drawing blood from peripheral intravenous cannula compared ... · comes; haemolysis of blood...
TRANSCRIPT

J Adv Nurs. 2019;00:1–27. wileyonlinelibrary.com/journal/jan | 1© 2019 John Wiley & Sons Ltd
Received:18July2018 | Revised:25February2019 | Accepted:2April2019DOI: 10.1111/jan.14078
R E V I E W P A P E R
Drawing blood from peripheral intravenous cannula compared with venepuncture: A systematic review and meta‐analysis
Linda L. Coventry RN, MS, PhD, Post‐Doctoral Research Fellow1,2 | Alycia M. Jacob BA, Research Assistant3 | Hugh T. Davies RN, MS, PhD, Lecturer3 | Laurita Stoneman RN, Clinical Support Nurse, Transfusion Trainer4 | Samantha Keogh RN, BSc(Hons), PhD, Professor of Nursing2,5 | Elisabeth R. Jacob RN, MEd., PhD, Associate Dean Nursing3
1CentreforNursingResearch,SirCharlesGairdnerHospital,SchoolofNursingandMidwifery,EdithCowanUniversity,Joondalup,Perth,Australia2AllianceforVascularAccessTeachingandResearchGroup(AVATAR),MenziesHealthInstituteQueensland,GriffithUniversity,Brisbane,Queensland,Australia3SchoolofNursingandMidwifery,EdithCowanUniversity,Joondalup,Perth,Australia4BairnsdaleRegionalHealthservice,Bairnsdale,Victoria,Australia5SchoolofNursing,InstituteofHealthandBiomedicalInnovation(IHBI),QueenslandUniversityofTechnology,Brisbane,Queensland,Australia
CorrespondenceLindaCoventry,SchoolofNursingandMidwifery,Building21,EdithCowanUniversity,270JoondalupDrive,Joondalup,Perth,6027,Australia.Email:[email protected]
AbstractAims: To synthesize the evidence evaluating if blood samples are similar when obtainedfromperipheralintravenouscannulacomparedwithvenepuncture.Design: Asystematicreviewandmeta‐analysiswasundertaken.Data sources: Searcheswereconducted indatabases forEnglish languagestudiesbetweenJanuary2000–December2018.Review methods: ThesearchadheredtotheMeta‐analysisofObservationalStudiesinEpidemiologyguidelines.ThemethodologicalqualityofstudieswasassessedusingJoannaBriggscriticalappraisalinstruments.TheoverallqualityoftheevidencewasassessedusingtheGRADE.Results: Sixteenstudieswereidentified.Findingssuggesthaemolysisratesarehigherinbloodsampled fromperipheral intravenouscannula.However,haemolysis ratesmaybelowerifaperipheralintravenouscannulabloodsamplingprotocolisfollowed.Forequivalenceofblood test results,even thoughsome resultswereoutside thelaboratory,allowableerrorandwereoutsidetheBland–AltmanLevelofAgreement,noneofthesevalueswouldhaverequiredclinical intervention.Withregardtothecontaminationratesofbloodcultures,theresultswereequivocal.Conclusion: Furtherresearchisrequiredtoinformtheevidenceforbestpracticerec‐ommendations,including,ifaprotocolfordrawingbloodfromaperipheralcannulaisofbenefitforspecificpatientpopulationsandinothersettings.Impact: Venepuncture can provoke pain, anxiety and cause trauma to patients.Guidelinesrecommendbloodsamplesfromperipheralintravenouscannulabetakenonlyoninsertion.Anecdotalevidencesuggestsdrawingbloodfromexistingcannulasmaybeacommonpractice.Furtherresearchisrequiredtoresolvethisissue.
K E Y W O R D S
acutecare,adultnursing,diagnostictests,haemolysis,peripheralvenouscatheterization,phlebotomy,systematicreviewsandmeta‐analyses,venepuncture

2 | COVENTRY ET al.
1 | INTRODUC TION
Patients admitted tohospital are frequently subjected tomultipleinvasive tests including venepuncture and peripheral intravenouscannula(PIVC)insertion.Patientsmayrequiremultiplebloodteststoassistindiagnosisandmanagementofmedicalconditionsandtheappropriatemethodofobtainingthebloodsamplecanbeatopicofdebate.Venepuncturecanprovokeanxiety,bepainfulanduncom‐fortable,causebruising,haematoma,infections,vasovagalreactionsandinrarecasesperipheralnervedamage(Buowari,2013;Tsukudaetal.,2016).Intheemergencydepartment(ED)itisacommonprac‐ticeforstafftotakethebloodsamplefromaPIVCwhenanewlineisplaced.Thisreducestheneedforanadditionalpainfulvenepunc‐ture.ItisestimatedthatoverabillionPIVCsworldwideareinsertedeachyear(Alexandrouetal.,2018).
1.1 | Background
Current Australian (Clinical Excellence Commission, 2013;GovernmentofWesternAustraliaDepartmentofHealth,2017;QueenslandGovernmentDepartmentofHealth,2015)andUKnational (RoyalCollegeofNursing,2016)guidelinesstatethatbloodsamplesmaybedrawn fromaPIVCdirectlyafter inser‐tion,butnotatothertimes.Twoguidelines(Gorskietal.,2016;GovernmentofWesternAustraliaDepartmentofHealth,2017)alsostateconsiderobtainingabloodsamplefromaPIVCinanemergency,whenthepatienthas limitedvascularaccess,or isatincreasedriskofbleeding,orreceivingthrombolytictherapy.Irrespectiveofcurrentguidelines,anecdotalevidencesuggeststhatwithdrawingbloodfromPIVCmaybeacommonpractice.Patientsmayoftenneedmultipleblood tests tomonitor theircondition. Examples include the patient with gastrointestinalbleedingmayneedrepeathaemoglobin;thepatientwithacutecoronarysyndromemayneedrepeattroponin;andthepatientrequiring glucose tolerance testing requires repeat blood glu‐cosetests.
AdvantagesofwithdrawingbloodfromaPIVCincludeconve‐nienceofaccess,decreasedstaffworkload,lowcostandlesspainforthepatientduetoanadditionalvenepuncture.Disadvantagesmayincluderiskofhaemolysis,non‐equivalenceofthebloodtestresults, riskof infectionand risk to thepatencyof thecannula.Haemolysis,or redcellbreakdown,canpotentially lead to inac‐curate blood test results andmay require a secondblooddrawthat leadstodelay intreatment, increasedstaffworkload,addi‐tionalcostsandunnecessarypaintopatientsduetotherequire‐mentof repeatedblood tests. TheAmericanSocietyofClinicalPathologybenchmarkforbestpracticedefinethattheacceptablerateofsamplerejectionduetohaemolysisis2%orless(Loweetal.,2008;Phelan,Reineks,Schold,Kovach,&Venkatesh,2016).Estimatesofhaemolysisratesrangefromlessthan1‐36%(Phelanetal.,2016).
A recently published systematic review (McCaughey et al.,2017) explored differences in haemolysis rates; however, they
did not conduct meta‐analysis.We found no published system‐atic review that analysed the equivalence of blood test results.Asystematicreview(Snyderetal.,2012)examinedeffectivenessforreducingbloodculturecontaminationratesandsearchedtheliterature up to 2011, so an updatewas timely. Although blooddrawsviavenepunctureareconsideredastandardpractice,acriti‐calevaluationofthepotentialvalueofblooddrawsusingthePIVCtechniqueisrequired.Therefore,asystematicreviewincludingameta‐analysiswasconductedtogiveanevidence‐basedanswertotheresearchquestion.
2 | THE RE VIE W
2.1 | Aims
The aimof this reviewwas to synthesize the evidence evaluatingifhaemolysisrates,equivalenceofbloodresultsandcontaminationrates,betweenbloodsamplesobtainedfromPIVCarecomparablewithvenepuncture.Assuch,thisreviewquestionis:Arehaemoly‐sisrates,bloodtestresultsandcontaminationratescomparableforbloodsamplesobtainedbyPIVCandvenepunctureforpatients inacutehealthservices?
2.2 | Design
2.2.1 | Types of participants
Thisreviewincludedstudiesinvolvingadultsaged18yearsandoverwhowereadmitted inanacutecarehospital settingand requiredbloodsamplestobecollected.
2.2.2 | Types of interventions
TypesofinterventionswerestudiesthatinvestigatedtheeffectofdrawingbloodfromaPIVC.
2.2.3 | Comparator
Onlystudieswithvenepunctureasthecomparatorwereincluded.
2.2.4 | Outcome
Thisreview includedstudiesthat investigatedthefollowingout‐comes; haemolysis of blood samples, equivalenceof blood sam‐plesandcontaminationofbloodculturesamples. Itwasdecideda priori for equivalence of blood samples that only studies thatconductedBland–Altmanplotsandanalysedmeandifferencesinbloodtestresultswouldbeincluded(Bland&Altman,1986).Otheroutcomeswe considered but did not find any research onwereriskof:catheterocclusion,phlebitis,dislodgement,devicefailure,catheter‐relatedbloodstreaminfections,infiltration,blockageandcannulapatency.

| 3COVENTRY ET al.
2.2.5 | Types of studies
This review considered published observational studies includingrandomized control trials, non‐randomized control trials, quasi‐ex‐perimentalstudies,beforeandafterstudies,prospectiveandretro‐spectivecohortstudiesandanalyticalcross‐sectionalstudies.Thisreviewalsoconsidereddescriptivestudydesignsforinclusion.
2.3 | Search methods
Thesearchstrategyadheredto theMeta‐analysisofObservationalStudies in Epidemiology study guidelines (Stroup et al., 2000) andwas undertaken using the databases CINAHL, Cochrane Library,MEDLINE, Scopus, ISI Web of Science and Joanna Briggs. Twosearches were conducted. The first search (January 2000–April2017)wasperformedusingacombinationofsearchterms,includingintravenouscatheterORintravenouscannulaORperipheralvenouscatheter OR peripheral venous cannula AND phlebotomy OR ve‐nepunctureORdirectvenouspuncture.Thesecondsearch(January2000–December2018)wasperformedtoupdatetheliteratureandincluded theoutcomemeasures in the search strategy. In addition,totheabovetermswealsoincludedriskfactors,infection,phlebitis,morbidity mortality, dwell time, device failure, device malfunction,occlusion,blockage,infiltration,extravasationanddislodgementwithassociatedBoolean logic. The search strategywas adapted for the
differentdatabasesandalltermsweresearchedwithMedicalSubjectHeadingsandaskey(text)words(Appendix1&2). Inaddition,thereferencesofretrievedarticleswerecheckedandotherarticlesthatcitedtheretrievedarticleswerecheckedusingcitationalertwiththeISIWebofKnowledge.Selectionofpapersforinclusioninthestudywasundertakenindependentlybytwomembersoftheresearchteam.
WeaimedtoincludeallpublishedresearchstudiesthatwerewritteninEnglish.Studiespublishedbefore2000wereexcluded.Therationaleforthiswassuchthatthereviewreflectedthecontemporarypracticeinproductswithvascularaccessandphlebotomy.Theinvasivecomponentofmodern‐daycathetersaremuchmorepliableandsmoothcomparedwiththepolymericnatureofPIVCsbefore2000thatmayhavehadanimpactontheresults.Studieswereexcludediftheywereconductedinpaediatric(age<18years)settingsandiftherewasnodirectcomparisonbetweenbloodsamplesobtainedbyPIVCandvenepuncture.
2.4 | Search outcomes
The study selectionprocess resulted in855 studies being identifiedfromthesearchstrategy(Figure1).Basedoncomparingthetitleandabstractofthecitationagainsttheinclusioncriteria,16studieswereidentified as eligible (Barnard et al., 2016; Corbo, Fu, Silver, Atallah,& Bijur, 2007; Dietrich, 2014; Grant, 2003; Hambleton, Gomez, &BernabeuAndreu,2014;Himberger&Himberger,2001;Kelly&Klim,2013; Lowe et al., 2008; Munnix, Schellart, Gorissen, & Kleinveld,
F I G U R E 1 PRISMAflowchartofthestudyselectionandinclusionprocess
Records identified through database searching
(N = 851)
Scr
eeni
ngIn
clud
edE
ligib
ility
Iden
tific
atio
n Additional records identified through other sources
(N = 4)
Initial Literature Search(N = 855)
Possible relevant citations identifiedby literature search
(N = 716)
Studies retrieved for detailed examination
(N = 19)
Studies excluded after evaluation of title and
abstract(N = 697)
Records excluded as duplicates(N = 139)
Studies included in analysis
(N = 16)
Studies excluded
(N = 11)
Studies identified through reference
and citation checking
(N = 8)

4 | COVENTRY ET al.
TAB
LE 1
GRADEevidenceprofile–PeripheralIntravenousCannula(PIVC)comparedwithvenepuncturefordrawingblood
Cert
aint
y as
sess
men
tM
etho
d of
blo
od d
raw
Effe
ct
Cert
aint
yIm
port
ance
No
of
stud
ies
Stud
y de
sign
Risk
of b
ias
Inco
nsis
tenc
yIn
dire
ctne
ssIm
prec
isio
nO
ther
con
side
ratio
ns
Perip
hera
l In
trav
enou
s C
annu
la (P
IVC)
Vene
punc
ture
Rela
tive
(95%
CI)
Abs
olut
e (9
5% C
I)
HemolysisofbloodsamplesobtainedbyPIVCcomparedwithvenepuncture
12Observational
studies
Veryserious
aNotserious
Notserious
Notserious
Publicationbias
stronglysuspected
Verystrongassocia‐
tion
Allplausibleresidual
confoundingwould
reducethedemon‐
stratedeffect
b
5673/59032
(9.6%)
70/6091(1.1%)OR4.58
(3.61–
5.80)
39 m
ore
per
1,000
(from
29 m
ore
to52
more)
⨁⨁
◯◯
lo
wImportant
EquivalenceofbloodsamplesobtainedbyPIVCcomparedwithvenepuncture
5Observational
studies
Veryserious
cNotserious
Notserious
Notserious
Publicationbias
stronglysuspected
dTwostudiessummarizedtheresultsasoutsideofthe
laboratoryallowableerrorandoutsideBland–Altman
LOA,noneofthesevalueswouldhaverequiredclinical
intervention.Twostudiessummarizedtheresultsasall
parameterswerewithinthelaboratory'sacceptederror
orconsideredequivalentexceptforvenousbloodgases.
Onestudyfoundbloodsamplesforpotassium,bicarbo‐
nateandglucosewerenotclinicallyequivalent.
⨁◯
◯◯
ve
ry lo
wCritical
(Continues)

| 5COVENTRY ET al.
Cert
aint
y as
sess
men
tM
etho
d of
blo
od d
raw
Effe
ct
Cert
aint
yIm
port
ance
No
of
stud
ies
Stud
y de
sign
Risk
of b
ias
Inco
nsis
tenc
yIn
dire
ctne
ssIm
prec
isio
nO
ther
con
side
ratio
ns
Perip
hera
l In
trav
enou
s C
annu
la (P
IVC)
Vene
punc
ture
Rela
tive
(95%
CI)
Abs
olut
e (9
5% C
I)
ContaminationofbloodculturesobtainedbyPIVCcomparedwithvenepuncture
2Observational
studies
Serious
eVeryseriousfNotserious
Very
seriousg
Publicationbias
stronglysuspected
hOnestudyreportedbloodculturescouldbetakenac‐
curatelyfromaPIVCwhencomparedwithvenepunc‐
ture;incontrast,theotherstudyreportedtakingblood
culturesfromPIVCincreasestheriskofcontamination.
⨁◯
◯◯
ve
ry lo
wImportant
Abbreviations:CI:Confidenceinterval;OR:Oddsratio.
GRADEWorkingGroupgradesofevidence.
Highquality:Furtherresearchisveryunlikelytochangeourconfidenceintheestimateofeffect.
Moderatequality:Furtherresearchislikelytohaveanimportantimpactonourconfidenceintheestimateofeffectandmaychangetheestimate.
Lowquality:Furtherresearchisverylikelytohaveanimportantimpactonourconfidenceintheestimateofeffectandislikelytochangetheestimate.
Verylowquality:Weareveryuncertainabouttheestimate.
a Therewasahighriskofbias:astheexposure(PIVC)couldhavebeenfromaPIVConinsertion,newlyinserted,oranexistingPIVC;theoutcome(haemolysis)wasmeasureddifferently–eithervisuallyor
automated;somestudiesdidnotcontrolforconfounding.
b TheFunnelplotisnotsymmetrical,suggestingthatpublicationbiasmaybeofconcern.
c Therewasahighriskofbiasas:theexposure(PIVC)couldhavebeenfromanewlyinsertedPIVC,oranexistingPIVC;theoutcome(equivalence)wasmeasureddifferentlyamongstudies.Somedefined
clinicalacceptableintervalothersusedBland–Altman95%or99%LevelofAgreement(LOA).SomestatedthateventhoughtheresultswereoutsidetheclinicalacceptableintervalortheBland–Altman
LOAthevalueswouldnothaverequiredclinicalintervention.
d WewereonlyabletocombinethreestudiesandthusunabletodoaFunnelPlot.TheGRADEHandbookrecommends,“Itisextremelydifficulttobeconfidentthatpublicationbiasisabsentandalmost
asdifficulttoplaceathresholdonwhentoratedownqualityofevidenceduetothestrongsuspicionofpublicationbias.ForthisreasonGRADEsuggestsratingdownqualityofevidenceforpublication
biasbyamaximumofonelevel”.
e Therewasahighriskofbiasas:theexposure(PIVC)couldbefromarecentlyinsertedPIVCoranexistingPIVC.
f Therewasseriousinconsistencyintheresultsofthetwostudies.
g Therewasseriousimprecisionconsideringthesmallnumberofstudiesandwideconfidenceintervals.
h WeconductedanarrativereviewandwereunabletodoaFunnelPlot.TheGRADEHandbookrecommends,“Itisextremelydifficulttobeconfidentthatpublicationbiasisabsentandalmostasdifficult
toplaceathresholdonwhentoratedownqualityofevidenceduetothestrongsuspicionofpublicationbias.ForthisreasonGRADEsuggestsratingdownqualityofevidenceforpublicationbiasbya
maximumofonelevel”.
TAB
LE 1
(Continued)

6 | COVENTRY ET al.
TAB
LE 2
Resultsofqualityappraisal(MAStARI)
JBI c
ritic
al a
ppra
isal
che
cklis
t for
cro
ss‐s
ectio
nal s
tudi
es
Aut
hor
Crite
ria
clea
rly
defin
edSu
bjec
t and
set
‐tin
gs d
escr
ibed
Expo
sure
mea
sure
d in
va
lid a
nd re
liabl
e w
ayO
bjec
tive,
sta
nd‐
ard
crite
riaCo
nfou
ndin
g fa
c‐to
rs id
entif
ied
Stra
tegi
es fo
r con
‐fo
undi
ng fa
ctor
sO
utco
mes
mea
sure
d in
va
lid a
nd re
liabl
e w
ayA
ppro
pria
te s
ta‐
tistic
al a
naly
sis
Barnardetal.(2016)
Unclear
Yes
Unclear
Yes
Yes
Yes
Yes
Yes
Corboetal.(2007)
Yes
Yes
Yes
Yes
Unclear
Unclear
Yes
Yes
Dietrich(2014)
Unclear
Unclear
Yes
Yes
Yes
No
Yes
Yes
Grant(2003)
Yes
Yes
Yes
Yes
Yes
No
Yes
Yes
Loweetal.(2008)
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Munnixetal.(2010)
Yes
Yes
Yes
Yes
Yes
Unclear
Yes
Unclear
Ongetal.(2008)
Yes
Unclear
Unclear
Yes
Yes
Yes
Unclear
Yes
Ortells‐Abuyeetal.
(2014)
Yes
Yes
Yes
Yes
Unclear
Unclear
Yes
Yes
Phelanetal.(2018)
Unclear
Yes
Unclear
Yes
Yes
Yes
Yes
Yes
Seemannand
Reinhardt(2000)
Yes
Yes
Yes
Yes
Yes
No
Yes
Yes
Wollowitzetal.
(2013)
Unclear
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Zlotowskietal.
(2001)
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Hambletonetal.
(2014)
Yes
Yes
Yes
Yes
Unclear
Unclear
Yes
Yes
Himbergerand
Himberger(2001)
Yes
Yes
Yes
Yes
Unclear
Unclear
Yes
Yes
Selfetal.(2012)
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
KellyandKlim(2013)
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes

| 7COVENTRY ET al.
2010;Ong, Chan,& Lim, 2008;Ortells‐Abuye, Busquets‐Puigdevall,Díaz‐Bergara,Paguina‐Marcos,&Sánchez‐Pérez,2014;Phelanetal.,2018;Seemann&Reinhardt,2000;Selfetal.,2012;Wollowitz,Bijur,Esses,&Gallagher,2013;Zlotowski,Kupas,&Wood,2001).
2.5 | Quality appraisal
Studies selected for retrieval were assessed by two independentreviewers formethodological validity prior to inclusion in the re‐view.Weused thestandardizedJoannaBriggs Institute (JBI)criti‐cal appraisal instrument from the JBI Meta‐Analysis of StatisticsAssessment andReview Instrument (JBIMAStARI). Any disagree‐mentsthatarosebetweenthereviewerswereresolvedthroughdis‐cussion.Elevenstudieswereexcluded(Appendix3).
2.6 | Data abstraction
Datawere extracted from the included studies by two reviewerstocheckaccuracy.Thedataextractedincludeddetailsaboutstudyyear,studycountry,studyaim,studysetting,studydesign,interven‐tionsandcomparators.Datawereextractedseparatelyforstudiesinvestigatinghaemolysis,accuracyofbloodresultsandcontamina‐tionofbloodcultures.Dataincludedsampletype,samplesize,meth‐ods,resultsandauthorrecommendations.
2.7 | Synthesis
Meta‐analysis was conducted for studies examining haemolysis.Forrest plots were produced to display the effect measures ofeach study that were expressed as prevalence, odds ratio (OR)with95%confidenceintervals(CIs).TheORistheratiooftheoddsofhaemolysisoccurring inabloodsampleobtainedfromaPIVCcomparedwiththeoddsofhaemolysisoccurringinabloodsampleobtainedbyvenepuncture.Aratioofoneimpliesthehaemolysisof ablood sample is equally likely if obtainedbybothPIVCandvenepuncture, a ratio of greater than one implies haemolysis ismore likely inabloodsampleobtained fromPIVCanda ratioofless than one implies haemolysis is less likely if blood sample isobtainedbyPIVC.
Meta‐analysis was also conducted for three studies (Corboet al., 2007; Hambleton et al., 2014; Zlotowski et al., 2001) ex‐amining equivalence of blood results. We attempted to contactthe authors for raw data and were unsuccessful for two studies(Himberger&Himberger,2001;Ortells‐Abuyeetal.,2014).Foronestudy(Hambletonetal.,2014)weusedRevMancalculator(ReviewManager(RevMan),2014)toinputthestandarddeviationandcon‐ductstatisticalmeta‐analysis.Effectsizeswereexpressedaspooledmeandifferencesandtheir95%CI.Resultswerepooledusingfixedeffectsmodels.Heterogeneitymeasuresthevariabilityamongthecombinedstudiesandthechi‐squaretestandthe I2 statisticwereusedtoassessheterogeneity.Thepooledresultwasconsideredhet‐erogeneousifthe I2statisticwas>40%andthepvaluewas<0.05(Higgins&Green,2011).
Forsomestudiesassessingequivalenceofbloodresultsandcon‐taminationofbloodcultures,meta‐analysiscouldnotbeperformed,andthefindingshave,therefore,beenpresentedinanarrativeform.Tablesaredisplayedtoaidindatapresentationwhereverappropriate.
Publication bias may occur when studies with non‐significantfindingsarenotsubmittedbytheinvestigatororarerejectedbytheeditorsofthejournal(Gordis,2009).When10ormorestudieswerecombined,publicationbiaswasassessedusingfunnelplotsandin‐terpretedbyvisualinspection(Higgins&Green,2011).
TheoverallqualityoftheevidencewasassessedusingtheGradingof Recommendations Assessment, Development and Evaluation(GRADE)assessment(Guyattetal.,2008).AGRADEassessmentin‐cludesassessmentofriskofbias,inconsistencyofresults,indirectnessofevidence,imprecisionofresults,thelikelihoodofpublicationbias,themagnitudeoftheeffectandtheeffectofplausibleresidualcon‐founding.Theoverallqualityofthebodyoftheevidenceisthengradedashigh,moderate,loworverylow.Twoindependentreviewers(LCandHD)performedtheGRADEassessments,differenceswerediscussedandconsensusagreed(Table1).Anarrativesummaryofequivalenceofbloodresultsandcontaminationofbloodcultureswasconducted.
3 | RESULTS
3.1 | Characteristics of included studies
The16studieswerecriticallyappraised(Table2)formethodologicalqualityusingtheJBIcriticalappraisaltools.Theoverallmethodolog‐icalqualityoftheincludedstudieswasgenerallypoor.Differencesamongthestudies included ifbloodsampleswereobtainedon in‐sertion,fromanewlyinserted,oranexistingPIVC.Theoutcomeofhaemolysiscouldhavebeenmeasuredeitherbyvisualinspectionorbyautomatedspectrometry.Confoundingfactorswerenotalwaysidentified and strategies to account for confounding factorswerenotalwaysincluded.
Theaimsofthestudiescanbesummarizedasfirstlyto:examineblood sample haemolysis rates between blood samples drawn viavenepuncturecomparedwithPIVC(Barnardetal.,2016;Corboetal.,2007;Dietrich,2014;Grant,2003;Loweetal.,2008;Munnixetal.,2010;Ongetal.,2008;Ortells‐Abuyeetal.,2014;Phelanetal.,2018;Seemann&Reinhardt,2000;Wollowitzetal.,2013;Zlotowskietal.,2001).Secondly,toexamineequivalenceofbloodtestresultsbetweenbloodsamplesdrawnviaPIVCcomparedwithvenepunc‐ture (Corbo et al., 2007; Hambleton et al., 2014; Himberger &Himberger,2001;Ortells‐Abuyeetal.,2014;Zlotowskietal.,2001).Thirdly, to examine blood culture contamination between bloodsamplesdrawnviavenepuncturecomparedwithPIVC(Kelly&Klim,2013;Selfetal.,2012).
Meta‐analysiswasconductedforthestudiesexamininghaemo‐lysis.Forthestudiesassessingequivalence,meta‐analysiswascon‐ductedforthreestudies(Corboetal.,2007;Hambletonetal.,2014;Zlotowskietal.,2001).Datacouldnotbeaggregatedfortwostud‐ies (Himberger &Himberger, 2001;Ortells‐Abuye et al., 2014) ofequivalenceandthestudiesexaminingbloodculturecontamination.

8 | COVENTRY ET al.
TA B L E 3 Summaryofcharacteristicsofincludedstudies
AuthorCountry Setting Data Collection Sample type Sample size Methods
Barnardetal.(2016) UK
UniversityteachinghospitalEmergencydepartment
Prospective ConveniencesampleCollectedover3months
Bloodsamples(N=844)Bloodsample:‐ Venepuncture(N=257)
‐ PIVC(N=587)
Corboetal.(2007) USA
Urbantertiaryhospi‐talLevel1TraumaCenterAdultemergencydepartment.
ProspectiveObservationalCase–Control
ConveniencesampleCollectedover2monthsInclusion‐ ExistingPIVCsalinelock
Patients(N=81)Usablepatientsamples(N=73)
ConcurrentsamplesExisting PIVC‐ Infusionshalted2minpriortotourniquet
‐ Tourniquetproximaltointravenousline
‐ Alcoholwipe‐ 5mldiscard‐ Vacutainerusedtoaspiratebloodsample
Venepuncture‐ 21Gbutterflyneedle‐ Vacutaineradaptor
Dietrich(2014) USA
188‐bedlevelIIITraumaCentreEmergencyDepartment
ProspectiveObservational
ConveniencesampleCollectedover4‐monthperiod
Bloodsamples(N=8,944)Bloodsample:‐ OnPIVCinsertion(N=3,803)
‐ Venepuncture(N=3,301)
‐ ExistingIVcatheter(N=1,840)
Grant(2003) USA
Metropolitanteach‐inghospitalEmergencyDepartment
ProspectiveObservational
ConveniencesampleCollectedover19days
Bloodsamples(N=454)Bloodsample:‐ OnPIVCinsertion(N=255)
‐ Venepuncture(N=117)
‐ ExistingIVcatheter(N=82)
Loweetal.(2008) USA
450‐bedLevelIItraumacentreCommunityteach‐inghospitalEmergencyDepartment
ProspectiveObservational
Non‐consecutivesampleCollectedover55days
Bloodsamples(N=853)Bloodsample:‐ OnPIVCinsertion(N=498)
‐ Venepuncture(N=355)
Munnixetal.(2010) Netherlands
HospitalEmergencydepart‐ment&Outpatientclinic
ProspectiveObservational
ConveniencesampleCollectedover3months
EDPatients(N=100)OutPatients(N=50)BloodSamples(N=600)Bloodsampledrawn:‐ OnPIVCinsertion(N=400)
‐ Venepuncture(N=200)
ConsecutivepatientspecimensFourconsecutivesampleswerecollectedforeverypatient
Ongetal.(2008) Singapore
HospitalEmergencyDepartment
ProspectiveObservational
Conveniencesample Bloodsamples(N=227)Bloodsampledrawn:‐ PIVC(N=168)‐ Venepuncture(N=59)
(Continues)

| 9COVENTRY ET al.
AuthorCountry Setting Data Collection Sample type Sample size Methods
Ortells‐Abuyeetal.(2014)Spain
Reference100‐bedhospitalInpatientwardandShortStayUnit
Cross‐sectionalstudySimplecrossoverdesign
Collectedover8monthsInclusion‐WithaPIVCExclusion‐ PIVCcollectiontime>20s
‐ Difficultvenoclysis‐ Arterio‐venousfistula‐ Languagedifficulties‐ Criticalcondition‐ Alteredstateofconsciousness
Patients(N=272) ConcurrentsamplesRandomizedcollectionsequence
Existing PIVC‐ IVfluidstoppedfor15s
‐ Aspiratedanddis‐carded4mlofblood
‐ Removedbloodsample‐FlushedPIVCwith4mlofsaline
Venepuncture‐ Oppositearm‐ 21‐gaugeneedle‐ 10mlsyringe
Phelanetal.(2018) USA
UrbantertiarycarehospitalEmergencydepartment
RetrospectiveObservational
AllED‐obtainedsamplesinwhichpotassiumanalysiswascompletedCollectedover12months
Bloodsamples(54,531)Bloodsample:‐ PIVC(47,266)‐ Venepuncture(615)
SeemannandReinhardt(2000)USA
Medium‐sizedcomprehensivehealthcarefacilityInpatientmedical
ward
ProspectiveObservationalCase–Control
ConveniencesampleInclusion‐ Nocoagulopathiesorsepsis
Bloodsamples(N=34)Bloodsample:‐ ExistingPIVC(N=17)‐ Venepuncture(N=17)
Wollowitzetal.(2013)USA
UrbanacademictertiaryhospitalAdultemergencydepartment.
ProspectiveObservationalCross‐Sectional
ConveniencesampleCollectedover40days
Bloodsamples(N=4,513)Bloodsample:‐ ExistingPIVC(N=3,727
‐ Venepunctureusingabutterflyneedle(N=786)
Existing PIVC‐ClosedIVcathetersys‐tem‐dual‐port,attachedtoaBDvacutainerleurlockand8.5mlBDvacutainertube
Venepuncture‐ Butterflyneedlecollectionset(pushbuttonwith21‐or23‐gaugebutterflyneedles)
Zlotowskietal.(2001)USA
TertiaryteachinghospitalEmergencyDepartment
ProspectiveObservationalCase–Control
Inclusion‐ Healthyvolunteers.
Samplesize(N=32)Bloodsamples(N=96)
Newly inserted PIVC‐ PIVCinsertedintoupperextremity
‐ 200mlbolusofNS administeredover10min
‐ 2minwaittime‐ Tourniquetapplied‐ 18‐gaugeneedleattachedtoa20mlsyringeaspirated12mlofblood
‐ Asecondaspirateof12mlwassimilarlyaspirated
Venepuncture‐ 21‐gaugebutterfly
needle‐ Vacutainer
TA B L E 3 (Continued)
(Continues)

10 | COVENTRY ET al.
AuthorCountry Setting Data Collection Sample type Sample size Methods
Hambletonetal.(2014)Spain
UniversityhospitalEmergencydepartment
ProspectiveObservationalCase–Control
ConsecutiveenrolmentCollectedover7monthsExclusionPatientswith‐ anaemia‐ vasculardisease‐ coagulopathy‐ receivinganticoagulation
‐ immunocompromised‐ difficultvenousaccess
Pairedbloodsamples(N=259)
ConcurrentsamplesExisting Double lumen
PIVC‐ Infusionshalted2min‐ Flushedbothlumenswith1mlsaline
‐ 2minlateratourniquetwasapplied
‐ Alcoholwipe‐ 2mldiscarded‐ Vacutainerwasusedtoaspiratebloodsample
Venepuncture‐ Oppositearm‐ 21‐gaugebutterfly
needle
HimbergerandHimberger(2001)USA
MilitaryteachinghospitalRegionalLevel1TraumaCentreEmergencydepartment
ProspectiveObservationalCase–Control
ConveniencesampleCollectedover10monthsInclusion‐ Adults‐ EnglishSpeaking‐ ReceivingIVhydration
‐ NoThrombophlebitis‐ Haemodynamicallystable
‐ SBP>90mmHg‐ Capableofconsent.
Patients(N=64)Bloodsamples(N=559)
ConcurrentsamplesExisting PIVC‐ IVpaused30s‐ Tourniquetapplied‐ 30secondspause‐ 5mldiscarded‐ IVtubenotdiscon‐nectedfromhub
‐ 10mlsyringewithan18‐gaugeneedleaspi‐ratedthebloodsample
‐ 10mlsalineflushafterVenepuncture‐ Oppositearm‐ 20‐gaugeneedle
KellyandKlim(2013)Australia
CommunityTeachinghospitalEmergencydepartment
ProspectiveObservational
Collectedover7‐monthperiod
Inclusion‐ Requiredabloodculture
‐ PIVCrecentlyplaced(<1hr)
Exclusion‐ PIVCplacedbyparamedic
Samplesize(N=472) Hospitalpolicyonsterility,skincleans‐ingandbloodculturebottlepreparationwasfollowed.
Selfetal.(2012) USA
TeachingHospitalAdultemergencydepartment.
Matchedhistori‐calcohort
Collectedover12‐monthperiod
Samplesize(N=505)matchedcultures
Existing PIVC‐ Skinantisepsiswith2%chlorhexidine/70%isopropylalcoholpriortoPIVCplacement
‐ Antisepsisofthecatheterwith70%isopropyl
‐ DrawingbloodthroughthePIVC
Venepuncture‐ Skinantisepsiswith2%chlorhexidine/70%ispropylalcohol
‐ Withdrawbloodfromthevein
TA B L E 3 (Continued)

| 11COVENTRY ET al.
Therefore, a narrative review is presented, asmeta‐analysis couldnotbeperformed.
StudieswereconductedintheUSA(Corboetal.,2007;Dietrich,2014;Grant,2003;Himberger&Himberger,2001;Loweetal.,2008;Phelanetal.,2018;Seemann&Reinhardt,2000;Selfetal.,2012;Wollowitzetal.,2013),Europe(Barnardetal.,2016;Hambletonetal.,2014;Munnixetal.,2010;Ortells‐Abuyeetal.,2014),Australia(Kelly&Klim,2013)andSingapore(Ongetal.,2008).Mostofthestudieswereprospective(Barnardetal.,2016;Corboetal.,2007;Dietrich,2014;Grant,2003;Hambletonetal.,2014;Himberger&Himberger, 2001;Kelly&Klim, 2013; Lowe et al., 2008;Munnix etal.,2010;Ongetal.,2008;Ortells‐Abuyeetal.,2014;Seemann&Reinhardt,2000;Wollowitzetal.,2013;Zlotowskietal.,2001)andretrospectiveinnature(Phelanetal.,2018;Selfetal.,2012).Manystudiesusedthesamegroupofpatients,thatis,onegroupofpa‐tientshadbloodsamplesfrombothPIVCandvenepuncture(Corboetal.,2007;Hambletonetal.,2014;Himberger&Himberger,2001;Ortells‐Abuyeetal.,2014;Seemann&Reinhardt,2000;Selfetal.,2012;Zlotowskietal.,2001).Otherstudiesusedseparategroupsofpatientsforbloodsamples,thatis,onegroupofpatientsbloodwassampled fromaPIVCandaseparategroupofpatientshadbloodsampled by venepuncture (Barnard et al., 2016; Dietrich, 2014;Grant,2003;Kelly&Klim,2013;Loweetal.,2008;Munnixetal.,2010;Ongetal.,2008;Phelanetal.,2018;Wollowitzetal.,2013).
Most studies were conducted in an emergency department(Barnardetal.,2016;Corboetal.,2007;Dietrich,2014;Grant,2003;Hambletonetal.,2014;Himberger&Himberger,2001;Kelly&Klim,2013;Loweetal.,2008;Munnixetal.,2010;Ongetal.,2008;Phelanetal.,2018;Selfetal.,2012;Wollowitzetal.,2013;Zlotowskietal.,2001).Onestudywasconductedinaninpatientwardandshortstayunit (Ortells‐Abuye et al., 2014) and one study in amedicalward(Seemann&Reinhardt,2000).
Conveniencesampling(Barnardetal.,2016;Corboetal.,2007;Dietrich,2014;Grant,2003;Himberger&Himberger,2001;Kelly&
Klim,2013;Loweetal.,2008;Munnixetal.,2010;Ongetal.,2008;Phelanetal.,2018;Seemann&Reinhardt,2000;Selfetal.,2012;Wollowitzetal.,2013;Zlotowskietal.,2001)wascommonwiththreestudiesusingconsecutivesampling(Hambletonetal.,2014;Munnixetal.,2010;Ortells‐Abuyeetal.,2014).Samplesizesvariedsignifi‐cantlywith thenumberof patients beingbetween17 and54,531anddatacollectionperiodsvaryingbetween19daysand12months.A fewstudiesexcludedpatientswhowereunstableorwithmulti‐plecomorbidities(Hambletonetal.,2014;Himberger&Himberger,2001;Ortells‐Abuyeetal.,2014;Seemann&Reinhardt,2000)andonestudyonlyincludedhealthyvolunteers(Zlotowskietal.,2001).
Many studies clearly articulated protocols for collecting bloodsamples (Corbo et al., 2007;Hambleton et al., 2014;Himberger&Himberger, 2001; Kelly & Klim, 2013; Ortells‐Abuye et al., 2014;Seemann&Reinhardt,2000;Selfetal.,2012;Wollowitzetal.,2013;Zlotowski et al., 2001) and others did not. Most studies sampledbloodfromexistingPIVCs(Corboetal.,2007;Hambletonetal.,2014;Himberger&Himberger,2001;Ortells‐Abuyeetal.,2014;Seemann&Reinhardt,2000;Selfetal.,2012;Wollowitzetal.,2013);andafewstudiessampledbloodonPIVCinsertion(Loweetal.,2008;Munnixet al., 2010).Two studies (Dietrich, 2014; Grant, 2003) comparedbloodsampledfrombothexistingPIVCsandonPIVCinsertion;andtwostudies(Kelly&Klim,2013;Zlotowskietal.,2001)statedbloodwas sampled from newly inserted PIVC (Table 3).The results havebeenpresentedaccordingtostudiesinvestigatinghaemolysis,equiv‐alenceofbloodresultsandcontaminationofbloodcultures.
3.2 | Haemolysis
TheratesofhaemolysisfrombloodsamplesobtainedbetweenPIVCandvenepuncturewasreportedin10studies(Figure2).Meta‐analy‐sisfoundthattheoddsratioofhaemolysiswere4.58(CI,3.61–5.80)timesmorelikelyinbloodsamplesobtainedviaPIVCcomparedwithvenepuncture. There was evidence of both clinical and statistical
F I G U R E 2 ForestplotofstudiesusingORincomparinghaemolysisinbloodsamplestakenviaPIVCcomparedwithvenepuncture.CI,confidenceinterval;M‐H,Mantel‐Haenszel;OR,oddsratio[Colourfigurecanbeviewedatwileyonlinelibrary.com]
CI, confidence interval; M-H, Mantel-Haenszel; OR, odds ratio
Total (95%Cl)Total eventsHeterogenity: Chi2 = 33.96, df = 10 (p = 0.0002); I2 = 71%
567359032 6091 100.0% 4.58 [3.61, 5.80]
0.01Favours [PIVC] Favours [venepuncture]
0.1 1 10 100
70
Test for overall effect: z = 12.57 (p < 0.00001)
Study or SubgroupPIVC
Events EventsTotal Total WeightOdds Ratio
M-H, Fixed,95% ClOdds Ratio
M-H, Fixed,95% ClVenepuncture
Barnard 2016Corbo 2007Dietrich 2014Grant 2003Lowe 2008Munnix 2011Ong 2008Ortells-Abuye 2012Phelan 2018Seeman & Reinhart 2000Wollowitz 2013Zlotowski 2001
840
555828264110
48214
5442
58781
5643337470400168272
4726617
372764
70311040
330
210
25781
3301117354200
59272615
17786
32
7.6%
3.4%1.1%1.0%0.6%4.1%0.4%
53.6%0.3%
27.1%0.6%
5.96 [2.72, 13.09]Not estimable
10.82 [3.38, 34.61]24.11 [3.30, 176.17]22.36 [3.03, 165.16]28.38 [1.72, 4.68.06]
4.44 [1.52, 13.00]21.80 [1.27, 373.91]
2.00 [1.41, 2.85]11.67 [0.58, 235.92]
6.23 [4.00, 9.70]2.60 [0.12, 55.77]

12 | COVENTRY ET al.
heterogeneity(chi‐square=33.96,p = 0.0002; I2=71%)andassuchresults must be interpretedwith caution. Sensitivity analysis wasconductedonfivestudiesthatfollowedaprotocolforwithdrawingbloodfromaPIVC.Thefindingsweresimilar(OR6.46;95%CI,4.21–9.91).Therewasnoevidenceofheterogeneity (chi‐square=1.22,p=0.75;I2=0%).
Haemolysis was measured by either visual techniques (Grant,2003; Lowe et al., 2008; Seemann & Reinhardt, 2000), automatedtechniques (Barnardetal.,2016;Corboetal.,2007;Dietrich,2014;Munnixetal.,2010;Phelanetal.,2018;Wollowitzetal.,2013),orthemeasurementtechniquewasnotreported(Ongetal.,2008;Ortells‐Abuye et al., 2014; Zlotowski et al., 2001). Blood sample rejection
TA B L E 4 Haemolysisassessmentmethods,rejectionratesandauthorsrecommendations
Author Haemolysis Assessment Haemolysis sample rejection (haemolysis rate) Authors recommendations
Barnard etal.(2016)
HaemolysismeasuredbyspectrophotometryHaemolysisdefinedas≥30µmol/lserumHb
Totalsamplerejections:92/844(10.9%)‐ PIVC:84/587(14.3%)‐ Venepuncture:7/257(2.7%) (OR5.63;95%CI,2.49–12.73) Sub‐analyses Side of patient
‐ Right:57/450(12.7%)‐ Left:34/394(8.6)(OR0.68;95%CI,0.42–1.10)Anatomical site‐ Antecubitalfossa:50/637(7.8%)‐ Distaltoantecubitalfossa:41/207(19.8%Significant(OR2.25;95%CI,1.40–3.63)Difficulty of sampling‐ Veryeasy(comparedto):24/393(6.1%)‐ Easy:24/266(9.0%)(OR1.29;95%CI,0.69–2.35)‐ Average:20/106(18.9%)(OR2.95;95%CI,1.51–5.77)‐ Difficult/verydifficult:23/79(29.1)(OR4.36;95%CI,2.04–9.32)
Estimated tourniquet time‐ <1min(comparedto):29/416(7.0%)‐ 1–2min:49/390(12.6%)(OR1.28;95%CI,0.76–2.16)‐ >2min:13/38(34.2%)(OR2.15;95%CI,0.82–5.65)
• WherepracticableallbloodsamplesshouldbeobtainedviavenepunctureratherthanaPIVC
• Theoveralleconomicimpactofseparatingvenepunctureandinser‐tionofPIVCiscomplexandrequiresfurtherevaluation.
Corboetal.(2007)
Notreported. NohaemolysedsamplesNocomplicationsduringaspirationofPIVC
• AspiratingbloodviaPIVCisanac‐ceptablemethodofobtainingbloodsamples
Dietrich(2014)
HaemolysismeasuredbyspectrophotometrySamplesclassifiedas:Usable–haemolysis<200mg/dlRejected–haemolysis>200mg/dlAcceptablerateofsamplerejectionforhaemolysiswasdefinedas2%asperbenchmarkbestpracticebytheAmericanSocietyofClinicalPathology
Totalsamplerejections:58/8,944(0.65%) Samplerejection:‐ PIVCinsertion:41/3,803(1.1%)‐ Venepuncture:3/3,301(0.1%)‐ ExistingIVcatheters:14/1,840(0.8%)
• Measurehaemolysisusingstandard‐izedspectrophotometricmeasure‐mentratherthancolourcharts
• Levelsofhaemolysisrequiredforrejectionshouldbestandardized
• Actualcostsofdelayedlaboratoryresultsshouldbemeasuredagainsttheactualcostsofperformingad‐ditionalvenepuncturesinallpatientswhoalreadyhaveIVaccessestab‐lishedbutinwhomnoadditionalvenepunctureisnecessary.
Grant(2003)
Visual Totalsamplerejections:59/454(13%)Samplerejection:‐ EDPIVCinsertion:50/255(20%)‐ Venepuncture:1/117(<1%)‐ ExistingIVcatheters:8/82(10%) (20%vs.<1%,p<0.001)
Sub‐analysesED PIVC insertion withdrawal methodSamplerejection:‐ Vacutainer:44/195(23%)‐ Syringe:5/60(9%) (22%vs.9%,p=0.02)
• DrawbloodinEDPIVCinsertionusingasyringeinsteadofavacu‐tainerandthentransferbloodtoatubeviatheneedlessconnector
(Continues)

| 13COVENTRY ET al.
rates for haemolysis varied between collection methods: from ve‐nepuncture between 0‐6.8%; from newly inserted PIVC between0‐20%;fromexistingPIVCbetween0.8‐24.4%;andfromstudiesthatfollowed a protocol between 0‐5.6%. Two studies (Dietrich, 2014;Loweetal.,2008)reportedthattheacceptablerateofsamplerejec‐tionforhaemolysiswasdefinedbya2%benchmarkbestpracticesetbytheAmericanSocietyofClinicalPathology.
Afewstudies(Barnardetal.,2016;Grant,2003;Loweetal.,2008;Munnixetal.,2010;Ongetal.,2008;Phelanetal.,2018;Wollowitzetal.,2013)conductedsub‐analyses;however,inonestudy(Munnixetal.,2010)nostatisticalanalysiswasperformedmakingitdifficulttoascertainthesignificanceoffindings.Twostudies(Grant,2003;Ongetal.,2008)foundthattheuseofavacutainercomparedwithsyringe resulted in higher PIVC haemolysis rates and one study
(Phelanet al., 2018) foundnodifferences. Three studies (Barnardetal.,2016;Phelanetal.,2018;Wollowitzetal.,2013)foundblooddrawnfromtheantecubitalfossawerelesslikelytobehaemolysedwhencomparedwithblooddrawn fromother sites, incontrast toanotherstudy(Loweetal.,2008)whofoundnodifferencesrelatedtoblooddrawsite.Twostudies(Phelanetal.,2018;Wollowitzetal.,2013)foundthattheuseoflargergaugeneedleswerelesslikelytohavehaemolysed samples comparedwith a smaller gaugeneedle,incontrasttoanotherstudybyOngetal.,2008whofoundnodif‐ferences related toneedlegauge size.The samestudy (Wollowitzetal.,2013)alsofoundthatthebloodsamplesweremorelikelytobehaemolysed if thebloodcollectiontubewas less thanhalf full.Twostudies(Phelanetal.,2018;Wollowitzetal.,2013)foundifthetourniquet timewasgreater than1minbloodsamplesweremore
Author Haemolysis Assessment Haemolysis sample rejection (haemolysis rate) Authors recommendations
Loweetal.(2008)
HaemolysisassessedvisuallyAcceptablerateofsamplerejectionforhaemolysiswasdefinedas2%asperbenchmarkbestpracticebytheAmericanSocietyofClinicalPathology
Totalsamplerejections:29/853(3.4%)Samplerejection:‐ EDPIVCinsertion:28/470(5.6%)‐ Venepuncture:1/354(<1%) (5.6%vs.<0.3%,p=0.001)
Sub‐analysesSamplerejectionbysiteVenepuncture; PIVCAntecubital1/309(<1%);4/135(2.9%)Forearm0/18;7/140(5%)Hand0/22;12/99(12%)Multi0/1;0/0Wrist0/2;5/92(5.4%)Nosignificantdifferences
• Venepunctureshouldbethestandardofcarefordrawingbloodsampleswiththeexceptionofhigh‐acuitypatientsandpatientswhohavedifficultvenousaccess.
Munnixetal.(2010)
Haemolysismeasuredbyspectrophotometry
Totalsamplerejections16/100(16%) Samplerejection‐ PIVC:16/100(16%)‐ Venepuncture:0/50(0%)Sub‐analysis
PIVC‐ 1sttube:16/100(16%)‐ 2ndtube:4/100(4%)‐ 3rdtube:4/100(4%)‐ 4thtube:2/100(2%)Difficult PIVC placement‐ No:6/77(8%)‐ Yes:10/23(44%)
Size of needle‐ 18Gauge:5/34(15%)‐ 20Gauge:11/65(17%)Blood collection‐ Needlewithpre‐attachedholder:10/86(12%)‐ Directdrawadaptor:6/12(50%)Site of blood draw‐ Leftantecubital:4/31(13%)‐ Rightantecubital:1/23(4%)‐ Leftforearm:4/20(20%)‐ Rightforearm:2/17(12%)‐ Lefthand:2/3(67%)‐ Righthand:3/5(60%)Nostatisticalanalysesreported
• Thenumberofhaemolysedspeci‐menssenttothelaboratorycanbesignificantlyreducedbyeliminationofthefirsttubeofblood.
TA B L E 4 (Continued)
(Continues)

14 | COVENTRY ET al.
likelytobehaemolysedwithonestudy(Barnardetal.,2016)findingnodifferences.Twostudies (Barnardetal.,2016;Wollowitzetal.,2013)foundbloodsamplesweremorelikelytobehaemolysedifthevenepuncturewasdifficult(Table4).
3.3 | Equivalence of blood tests
Meta‐analysiswasconductedforthreestudies(Corboetal.,2007;Hambletonetal.,2014;Zlotowskietal.,2001) thatcompared the
Author Haemolysis Assessment Haemolysis sample rejection (haemolysis rate) Authors recommendations
Ongetal.(2008)
Haemolysisassessedusingvalidatedmethodsinabiochemistrylaboratory.
Totalsamplerejections:45/227(19.8%) Samplerejection‐ PIVC:41/168(24.4%)‐ Venepuncture:4/59(6.8%)Univariableanalysis:(OR4.4;95%CI,1.5–13.0)Univariable Sub analysis‐ Syringe:16/146(11%)‐ Vacutainer:29/81(35.8%) (OR4.5;95%CI,2.3–9.0)
Size of needle‐ ≤21G:15/86(17.4%)‐ >21G:30/141(21.3%)NotsignificantOperator‐ Registrar:2/18(11.1%)‐ Medicalofficer:22/137(16.1%)‐ Consultant:4/18(22.2%)‐ Student/nurse:17/54(31.5%)NotsignificantMultivariable analysis‐ Useofavacutainerwasassociatedwithasignificantlyhigherratesofhaemolysis(adjustedOR,6.0;95%CI,2.3–15.1)
• Drawingbloodwithavacutainerhadincreasedratesofhaemolysis
• Ifasyringeisusedtodrawblood,whetherfromIVcannulaorvenepuncture,aneedlessmethodshouldbeusedforsampletransfer.
Ortells‐Abuyeetal.(2014)
Samplerejection:‐ Venepuncture0/272(0%)‐ PIVC10/272(3.7%)
• Bloodsamplesobtainedbyve‐nepunctureandPIVCcanbeusedroutinelyformostroutinelaboratorytests
Phelanetal.(2018)
Haemolysismeasuredbyspectrophotometry Haemolysis>300serumHb=grosslyhaemolysedandsamplerejected Haemolysis>80≤300serumHb=haemolysedwithcomment
Totalsamplerejections: Combined(haemolysedwithcommentandgrosshaemolysis):5,439/54,531(10%)‐ PIVC:4,821/47,266(10.2%)‐ Venepuncture:33/615(5.4%) Significant
Sub‐analysis:PIVCSite‐ Antecubital:2,117/28,786(7.4%)‐ Peripheral:2,622/17,960(14.6%)‐ SignificantSyringe/ Vacutainer‐ Syringe:92/705(13.0%)‐ Vacutainer:1,825/16,590(11.0%)NotsignificantSize of needle‐ 16–20G:3,882/44,571(9.3%)‐ Other:939/5,633(16.7%)SignificantTourniquet time‐ >1min:532/3,832(13.9%)‐ <1min:1,362/13,162(10.3%)Significant
• Bloodsamplesobtainedbyve‐nepunctureandintheantecubitallocationareassociatedwithreducedhaemolysis
• ForbloodsamplesobtainedbyPIVCshortertourniquettimesandlargergaugeneedleareassociatedwithlowerhaemolysis
Seemannand Reinhardt(2000)
Haemolysisassessedvisually
Totalsamplerejections:4/34(11.8%) Samplerejection:‐ ExistingPIVC4/17(23.5%)‐ Venepuncture0/17(0%)
• PIVCisavalidmethodofproducingviablebloodsamples
TA B L E 4 (Continued)
(Continues)

| 15COVENTRY ET al.
Author Haemolysis Assessment Haemolysis sample rejection (haemolysis rate) Authors recommendations
Wollowitzetal.(2013)
Haemolysisassessedbymeasurementoffreeserumhaemoglobinlevels
Totalsamplerejections564/4513(12.5%) Samplerejections:‐ PIVC544/3727(14.6%)‐ Venepuncture21/786(2.7%)Sub‐analysisSite of blood draw‐ Antecubitalfossa:306/3160(9.7%)‐ Other:260/1353(19.2%)Needle/catheter gauge‐ 14–1829/373(7.8%)‐ 20406/2922(13.9%)‐ 216/322(1.9%)‐ 2315/464(3.2%)Fullness of collection tubes‐ <halffull147/639(23%)‐ ≥halffull418/3874(10.8%)Tourniquet time‐ >1min214/1221(17.5%)‐ ≤1min352/3,292(10.7%)Difficulty of venepuncture‐ Difficult224/954(23.5%)‐ Notdifficult341/3559(9.6%)
• ThemosteffectivestrategytoreducetherateofhaemolysisintheEDistousebutterflyneedlesforphlebotomyratherthanIVcatheters.
Zlotowskietal.(2001)
Haemolysisfromvenepuncture0/32(0%) HaemolysisfromPIVC2/64(3.1%)
• SupportsuseofbloodsamplesobtainedfromPIVC
TA B L E 4 (Continued)
TA B L E 5 PooledmeanandpooledmeandifferencebetweenbloodtestsobtainedbyPIVCcomparedwithvenepuncture
Studies Lab testNumber of blood tests
Pooled PIVC Mean
Pooled Venepuncture Mean
Pooled Mean Difference [95% CI]
Heterogeneity
Chi p‐value I2
Corboetal.(2007);Hambletonetal.(2014);Zlotowskietal.(2001)
Sodium(mEq/L)
728 139.3 139.2 −0.10[−0.13,0.32] 0.4 0.8 0%
Corboetal.(2007);Hambletonetal.(2014);Zlotowskietal.(2001)
Potassium(mEq/L)
728 3.9 3.9 −0.01[−0.02,0.01] 15.5 <0.001 87%
Corboetal.(2007);Hambletonetal.(2014);Zlotowskietal.(2001)
Chloride(mEq/L)
728 105.2 104.9 0.32[0.09,0.5]) 0.58 0.75 0%
Hambletonetal.(2014);Zlotowskietal.(2001)
Bicarbonate(mmol/L)
582 26.2 26.8 −0.6[−0.8,−0.4] 0.59 0.44 0%
Corboetal.(2007);Hambletonetal.(2014);Zlotowskietal.(2001)
Glucose(mg/dl) 728 116.6 116.4 0.6[−0.4,1.6] 0.88 0.64 0%
Hambletonetal.(2014);Zlotowskietal.(2001)
Albumin(g/dl) 582 3.6 3.6 −0.06[−0.17,−0.05] 0.75 0.39 0%
Corboetal.(2007);Hambletonetal.(2014)
Troponin(µg/L) 664 0.002 0.0017 0.00[−0.00,0.00] 0.79 0.37 0%
Hambletonetal.(2014);Zlotowskietal.(2001)
Hemoglobin(g/dl)
582 12.7 12.8 −0.1[−0.13,−0.07] 0.07 0.8 0%
Corboetal.(2007);Zlotowskietal.(2001)
Hematocrit(%) 210 38.5 38.7 −0.26[−1.31.0.79] 0.19 0.66 0%
Hambletonetal.(2014);Zlotowskietal.(2001)
Platelets(K/µl) 582 208.6 211.0 −2.4[−3.48,−1.32] 0.0 0.98 0%
Hambletonetal.(2014);Zlotowskietal.(2001)
INR 582 1.1 1.2 −0.01[−0.02,0.00] 0.15 0.7 0%

16 | COVENTRY ET al.
TAB
LE 6
Equivalenceofbloodresults
Aut
hor
Equi
vale
nce
Aut
hor
reco
mm
enda
tions
Aut
hor r
ecom
men
datio
ns
Corboetal.
(2007)
1. D
iffer
ence
bet
wee
n La
b te
sts a
nd n
umbe
r exc
eedi
ng C
LIA
stan
dard
s and
Bla
nd‐A
ltman
LO
A•Eventhough43/584(7.4%)couldnot
beexplainedbyallowableerrorforCLIA
and35/584(6.0%)felloutsideBland‐
AltmanLOAnoneofthesevalueswould
haverequiredclinicalintervention
•Samplesforhemocrit,electrolytes,
serumglucose,andcardiacenzymescan
betakenfromaPIVCsalinelockdevice
instablepatientsinED
LabTest
Venepuncture
Mean(+
SD)
PIVC
Mean(+
SD)
Mea
n difference
Numberexceed
National
Reco
mm
ende
d CLIARange
a N(%)
Numberexceed
Bland‐Altman95%
LOA1
SD
; N(%)
Na+(m
Eq/L
)140.1(2.9)
140.4(3.0)
−0.36
0(0)
6(8.2)
K+(m
Eq/L
)4.1(2.9)
4.1(0.4)
−0.04
4(5.5%)
2(2.7%)
CO2 (
mEq
/L)
25.5(3.9)
25.5(3.6)
−0.08
15(20.5%)
4(5.5%)
Cl‐
(mEq
/L)
106.1(3.5)
106.3(3.5)
−0.23
05(6.8%)
Glucose(m
g/dl
)115(57.0)
115.9(58.1)
−0.60
7(9.5%)
6(8.2%)
CPK(U
/L)
137.9(223.9)
142.9(224.6)
−5.019
4(5.5%)
2(2.7%)
TroponinI
(µg/
L)0.004(0.01)
0.006(0.016)
−0.0016
12(16.4%)
6(8.2%)
HCT
(%)
38.5(3.9)
38.4(4.0)
0.11
1(1.3%)
4(5.5%)
Total
43(7.4%)
35(6.0%)
2. A
spira
tion
succ
ess r
ates
Cathetersize
Numberofsuccess/
numberofattempts
(95%CI)
186/6
100(54.1–100)
2063/69
91.3(82–96.7)
224/6
66.7(22.3–95.7)
Total
73/8
190.1(81.5–95.6)
(Continues)

| 17COVENTRY ET al.
Aut
hor
Equi
vale
nce
Aut
hor
reco
mm
enda
tions
Aut
hor r
ecom
men
datio
ns
Hambleton
etal.
(2014)
1. D
iffer
ence
bet
wee
n La
b te
sts a
nd n
umbe
r exc
eedi
ng la
bora
tory
acc
epte
d sy
stem
atic
err
or a
nd B
land
‐Altm
an L
OA
•CollectingbloodsthroughPIVCisvalid
whenanalyzingformostcommonly
studiedbloodparametersinED.
•Allparametersshoweddifferences
belowthelaboratory'sacceptedsystem‐
aticerrorexceptforvenousbloodgases.
•Remainsvalidregardlessofthetypeof
druginfusionsadministered.
•Theminimumdiscardofbloodistwice
thedeadspacevolumeofthedevice.
•EDnursesshouldconsiderusingPIVCas
afirstoptionforpatients’blooddraws.
LabTest
Venepuncture
Mean(+
SD)
PIVC
Mean(+
SD)
Meandiff
Differencesbelow
thelaboratory
acceptedsystem‐
aticerror
b
Numberexceed
Bland‐Altman95%
LOA
2
SD; N(%)
Glucose
120.
812
1.4
0.66
Yes
8(3.5)
Urea
41.9
41.8
−0.05
Yes
16(7.7)
Creatinine
1.09
1.07
−0.01
Yes
7(3.0)
Na+
138.
4138.5
0.11
Yes
9(3.9)
K+3.
93.
9−0.05
Yes
11(5.1)
Cl‐
104.
9105.2
0.33
Yes
9(6.34)
Ca2+
8.8
8.7
−0.08
Yes
14(6.51)
Albumin
3.5
3.5
−0.05
Yes
15(6.64)
Amylase
51.9
52.4
−0.54
Yes
4(1.96)
CreatinKinase
152.97
157.01
4.04
Yes
1(0.5)
Bilir
ubin
0.7
0.6
−0.01
Yes
10(5.6)
pH7.
47.
40.
01Yes
4(1.78)
pCO
243
.842
.01
−1.78
No
15(6.52)
pO2
38.6
45.6
7.01
No
20(9.1)
HCO
326.6
25.97
−0.63
No
16(6.9)
Troponin
1.1
1.1
0.04
Yes
1(2.0)
Osmolality
292.
829
2.2
−0.58
Yes
2(2.6)
Leucocytes
9.1
8.99
−0.07
Yes
15(6.2)
RedBloodCells
4.3
4.3
−0.03
Yes
9(3.8)
Hemoglobin
12.7
12.6
−0.11
Yes
17(7.0)
Platlets
209.
3206.9
−2.34
Yes
16(6.6)
aPTT
33.1
32.4
−0.63
Yes
20(8.7)
INR
1.2
1.2
0.01
Yes
6(2.6)
TAB
LE 6
(Continued)
(Continues)

18 | COVENTRY ET al.
Aut
hor
Equi
vale
nce
Aut
hor
reco
mm
enda
tions
Aut
hor r
ecom
men
datio
ns
Himberger
and
Himberger,
(2001)
1. D
iffer
ence
bet
wee
n La
b te
sts a
nd n
umbe
r exc
eedi
ng la
bora
tory
clin
ical
acc
epte
d in
tern
val a
nd B
land
‐Altm
an L
OA
•Bloodscanbecollectedfromvenepunc‐
tureandPIVCinterchangeably
•Eventhoughafewvaluesexceededthe
LOAthesevalueswouldnotresultin
clinicaltreatment
•Strictadherencetoprocedureprotocols
isnecessary
•Eachspecimenshouldbemonitoredfor
haemolysis
LabTest
Venepuncture
Mean(+
SD)
PIVC
Mean(+
SD)
Mea
n difference
Numberexceed
National
Reco
mm
ende
d CLIARange
a N(%)
Numberexceed
Bland‐Altman95%
LOA1
SD
; N(%)
WBCx109 /L
Notreported
Notreported
−0.02
0/46(0%)
0(0%)
RBCx10
6 /µl
0.09
0/46(0%)
0(0%)
Hct
−1.5
0/46(0%)
2(4.4%)
Hgbg/dl
0.1
2/46(4.4%)
3(6.5%)
Pltx10
9
−0.2
1/46(2.2%)3
(6.5%)
SodiummEq/L
0.4
1/47(2.1%)
3(6.4%)
PotassiummEq/L
0.05
2/47(4.3%)
3(6.4%)
ChloridemEq/L
0.3
1/47(2.1%)
3(6.4%)
C0 2m
Eq/L
0.15
2/47(4.3%)
2(4.3%)
Glucosemg/dl
−2.44
3/47(6.4%)
2(4.3%)
Creatininemg/dl
0.17
1/47(2.1%)
2(4.3%)
SUNmg/dl
0.1
1/47(2.1%)
1(2.1%)
2.Overallsuccessrate
58/64(90.7%)ofaspirat‐
ingbloodfromaPIVC
3.Therewerenoreported
complicationswithIVsite
withanystudypar‐
ticipantsindicatingthis
isasafeandeffective
methodforobtaining
bloodspecimens
TAB
LE 6
(Continued)
(Continues)

| 19COVENTRY ET al.
Aut
hor
Equi
vale
nce
Aut
hor
reco
mm
enda
tions
Aut
hor r
ecom
men
datio
ns
Ortells‐
Abuye
etal.(2014)
1.DifferencebetweenLabtestsandnumberexceedinglaboratoryclinicalacceptedinternvalandBland‐
AltmanLOA
•VenepunctureandPIVCcanbeconsid‐
eredequivalentformostroutinelabora‐
torytestsbutnotpCO2andpO2
•Non‐equivalenceofpCO2andpO2may
beduetohandlingandtransferofblood
sampletobloodgassyringe
•IfpatientshaveexistingPIVC,usingthat
forblooddrawsispreferable
•PIVCcouldbeusedforblooddraws
inpatientswhoarebleedingorhave
infectiousdiseaseandrequiremultiple
requestsforhaemograms
LabTest
Venepuncture
Mean(+
SD)
PIVC
Mean(+
SD)
Mea
n difference
Numberexceed
National
Reco
mm
ende
d CLIARange
c N(%)
Numberexceed
Bland‐Altman95%
LOA1
SD
; N(%)
AmylaseU/L
Notreported
Notreported
Not
reported
1/265(0.4%)
1/265(0.4%)
Calciummg/dl
2/266(0.8%)
7/266(2.6)%
Totalcholesterol
12/269(4.5%)
6/269(2.2%)
Creatininemg/dl
4/271(1.5%)
4/271(1.5%)
CreatininekinaseU/L
13/262(5.0%)
9/262(3.4%)
Basalglucosemg/dl
17/271(6.3%)
9/272(3.3%)
Aspartateaminotrans‐
ferase(SGOT)U/L
7/269(2.6%)
11/269(4.1%)
PotassiummEq/L
19/269(7.1%)
13/269(4.8%)
SodiummEq/L
4/271(1.5%)
12/271(4.4%)
Ureamg/dl
9/269(3.3%)
7/269(2.6%)
Redbloodcells106/µl
3/268(1.1%)
12/268(4.5%)
Haemoglobing/dl
9/268(3.4%)
8/268(3.0%)
Leucocytes103 /µl
4/268(1.5%)
5/268(1.9%)
Platelets103/µl
3/267(1.1%)
7/267(2.6%)
Prothrombinratio(%)
22/269(8.2%)
5/269(1.9%)
VenousCO
2potentialpH
2/260(0.8%)
11/260(4.2%)
VenousCO
2partialpres‐
surepCO
2mmHg
55/260(21.2%)
10/260(3.8%)
VenousO
2partialpressure
pO2mmHg
190/260(73.1%)
10/260(3.8%)
TAB
LE 6
(Continued)
(Continues)
20 | COVENTRY ET al.
Aut
hor
Equi
vale
nce
Aut
hor
reco
mm
enda
tions
Aut
hor r
ecom
men
datio
ns
Zlotowski
etal.(2001)
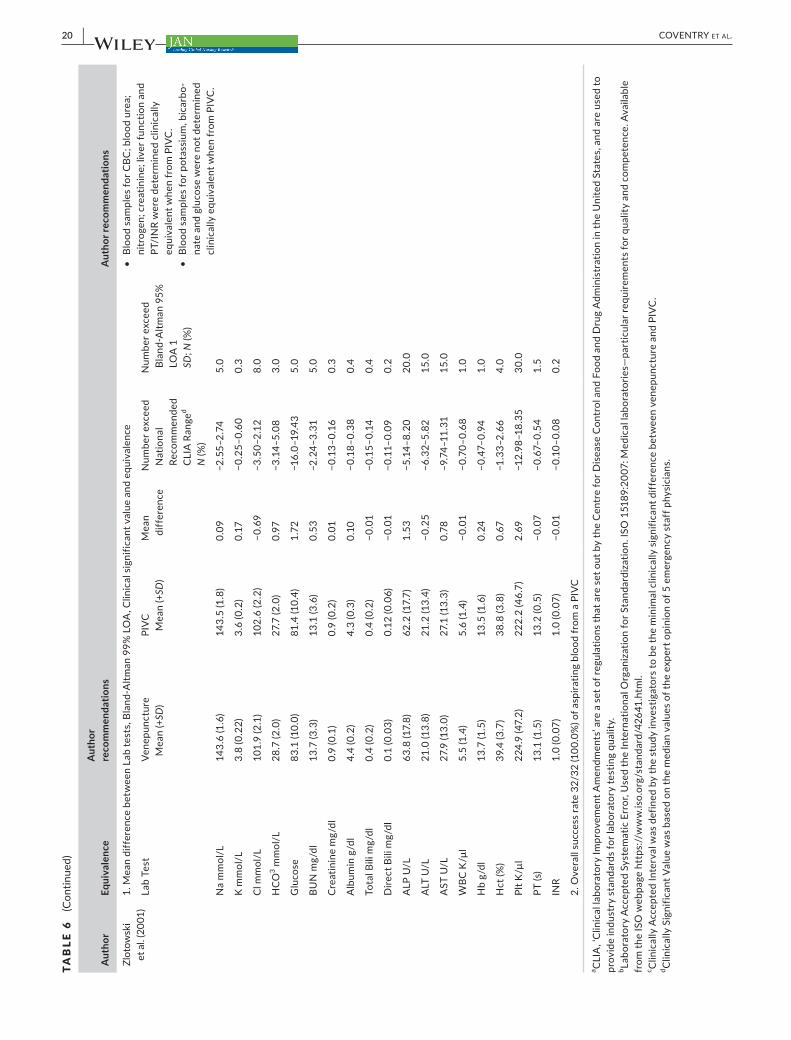
1.MeandifferencebetweenLabtests,Bland‐Altman99%LOA,Clinicalsignificantvalueandequivalence
•BloodsamplesforCBC;bloodurea;
nitrogen;creatinine;liverfunctionand
PT/INRweredeterminedclinically
equivalentwhenfromPIVC.
•Bloodsamplesforpotassium,bicarbo‐
nateandglucosewerenotdetermined
clinicallyequivalentwhenfromPIVC.
LabTest
Venepuncture
Mean(+
SD)
PIVC
Mean(+
SD)
Mea
n difference
Numberexceed
National
Reco
mm
ende
d CLIARange
d N(%)
Numberexceed
Bland‐Altman95%
LOA1
SD
; N(%)
Nammol/L
143.6(1.6)
143.5(1.8)
0.09
−2.55–2.74
5.0
Kmmol/L
3.8(0.22)
3.6(0.2)
0.17
−0.25–0.60
0.3
Cl m
mol
/L101.9(2.1)
102.6(2.2)
−0.69
−3.50–2.12
8.0
HCO
3 mm
ol/L
28.7(2.0)
27.7(2.0)
0.97
−3.14–5.08
3.0
Glucose
83.1(10.0)
81.4(10.4)
1.72
−16.0–19.43
5.0
BUNmg/dl
13.7(3.3)
13.1(3.6)
0.53
−2.24–3.31
5.0
Creatininemg/dl
0.9(0.1)
0.9(0.2)
0.01
−0.13–0.16
0.3
Albuming/dl
4.4(0.2)
4.3(0.3)
0.10
−0.18–0.38
0.4
TotalBilimg/dl
0.4(0.2)
0.4(0.2)
−0.01
−0.15–0.14
0.4
DirectBilimg/dl
0.1(0.03)
0.12(0.06)
−0.01
−0.11–0.09
0.2
ALPU/L
63.8(17.8)
62.2(17.7)
1.53
−5.14–8.20
20.0
ALTU/L
21.0(13.8)
21.2(13.4)
−0.25
−6.32–5.82
15.0
ASTU/L
27.9(13.0)
27.1(13.3)
0.78
–9.7
4–11
.31
15.0
WBCK/µl
5.5(1.4)
5.6(1.4)
−0.01
−0.70–0.68
1.0
Hbg/dl
13.7(1.5)
13.5(1.6)
0.24
−0.47–0.94
1.0
Hct(%)
39.4(3.7)
38.8(3.8)
0.67
−1.33–2.66
4.0
PltK/µl
224.9(47.2)
222.2(46.7)
2.69
−12.98–18.35
30.0
PT(s)
13.1(1.5)
13.2(0.5)
−0.07
−0.67–0.54
1.5
INR
1.0(0.07)
1.0(0.07)
−0.01
−0.10–0.08
0.2
2.Overallsuccessrate32/32(100.0%)ofaspiratingbloodfromaPIVC
a CLIA,‘ClinicallaboratoryImprovementAmendments’areasetofregulationsthataresetoutbytheCentreforDiseaseControlandFoodandDrugAdministrationintheUnitedStates,andareusedto
provideindustrystandardsforlaboratorytestingquality.
b LaboratoryAcceptedSystematicError,UsedtheInternationalOrganizationforStandardization.ISO15189:2007:Medicallaboratories—particularrequirementsforqualityandcompetence.Available
fromtheISOwebpagehttps://www.iso.org/standard/42641.html.
c ClinicallyAcceptedIntervalwasdefinedbythestudyinvestigatorstobetheminimalclinicallysignificantdifferencebetweenvenepunctureandPIVC.
d ClinicallySignificantValuewasbasedonthemedianvaluesoftheexpertopinionof5emergencystaffphysicians.
TAB
LE 6
(Continued)

| 21COVENTRY ET al.
equivalenceofbloodtestsbetweenPIVCandvenepuncture(Table5).Therewerenosignificantmeandifferencesinmostbloodtestswiththeexceptionofplateletsandbicarbonate(meanvalueswerelowerin the PIVC group compared with the venepuncture group) andchloride(meanvaluewashigher inthePIVCgroupcomparedwiththe venepuncture group). Statistical heterogeneity was not pre‐sent in any pooled analyses except potassium,where the I2 value was87%.This result showed the substantial heterogeneitywhichmustbe interpretedwithcareasthere isconsiderablevariation inthecombinedorpooledresultsanditmaybemisleadingtoreportacombinedsummarymeasure.Twostudies(Himberger&Himberger,2001;Ortells‐Abuyeetal.,2014)wereunable tobecombined formeta‐analysisandthefollowingdataareanarrativesynthesisofthefindingsofallfivestudiesreportingbloodtestequivalence.
Itisworthnotingthat,studiesdefinedtheclinicallyacceptedinter‐valdifferently;twostudies(Corboetal.,2007;Himberger&Himberger,2001)usedtheClinicalLaboratoryImprovementAmendments(CLIA),thatareasetofregulationssetoutbytheCentreforDiseaseControlandtheFoodandDrugAdministration,thatofferindustrystandardsforlaboratorytestingquality.Onestudy(Hambletonetal.,2014)usedtheLaboratoryAcceptedSystematicError;inanotherstudy(Ortells‐Abuye et al., 2014), the investigators defined the clinically accept‐ableinterval;andinthelaststudy(Zlotowskietal.,2001);anexpertpaneloffiveemergencyphysiciansdefinedtheclinicallyacceptableinterval.Similarly,fourstudies(Corboetal.,2007;Hambletonetal.,2014;Himberger&Himberger,2001;Ortells‐Abuyeetal.,2014)usedBland–Altman95%levelofagreement(LOA)andonestudy(Zlotowskietal.,2001)usedBland–Altman99%LOA.
Twostudies(Corboetal.,2007;Himberger&Himberger,2001)summarized the resultsasnot requiringclinical intervention,even
though some values were outside the laboratory allowable errorandwereoutsideBland–AltmanLOA.Onestudy(Hambletonetal.,2014)summarizedtheresultsasallparameterswerewithinthelab‐oratory's accepted error except for venous blood gases. Similarly,another study (Ortells‐Abuye et al., 2014) also summarized bloodresults,whichcouldbeconsideredequivalentwiththeexceptionofvenousbloodgases.Incontrast,onestudy(Zlotowskietal.,2001)foundbloodsamplesforpotassium,bicarbonateandglucosewerenotclinicallyequivalent.
In addition, three studies (Corbo et al., 2007;Himberger&Himberger, 2001; Zlotowski et al., 2001) reported that the as‐piration of PIVC success rates were between 90% and 100%;with one study (Corbo et al., 2007) further analysing aspira‐tion success for 18‐, 20‐ and 22‐gauge needles (100%, 91.3%,66.7% respectively). Another study (Hambleton et al., 2014)reportedbloodsamplesfromPIVCswithandwithout infusionsand venepuncture were similar; and one study (Himberger &Himberger,2001)reportednocomplicationswiththePIVCwithanyofthestudyparticipantsandconcludedwithdrawingbloodfromaPIVCwassafeandeffectivemethodofobtainingbloodsamples(Table6).
3.4 | Contamination of blood cultures
Twostudies(Kelly&Klim,2013;Selfetal.,2012)examinedtherateof contaminationofblood cultures if theblood samplewas takenfromaPIVCcomparedwithvenepuncture(Table7).Onestudy(Kelly& Klim, 2013) reported blood cultures could be taken accuratelyfromaPIVCwithin1hrofPIVCinsertionwhencomparedwithve‐nepuncture.Incontrast,theotherstudy(Selfetal.,2012)reported
TA B L E 7 Contaminationofbloodcultures
Author
Results
Author recommendationsBlood cultures
KellyandKlim(2013) 1.Numberofpositivecultures:N=65/472,(13.8%)
2.Numberoftruepositivecultures:N=49/65,(75.4%)
3.Numberoffalsepositivecultures:N=16/65,(24.6%)Falsepositiveviavenepuncture:N=8/224(3.6%) FalsepositiveviaPIVC:N=8/248(3.2%)
4.OddsratioforcontaminatedculturesinPIVC:(OR,0.9;95%CI,0.33–2.44)
• BloodculturescanbeaccuratelytakenfromaPIVCwithin1hrofinsertioninanEDwheninfectioncontrolproce‐duresarefollowed.
Selfetal.(2012) 1. Overall2.PIVCcontaminated:33/505(6.5%)3.Venepuncturecontaminated:18/505(3.6%)
4.RelativeriskofcontaminationPIVCcomparedwithvenepuncture(RR1.83;95%CI,1.08–3.11)UseofPIVCcomparedwithvenepunctureresultedin2.97(95%CI,0.29–7.51)additionalcontaminatedculturesper100culturescollected
• ThisstudysuggeststhatcollectingbloodculturesfromPIVCsincreasestheriskofcontaminationcomparedwithvenepuncture

22 | COVENTRY ET al.
takingbloodculturesfromPIVCincreasestheriskofcontaminationandfalsepositiveresultscomparedwithvenepuncture.
3.5 | Publication bias
Afunnelplotwasusedtoassesspublicationbiasforthestudiesonhaemolysis. The plot is not symmetrical, suggesting that publica‐tionbiasmaybeofconcern.Figure3displaysthefunnelplotforthepooledORofhaemolysis.
4 | DISCUSSION
Thisreviewsynthesizedthestudiesontheeffectofobtainingbloodsamples fromaPIVCcomparedwithvenepuncture.Sixteenstudiesmettheinclusioncriteria,with12studiesexamininghaemolysisrates,fivestudiesexaminingequivalenceofbloodtestresultsandtwostud‐iesexaminingcontaminationratesofbloodcultures.WedidnotfindanystudythatinvestigatedriskofbloodstreaminfectionandrisktothepatencyofthecannulaafterwithdrawingbloodsamplesfromthePIVC.Majorfindingsofthisreviewsuggestthathaemolysisratesarehigher inbloodsampledfromaPIVCcomparedwithvenepuncture.Withregardtoequivalenceofbloodtestresults,eventhoughsomere‐sultswereoutsidethelaboratoryallowableerrorandwereoutsidetheBland–AltmanLOA,noneofthesevalueswouldhaverequiredclinicalintervention.Somestudiesdidnotconsidervenousbloodgaseswereequivalentandasinglestudyfoundbloodsamplesforpotassium,bi‐carbonateandglucosewerenotclinicallyequivalent.Withregardtocontaminationratesofbloodcultures,theresultswereequivocal.
In this systematic review,we highlighted variations in draw‐ingbloodfromaPIVC(oninsertion,newlyinserted,oranexistingPIVC),inhowtheoutcomeofhaemolysiswasmeasured(visuallyorautomated)andsomestudiesdidnotcontrolforconfounding(e.g.
vacutainervs.syringe,needlegauge,siteofblooddrawnetc.).Thevisualmethodofdetectinghaemolysisissubjectiveanddependson the individual's visual acuity and colour perception (Dietrich,2014). The outcome of equivalence was measured differentlyamong the studies (e.g. clinical acceptable intervals and Bland–Altmanplots).Thesevariationscertainly impede the strengthofrecommendationsthatcanbedrawnacrossstudies.Nonetheless,there was sufficient homogeneity to allowmeta‐analysis of thestudiesofhaemolysis.
Meta‐analysis foundtheoddsofhaemolysiswere4.58timesmore likely in blood samples obtained via PIVC compared withvenepuncture.Thisfinding issimilartoothersystematicreviews(Heyeretal.,2012;McCaugheyetal.,2017).Inourstudy,haemo‐lysisratesforbloodobtainedviavenepuncturewerelowandlessthan2.7%innineof10studies.Interestingly,thehaemolysisratesforbloodobtainedviaPIVCvariedgreatlyalsobetween0%and24.4%,withfivestudies(Corboetal.,2007;Dietrich,2014;Loweetal.,2008;Ortells‐Abuyeetal.,2014;Zlotowskietal.,2001)thatfollowed a protocol forwithdrawingblood reportinghaemolysisratesbetween0‐5.6%.Eventhoughoursensitivityanalysiscon‐ductedon the five studies that followedaprotocolwere similar(OR6.46)wecontendhaemolysisrateslessthan5%areapproach‐ingtheAmericanSocietyofClinicalPathologybenchmarkof2%.Acceptinghaemolysisratesoflessthan5%inpatientsknowntobeadifficultvenepunctureorwhorequiremultipleblooddrawsmaybeconsideredapragmaticoption. Inaddition,onestudy (Grant,2003)thatreportedahighhaemolysisrate(20%)implementedaclinicalpracticechangeandencouragedphlebotomiststosamplebloodwithasyringeinsteadofavacutainerandthentransferthebloodtoatubeviaaneedlelessconnector.Audits followingthispracticechangeshowedhaemolysisrateshaddecreasedbetween4‐5%.Other variables thatmay be important regarding haemo‐lysisratesincludesiteoftheblooddrawn,theneedlegauge,the
F I G U R E 3 FunnelplotforthepooledORofhaemolysis.Abbreviations:SE(log[OR]):StandardError(logarithm[OddsRatio])[Colourfigurecanbeviewedatwileyonlinelibrary.com]
Abbreviations: SE(log[OR]): Standard Error (logarithm[Odds Ratio])
Phelan 2018 Wollowitz 2013
Barnard 2016
Ong 2008 Dietrich 2014
Zlotowski 2001Seaman 2000
Lowe 2008
Grant 2003
Munnix 2011
Ortells-Abuye 2012
OR
1001010.10.012
1.5
1
0.5
0SE(log[OR])

| 23COVENTRY ET al.
fullnessofthecollectiontube,tourniquetuseandifthevenepunc‐turewasconsidereddifficult.
Mostofthestudiesconsideredbloodsamplesfromvenepunc‐tureandPIVCwereequivalent.Irrespectiveofthelaboratoryclin‐icallyacceptederrororBland–Altmananalyses it seems logical toevaluateequivalencewithwhetherthedifferenceintestswouldre‐quireclinicalintervention.Non‐equivalenceofvenousbloodgaseshasbeensuggestedduetohandlingerror.Inthat,contactwithairmaycausechangesinbloodresults.Thebloodsampleneedstobetransferredfromasyringetoabloodgassyringe,thebloodgassy‐ringeneeds tobe filledwith thecorrectamountofbloodandex‐cessairneedstoberemoved.Thestudy(Zlotowskietal.,2001)thatreportednon‐equivalence forpotassium,bicarbonateandglucosesuggestedthismayberelatedtohaemodilution,astheycomparedtheresultsafteradministeringanormalsalinesolutionbolus.
We only found two studies that evaluated contamination ofblood cultures between venepuncture and PIVC.One study sup‐portedobtainingbloodculturesfromPIVCandtheotherstudydidnot.Consideringanothermeta‐analysis(Snyderetal.,2012)evaluat‐ingvenepuncturewithintravenouscathetersrecommendedagainstobtainingbloodfromanintravenouscatheterduetoincreasedcon‐taminationrates,wealsosupportthisrecommendation.Thismeta‐analysis(Snyderetal.,2012)wasdifferenttooursinthatitincludedintravenouscatheterscomprisingofcentrallines,arteriallinesandportacathetersandincludedstudieswithpaediatricpatients.
4.1 | Limitations
This reviewhas some limitations.Somestudiesexaminingequiva‐lenceofbloodtestresultswereexcludedastheirdataanalysesre‐portedpairedttestsandcorrelationcoefficients.Itwasdetermineda priori the most appropriate analyses were the Bland–Altmanmethod(Bland&Altman,1986).ThisreviewwaslimitedtoEnglishlanguage studies, a limitation that may also introduce bias. EventhoughwefollowedtheMeta‐analysisofObservationalStudies inEpidemiology guidelines (Stroup et al., 2000) there remains somesubjectivityinconsensusagreementforratingstudyqualityforin‐clusionandgradingtheoverallstrengthoftheevidence.
The range of settings in the reviewed studies has implicationsforclinicalandstatisticalheterogeneitywithsystematicreviewsandmeta‐analysesbutenhancesgeneralizability.Theresultsofthisreviewhavegeneralizabilitylimitedtoadultpatientsinacutecareandemer‐gencysettings.Limitationsoutsidethecontrolofthereviewauthorsincluded:allthestudieswerefromsingleinstitutions;somestudieshadsmallsamplesizes;manystudiesdidnotincludeunstablepatients;andmostofthelaboratoryresultsanalysedfellinsidethenormalrange.Inaddition,awidevarietyofpracticeswereobservedfordrawingbloodfromaPIVCandnotallstudiescontrolledforconfoundingvariables.
4.2 | Recommendations for practice
The resultsof this reviewcanhelpguide clinical practice in sev‐eral ways. This systematic review showed that five studies with
haemolysisrates lessthan5%usedaprotocoltowithdrawbloodfromaPIVCandonestudyhadlowerratesofhaemolysisafterim‐plementingaprotocoltowithdrawbloodfromaPIVC.SomeofthesuggestionsflowingonfromthisreviewuntilsupportedbyfurtherresearchsuggestthataPIVCprotocolshouldinclude:strictaseptictechnique;haltinfusionofsolutionforatleast2minpriortoblooddraw;usea20‐gaugeorlargercatheter;andthequantityofbloodtobediscardedshouldbedouble thedeadspace.Other sugges‐tionsincludedusinganeedlelessconnectortodrawbloodfromthePIVC,thusreducingtheopportunityofapotentialneedlestickin‐jury,useasyringetoaspiratethebloodnotavacutainerandavoidexcessiveaspirationforceanddonotunder‐fillthebloodtubes.
Hospitals shouldalsobeencouraged toaudithaemolysis ratesregularlyintheirdepartments,notonlytoincreasestaffawareness,but also to potentially implement clinical practice change to de‐creasehaemolysisratesifrequired.
4.3 | Recommendations for research
Large randomized controlledmultisite trials are required to defini‐tivelycompareeffectivenessofPIVCblooddrawscomparedwithve‐nepuncture.Aclusterdesignisrecommendedtoinvestigatetheeffectofablooddrawprotocol.Theclusterdesignwillmanagetheriskofcontaminationoftheblooddrawprotocolbetweentheinterventionandcontrolgroup.Allstudiesneedtoclearlyarticulate ifthebloodwassampledfromthePIVCon‐insertion,newlyinsertedorfromanexistingPIVC.ThestudiesneedtoevaluateifdrawingbloodfromaPIVCinfluencesprematurecannulafailure,causephlebitis,leadingtoblood‐streaminfectionsandeconomicanalysesshouldbeconducted.
Morestudiesarerequiredthatanalyseabnormallaboratoryval‐ues,thatis,valuesoutsidethenormalrange.Analysisofequivalenceofbloodtestresultsshouldbereportedusingclinicalacceptablelab‐oratoryerror,Bland–Altmanplotsandmoreimportantlywouldtheresultofchangedclinicaltreatment.
Further research is requiredto investigate ifdrawingbloodfromaPIVCisofbenefitforspecificpatientpopulationsandinothersettingsbesidestheemergencydepartment.Someexam‐plesincludepatientswhoareknowntobeadifficultvenepunc‐ture; who have limited venous access; require multiple blooddraws;whoareobese,dehydratedoroedematous;andpatientsonanticoagulation therapywhoareat increased riskofbleed‐ing.Moreover,therehasbeenarecentsinglestudy(Mulloy,Lee,Gregas,Hoffman,&Ashley,2018)intoadevicethatattachestothe PIVC and threads a sterile catheter through the PIVC intothe vein allowing needle‐free blood draws. This study shouldbe replicated indifferentpatientpopulationsandaneconomicanalysisconducted.
5 | CONCLUSION
Hospitalizedpatientsoftenrequiremultiplebloodteststoassistindiagnosis andmanagement of their conditions. Findings from this

24 | COVENTRY ET al.
reviewsuggestbloodsamples forPIVCcomparedwithvenepunc‐turehavehigherhaemolysisrates;however,someindividualstudiesdemonstrated that if aprotocolwas followed, these ratesmaybelower. Blood test results may be considered equivalent as differ‐ences in resultswouldnotaffectclinical treatmentandbloodcul‐turesshouldnotbetakenfromPIVC.Furthermore,drawingbloodfromPIVCsmaybethebestavailableoptioninsomepatientgroups,however,furtherresearchisrequiredtoinformtheevidenceforbestpracticerecommendations.
FUNDING S TATEMENT
Thisresearchdidnotreceiveanyspecificgrantfromfundingagen‐ciesinthepublic,commercialornot‐for‐profitsectors.
CONFLIC T OF INTERE S T
SK and LC aremembers of theAVATAR group. AVATAR researchis supported by competitive government, university, hospital andprofessional organization research grants as well as industry un‐restricted donations, investigator initiated research/educationalgrants and occasional consultancy payments from the followingcompanies: 3M, Adhezion, Angiodynamics, Bard, Baxter, BBraun,BD, Carefusion, Centurion, Cook, Entrotech, Flomedical, Hospira,Mayo,Medtronic,ResQDevices,Smiths,Teleflex,Vygon.Thismanu‐scriptisindependentlypreparedandreflectsnocommercialentitynorpromotesparticularproductsunlessthesearesupportedbyre‐searchdata.Noconflictofinteresthasbeendeclaredbytheotherauthors.
AUTHOR CONTRIBUTIONS
LC, AJ, HD, LS, SK, EJ: Made substantial contributions to con‐ception anddesign, or acquisitionof data, or analysis and inter‐pretationofdata;LC,AJ,HD,LS,SK,EJ:Involvedindraftingthemanuscriptor revising itcritically for important intellectualcon‐tent; LC,AJ,HD, LS, SK,EJ:Given final approvalof theversiontobepublished.Eachauthorshouldhaveparticipatedsufficientlyintheworktotakepublicresponsibilityforappropriateportionsofthecontent;LC,AJ,HD,LS,SK,EJ:Agreedtobeaccountablefor all aspectsof thework in ensuring thatquestions related totheaccuracyorintegrityofanypartoftheworkareappropriatelyinvestigatedandresolved.
ORCID
Linda L. Coventry https://orcid.org/0000‐0002‐3598‐9942
Alycia M. Jacob https://orcid.org/0000‐0003‐2458‐6715
Hugh T. Davies https://orcid.org/0000‐0002‐0867‐2288
Samantha Keogh https://orcid.org/0000‐0002‐2797‐4388
Elisabeth R. Jacob https://orcid.org/0000‐0002‐3506‐8422
R E FE R E N C E S
Alexandrou, E., Ray‐Barruel, G., Carr, P. J., Frost, S. A., Inwood, S.,Higgins,N.,…Rickard,C.M.;OMGStudyGroup.(2018).Useofshortperipheral intravenouscatheters:Characteristics,managementandoutcomes worldwide. Hospital Medicine, 13(5), E1–E7, https://doi.org/10.12788/jhm.3039
Barnard,E.B.G.,Potter,D.L.,Ayling,R.M.,Higginson,I.,Bailey,A.G.,&Smith,J.E. (2016).Factorsaffectingbloodsamplehaemolysis:Across‐sectional study. European Journal of Emergency Medicine, 23,143–146.https://doi.org/10.1097/mej.0000000000000195
Bland, J.M.,&Altman,D.G. (1986). Statisticalmethods for assessingagreementbetweentwomethodsofclinicalmeasurement.Lancet,1,307–310.https://doi.org/10.1016/S0140‐6736(86)90837‐8
Buowari, O. (2013). Complications of venepuncture. Advances in Bioscience and Biotechnology,4, 126–128. https://doi.org/10.4236/abb.2013.41A018
ClinicalExcellenceCommission. (2013).Guideline for PIVC insertion and post insertion care in adult patients. (GL2013_013). Sydney, NSW:NSWGovernmentHealth.Retrievedfromhttp://www1.health.nsw.gov.au/pds/ActivePDSDocuments/GL2013_013.pdf.
Corbo,J.,Fu,L.,Silver,M.,Atallah,H.,&Bijur,P.(2007).Comparisonoflaboratoryvaluesobtainedbyphlebotomyversussalinelockdevices.Academic Emergency Medicine,14,23–27.https://doi.org/10.1197/j.aem.2006.06.053
Dietrich,H. (2014).One poke or two:Can intravenous catheters pro‐videanacceptablebloodsample?Adatasetpresentation,reviewofpreviousdatasetsanddiscussion.Journal of Emergency Nursing,40,575–578.https://doi.org/10.1016/j.jen.2012.11.002
Gordis,L.(2009).Epidemiology(4thed).Philidelphia:SaundersElsevier.Gorski,L.,Hadaway,L.,Hagle,M.E.,McGoldrick,M.,Orr,M.,&Doellman,
D. (2016). Infusion Therapy Standards of Practice (Vol.39 Supp 1S).Norwood,MA:InfusionNursesSociety.
Government of Western Australia Department of Health. (2017).Insertion and management of peripheral intravenous cannulae in Western Australian Healthcare Facilities Policy. Western Australia:Department of Health. Retrieved from http://www.health.wa.gov.au/circularsnew/pdfs/13345.pdf.
Grant,M.S.(2003).TheeffectofblooddrawingtechniquesandequipmentonthehemolysisofEDlaboratorybloodsamples.Journal of Emergency Nursing,29(2),116–121.https://doi.org/10.1067/men.2003.66
Guyatt,G.H.,Oxman,A.D.,Vist,G.E.,Kunz,R.,Falck‐Ytter,Y.,Alonso‐Coello,P.,&Schünemann,H.J.(2008).GRADE:Anemergingconsen‐susonratingqualityofevidenceandstrengthofrecommendations.BMJ,336,924–926.https://doi.org/10.1136/bmj.39489.470347.AD
Hambleton, V. L., Gomez, I. A., & Bernabeu Andreu, F. A. (2014).Venipuncture versus peripheral catheter: Do infusions alter labo‐ratoryresults?Journal of Emergency Nursing,40,20–26.https://doi.org/10.1016/j.jen.2012.03.014
Heyer,N.J.,Derzon,J.H.,Winges,L.,Shaw,C.,Mass,D.,Snyder,S.R.,…Liebow,E.B.(2012).Effectivenessofpracticestoreducebloodsam‐plehemolysisinEDs:Alaboratorymedicinebestpracticessystem‐aticreviewandmeta‐analysis.Clinical Biochemistry,45,1012–1032.https://doi.org/10.1016/j.clinbiochem.2012.08.002
Higgins,J.P.T.,&Green,S.(Eds).(2011).Cochrane handbook for systmatic reviews of interventions version 5.1.0[updatedMarch2011].Retrievedfromhttp://handbook.cochrane.org.
Himberger,J.R.,&Himberger,L.C.(2001).Issuesinaccuracyoflabora‐toryresults.Accuracyofdrawingbloodthroughinfusingintravenouslines.Heart & Lung: The Journal of Acute and Critical Care,30,66–73.https://doi.org/10.1067/mhl.2001.110535
Kelly,A.‐M.,&Klim,S.(2013).Takingbloodculturesfromanewlyestab‐lished intravenous catheter in the emergency department does notincreasetherateofcontaminatedbloodcultures.Emergency Medicine Australasia,25,435–438.https://doi.org/10.1111/1742‐6723.12121

| 25COVENTRY ET al.
Lowe, G., Stike, R., Pollack, M., Bosley, J., O'Brien, P., Hake, A., …Stover, T. (2008). Nursing blood specimen collection techniquesandhemolysis rates in anemergencydepartment:Analysisof ve‐nipuncture versus intravenous catheter collection techniques.Journal of Emergency Nursing,34, 26–32. https://doi.org/10.1016/ j.jen.2007.02.006
McCaughey,E.J.,Vecellio,E.,Lake,R.,Li,L.,Burnett,L.,Chesher,D.,…Georgiou,A.(2017).Keyfactorsinfluencingtheincidenceofhemoly‐sis:Acriticalappraisalofcurrentevidence.Critical Reviews in Clinical Laboratory Sciences, 54, 59–72. https://doi.org/10.1080/10408363.2016.1250247
Mulloy,D.F.,Lee,S.M.,Gregas,M.,Hoffman,K.,&Ashley,S.W.(2018).EffectofperipheralIVbasedbloodcollectiononcatheterdwelltime,bloodcollectionandpatientresponse.Applied Nursing Research,40,76–79.https://doi.org/10.1016/j.apnr.2017.12.006
Munnix, I.C.A., Schellart,M.,Gorissen,C.,&Kleinveld,H.A. (2010).Factors reducinghemolysis rates inbloodsamples from theemer‐gency department. Clinical Chemistry and Laboratory Medicine, 49,157–158.https://doi.org/10.1515/CCLM.2011.012
Ong,M.E.H.,Chan,Y.H.,&Lim,C.S. (2008).Observationalstudytodetermine factors associatedwithblood samplehaemolysis in theemergency department.Annals Academy of Medicine Singapore,37,745–748.
Ortells‐Abuye, N., Busquets‐Puigdevall, T., Díaz‐Bergara,M., Paguina‐Marcos,M.,&Sánchez‐Pérez, I. (2014).A cross‐sectional study tocomparetwobloodcollectionmethods:Directvenouspunctureandperipheralvenouscatheter.British Medical Journal Open,4,e004250.https://doi.org/10.1136/bmjopen‐2013‐004250
Phelan,M.P.,Reineks,E.Z.,Schold,J.D.,Hustey,F.M.,Chamberlin,J.,&Procop,G.W. (2018).Preanalytic factorsassociatedwithhemo‐lysisinemergencydepartmentbloodsamples.Archives of Pathology and Laboratory Medicine, 142, 229–235. https://doi.org/10.5858/arpa.2016‐0400‐OA
Phelan,M.P.,Reineks,E.Z.,Schold,J.D.,Kovach,A.,&Venkatesh,A.(2016). Estimated national volume of laboratory results affectedby hemolyzed specimens from emergency departments. Archives of Pathology and Laboratory Medicine, 140, 621–621. https://doi.org/10.5858/arpa.2015‐0434‐LE
Queensland Government Department of Health (2015). Guideline Peripheral intravenous catheter (PIVC). Brisbane Queensland:Queensland Health. Retrieved from https://www.health.qld.gov.au/__data/assets/pdf_file/0025/444490/icare‐pivc‐guideline.pdf
Review Manager (RevMan). (2014). (Version 5.3). Copenhagen: TheNordicCochraneCentre,T.C.C.
RoyalCollegeofNursing. (2016).Standards for infusion therapy,4thed.London,UK:RoyalCollegeofNursing.
Seemann, S., & Reinhardt, A. (2000). Blood sample collection from aperipheral catheter system compared with phlebotomy. Journal of Intravenous Nursing,23,290–297.
Self,W. H., Speroff, T., McNaughton, C. D.,Wright, P.W., Miller, G.,Johnson, J. G., … Talbot, T. R. (2012). Blood culture collectionthroughperipheralintravenouscathetersincreasestheriskofspec‐imen contamination among adult emergency department patients.Infection Control and Hospital Epidemiology,33,524–526.https://doi.org/10.1086/665319
Snyder, S.R., Favoretto,A.M.,Baetz,R.A.,Derzon, J.H.,Madison,B.M.,Mass,D.,…Liebow,E.B.(2012).Effectivenessofpracticesto reduce blood culture contamination: A Laboratory MedicineBest Practices systematic review and meta‐analysis. Clinical Biochemistry, 45, 999–1011. https://doi.org/10.1016/j.clinbiochem.2012.06.007
Stroup,D.,Berlin,J.,Morton,S.,Olkin,I.,Williamson,D.,Rennie,D.,&Thacker,S.(2000).Meta‐analysisofobservationalstudiesinepide‐miology aproposal for reporting. JAMA,283, 2008–2012. https://doi.org/10.1001/jama.283.15.2008
Tsukuda, Y., Funakoshi, T., Nasuhara, Y., Nagano, Y., Shimizu, C., &Iwasaki,N.(2016).Venipuncturenerveinjuriesintheupperextrem‐ityfrommorethan1millionprocedures.Journal of Patient Safety,1.https://doi.org/10.1097/PTS.0000000000000264
Wollowitz,A.,Bijur,P.,Esses,D.,&Gallagher,J.(2013).Useofbutterflyneedles to draw blood is independentlyly associatedwithmarkedreductioninhemolysiscomparedtointravenouscatheter.Academic Emergency Medicine, 20, 1151–1155. https://doi.org/10.1111/acem.12245
Zlotowski,S.J.,Kupas,D.F.,&Wood,G.C.(2001).Comparisonoflab‐oratory values obtained bymeans of routine venipuncture versusperipheralintravenouscatheterafteranormalsalinesolutionbolus.Annals of Emergency Medicine,38,497–504.https://doi.org/10.1067/mem.2001.118015
How to cite this article:CoventryLL,JacobAM,DaviesHT,StonemanL,KeoghS,JacobER.Drawingbloodfromperipheralintravenouscannulacomparedwithvenepuncture:Asystematicreviewandmeta‐analysis.J Adv Nurs. 2019;00:1–27. https://doi.org/10.1111/jan.14078
APPENDIX 1ELEC TRONIC DATABA SE FIRS T SE ARCH S TR ATEGY ( JANUARY 20 0 0 –APRIL 2017)
MEDLINE search strategy(((MH“phlebotomy”))OR(“directvenouspuncture”)OR(“venepunc‐ture”)AND((MH“cannula”))OR((MH“Catheter”))OR(“intravenouscannula*”) OR (“intravenous catheter*”) OR (“peripheral venouscatheter*”)OR(“peripheralvenouscannula*”)OR(“peripheralcath‐eter*”)OR(“peripheralcannula*”))
CINAHL search strategy(((MH“phlebotomy”))OR(“directvenouspuncture”)OR(“venepunc‐ture”)AND((MH“cannula”))OR((MH“Catheter”))OR(“intravenouscannula*”) OR (“intravenous catheter*”) OR (“peripheral venouscatheter*”)OR(“peripheralvenouscannula*”)OR(“peripheralcath‐eter*”)OR(“peripheralcannula*”))
Cochrane Library(((MH“Phlebotomy”))OR(“venipuncture*”)AND((MH“Catheters”))OR(Cannula)or((MH“Catheterization”))or(PeripheralCatheterization*))
ScopusKeywords((Phlebotomy))OR (venepuncture)) ((Catheter*)OR (Intravenous
Catheter))
ISI Web of Science
TS=(Phlebotom* OR Venepuncture* OR Direct Venous Puncture)ANDTS=(Catheter*OR“IntravenousCatheter*”ORCatheteriz*)
Joanna Briggs (OVID)(sh(BloodSpecimenCollection)OR(Phlebotomy)OR(Venipuncture))AND(sh(Catheter*)OR(Cannula))

26 | COVENTRY ET al.
APPENDIX 2
ELEC TRONIC DATABA SE SECOND SE ARCH S TR ATEGY (1 JANUARY 20 0 0 –31 DECEMBER 2018)
MEDLINE search strategy(((MH“phlebotomy”))OR(“directvenouspuncture”)OR(“venepunc‐ture”)AND((MH“cannula”))OR((MH“Catheter”))OR(“intravenouscannula*”)OR(“intravenouscatheter*”)OR(“peripheralvenouscath‐eter*”)OR(“peripheralvenouscannula*”)OR(“peripheralcatheter*”)OR(“peripheralcannula*”))AND“occlusion”OR(MH“phlebitis”)OR“dislodge*”OR“failure”OR“devicefailure”OR“infection*”OR(MH“Catheter‐Related Infections”)OR “Infiltration”OR “extravasation”OR “blockage” OR “leakage” OR “he#molysis” OR “accuracy” OR“equivalence”OR“contamination”
CINAHL search strategy((MH "Venipuncture") OR (MH "Phlebotomy") OR "venepunctureor venipuncture or phlebotomy") AND ((MH "Catheterization,Peripheral +") OR "catheteri#ation, peripheral" OR "peripheralintravenous catheter" OR "peripheral venous cannula" OR "pe‐ripheral venousdevice"OR "pivc"OR "piv")AND ((MH"CatheterOcclusion +") OR "occlusion" OR (MH "phlebitis+") OR phlebitisOR"dislodgement"ORfailureOR"devicefailure"OR"devicemal‐function"OR(MH"Catheter‐RelatedBloodstreamInfections")OR(MH "Catheter‐Related Infections")OR infectionOR "infiltration"OR"extravasation"OR"blockage"OR"leakage"OR"he#molysisofbloodsamples"OR"he#molysis inbloodtesting"OR"accuracy inbloodtest"OR"equivalenceinbloodtests"OR"contaminationofbloodcultures")
Cochrane Library(MH “Phlebotomy”) OR “venipuncture*”AND (MH “Catheters”) OR“Cannula” or (MH “Catheterization”) or (Peripheral Catheterization*)AND “occlusion” OR (MH “phlebitis”) OR “dislodge*” OR “failure”OR “infection*” OR “Infiltration” OR “extravasation” OR “blockage”OR “leakage”OR “he#molysis”OR “accuracy”OR “equivalence”OR“contamination”
Scopus("Phlebotomy" OR "venepuncture") AND ("Catheter*" OR"Intravenous Catheter") AND ("occlusion" OR "phlebitis" OR "dis‐lodge*"OR"failure"OR"infection*"OR"Infiltration"OR"extravasa‐tion"OR "blockage"OR "leakage"OR "he#molysis"OR "accuracy"OR"equivalence"OR"contamination")
IS I Web of ScienceTS=(Phlebotom* OR Venepuncture* OR Direct Venous Puncture)ANDTS=(Catheter*ORIntravenousCatheter*ORCatheteriz*)ANDTS=(occlusionORphlebitisORdislodge*ORfailureORinfection*ORInfiltrationORextravasationORblockageORleakageORhemolysisORhaemolysisORaccuracyORequivalenceORcontamination)
Joanna Briggs (OVID)(Blood SpecimenCollection)OR (Phlebotomy)OR (Venipuncture))AND(Catheter*)OR(Cannula))AND((occlusionORphlebitisORdis‐lodge*ORfailureORinfection*ORInfiltrationORextravasationORblockageORleakageORhemolysisORhaemolysisORaccuracyORequivalenceORcontamination)
APPENDIX 3
E XCLUDED S TUDIE S AND RE A SONS FOR E XCLUSION
Alexandrou, E., Ray‐Barruel, G., Carr, P. J., Frost, S., Inwood, S.,Higgins,N., Rickard,C.M. (2015). International prevalence of theuseofperipheralintravenouscatheters.Journal of Hospital Medicine, 10(8),530‐533.https://doi.org/10.1002/jhm.2389Reasonforexclusion:Nodirectcomparisonbetweenthegroups,
PIVCandvenepuncture.Burns,E.R.,&Yoshikawa,N.(2002).HemolysisinSerumSamples
Drawn by Emergency Department Personnel versus LaboratoryPhlebotomists. Laboratory Medicine, 33(5), 378‐380. https://doi.org/10.1309/PGM4‐4F8L‐2P1M‐LKPBReason for exclusion: The first part of the study compared ED
with non‐ED setting – unable to ascertain if the comparisonwasbetweenPIVCandvenepuncture.Thesecondpartofthestudyin‐cludedpaediatricpatients.Carraro,P.,Servidio,G.,&Plebani,M.(2000).Hemolyzedspeci‐
mens:areasonforrejectionoraclinicalchallenge?Clinical Chemistry, 46(2),306‐307.Reason for exclusion: Unclear if they compared between the
groups,PIVCandvenepuncture.Cox,S.R.,Dages,J.H.,Jarjoura,D.,&Hazelett,S.(2004).Blood
samples drawn from IV catheters have less hemolysiswhen5‐mL(vs10‐mL)collectiontubesareused.Journal of Emergency Nursing, 30(6),529‐533.https://doi.org/10.1016/j.jen.2004.10.004Reasonforexclusion:Nodirectcomparisonbetweenthegroups,
PIVCandvenepuncture.Dugan,L.,Leech,L.,Speroni,K.G.,&Corriher,J.(2005).Factors
affectinghemolysisratesinbloodsamplesdrawnfromnewlyplacedIV sites in the emergency department. JEN: Journal of Emergency Nursing, 31(4),338‐418.https://doi.org/10.1016/j.jen.2005.05.004Reasonforexclusion:Nodirectcomparisonbetweenthegroups,
PIVCandvenepuncture.Dwyer, D. G., Fry, M., Somerville, A., & Holdgate, A. (2006).
Randomized,singleblindedcontroltrialcomparinghaemolysisratebetween two cannula aspiration techniques. Emergency Medicine Australasia, 18(5‐6),484‐488.https://doi.org/10.1111/j.1742‐6723. 2006.00895.xReasonforexclusion:Nodirectcomparisonbetweenthegroups,
PIVCandvenepuncture.Everts,R. J.,Vinson,E.N.,Adholla,P.O.,&Reller,L.B. (2001).
Contamination of catheter‐drawn blood cultures. Journal of Clinical Microbiology, 39(9), 3393‐3394. https://doi.org/10.1128/JCM.39.9.3393‐3394.2001

| 27COVENTRY ET al.
Reason for exclusion: Contained data on an excluded group(paediatrics).Fang, L., Fang, S. H., Chung, Y. H., & Chien, S. T. (2008).
Collecting factors related to the haemolysis of blood speci‐mens. Journal of Clinical Nursing, 17(17), 2343‐2351. https://doi.org/10.1111/j.1365‐2702.2006.02057.xReason for exclusion: Contained data on an excluded group
(paediatrics).Prue‐Owens,K.(2006).Useofperipheralvenousaccessdevices
forobtainingblood samples formeasurementofActivatedPartialThromboplastinTimes.Critical Care Nurse, 26(1), 30–38.Reasonforexclusion:Dataanalysisdidnot includeBland–Altman
plots.
Straszewski,S.,Sanchez,L.,McGillicuddy,D.,Boyd,K.,DuFresne,J.,Joyce,N.,...Mottley,J.(2011).UseofseparatevenipuncturesforIVaccessandlaboratorystudiesdecreaseshemolysisrates.Internal and Emergency Medicine, 6,357‐359.Reasonforexclusion:Thisstudyevaluatedapolicychange–we
were unsure if in the baseline data collection if blood could havebeencollectedbyeithervenepunctureorfromaPIVC.Zengin,N.,&Enç,N.(2008).Comparisonoftwobloodsampling
methods in anticoagulation therapy: venipuncture and peripheralvenouscatheter.Journal of Clinical Nursing, 17(3),386‐393.https://doi.org/10.1111/j.1365‐2702.2006.01858.xReasonforexclusion:Dataanalysisdidnot includemeandiffer‐
enceandBland–Altmanplots.
TheJournal of Advanced Nursing (JAN)isaninternational,peer‐reviewed,scientificjournal.JANcontributestotheadvancementofevidence‐basednursing,midwiferyandhealthcarebydisseminatinghighqualityresearchandscholarshipofcontemporaryrelevanceandwithpotentialtoadvanceknowledge for practice, education, management or policy. JAN publishes research reviews, original research reports and methodological andtheoreticalpapers.
Forfurtherinformation,pleasevisitJANontheWileyOnlineLibrarywebsite:www.wileyonlinelibrary.com/journal/jan
Reasons to publish your work in JAN:
• High-impact forum:theworld’smostcitednursingjournal,withanImpactFactorof1.998–ranked12/114inthe2016ISIJournalCitationReports©(Nursing(SocialScience)).
• Most read nursing journal in the world:over3millionarticlesdownloadedonlineperyearandaccessibleinover10,000librariesworldwide(includingover3,500indevelopingcountrieswithfreeorlowcostaccess).
• Fast and easy online submission: onlinesubmissionathttp://mc.manuscriptcentral.com/jan.• Positive publishing experience:rapiddouble‐blindpeerreviewwithconstructivefeedback.• Rapid online publication in five weeks:averagetimefromfinalmanuscriptarrivinginproductiontoonlinepublication.• Online Open:theoptiontopaytomakeyourarticlefreelyandopenlyaccessibletonon‐subscribersuponpublicationonWileyOnlineLibrary,aswellastheoptiontodepositthearticleinyourownoryourfundingagency’spreferredarchive(e.g.PubMed).