dr w afa ababtain,md int medicine department,kfhu january,31,2011
TRANSCRIPT

Dr Wafa Ababtain ,MDInt medicine department,KFHU
January,31,2011
Latent tuberculosis infection new Saudi guide lines

Outlines• Global and local epidemiological data• Latent TB infection• Why and how to identify LTBI• BCG and TST interpretation• Technique ,reading and interpretation of TST • Serial tuberculin testing• IGRA and Saudi recommendations• Indication for TST and who should be treated• Recommended regimen for LTBI• Special situations with LTBI• Cases study• conclusion

Global TB statistics• one third of world's population or two billion people carry
the TB bacteria. • more than 9 million become sick each year with “active”
TB which can be spread to others.• about 2 million deaths/year due to TB, > 90% deaths in
low- and middle-income countries .• 22 countries account for 80% of all new TB cases,> 50% in
5 countries .India, China, South Africa, Nigeria, and Indonesia.
• TB is leading cause of morbidity and mortality among HIV-infected persons
the Kaiser Family Foundation’s The Global Tuberculosis Epidemic fact sheet June 2010



- 1.7 million people died from TB (including380 000 women) in 2009, including 380 000people with HIV, equal to 4700 deaths a day.
- The TB death rate has fallen by 35% since 1990


- There were 9.4 million new TB cases (including 3.3 million women) in 2009, including 1.1 million cases among people with HIV
- Most cases were in the South-East Asia, African and Western Pacific regions (35%, 30% and 20%,
respectively).- An estimated 11–13% of incident cases were HIV-
positive, the African Region accounted for approximately 80% of these cases.



- Multidrug-resistant TB (MDR-TB) is a form of TB that is difficult and expensive to treat and fails to respond to standard first-line drugs
- There were an estimated 440 000 new MDR-TB cases in 2008, and 150 000 deaths from MDR-TB
- In 2010, the largest WHO MDR-TB survey reported the highest rates ever of MDR-TB, with peaks of up to 28% of new TB cases in some settings of the former Soviet Union

- Extensively drug-resistant TB (XDR-TB) occurs when resistance to second-line drugs develops
on top of MDR-TB- XDR-TB cases have been confirmed in 58
countries

WHO
Tuberculosis profile in Saudi Arabia

Saudi ArabiaTuberculosis profile
Population 2009 (millions) 26

Country profile 2008-2009: SAUDI ARABIATB Unit of the WHO Regional Office for Eastern-Mediterranean Region

Saudi Arabia Tuberculosis profile

Country profile 2008-2009: SAUDI ARABIATB Unit of the WHO Regional Office for Eastern-Mediterranean Region

Major challenges still exist: • Deaths - 1.7 million died in 2009 from what is a curable
disease. • Incidence - though falling, it is falling too slowly. Under
the current rate of decline, TB will not be eliminated in our lifetime.
• MDR-TB response - the response is still insufficient and more efforts are needed to scale up and strengthen programmes, especially with 440 000 new cases emerging each year, and that less than 5% of those cases being properly treated.

Scanning electron micrograph of Mycobacterium tuberculosis bacilli.

Latent tuberculosis (LTB)
Definition• mycobacterial infection, dormant state, diagnosed
by positive skin test (PPD)• people with latent tuberculosis infection retain
viable M. tuberculosis bacilli within their lungs, even though they are asymptomatic and not infectious.
• When becomes immunosuppressed , the dormant bacteria can reactivate within the calcified tubercles and develop active TB disease.

GIT

Why to identify Latent Tuberculosis
• Identification and treatment of latent tuberculosis infection can reduce the risk of development of disease by as much as 90 percent
• to protect the health of the individuals as well as the public by reducing the number of potential sources of infection

• most cases of tuberculosis in saudi arabia are due to reactivation of latent infection
• targeted testing of individuals at high risk of disease progression is a key component of tuberculosis control
• many practitioners remain reluctant to use the TST, and therefore, do not give therapy for latent TB infection even to patients at high risk of reactivation.
Latent Tuberculosis

Diagnosis of LTBI • active tuberculosis be excluded by medical evaluation• medical history and a physical examination to check
for suggestive symptoms and signs• chest radiograph• testing of sputum or other clinical samples for the
presence of M. tuberculosis.• Neither an IGRA nor TST can distinguish LTBI from
active tuberculosis.


Saudi guidelines for testing and treatment of latent tuberculosis infection
Ann Saudi Med. 2010 Jan–Feb; 30(1): 38–49Al Jahdali, H. Baharoon, S. Abba, A. Menzies, D.• the Saudi Thoracic Society (STS)• the Saudi Society of Medical Microbiology and
Infectious Disease (SSMMID)• Saudi Association of Public Health (SAPH) • Society of Family and Community Medicine provides the first national recommendation for targeted
tuberculin testing and treatment regimens for person with latent tuberculosis infection in Saudi Arabia.

Prevalence of LTBI in Saudi Arabia
The prevalence of LTBI at 10 and 20 years is
3.4% and 6.7% respectively, placing Saudi Arabia in the intermediate prevalence
(2%-14%) category

Making the diagnosis
methods of detection of latent TB • PPD skin test - induration ≥ 5 mm in immunocompromized or
exposed persons -induration ≥ 10 mm in high risk persons -induration ≥ 15 mm in persons with no risk factors • interferon-gamma blood test • chest x-ray - may not be helpful as most latent TB is clinically
inapparent

• BCG vaccination was started in 1964 in Saudi Arabia and a 95.9% coverage rate was achieved by 2007
• Al Kassimi et al in 1993 – the first comprehensive and nationwide
tuberculin survey in Saudi Arabian general population with urban/rural stratification. 33% of the subjects had a positive TST, and 56% were aged 45 years and older.
BCG and TST interpretation
al-Kassimi FA,Tuber Lung Dis. 1993

BCG and TST interpretation
• A meta-analysis including more than 24 studies found that only 1% of patients who received BCG during infancy were TST positive if tested more than ten years after BCG vaccination
• longer-lasting effect on TST if BCG was given later in life
• Most of the international guidelines recommend ignoring BCG's effect on the interpretation of TST in persons at increased risk of developing active TB.

Technique for the TST• A standard tuberculin
syringe with a 27-gauge needle is used to inject 5 tuberculin units of purified protein derivative (PPD) intradermally.
• The inner surface of the forearm is used. . A small wheal 5 mm in diameter should be elicited at the time of injection.

• If incorrect administration is suspected, a second test dose can be given immediately at a site that is at least 5 cm away from the first one.
• It should be administered as soon as feasible after filling the syringe, ideally within 20 minutes.
• Long-term storage of prefilled syringes is not recommended. Tuberculin material should be kept refrigerated but not frozen, and most importantly, kept protected from light

Reading the TST
• a delayed hypersensitivity immune reaction.. Reading is done between 48 and 72 hours.
• The transverse diameter of the induration, but not erythema, is demarcated The induration is measured and recorded in millimeters. If there is no reaction, the size should be recorded as 0 mm and not simply as “negative”.
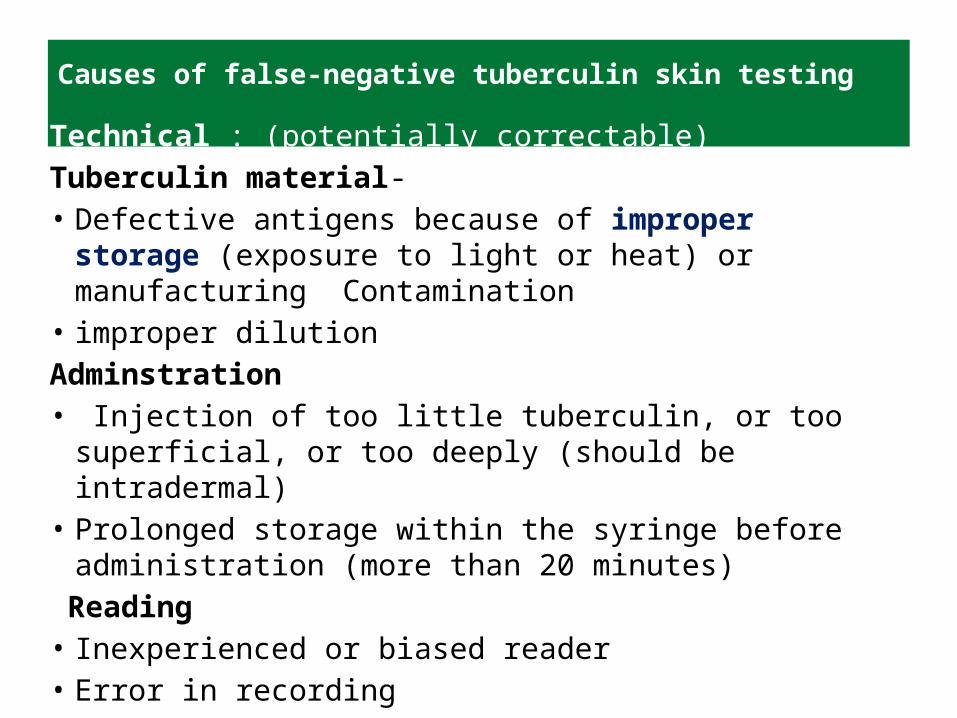
Causes of false-negative tuberculin skin testing
Technical : (potentially correctable)Tuberculin material-• Defective antigens because of improper storage (exposure
to light or heat) or manufacturing Contamination• improper dilution Adminstration• Injection of too little tuberculin, or too superficial, or too
deeply (should be intradermal)• Prolonged storage within the syringe before
administration (more than 20 minutes) Reading• Inexperienced or biased reader • Error in recording

Causes of false-negative tuberculin skin testing Biological factors: (not correctable)
Infections -activeTB (more advanced diseas ) -Viral, bacterial, or fungal infections -HIV (especially if CD4 count <200)• Live virus vaccination within the past two months• Metabolic derangement, protein depletion, chronic renal failure,
severe malnutrition, stress (surgery, burns)• Concurrent use of immunosuppressive drugs: (corticosteroids,
TNF inhibitors, and others)• Very young <6 months or elderly • Diseases of lymphoid organs: (lymphoma, chronic lymphocytic
leukemia, sarcoidosis

Causes of false-positive tuberculin skin testing
• Nontuberculous mycobacteria– Reactions caused by nontuberculous
mycobacteria are usually 10 mm of induration
• BCG vaccination– Reactivity in BCG vaccine recipients generally
wanes over time; positive TST result is likely due to TB infection if risk factors are present

Serial tuberculin testing (conversion or boosting)
When repeated tuberculin testing has been performed, some individuals may manifest an increased tuberculin reaction on their second test in the absence of any obvious exposure.

Boosting
• the restimulation of previously acquired immunity from earlier exposure.• the risk of developing active tuberculosis actually lower than those with an
initial positive TST, and much lower than in persons with tuberculin conversion
Tuberculin conversion
• occurs after an initial tuberculin infectiona, TST reaction of 10 mm or more plus an increase of 6 mm or more from the previous TST results within a two-year period.
• the risk of disease is between 5% and 20% over the next two years alone• The ATS/CDC/IDSA definition of conversion requires an increase of 10 mm or more from the previous TST result.

boosting
there is no intervening exposure
If the second TST is performed soon (within two weeks) after the first one

Two-step testing protocol
TST -tuberculin skin test*TST_tuberculin skin test

Patient history• 36-year-old Asian female • Moved to U.S. from Philippines > 15 years ago• Plans to work in a correctional facility • TST result negative 1 year ago • TST for pre-employment physical = 26 mm of
induration • CXR normal • No symptoms of TB disease• No known contact with a TB patient

• Patient’s TST converted from negative to positive (within a 2-year period)
• TST conversion increases risk for progressing from LTBI to TB disease
• Foreign-born status is less of a risk factor, i.e., she immigrated more than 5 years ago

IGRA• Interferon
Gamma ReleaseAssay
• in-vitro tests that measure the levels of interferon-g released by sensitized T lymphocytes after stimulation with antigens of M. tuberculosis.
• These (IGRA) do not present cross-reaction with (BCG), nor with the majority of nontuberculous mycobacteria


• provide results in a single patient visit.• They do not have a ‘booster’ effect• can be repeated without the need for two-step testing.• They have excellent specificity and are unaffected by
BCG and NTM (estimated specificity >98%).• IGRA sensitivity in active TB has been found to be
comparable to the sensitivity of TST (up to 30% negative).
• IGRAs are NOT recommended for the diagnosis of active TB
IGRA

• the CDC guidelines recommend using either TST or IGRA for LTBI testing.
• UK, Canada, Spain, Italy recommend a two-step approach where TST is done first, followed by IGRA.
• There is a potential boosting effect of TST on IGRA results, it may be best to collect blood for IGRA at the time the TST is read (i.e., within three days of placing PPD)
IGRA

Disadvantages• higher material cost• the need for an equipped laboratory• requirement to draw peripheral blood.• interpretation of IGRA conversions and
reversions is unclear• evidence is rather limited in children and
immunocompromised populations.
IGRA

Recommendations
• IGRAs should not be used to diagnose active TB in adults. In children, they may be used as an adjunct test, in combination with TST, chest x-ray, and microbiological investigations. A negative IGRA alone should not be used to rule out active TB.
• In BCG-vaccinated individuals (adults and children), IGRAs may be used to confirm a positive TST result (i.e., to check if the TST result is a false positive). If a positive TST result is confirmed by a positive IGRA result, LTBI treatment should be initiated after ruling out active TB.
• In immunocompromised patients, if a false-negative TST result is suspected, IGRAs may be used to rule out LTBI.

Indication for TST and who should be treated
1. high risk of recent infection.2. who are at high risk of progression from LTBI
to TB disease.• High-risk individuals –risk for reactivation is 6 x higher than for normal• Moderate-risk - 3 - 6 X normal• Low-risk individuals - 1.5 – 3X normal


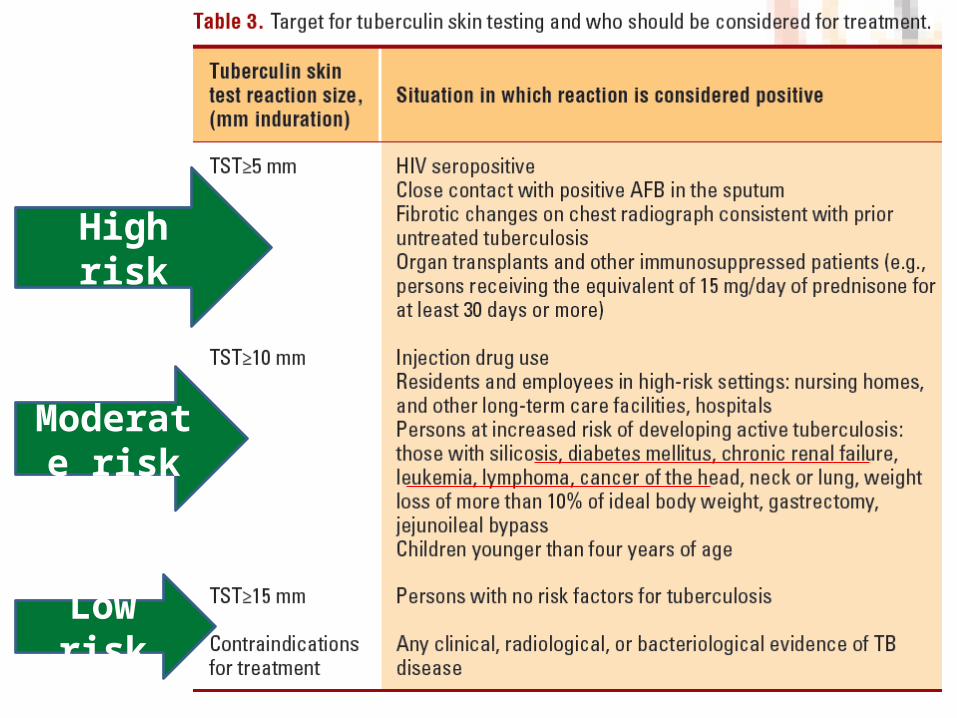
High risk
Low risk
Moderate risk

• Testing is not recommended for individuals ≥65 years unless they are at high risk for reactivation.
• In newly detected LTBI ,no treatment to be started before excluding active TB disease
• Medical examination,symptoms and chest x-ray with radiographic signs, sputum smear microscopy and culture to rule out active TB.
indications and precautions in LTBI testing and treatment

• If the radiograph is normal but the patient has a clinical presentation consistent with TB, further workup is indicated and treatment of LTBI should be delayed
• If the radiograph is abnormal and consistent with TB sputum for AFB stain and culture should be obtained.
-Starting treatment pending the culture results or -waiting for culture results before starting
therapy dependent on benefit-risk.

Recommended regimens for treatment
• Four basic regimens are currently recommended
• Completion of therapy is based on the total number of doses administered, not the duration of therapy alone
• Treatment interruptions of more than two months require another evaluation to exclude active TB before restarting therapy.
• Isoniazid alone—preferred regimen

Isoniazid alone• Daily INH for 9 months is the preferred regimen for the
treatment of LTBI for - children and adolescents (up to age 18 years). -HIV-infected persons or persons suspected of having HIV
infection. - immunocompetent adults.• Intermittent (twice weekly) INH for 9 months (DOTS)
acceptable alternative, provided all doses of therapy are directly observed.
• Six months INH alone if there are any concerns about side effects or adherence

RifampinRifampin for 4 to 6 months – Patients who cannot tolerate INH – persons exposed to cases with resistance to INH,
but susceptible to RIF.– Rifampin (RIF) alone for four months for adults.– Rifampin alone for six months for children.– Rifabutin (RFB) may be substituted for rifampin
where it cannot be given, such as in HIV-infected persons taking protease inhibitors or non-nucleoside reverse transcriptase inhibitors.

• Rifampin and pyrazinamide for two months—NOT recommended due to fatal hepatotoxicity.
Follow-up evaluation at least monthly - careful questioning - brief physical examination -assess for adherence to the regimen -symptoms and signs of adverse drug reactions.

Clinical Monitoring• Incidence of hepatitis in persons taking INH is
lower than previously thought (0.1 to 0.15%)• Hepatitis risk increases with age– Uncommon in persons < 20 years old– Nearly 2% in persons 50 to 64 years old
• Risk increased with underlying liver disease or heavy alcohol consumption

• Indications for monthly LFTs serum bilirubin and either AST or ALT– Abnormal baseline LFT– Chronic liver disease– Regular alcohol use– Current use of hepatotoxic drugs

withholding INH if– serum transaminase concentrations > 3x the
upper limit of the normal range when accompanied by symptoms
– 5x the upper limit of the normal range in asymptomatic patients.

Treatment of latent tuberculosis in special situations
Pregnancy/lactation• There is no risk of progression of LTBI to active disease
during pregnancy• treatment can be delayed until 2-3 months after delivery.• HIV-positive or other high risk factor of progression to
active disease, therapy should not be delayed on the basis of pregnancy alone, even during the first trimester.
• INH is not toxic to the unborn child, even during the first 4 months of gestation and breastfeeding is not a contraindication

HIV-infected persons• INH nine months of therapy is recommended rather
than six months.• rifampin should generally be avoided in persons who
are taking protease inhibitors (PIs) or NNRTIs.• management of persons co-infected with HIV and
LTBI can be highly complex.it has to be done by physicians who are experts in the treatment of TB and HIV.

Persons with fibrotic lesions/suspected disease• upper lobe fibronodular changes or scarring and a
positive TST (>5 mm) without evidence of active disease and no history of treatment for TB, are considered at high risk of reactivation and should receive treatment.
• evidence of healed, primary TB (i.e., calcified solitary pulmonary nodules, calcified hilar lymph nodes, and apical pleural capping) have only slightly increased risk for TB (about double that of the healthy). Their risk for TB and need for treatment of LTBI should be determined by considering other risk factors

Renal failure• at a high risk of reactivation (relative risk, 10.0-25.3) • all patients with positive reaction (10mm) are
recommended for therapy.• anergic reaction is common so that TST may not be
very sensitive to detect LTBI• In the absence of randomized trials that are specific
for this population, nine months of isonizid (INH) is recommended.

Children and adolescents• Infants and young children (younger than five years)
with LTBI are at high risk of progression to active TB. If untreated, they have up to 40% likelihood of developing active TB.
• more likely than older children and adults to develop life-threatening forms of TB, especially meningeal and disseminated disease.
• 9 months INH therapy for LTBI is more effective for children than adults, with risk reduction of 70-90%.

Liver disease• special problem, as all available regimens are
potentially hepatotoxic• Four months of RIF may be safer although the
efficacy of such a regimen has not been established.
• frequent clinical and laboratory monitoring for drug side effects is prudent.

Solid organ transplantation• very high risk of LTBI reactivation to active TB. • The incidence of infection is estimated to be 20-74 x
the general population.• Safety of INH remains a concern, especially in liver
transplant recipients, but is generally safe as long as pretreatment liver transaminase levels are normal.
• INH for nine months or RIF for four months. • Patients should be treated during the pretransplant
period, if possible.

Contacts of patients with drug-susceptible tuberculosis index case
• positive TST reactions should be treated with one of the recommended regimens.
• TST negative close contacts at high risk to develop severe active disease (e.g., children younger than five years of age) should be treated and another skin test performed a few weeks after contact has ended.
• repeat skin test is negative, the treatment should be discontinued
• Immunosuppressed persons, including HIV, with close contacts with active TB, should receive treatment, even if repeat skin testing remains negative.

Contacts of index cases with isoniazid-resistant tuberculosis
• TST-positive contacts - recommend treatment with four months of RIF
• If RIF cannot be used, rifabutin can be substituted.Contacts of patients with a multidrug-resistant
tuberculosis index case• has not been evaluated in a randomized trial• preventive therapy with two drugs to which the
organism is expected to be susceptible is recommended.

• Pyrazinamide (PZA) and ethambutol (EMB) for 6 to 12 months for adults and for 9 to 12 months for children
• PZA and fluoroquinolones (FQN) have been recommended. however, it is very poorly tolerated and is contraindicated in pediatric
• Saudi guide lines recommend FQN (levaquin or moxifloxacin) and EMB as the preferred regimen for adults.
• followed for at least two years


Management of Patient Who Missed Doses
• Extend or re-start treatment if interruptions were frequent or prolonged enough to preclude completion
• When treatment has been interrupted for more than 2 months, patient should be examined to rule out TB disease
• Recommend and arrange for DOT as needed

Case Study
Patient history
• 29-year-old saudi female
• History of diabetes
• 35 weeks pregnant
• TST = 20 mm of induration
• No symptoms of TB disease
• CXR, CBC, LFTs normal
• No known contact with TB patient

• Persons with diabetes mellitus are 2 to 4 times more likely to develop TB disease than those without diabetes
• Risk may be higher in insulin-dependent diabetics and those with poorly controlled diabetes
• Pregnancy has minimal influence on the pathogenesis of TB or the likelihood of LTBI progressing to disease
• Pregnant women should be targeted for TB testing only if they have specific risk factors for LTBI or progression to disease
management• Some experts prefer to delay treatment until after the early
postpartum period, unless the person has recent TB infection or HIV infection

Patient history
• 47-year-old indian male
• Moved to saudi arabia 4 years ago
• Known contact of infectious TB case
• TST = 5 mm of induration
• 3 months later TST = 23 mm of induration
• No symptoms of TB disease
• Normal CXR, CBC, AST, and bilirubin

• Patient is a contact of an infectious TB case• Recent entry to saudi arabia from a country with
a high prevalence of TB• Should be treated for LTBI if TST reactions 10
mm of induration• As a contact of an active TB case, 5 mm of
induration is considered positive• This patient should have been treated for LTBI
immediately after the first TST

Conclusions
Saudi Arabia is a country of medium prevalence for TB infection. The TST remains a useful tool in the identification of subjects with latent TB infection. NTM infection and BCG vaccination (routinely given in infancy) do not interfere with the interpretation of the test in adolescents and adults. Patients at high risk of developing active TB should be treated with the standard regimens advocated in this statement after due care is taken in excluding active TB disease.
