dr.aruna chaminda registrar - emergency medicine · p /c : tightening chest pain for 6 hours...
TRANSCRIPT
Dr.Aruna Chaminda
Registrar - Emergency Medicine
Patient details
Age : 29 yrs
Sex : Male
Address : Aluvihare , Matale
Marital status : Unmarried
P /C : Tightening Chest Pain for 6 hours
History of presenting Complaint :
Patient had L/sore throat for 1 day and taken treatment from GP
Sudden onset ,bilateral tightening continuous chest pain for the 6 hrs
Severe pain, not radiating, not relieved by rest
Associated with nausea and sweating ,No vomiting
Pain not increase by inspiration or changing in position.
No history of shortness of breath, no palpitation, no history of fever
No history of trauma.
Review of systems :
General:
No loss of weight No change in appetite, No malaise or weakness, No
sleep disturbance
GIT:
No abdominal pain No Diarrhea or constipation , No haematamesis or
melena
Respiratory system:
No difficulty in breathing,No cough
Genito urinary:
No burning micturition No haematuria
CNS:
No fits, No weakness
P.Medical History : No history of heart disease
hypertension,Chest pain or diabetes
P.Surgical History : No significant events
Family History : Mother has DM,No cardiac diseases
Allergic History : No food or drug allergies
Social History : Unmarried, Heavy vehicle driver,
Smoking – 3 cigarette per week
Alcohol – ¼ bottle of Arrack per week
No other substance/drug abuse
Summary :
29 years old male presented with history of bilateral tightening
chest pain for the 6 hrs, chest pain was continuous severe pain associated with nausea and sweating.

Examination :
Male with average height and built lying on bed conscious and oriented.
Temperature: 37.0 c , BMI - 19
No pallor or jaundice, mild plethora. No clubbing or splinter hemorrhages JVP not raised
No neck swelling No palpable lymph nodes
Cardiovascular examination :
Pulse: 68 b/ min regular BP: 140/ 90 mmHg
Pulses equally palpable on both sides, normal volume No radio femoral delay No lower limb or sacral edema
Apex beat in 5th intercostal space at mid clavicular line, non sustained. No thrill or heave , No local tenderness, S1 and S2 with normal intensity No gallop or murmur .
Respiratory system :
Respiratory system Chest bilaterally symmetrical moving with respiration. Vesicular breathing No crepits or ronchi
Gastrointestinal system :
Gastrointestinal system No hepatosplenomegaly
Central Nervous System
Normal sensory and motor exam
SUMMARY :
29 years old male smoker presented with history of bilateral
tightening chest pain for the 6 hrs, chest pain was continuous
severe pain associated with nausea and sweating.
On examination – Mild elevation of blood pressure and no
significant exam finding.
Differential diagnosis :
Myocardial infarction
Coronary vasospasm (Printzmetal’s angina)
Aortic dissection
Musculoskeletal pain
Pulmonary Embolism
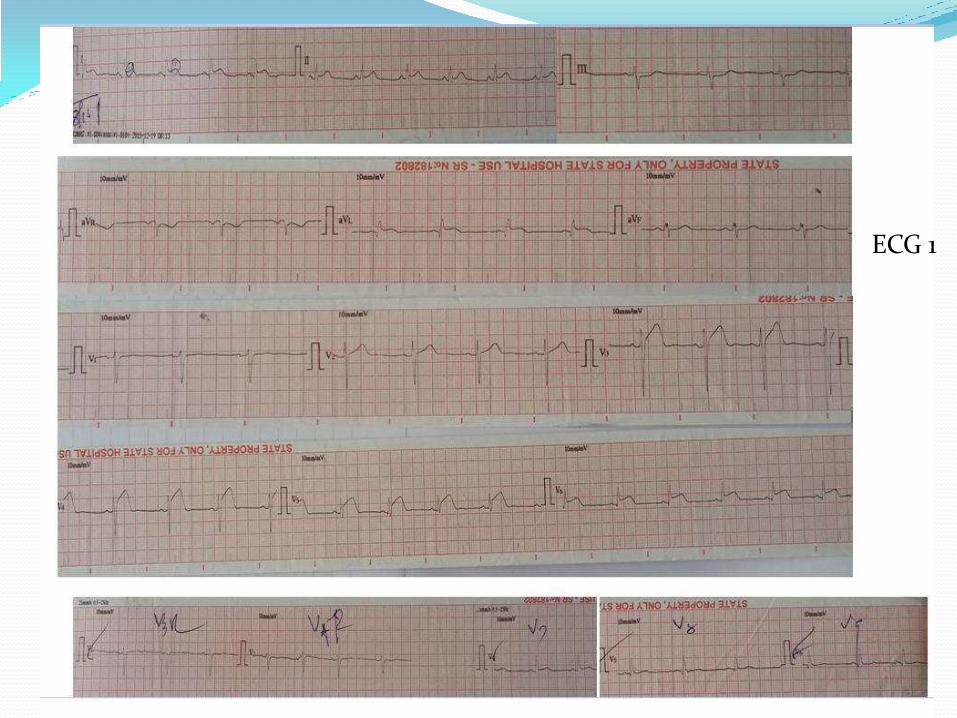
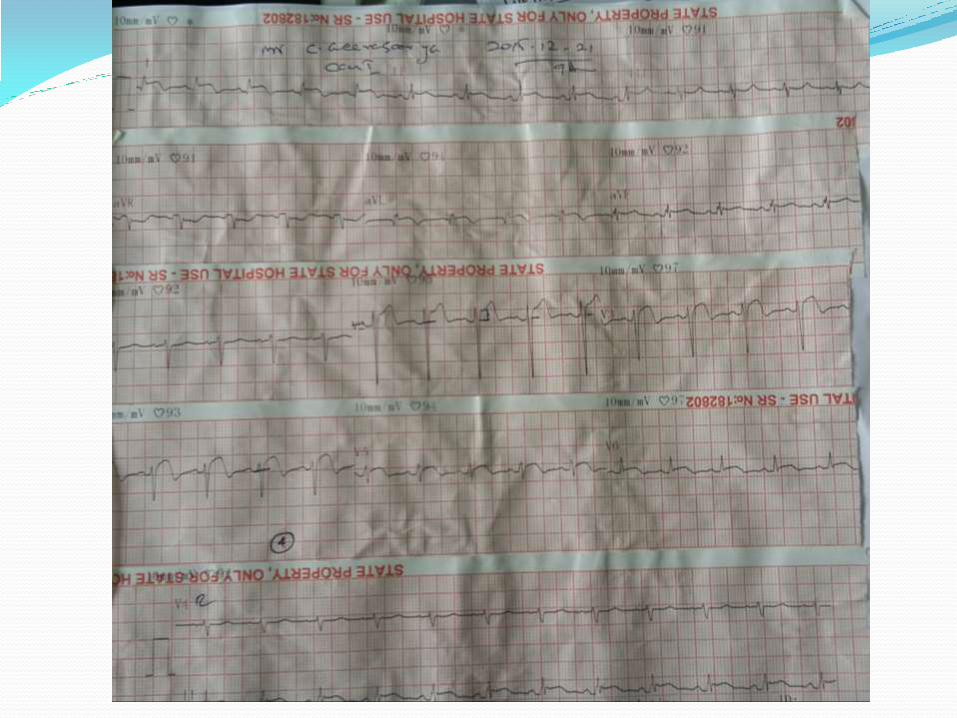
ECG 1

Patient was diagnosed as having Anterior STEMI
Patient given Aspirin 300mg
Clopidogrel 300mg
Atovastatin 40 mg
STK infusion started

ECG 2 Post STK
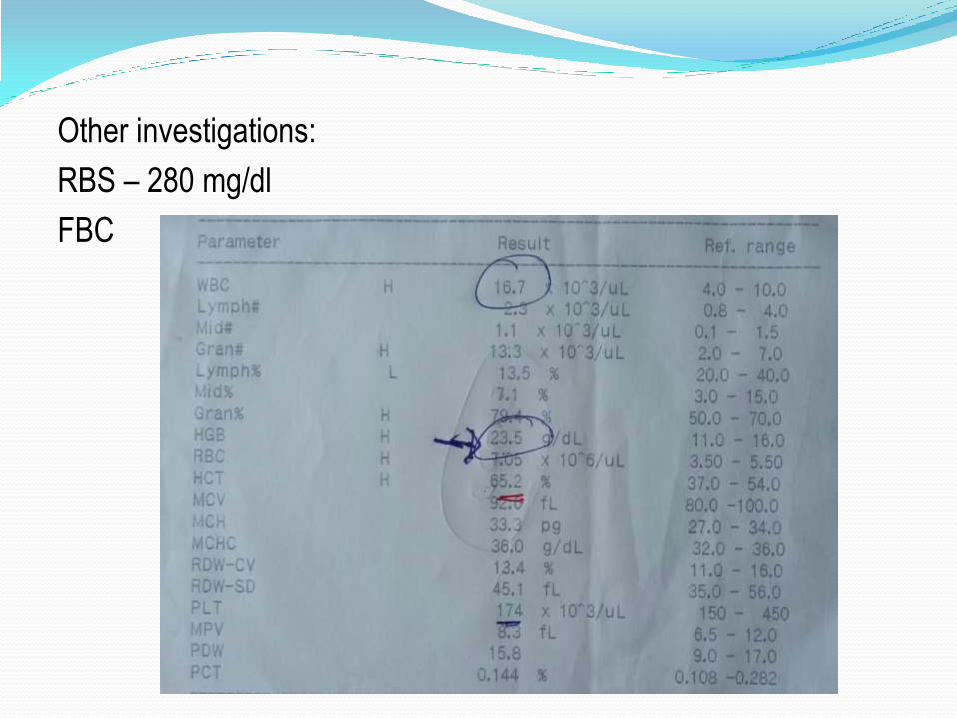
Other investigations:
RBS – 280 mg/dl
FBC
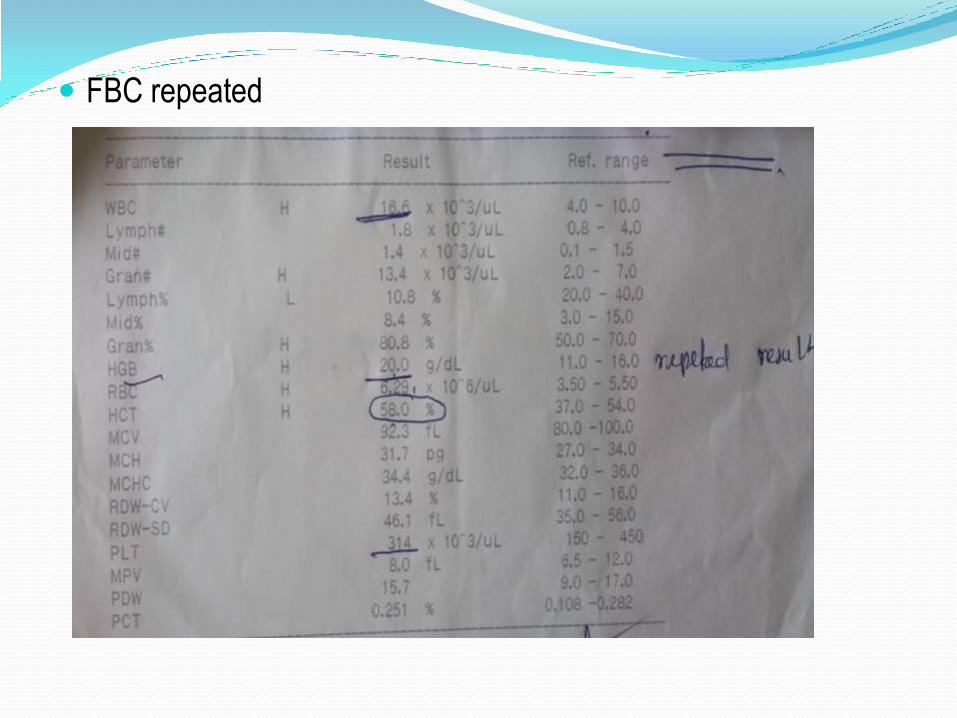
FBC repeated
Symptomatically chest pain was relived with thrombolysis and
other initial treatment and he was haemodynamically stable.
Patient was transferred to Tertiary Hospital for further
investigation and managment.
Cath lab was not functioning
Started on Enoxaparin 60mg BD
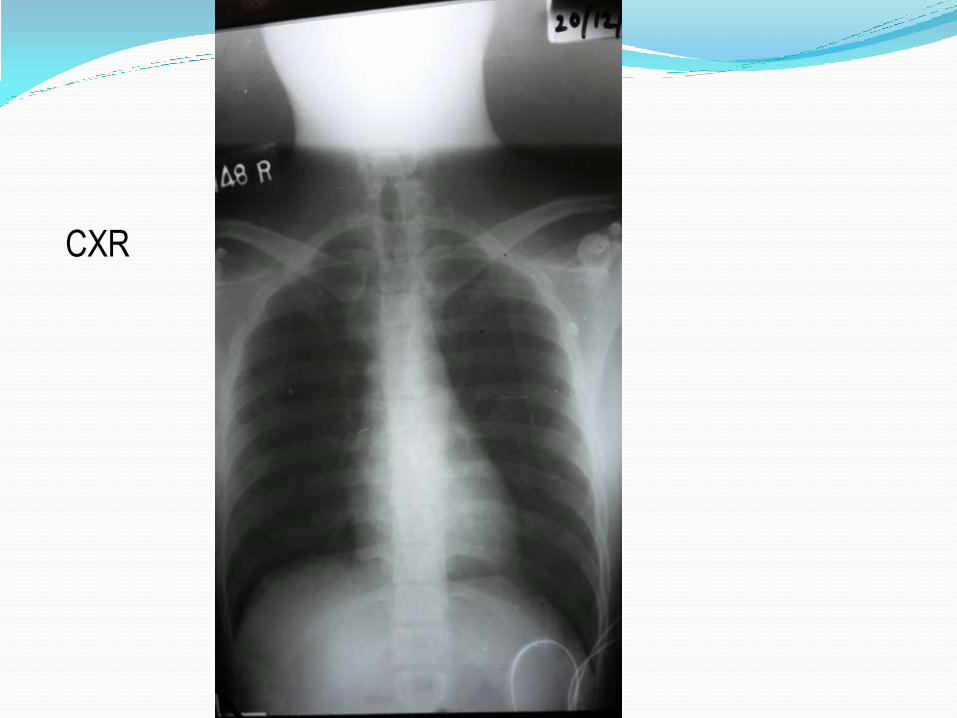
CXR
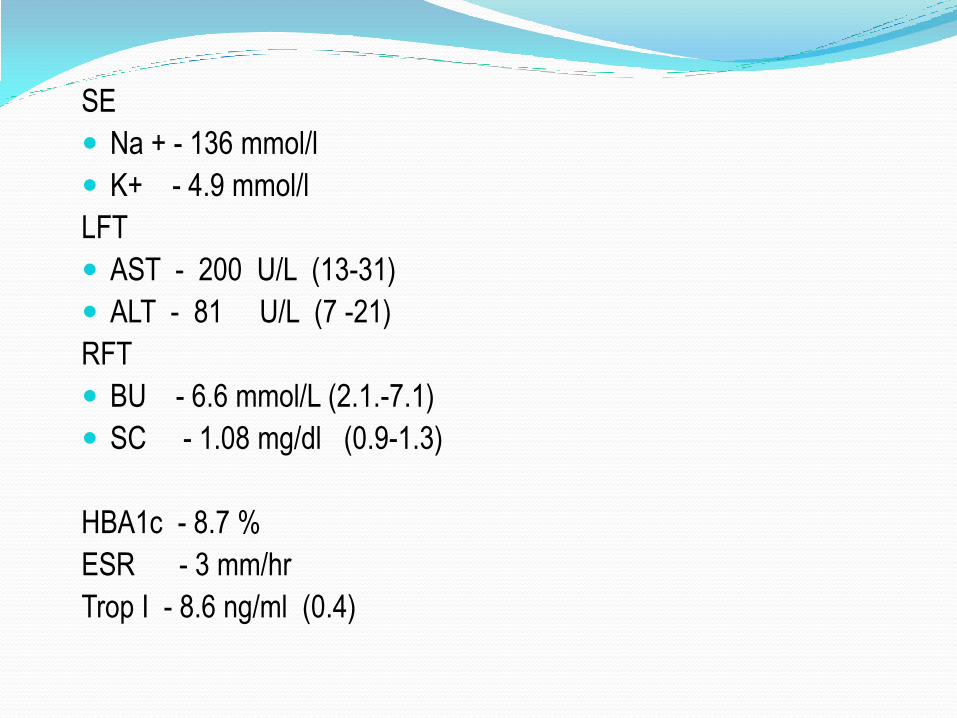
SE
Na + - 136 mmol/l
K+ - 4.9 mmol/l
LFT
AST - 200 U/L (13-31)
ALT - 81 U/L (7 -21)
RFT
BU - 6.6 mmol/L (2.1.-7.1)
SC - 1.08 mg/dl (0.9-1.3)
HBA1c - 8.7 %
ESR - 3 mm/hr
Trop I - 8.6 ng/ml (0.4)
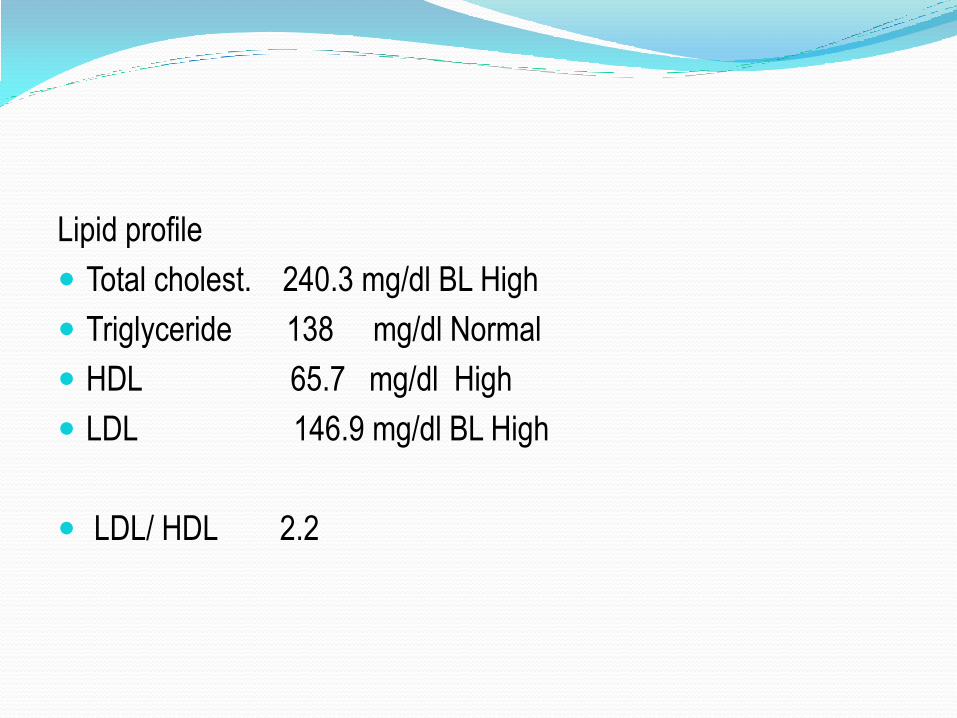
Lipid profile
Total cholest. 240.3 mg/dl BL High
Triglyceride 138 mg/dl Normal
HDL 65.7 mg/dl High
LDL 146.9 mg/dl BL High
LDL/ HDL 2.2
Blood picture
RBC - Normochromic normocytic red cells with mild red cell
crowding.
WBC – Total count elevate absolute neutrophil lekocytosis
Plt –Normal
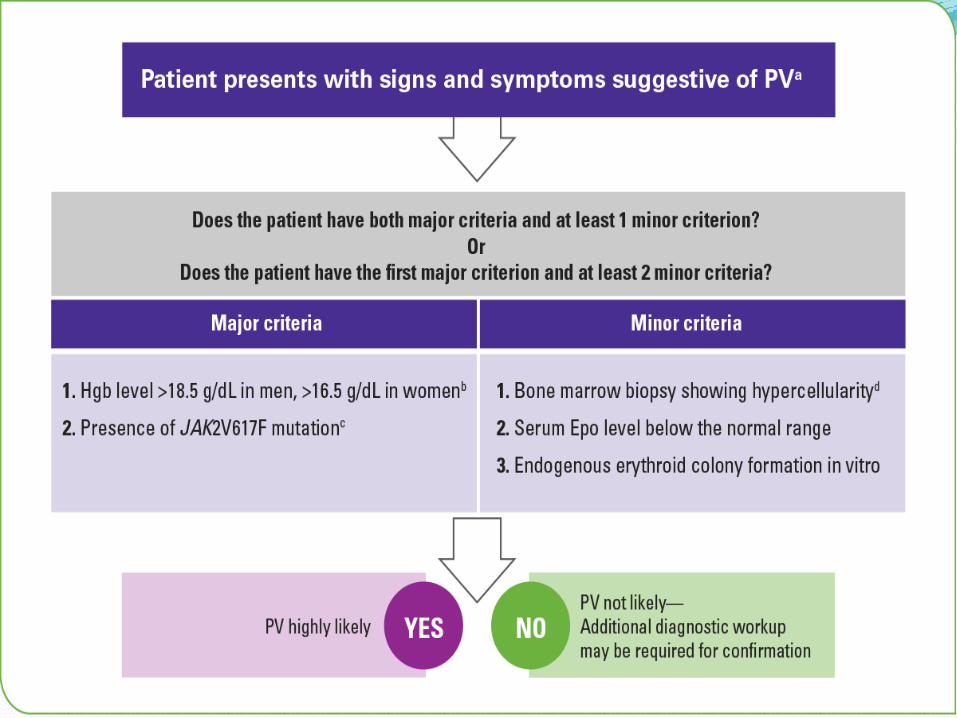
Polycythemia ? Primary or Secondary ?
Haematology and endocrinology referral done.
Isovolemic venesection done
ABG – Sample clotted repeated attempts,
SpO2 – 98% (Room air)
JAK-2 V617F mutation was Negative.
The abdominal ultrasound was normal with no
hepatosplenomegaly.
Echocardiography- EF 50% with anterior,apex and lateral wall hypokinasesia ,no intracardiac thrombus.
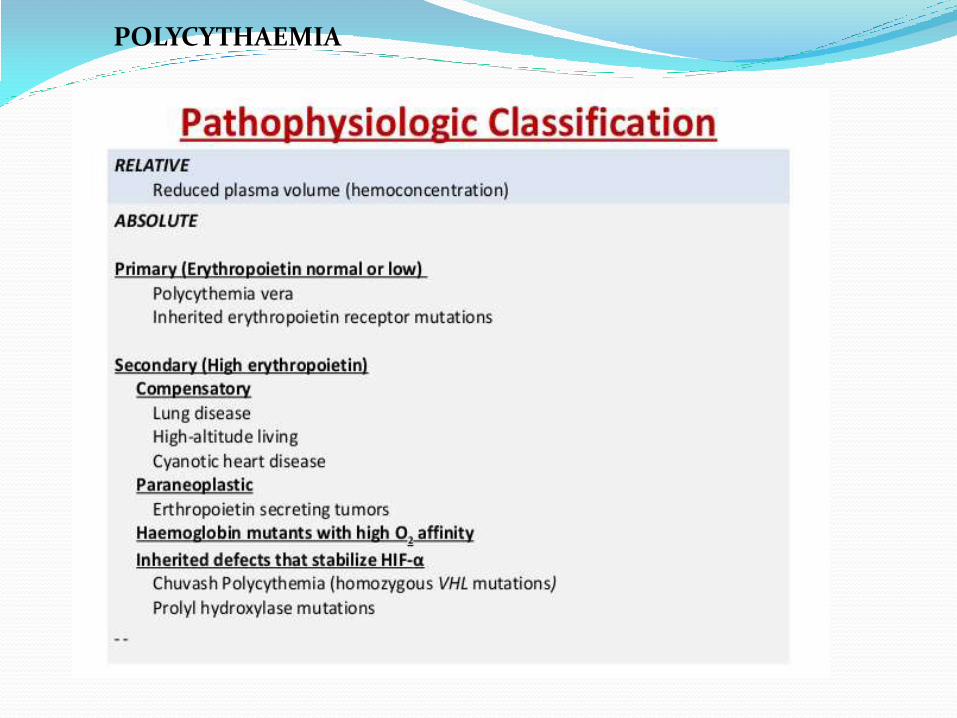
POLYCYTHAEMIA
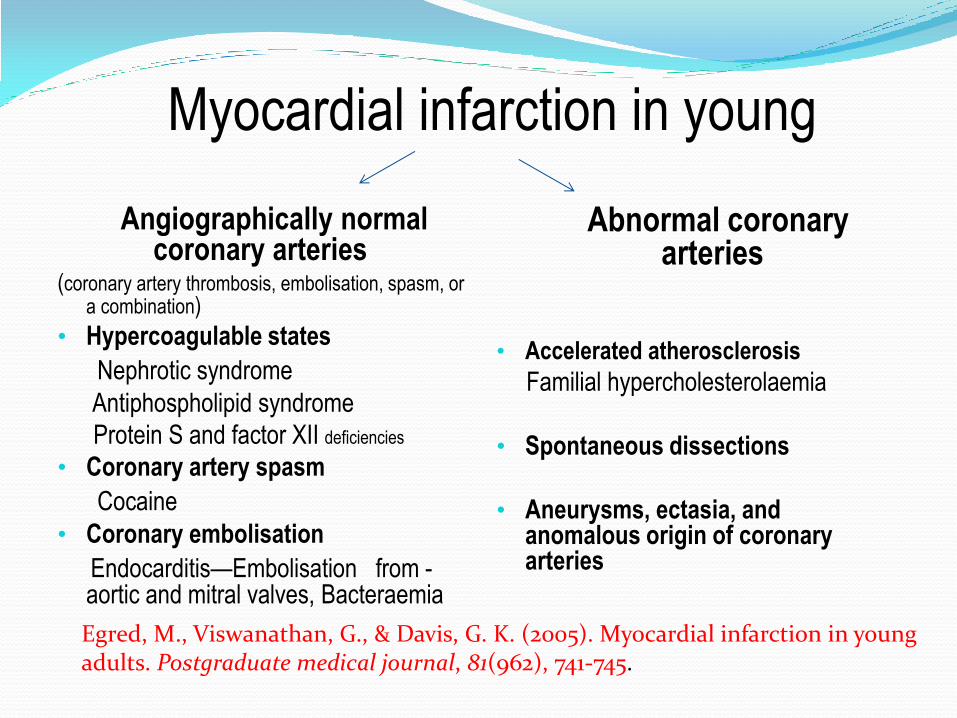
Myocardial infarction in young
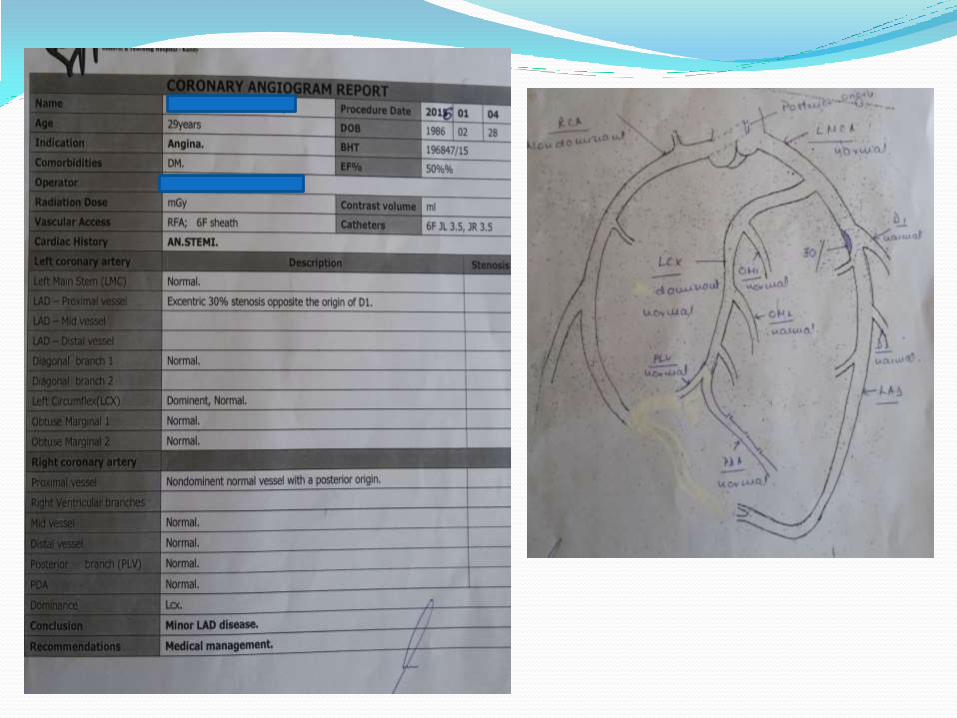
Angiographically normal coronary arteries
(coronary artery thrombosis, embolisation, spasm, or a combination)
• Hypercoagulable states
Nephrotic syndrome
Antiphospholipid syndrome
Protein S and factor XII deficiencies
• Coronary artery spasm
Cocaine
• Coronary embolisation
Endocarditis—Embolisation from - aortic and mitral valves, Bacteraemia
Abnormal coronary arteries
• Accelerated atherosclerosis
Familial hypercholesterolaemia
• Spontaneous dissections
• Aneurysms, ectasia, and anomalous origin of coronary arteries
Egred, M., Viswanathan, G., & Davis, G. K. (2005). Myocardial infarction in young adults. Postgraduate medical journal, 81(962), 741-745.
Literature review
Introduction
Diagnosis Myocardial infarction in young is challenging, as the disease is less likely, due to atherosclerosis.STEMI as first presentation of hypercoagulable state is rare.
Case reports
Presentation of Polychythaemia as AMI is very rare. There are some reports documenting PRV/Secondary Polycythaemia presenting as AMI.
Majority of cases were young males with minimal coronary occlusion.

Shah, N. C., Munir, S. M., & Alp, N. J. (2011). Spontaneous aortic thrombosis causing left main coronary occlusion in a man with secondary polycythaemia. JACC: Cardiovascular Interventions, 4(8), 934-935.
25 yrs old male with sec. polycythaemia(smoker) with a history of DVT
presented with anterolateral STEMI
Angiogram -showed a large filling defect in the left coronary
sinus that extended into the left main coronary artery
The coronary arteries were otherwise angiographically normal.
LCA -directly stented.
Bahbahani, H., Aljenaee, K., & Bella, A. (2015). Polycythemia vera presenting as acute
myocardial infarction: An unusual presentation. Journal of the Saudi Heart Association, 27(1), 57-60.
37-year-old Egyptian woman presented to A& E with severe retrosternal compressive chest pain 3 Hrs. - AMI
.
Due to the unavailability of a cardiac catheterization facility thrombolyzed with reteplase 10 units IV bolus, then 10 units given over 30 min, enoxaparin 1 mg/kg, aspirin 81 mg, clopidogrel 75 mg, lisinopril 10 mg, bisoprolol 10 mg and simvastatin 20 mg.
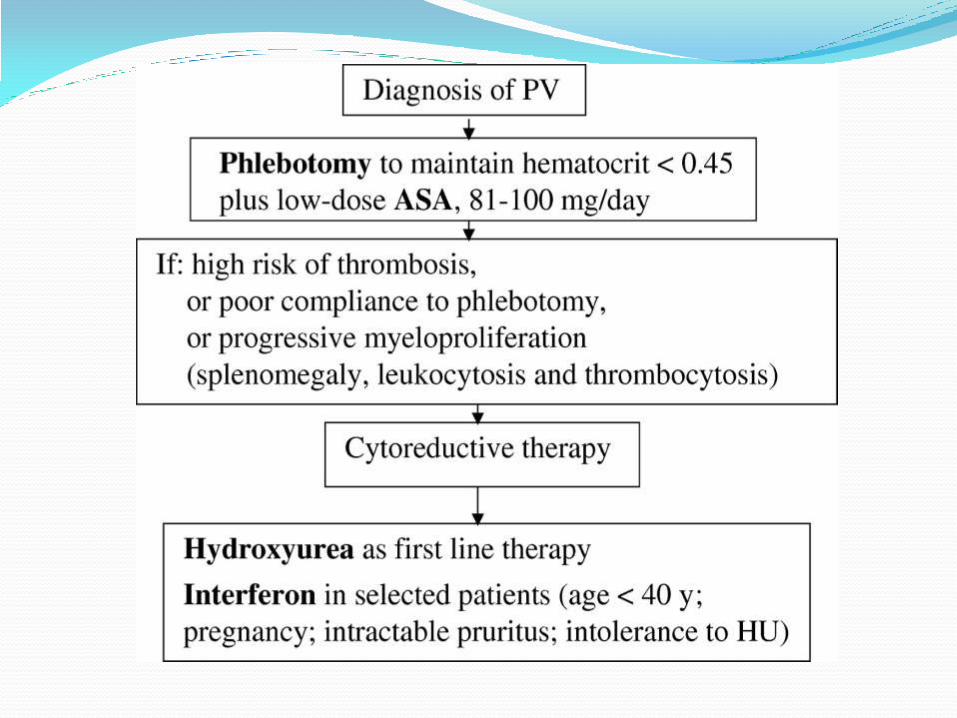
Patient was diagnosed with polycythemia vera (PV) started on
hydroxyurea 15 mg/kg, aspirin 81 mg,
regular phlebotomy to keep hematocrit less than 45%.
Four weeks later, the patient had myocardial perfusion scintigraphy, CT coronary angiography - normal.

Gouri, A., Yakhlef, A., Dekaken, A., & Bentorki, A. A. (2012, July). Acute myocardial infarction revealing a polycythemia vera. In Annales de biologie clinique (Vol. 70, No. 4, pp. 489-491).
Algeria
55-year-old man with ST-segment elevation myocardial infarction;
Treated beta-blocker,aspirin, statin, low- molecular- weight heparin and & ACE.
After stabilization patient was transferred to another hospital for angiography - stenosis and heterogeneous appearance of the anterior descending coronary artery, with apical akinesia.
Goethals P., Evrard S., Dubois C. Recurrent coronary stent thrombosis. Acta Cardiol. 2000;55(6):371–373
Goethals described the difficulty of maintaining a patent coronary artery due to repeated thrombosis
Wei, Z., Yan, Z., Yuguo, L., Rai, G. I., Duoduo, Z., Pai, L., & Jingjing, K. (2014). Acute ST-elevation myocardial infarction in a patient with polycythaemia vera. Chinese medical journal, 127(2)
Periinterventional GP IIb/IIIa antagonist treatment should be considered for patients with PV and AMI, especially for PCI. Reasonable reperfusion methods should be considered carefully including thrombus suction and intracoronary thrombolysis during PCI.
Wu, C. F., Armstrong, G. P., Henderson, R. A., & Ruygrok, P. N. (2005). Polycythaemia vera presenting as ST-elevation myocardial infarction. Heart, Lung and Circulation, 14(1), 51-53.
Wirth, L. (1960). Myocardial infarction as the initial
manifestation of polycthaemia vera. Military medicine, 125, 544.
Vacca J.B., Thoma G.E., Jr. Myocardial infarction as the initial manifestation of polycythaemia vera. AMA Arch Intern Med. 1959;103(6):974–977
Hermanns B., Handt S., Kindler J., Füzesi L. Coronary vasculopathy in polycythaemia vera. Pathol Oncol Res. 1998;4(1):37–39.
Tekin, M., Gökaslan, S., Diker, E., & Aydoğdu, S. (2008). Development of acute coronary syndrome in three patients with essential thrombocythemia or polycythemia vera. Turk Kardiyol Dern Ars, 36(1), 35-8.
Standard pharmacological treatment for myocardial infarction was effective without the need for an emergency coronary intervention
Conclusions
Young patients with myocardial infarction or ischemic stroke always look for FBC and suspect hypercoagulable state.
Early diagnosis of polycythaemia and treatment is important to prevent systemic thrombotic complications
Standard pharmacological treatment,acute coronary intervntion, periinterventional GP IIb/IIIa antagonist treatment and cytoreduction are the main current strategies for the treatment of AMI in Polycythaemia..
Myelo-proliferative disorders require special attention in maintaining the delicate balance between the risk of hemorrhage and thrombosis tendency.
However, sufficient data do not exist as to the most appropriate treatment approach to these patients, requiring further studies with larger patient groups.
