dr. s kapurubandara 1,2, dr. v qin 3,5, dr. d gurram 1,5, dr. a anpalagan 1, a/prof h merkur 3, 5,...
TRANSCRIPT

DR. S KAPURUBANDARA1,2, DR. V QIN3,5, DR. D GURRAM1,5 , DR. A ANPALAGAN1, A/PROF H MERKUR3, 5, A/PROF R HOGG2, 4, DR. A BRAND2, 4
1 O&G DEPARTMENT, WESTMEAD HOSPITAL2 UNIVERSITY OF SYDNEY
3 SYDNEY WEST ADVANCED PELVIC SURGERY4 GYNAEONCOLOGY DEPARTMENT, WESTMEAD HOSPITAL
5 UNIVERSITY OF WESTERN SYDNEY,
SURVEY TO ASSESS CURRENT PRACTICE AND FACTORS AFFECTING CLINICIANS’ DECISION TO PERFORM
OPPORTUNISTIC BILATERAL SALPINGECTOMY DURING GYNAECOLOGICAL SURGERY FOR BENIGN DISEASE


OVCARE – British Columbia
• Sept 2010 Media release : “ovarian cancer related deaths can be reduced by 40%”
• RRS at hysterectomy
• RRS for permanent sterilization
• Genetic testing for HG serous cancers
Based on modelling study
No evidence
No RCT’s
No case control studies
No cohort studies

FOR
Ovarian Cancer
Less tubal-related
reasons for reoperation
Pelvic painImplications
on future imaging
No benefit with tubal retention

AGAINST
Insufficient evidence
Early menopause
Intra-operative
complications
Longer operative
time
Post -operative recovery

Methodology
Validated online survey to all RANZCOG fellows
ObjectiveTo assess current practice
RANZCOG statement C-25 Consideration be given and discussed with patient

26% response
1490
382
366

Designation
VMO Staff specialist Fellow Other (please specify)
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
48%
26%
21%
5%
VMO Staff specialist
Fellow Other (please specify)
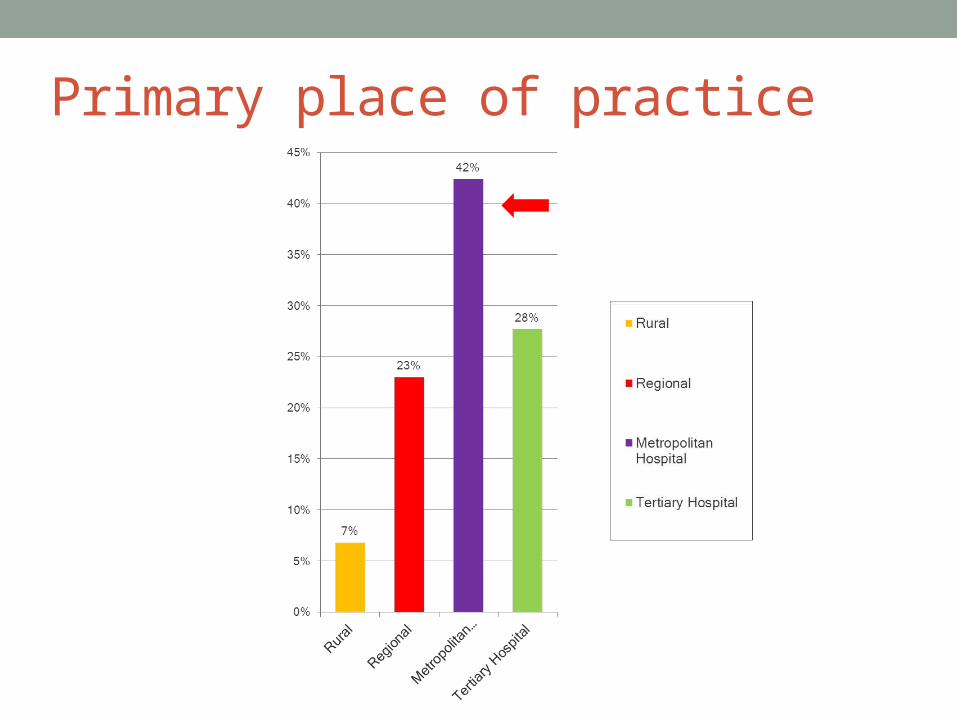
Primary place of practice

Years of clinical practice
1-5 6-10 11-15 16-20 21-25 26-30 ≥ 310%
5%
10%
15%
20%
25%23%
11%
17%
12%
8%
13%
17%

Type of specialist
Gener
alist
Gynae
colo
gist
Obste
tricia
n
Urogy
naec
olog
ist (C
U)
Gynae
onco
logi
st (.
..
CMFM
Lapa
rosc
opic
Surg
eon
CREI
COGU0%
10%
20%
30%
40%
50%
60%
70%
80%
67%
17%
1% 2%5%
0%
5%3%
1%

Do you discuss or offer opportunistic bilateral salpingectomy during gynaecological surgery for benign indications with ovarian preservation (in a low risk population)?

Which situations would you offer RRS
AH LH VH Abdo Sx Lap Sx Lap Steri TL at CS0%
20%
40%
60%
80%
100%
120%
96%
76%
28%
57%49%
42%
25%
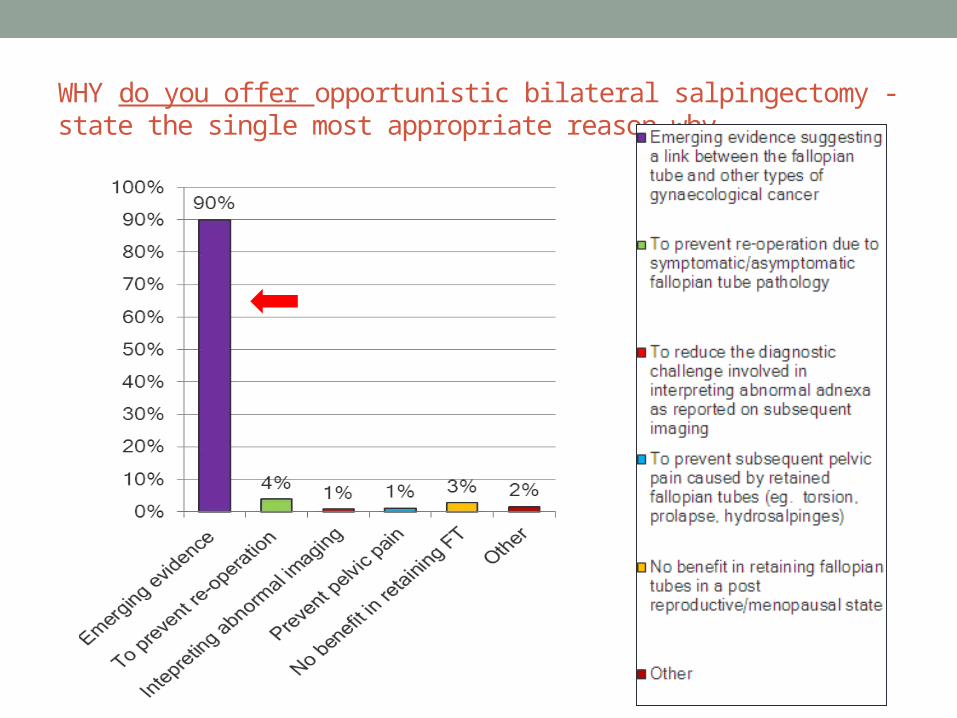
WHY do you offer opportunistic bilateral salpingectomy - state the single most appropriate reason why.

If you do not offer opportunistic bilateral salpingectomy, the single most appropriate reason why.

Survey Summary
70% would offer and discuss RRS
Most offered at AH and LH
Future directions
Further research to define protective effect and surgical outcomes
Role of registry and method of long term follow up

Thank you