dr. sarah ehsan (pt). topics to be covered in this lecture: arthritis–arthrosis fibromyalgia and...
TRANSCRIPT

Ch # 11Joint, Connective Tissue,and Bone Disorders andManagement
Dr. Sarah Ehsan (PT)

Topics to be covered in this lecture:Arthritis–arthrosis Fibromyalgia and myofascial pain syndrome Osteoporosis Fractures–post-traumatic immobilization Indications for surgical intervention
ARTHRITIS :inflammation of a jointRheumatoid arthritis and osteoarthritis
Arthrosis : limitation of a joint without inflammationTrauma, recovering from a fracture,
immobilizationDue to involvement of connective tissues and
muscles

Clinical Signs and SymptomsImpaired Mobility
capsular pattern (characteristic pattern of limitation)
Reduced joint playFirm end-feel (guarded incase of acute condition)Effusion
Impaired Muscle PerformanceImpaired Balance (reduced sensory input from
mechanoreceptors and muscle spindles)
Activity Limitations/Participation restriction

Comparison of Osteoarthritis and Rheumatoid Arthritis

Rheumatoid ArthritisAn autoimmune Chronic inflammatory,
systemic disease primarily affecting the synovial lining of joints as well as other connective tissue.
Fluctuating courseSymptoms vary from mild stiffness requiring
minor lifestyle changes and medication OR abrupt swelling, stiffness and progressive deformities requiring major life style modification, surgery and medication

Rheumatoid Arthritis: Characteristics Exacerbation (flare) and
remissionInflammatory changes in
Synovial membranearticular cartilageSubchondral marrow spacesTendon sheath
Granulation tissue (pannus) ,Erodes the articular cartilage, bone, and ligaments, Adhesions, Fibrosis, ossific ankylosis, or subluxation ,Deformity and disability
Tenosynovitis , tendon sheaths may rupture
Extra-articular changesRheumatoid nodulesAtrophy and fibrosis of
musclesMuscular weaknessFatiguemild cardiac changes

Radiographic hallmarks

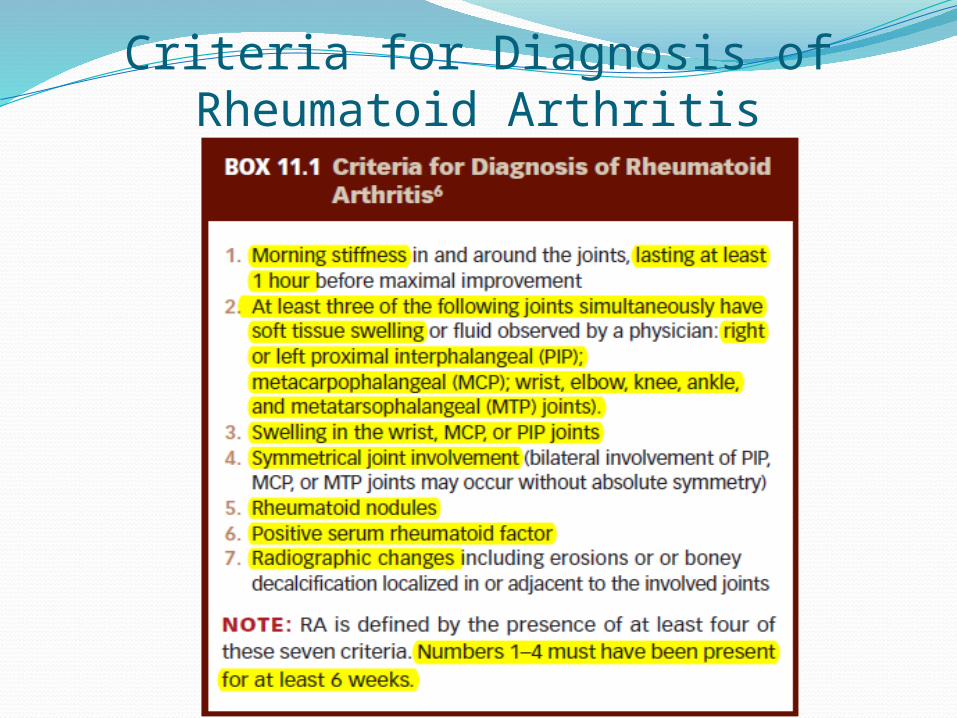
Criteria for Diagnosis of Rheumatoid Arthritis

Signs and Symptoms—Periods of Active Disease (may last months to more than a year)Effusion and swelling of the jointsJoint stiffness in morningpain on motionPain and stiffness worsen after strenuous activitysmaller joints of the hands and feet ,PIPbilateraldeformed and may ankylose or subluxate
Nonspecific symptoms low-grade fever loss of appetiteWeight, malaise, and fatigue

Principles of Joint ProtectionDo’sMonitor activitiesfrequent but short episodes
of exerciseAlternate activities to avoid
fatigueDecrease level of activitiesfunctional level of ROM,
strength and enduranceIncrease rest during flares
of the disease.appropriate adaptive
equipment
Do Not’sAvoid deforming
positions.Avoid prolonged
static positioning; change positions during the day every 20 to 30 minutes
Muscular and total body fatigue

Principles of Management—Subacuteand Chronic StagesJoint protection (splints, avoid over use,
modify environment)Improving flexibilityMuscle performanceCardiopulmonary endurance
Low–impact conditioning exercisesSwimming and bicyclingImprove aerobic capacityDecrease depression and anxiety.Group activities such as water aerobics

Principles of Management—Subacuteand Chronic StagesPRECAUTIONS
Dosage of stretching and joint mobilization techniques
CONTRAINDICATIONSVigorous stretching or manipulative techniques

Osteoarthritis—Degenerative Joint DiseaseOsteoarthritis (OA) is a
chronic degenerative disorder primarily affecting the articular cartilage of synovial joints, with eventual boney remodeling and overgrowth at the margins of the joints (spurs and lipping)
Etiology etiology of OA is not knownMechanical injury to the joint due to a major
stress repeated minor stresses poor movement of synovial fluid when the
joint is immobilizedgenetically related, especially in the hands
and hips and to some degree in the knees.

risk factorsObesityWeakness of the quadriceps musclesJoint impactSports with repetitive impact and twisting
(e.g., soccer, baseball pitching, football)Occupational activities such as jobs that
require kneeling and squatting with heavy lifting

Characteristics of OAcapsular laxity ,hypermobility or instability in
some part of rangepain and decreased willingness to move lead
to contractures eventually.Rapid destruction of articular cartilage
occurs with immobilization

Characteristics of OAThe cartilage splits and thins out, losing its
ability to withstand stress. As a result, crepitation or loose bodies may
occur in the joint. Eventually, subchondral bone becomes exposed. There is increased density of the bone along
the joint line, with cystic bone loss and osteoporosis in the adjacent metaphysis.
During the early stages, asymptomatic because the cartilage is avascular and aneural

Characteristics of OAEnlargement of
effected joints:Heberden’s nodes
(enlargement of the distal interphalangeal joint of the fingers)
Bouchard’s nodes (enlargement of the proximal interphalangeal joints)

Commonly involved jointsWeight-bearing joints (hips and knees)Cervical and lumbar spineDistal interphalangeal joints of the fingersCarpometacarpal joint of the thumb 1st MTP



Adaptive/assistive devices for OA and RA

V