dr. sharifa al-duraibi. degeneration of one or more intervertebral disc(s) of the spine. disc...
TRANSCRIPT

Dr. Sharifa AL-Duraibi
Degenerative Disease

Degeneration of one or more intervertebral disc(s) of the spine.
Disc degeneration is a disease of aging, and though for most people is not a problem, in certain individuals a degenerated disc can cause severe chronic pain if left untreated.
Degenerative disc disease

low back pain world wide
common complaint among adults.
lifetime prevalence in working population up to 80%.
60% experience functional limitation or disability.
second most common reason for work disability.
despite advances in imaging and surgical techniques
LBP prevalence and its cost are relatively unchanged.

Pathologic changes
Fibrocartilage replaces the gelatinous mucoid material of the nucleus pulposus as the disc changes with age.
There may be splits in the annulus fibrosis, permitting herniation of elements of nucleus pulposus.
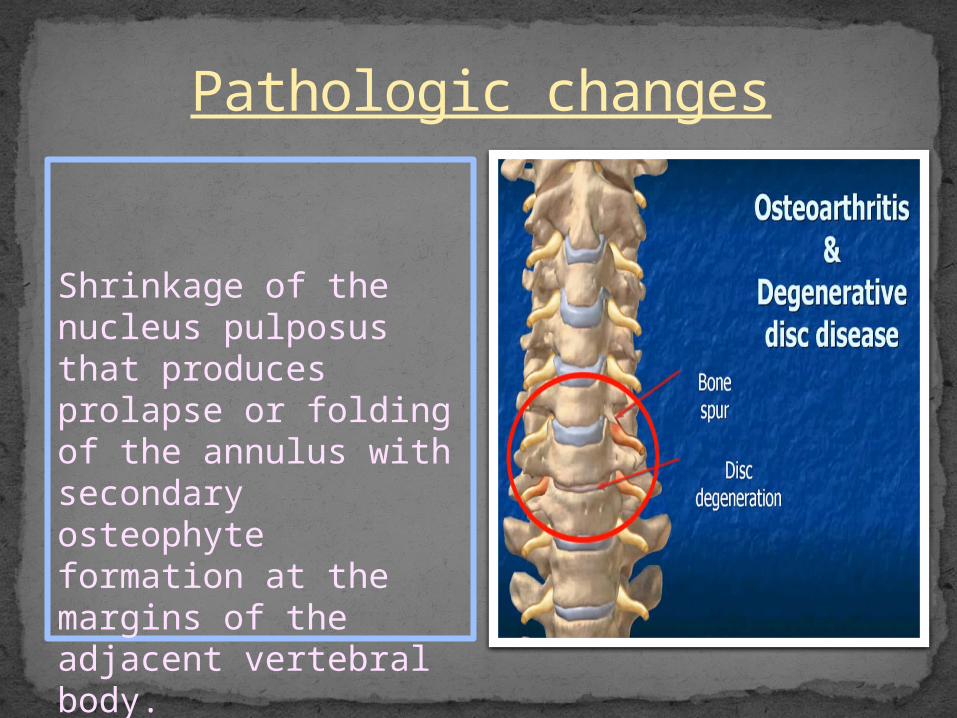
Shrinkage of the nucleus pulposus that produces prolapse or folding of the annulus with secondary osteophyte formation at the margins of the adjacent vertebral body.
Pathologic changes

Disc pathology vs Pain
degree of disc injury (size of tear / herniation), nor the degree of nerve root compression correlate with subjective pain or functional disability.
Karppinen J. et al. “Severity of Symptoms and Signs in Relation to MRI Findings Among Sciatica Patients.” Spine 2001; 26(7):E149-E154
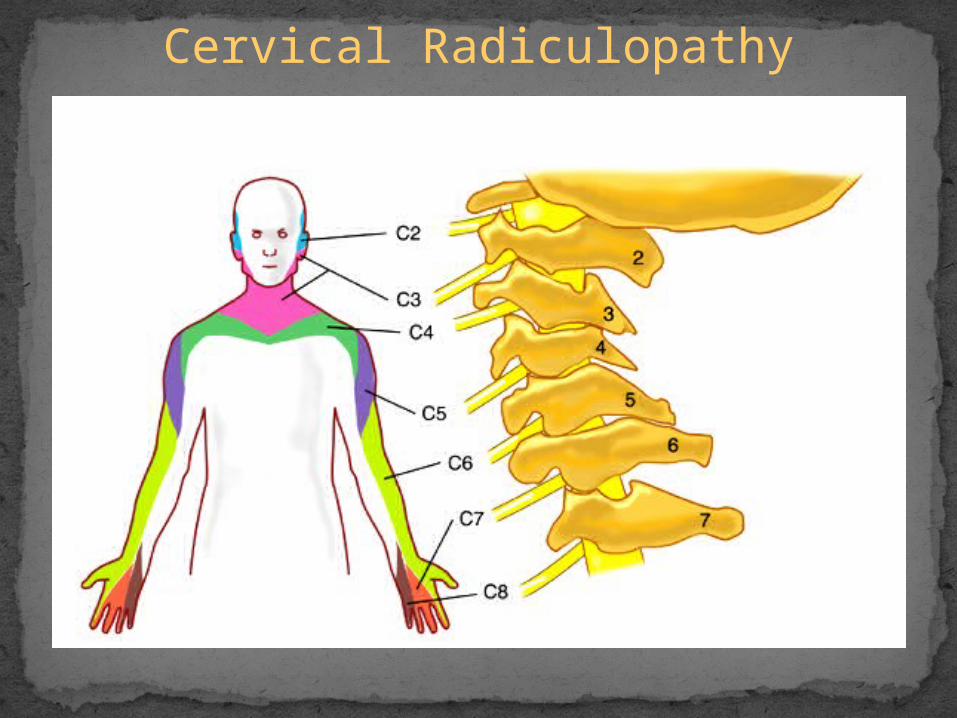
Cervical Radiculopathy
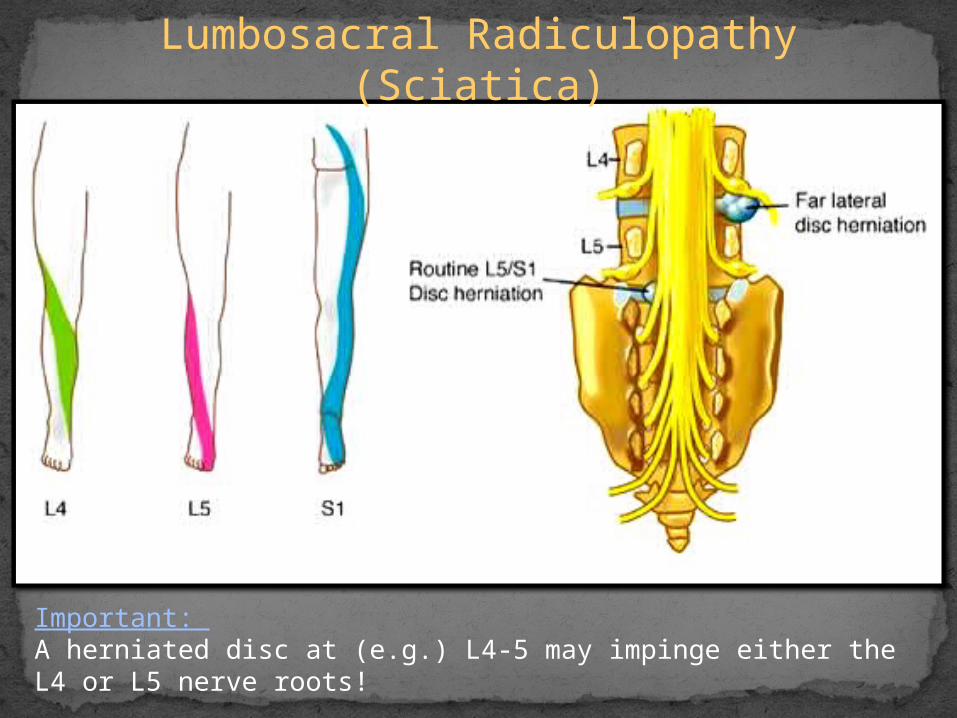
Lumbosacral Radiculopathy (Sciatica)
Important: A herniated disc at (e.g.) L4-5 may impinge either the L4 or L5 nerve roots!
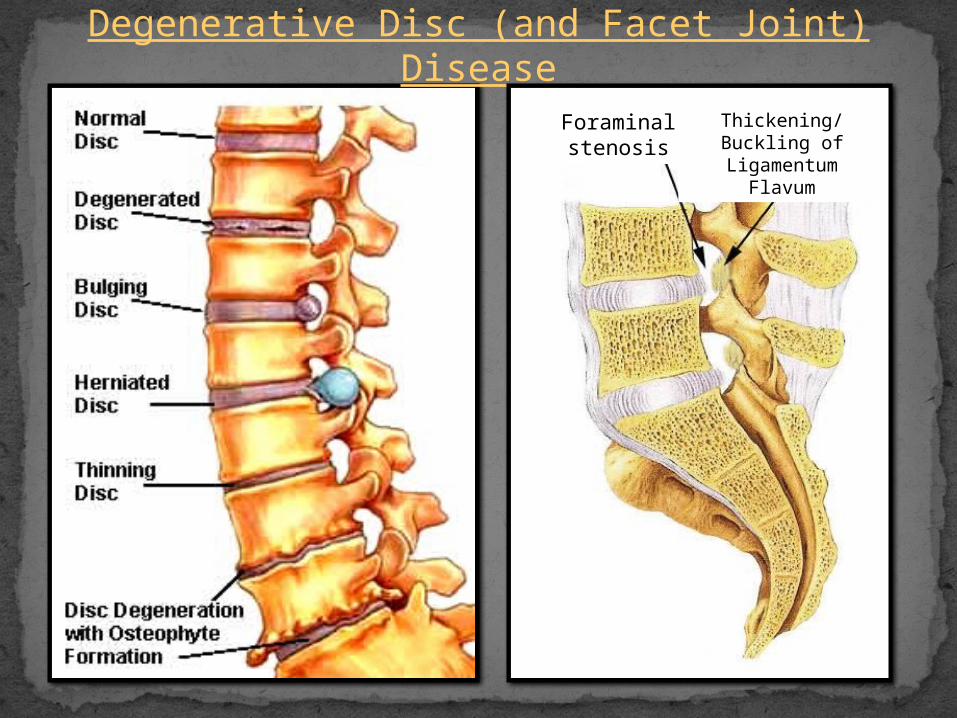
Degenerative Disc (and Facet Joint) Disease
Foraminal stenosis
Thickening/Buckling of Ligamentum Flavum
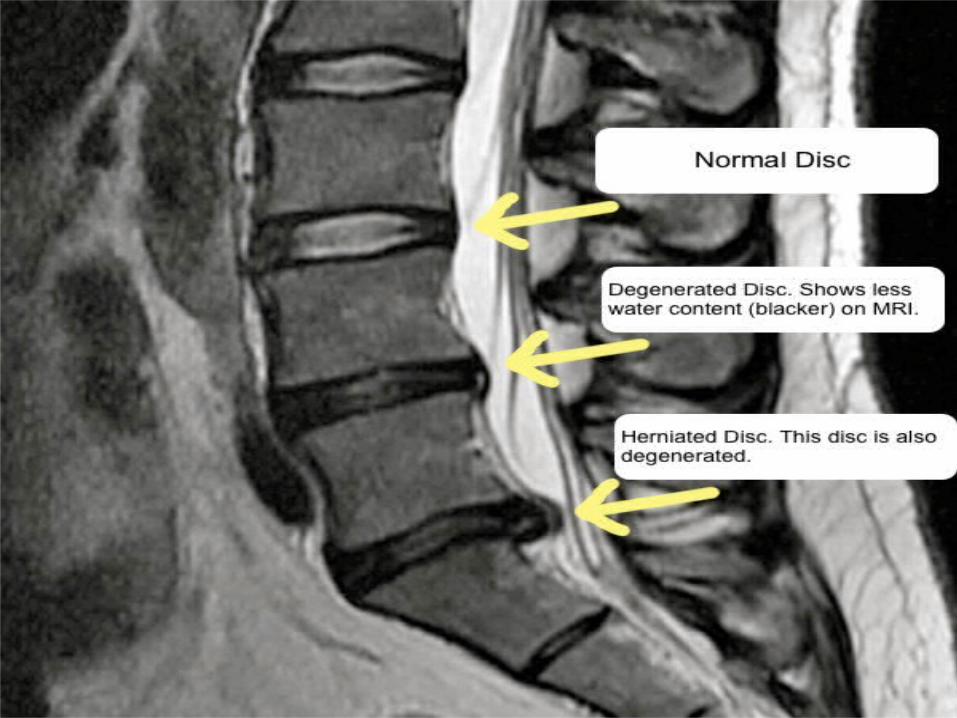

MRI - Degenerative Disc Disease
Age:20-40 36% have degenerated disc.50 85-95% have degenerated disc.60-80 98% have degenerated disc.** <60 20% have asymptomatic disc herniation.
Conclusion: Abnormal findings on MRI frequently DO NOT relate to symptoms (and vice versa) !!

MRI – Herniated Disc Levels
85-95% at L4-L5/ L5-S1.5-8% at L3-L4.2% at L2-L3.1% at L1-L2/ T12-L1.
** Cervical: most common C4-C7.
**Thoracic: 15% in asymptomatic pts. at multiple levels, not often symptomatic.

Anular tear
Separations between anular fibers, avulsion of fibers from their vertebral body insertions, or breaks through fibers involving one or many layers of the anular lamellae. The terms 'tear' or 'fissure' does not imply that the lesion is consequent to trauma. In case of a traumatic event the term 'rupture' is appropriate.a
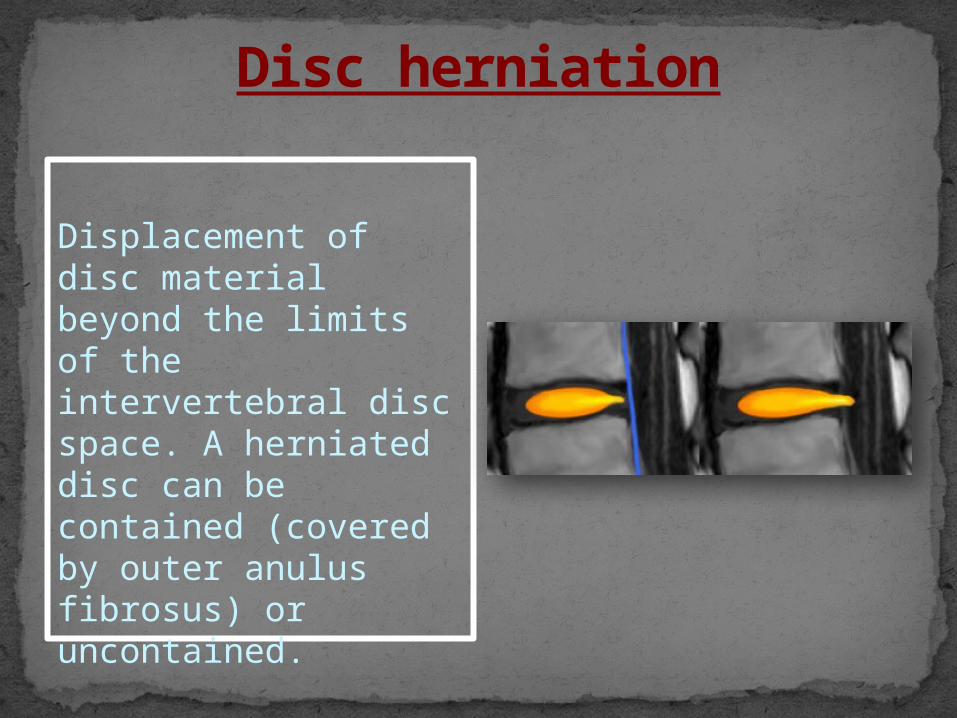
Disc herniation
Displacement of disc material beyond the limits of the intervertebral disc space. A herniated disc can be contained (covered by outer anulus fibrosus) or uncontained.

Focal Herniation
Is a herniated disc less than 90? of the disc circumference.
Disc herniation
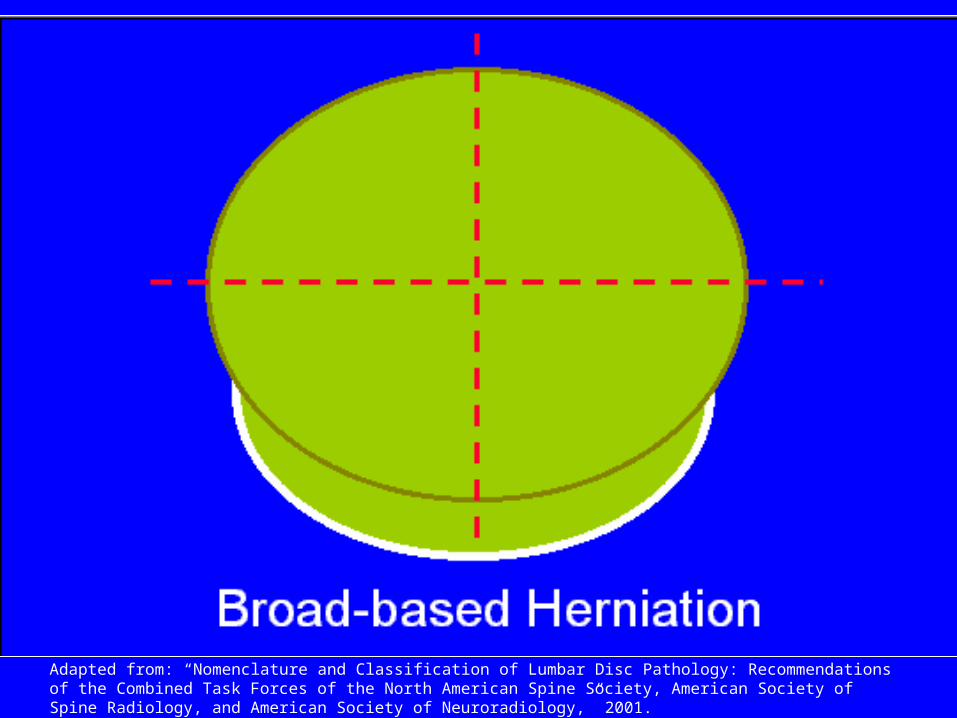
Broad based hernia
Is a herniated disc in between 90?-180? of the disc circumference.
Disc herniation
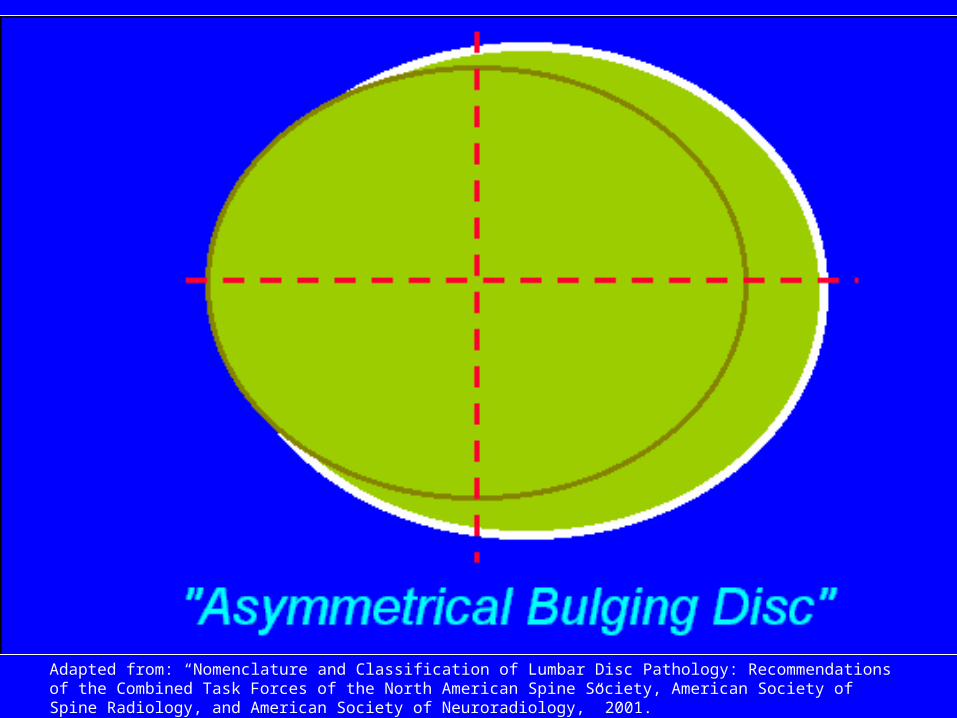
Is the presence of disc tissue 'circumferentially' (180?-360?) beyond the edges of the ring apophyses and is NOT considered a form of herniation.
Bulging Disc
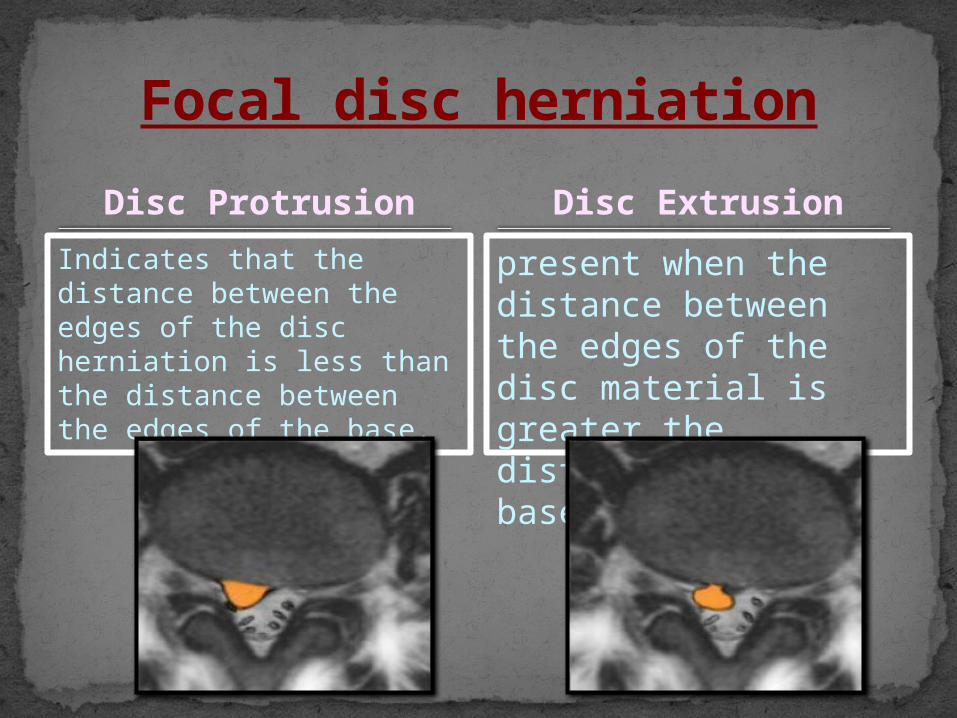
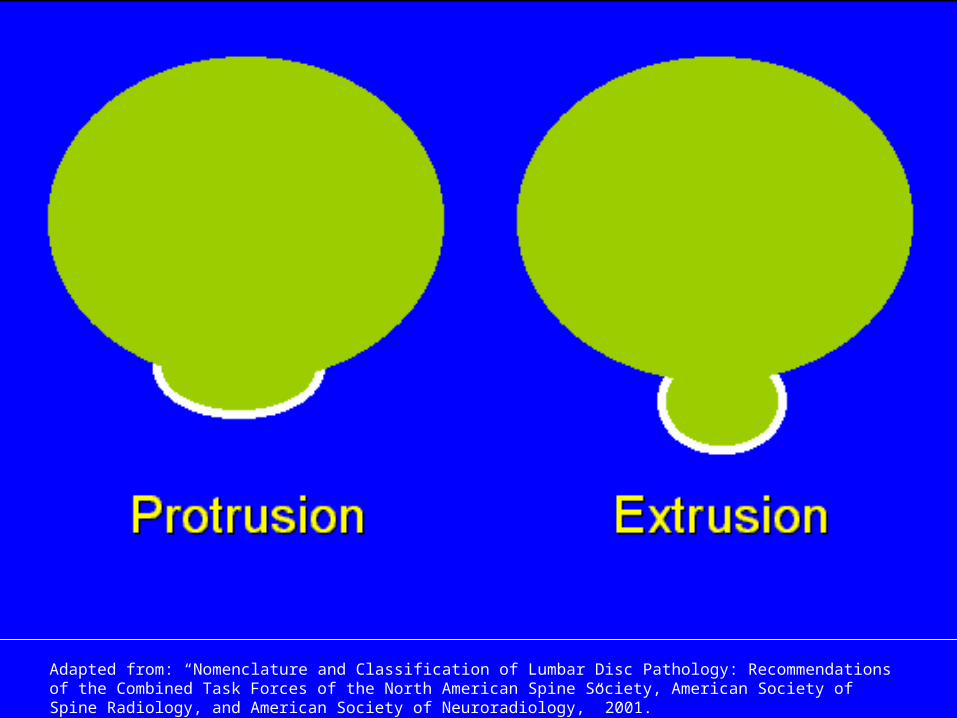
Disc Protrusion
Indicates that the distance between the edges of the disc herniation is less than the distance between the edges of the base.
Focal disc herniation
Disc Extrusion
present when the distance between the edges of the disc material is greater the distance at the base.
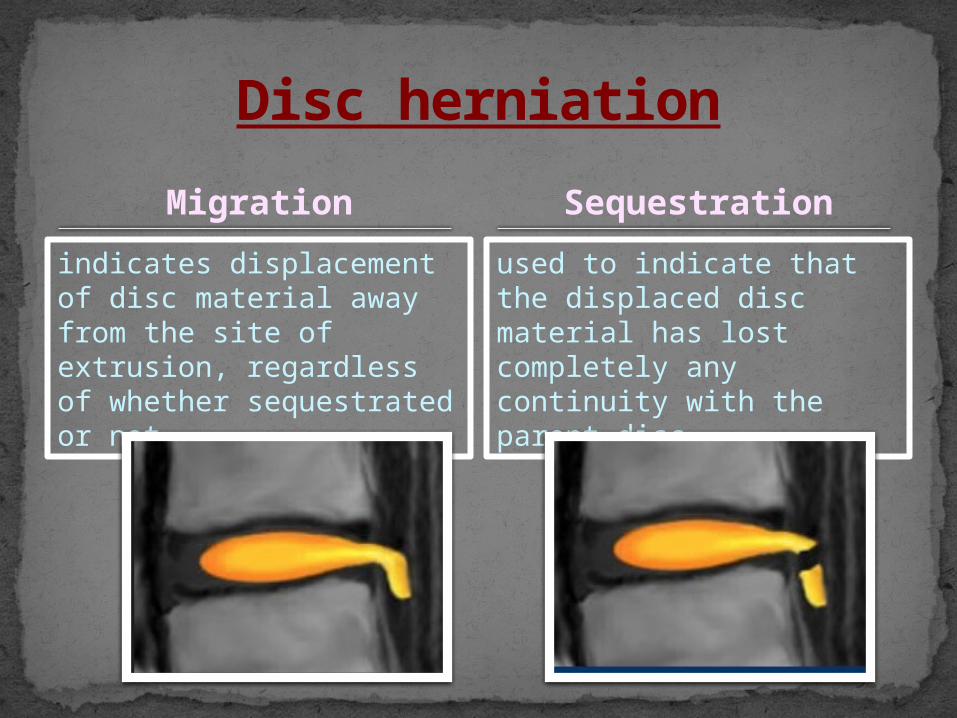
Migration
indicates displacement of disc material away from the site of extrusion, regardless of whether sequestrated or not.
Disc herniation
Sequestration
used to indicate that the displaced disc material has lost completely any continuity with the parent disc
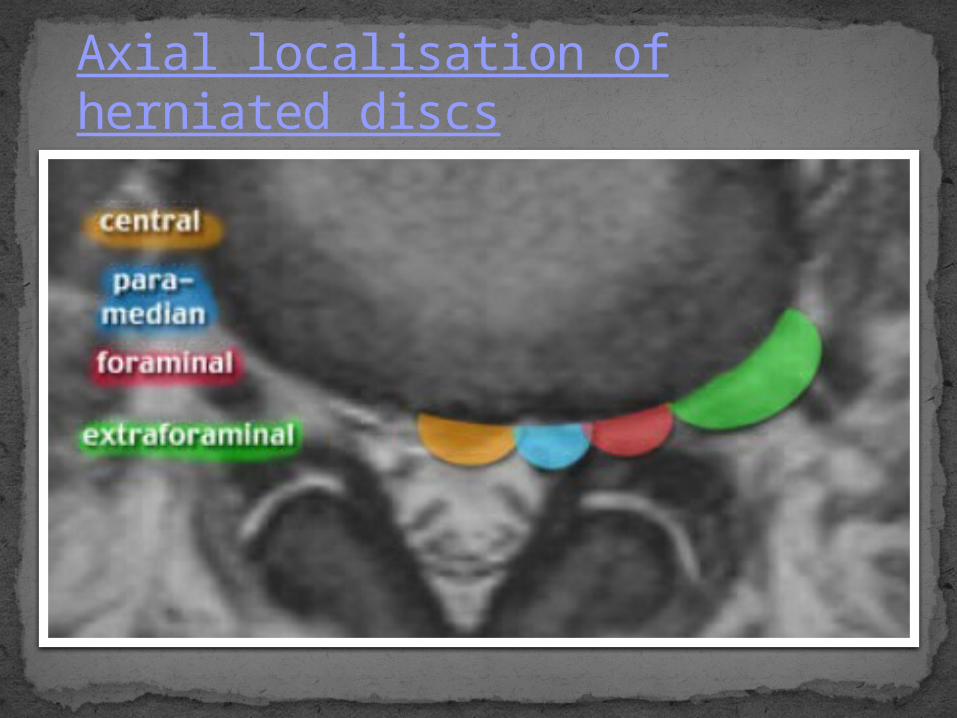
Axial localisation of herniated discs

Adapted from: “Nomenclature and Classification of Lumbar Disc Pathology: Recommendations of the Combined Task Forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology,” 2001.
Adapted from: “Nomenclature and Classification of Lumbar Disc Pathology: Recommendations of the Combined Task Forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology,” 2001.
Adapted from: “Nomenclature and Classification of Lumbar Disc Pathology: Recommendations of the Combined Task Forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology,” 2001.

Adapted from: “Nomenclature and Classification of Lumbar Disc Pathology: Recommendations of the Combined Task Forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology,” 2001.
Adapted from: “Nomenclature and Classification of Lumbar Disc Pathology: Recommendations of the Combined Task Forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology,” 2001.
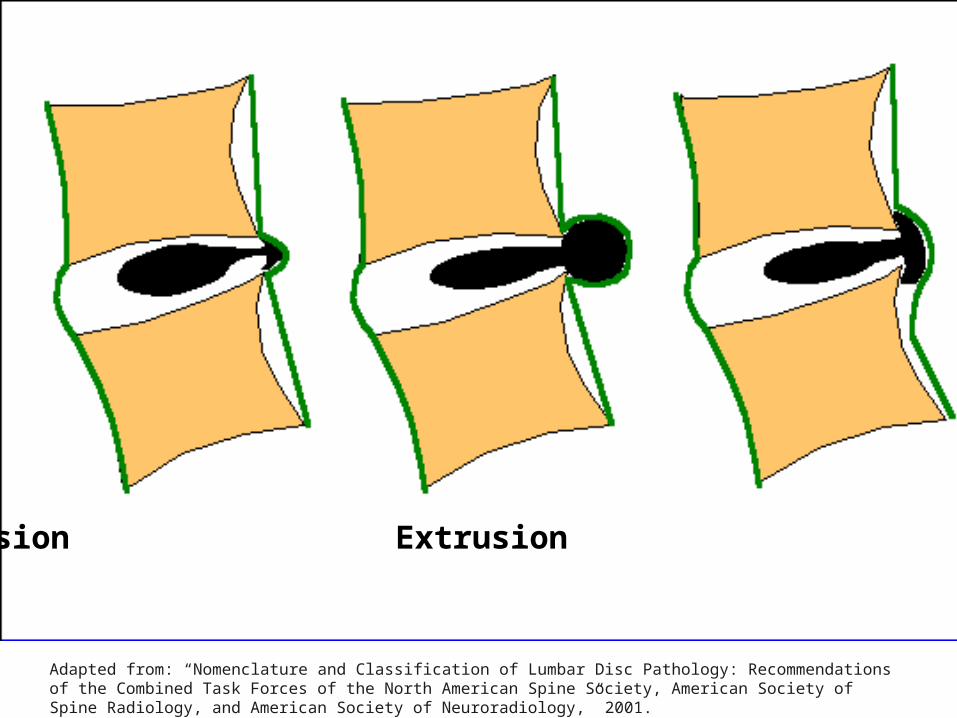
Protrusion Extrusion Extrusion
Adapted from: “Nomenclature and Classification of Lumbar Disc Pathology: Recommendations of the Combined Task Forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology,” 2001.

Protrusion Protrusion w/migration
Protrusion w/migration +
sequestration
Adapted from: “Nomenclature and Classification of Lumbar Disc Pathology: Recommendations of the Combined Task Forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology,” 2001.
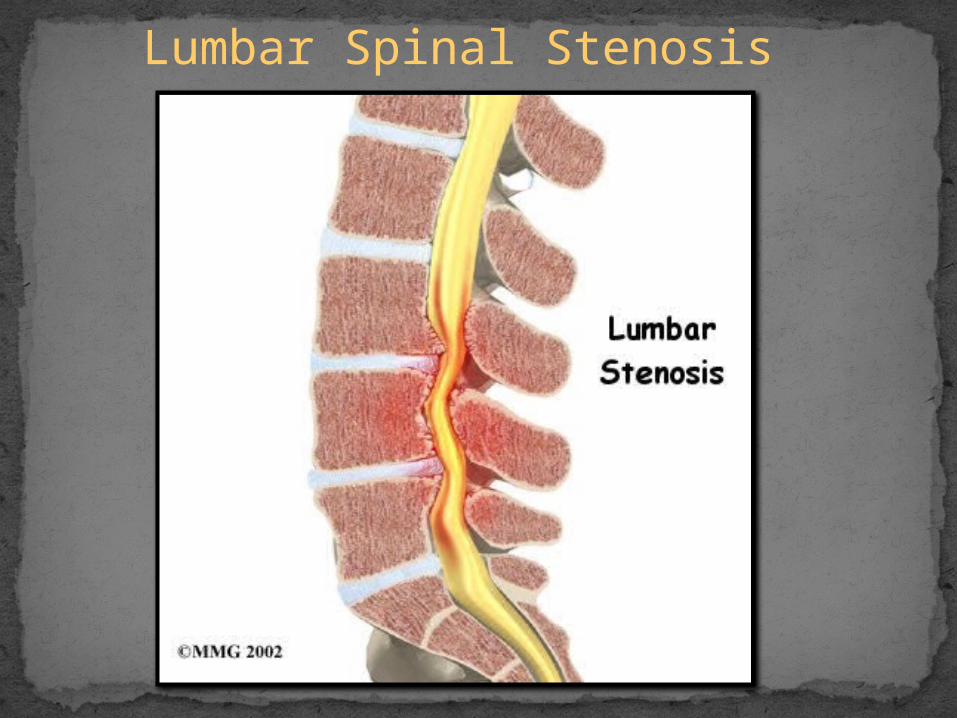
Lumbar Spinal Stenosis
Lumbar Spinal Stenosis
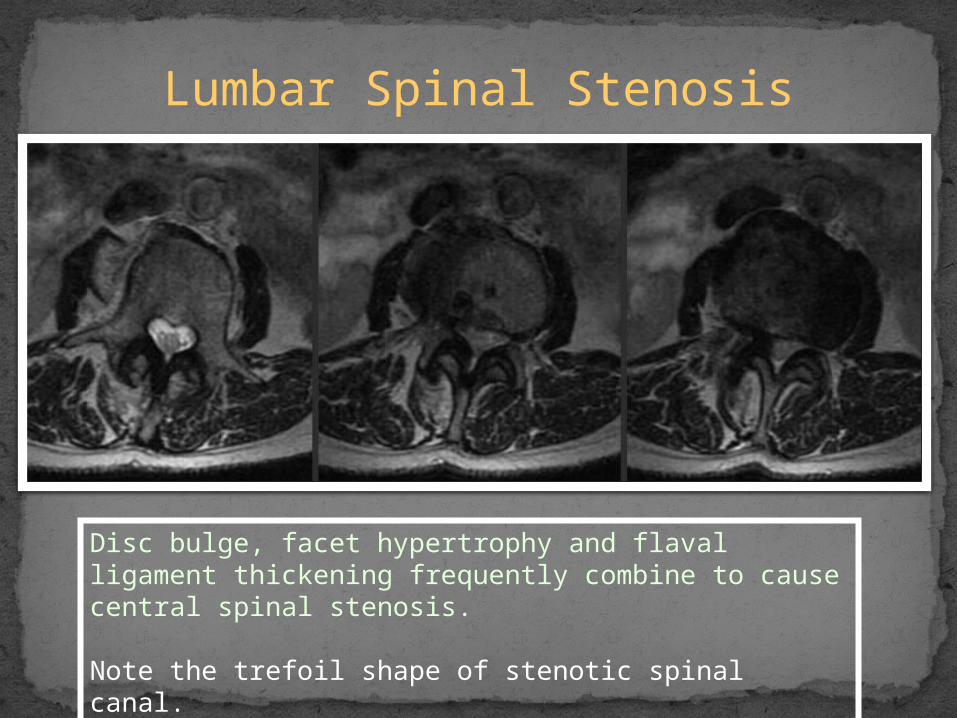
Disc bulge, facet hypertrophy and flaval ligament thickening frequently combine to cause central spinal stenosis.
Note the trefoil shape of stenotic spinal canal.

Lumbar Spinal Stenosis
Disc bulge, facet hypertrophy and ligament flavum thickening frequently combine to cause central spinal stenosis
Note the trefoil shape of stenotic spinal canal
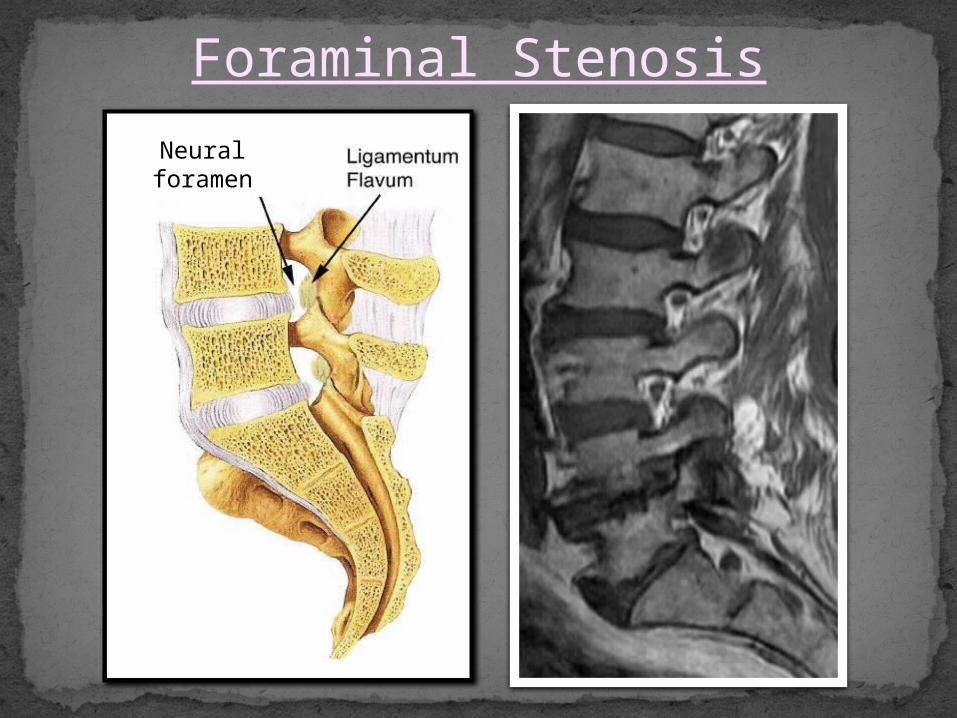
Foraminal Stenosis
Neural foramen
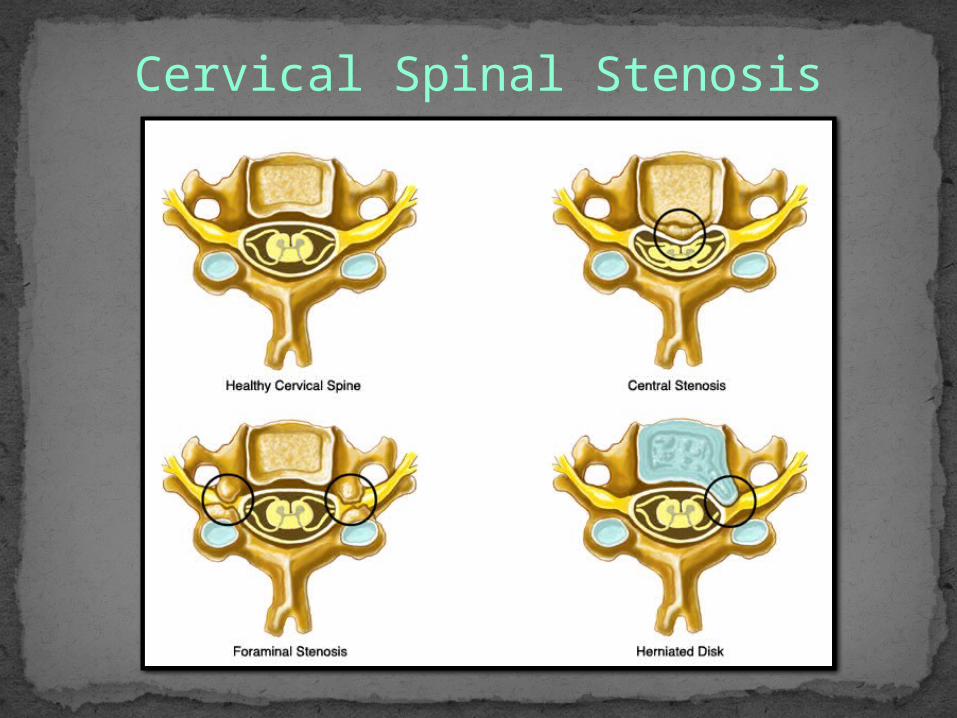
Cervical Spinal Stenosis
case study - annie 30 y.o. female presents with low back
pain.
Pain radiating down right leg.
Initial onset approximately 1 year.
Referred by orthopedic surgeon.
On motrin, previously darvocet, flexeril and valium.
Previous treatments: chiropractic and physical therapy.
Diagnostic studies• A-P / lateral Plain Film:
Degenerative disc height loss at L4-5 level.
• MRI:L4-L5: Large central disc herniation (9mm in AP
X 10mm Broad) effacing the ventral thecal sac and impressing upon the central canal.
• This produces moderate canal stenosis.L5-S1: broad disc bulge with radial tear.
• mild effacement upon the ventral thecal sac.

Imaging
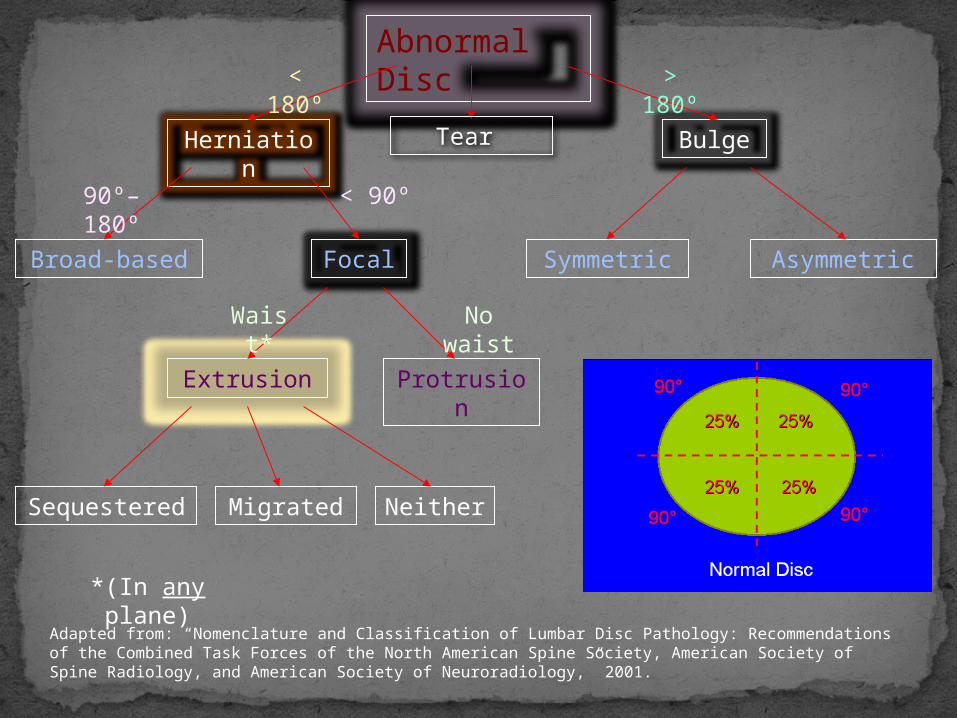
Abnormal Disc
Bulge
Symmetric Asymmetric
Herniation
Broad-based Focal
Extrusion Protrusion
Sequestered Migrated Neither
> 180º
< 180º
< 90º90º–180º
No waist
Waist*
Adapted from: “Nomenclature and Classification of Lumbar Disc Pathology: Recommendations of the Combined Task Forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology,” 2001.
*(In any plane)
Tear
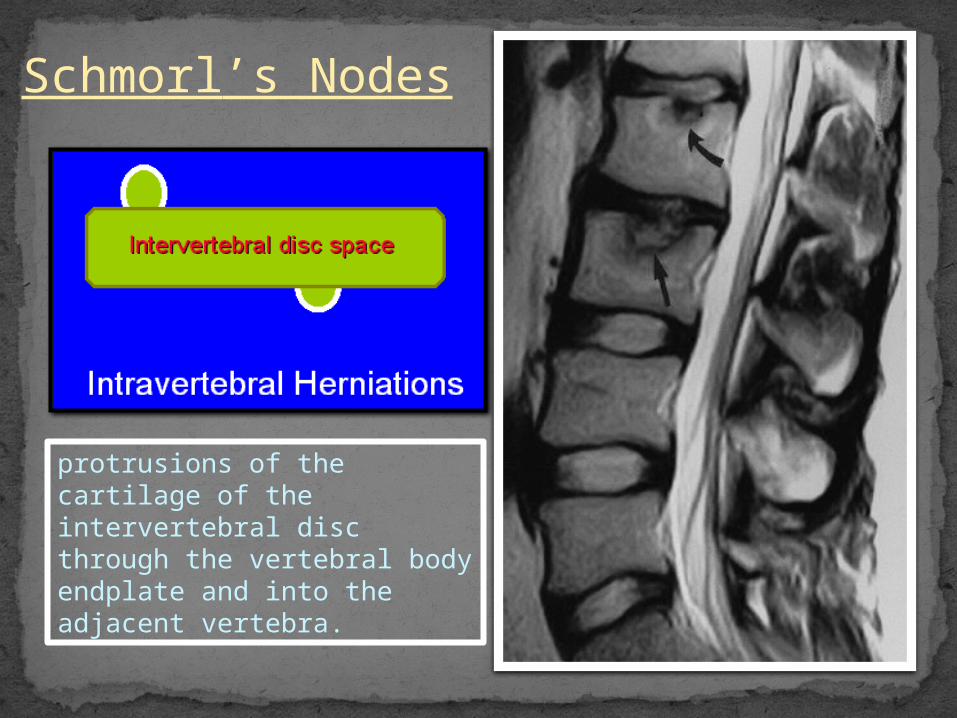
Schmorl’s Nodes
protrusions of the cartilage of the intervertebral disc through the vertebral body endplate and into the adjacent vertebra.

Confusing “Spondy-” Terminology
Spondylosis = “spondylosis deformans” = degenerative spine.
Spondylitis = Inflamed spine (e.g. ankylosing, pyogenic, etc.).
Spondylolysis = Chronic fracture of pars interarticularis with nonunion (“pars defect”).
Spondylolisthesis = anterior slippage of vertebra typically resulting from bilateral pars defects.
Pseudospondylolisthesis = “degenerative spondylolisthesis” (spondylolisthesis resulting from degenerative disease rather than pars defects)

Spondylolysis / Spondylolisthesis

current therapies for discogenic pain or disc pathology
Medication and limited activity
Spinal rehabilitation.
Interventional pain management.
Spinal surgery.
