinpyrazone - 200-800mg/dayProbenecid – named patient basisBenzbromarone if mild – moderate renal impairment (GFR 30-
60ml/min) – named patient basis
Or combination therapyLosartan and Fenofibrate – weak uricosurics
ManagementLong term Prophylaxis - Pharmacological
Febuxostat currently approved by NICE if:adverse effects on allopurinol OR further dose escalation contra-indicated with suboptimal
serum uratemost common side effects
diarrhoea, nausea, headache, abnormal LFTs, rash
Renal Uric acid Excretion
Urinary uric acid:creatinine ratio to diagnose over excretors
Should be determined in :Young patients diagnosed with gout <25 yrsPatients with a family history of young onset goutPatients with renal calculi
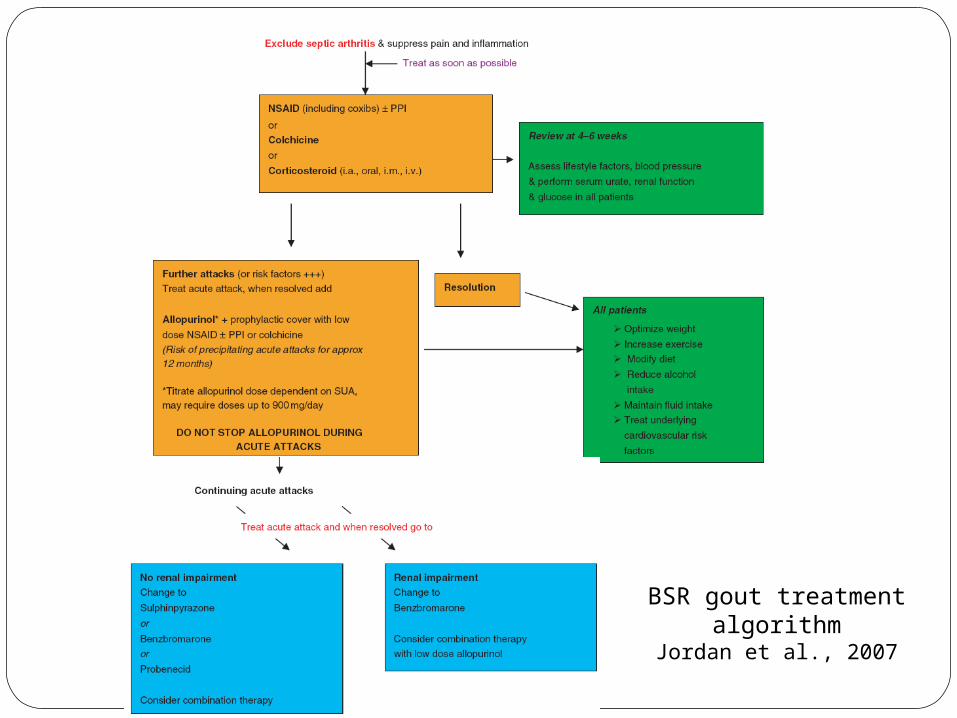
BSR gout treatment algorithmJordan et al., 2007
Future Treatments
Uricases – convert urate to allantoin?debulking urate load in tophaceous gout
IL-1 antagonists to treat severe acute flaresAnakinra, Canakinumab
Gout – Top Tips1. Gout is very rare in pre-menopausal women,
referral advised.
2. Hyperuricaemia + joint inflammation ≠ gout
3. Serum urate is often normal during a gouty flare.
4. X-rays are not useful in acute/early gout.
5. Avoid any changes to Allopurinol dosing during or within a fortnight of an acute flare of gout.
6. Commonest cause for Allopurinol failure is non compliance.
REFERENCES Mikuls TR, Farrar JT, Bilker WB et al. Gout epidemiology: results from the UK
general practice research database, 1990-1999. Ann Rheum Dis (2005), 64:267-272. Underwood M. Diagnosis and management of gout. BMJ. 2006; 332: 1315-1319 Lee H Y, Ariyasinghe J T N, Thirumoorthy T. Allopurinol hypersensitivity
syndrome: a preventable severe cutaneous adverse reaction? Singapore Med J 2008; 49(5) : 384
Borstad GC, Bryant LR, Abel MP et al. Colchicine for prophylaxis of acute flares when initiating allopurinol for chronic gouty arthritis. J Rheumatol (2004), 31:2429-2432
Zhang W, Doherty M, Pascual E et al. EULAR evidence based recommendations for gout. Parts I and II. Ann Rheum Dis (2006), 65:1301-1324
Jordan KM, Cameron JS, Snaith M et al. British Society for Rheumatology and British Health Professionals in Rheumatology guideline for the management of gout. Rheumatology (2007), 46:1372-1374
http://www.nice.org.uk/nicemedia/pdf/TA164Guidance.pdf Febuxostat for the management of hyperuricaemia in people with gout