drug-drug interactions that really matter – focus on ... · grÜnenthal name der präsentation...
TRANSCRIPT

GRÜNENTHAL Name der Präsentation Datum GRÜNENTHAL Page 1
Drug-drug interactions that really matter – focus on transporters AGAH Annual Meeting 2014 │13 Mar 2014 Jens Rengelshausen

GRÜNENTHAL Name der Präsentation Datum GRÜNENTHAL Page 2
Content
Which drug-drug interactions do really matter? 3
Clinically relevant transporter-mediated drug-drug interactions 5
DDI - Transporter 13 Mar 2014
Predicting transporter-mediated drug-drug interactions 16
GRÜNENTHAL Name der Präsentation Datum GRÜNENTHAL Page 3
Pharmacokinetic drug-drug interactions: basic principles
DDI - Transporter 13 Mar 2014
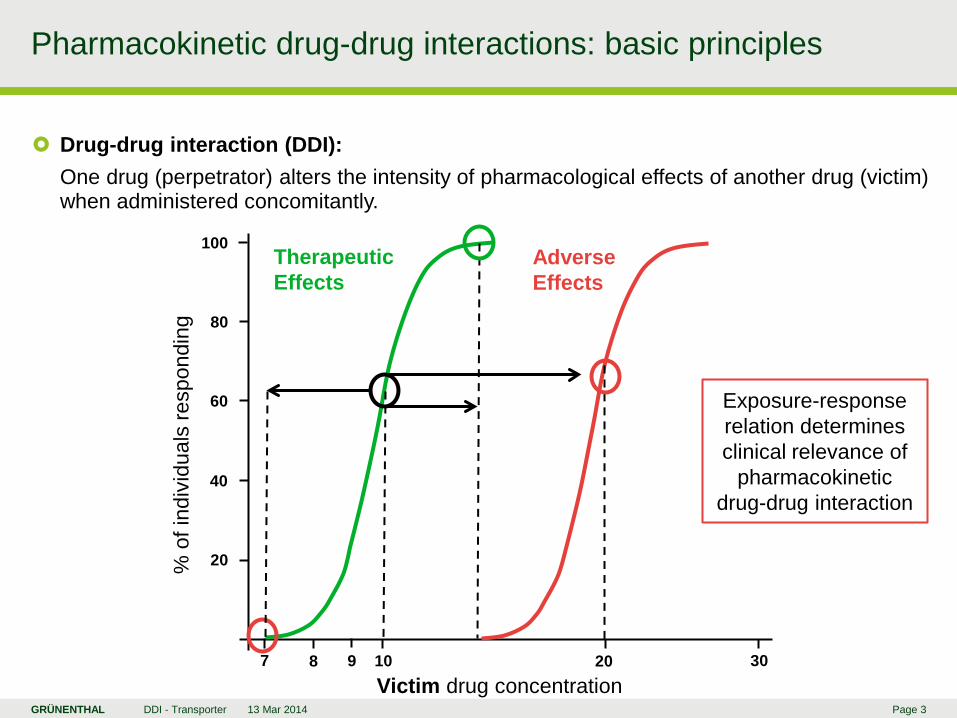
Drug-drug interaction (DDI): One drug (perpetrator) alters the intensity of pharmacological effects of another drug (victim) when administered concomitantly.
10 20 30 9 8 7 Victim drug concentration
20
40
60
80
100
% o
f ind
ivid
uals
resp
ondi
ng
Therapeutic Effects
Adverse Effects
Exposure-response relation determines clinical relevance of
pharmacokinetic drug-drug interaction

GRÜNENTHAL Name der Präsentation Datum GRÜNENTHAL Page 4
Clinical relevance: high-priority drug-drug interactions
DDI - Transporter 13 Mar 2014
Electronic knowledge base utilized to generate clinical decision support (PHS MKB) – Selection of high-priority DDIs out of 3327 DDI pairs by expert panel based on severity of
clinical outcome, monitoring options, probability of occurrence, evidence from literature – 15 DDIs identified: 7 pharmacodynamic interactions, 8 pharmacokinetic interactions
Selected highly clinically significant pharmacokinetic drug-drug interactions
Victim drug Perpetrator drug PK and clinical consequence Triptans MAO-A inhibitors AUC▲ up to 7-fold, cardiovascular ADRs Ramelteon Strong CYP1A2 inhibitors AUC▲ up to 190-fold, CNS ADRs Tizanidine CYP1A2 inhibitors AUC▲ up to 10-fold, hypotonia Lova-/Simvastatin CYP3A4 inhibitors AUC▲ up to 20-fold, rhabdomyolysis Irinotecan CYP3A4 inhibitors SN-38 AUC▲ 2-fold, cytotoxicity Ergot alkaloids CYP3A4 inhibitors Vasoconstriction, necrosis (ergotism) Protease inhibitors Strong CYP3A4 inducers AUC▼ by 80%, lack of efficacy Atazanavir Proton pump inhibitors AUC▼ by 60%, lack of efficacy
Phansalkar S et al. J Am Med Inform Assoc 2012;19:735-43

GRÜNENTHAL Name der Präsentation Datum GRÜNENTHAL Page 5
Drug transport proteins: gatekeepers of the body
DDI - Transporter 13 Mar 2014
≈ 30 drug transporters
ABC transporters
SLC transporters
Absorption Disposition Uptake for metabolism
and excretion Excretion
> 400 membrane transport proteins in human genome
Zhang L et al. Clin Pharmacol Ther 2011;89:481-4
Drug-drug interaction potential !

GRÜNENTHAL Name der Präsentation Datum GRÜNENTHAL Page 6
Alignment on relevant transporters for drug ADME
DDI - Transporter 13 Mar 2014
International Transporter Consortium
(ITC)
Goal 1 To provide overview of key drug transporters involved in drug ADME
Goal 3 To provide criteria for the design and conduct of clinical studies of transporter-related DDIs => decision trees
Goal 2 To provide examples of various technologies in studies of transporter-related DDIs
Huang SM and Woodcock J. Nat Rev Drug Discov 2010;9:175-6
Key mile- stones
FDA critical path initiative: ITC established in 2007 First Workshop 2008, first White Paper 2010 ITC recommendations taken up in revised draft of FDA Guidance for
Industry on Drug Interaction Studies in February 2012 Second Workshop March 2012, second set of White Papers 2013
Giacomini KM et al. Nat Rev Drug Discov 2010;9:215-36
11 international experts from
academia
11 international experts from
pharma-industry
2 experts from FDA

GRÜNENTHAL Name der Präsentation Datum GRÜNENTHAL Page 7
Drug transporters of clinical importance selected by the ITC
DDI - Transporter 13 Mar 2014
ABC transporters involved in drug absorption, disposition and excretion Transporter Relevant tissue Substrate (e.g.) Inhibitor (e.g.) P-glycoprotein Intestinal enterocyte Digoxin Quinidine (P-gp, MDR1) Kidney proximal tubule Clarithromycin Hepatocyte (canalicular) Brain endothelia BCRP as P-glycoprotein Topotecan Elacridar SLC transporters involved in drug disposition and excretion Transporter Relevant tissue Substrate (e.g.) Inhibitor (e.g.) OATP1B1 Hepatocyte (sinusoidal) Pravastatin Cyclosporine OATP1B3 Hepatocyte (sinusoidal) Rosuvastatin Lopinavir/ritonavir OAT1 Kidney proximal tubule Cidofovir Probenecid OAT3 Kidney proximal tubule Furosemide Probenecid OCT2 Kidney proximal tubule Metformin Cimetidine MATE1, MATE2K Kidney proximal tubule Metformin Cimetidine Hepatocyte (MATE1)
Zhang L et al. Clin Pharmacol Ther 2011;89:481-4 Hillgren KM et al. Clin Pharmacol Ther 2013;94:52-63

GRÜNENTHAL Name der Präsentation Datum GRÜNENTHAL Page 8
Drug transporters in the intestinal epithelia
DDI - Transporter 13 Mar 2014
Intestinal lumen (apical)
Blood (basolateral)
ATP P-gp
BCRP ATP
MRP2
MCT1
ASBT
PEPT1 PEPT2
OATP1A2 OATP2B1
ATP
ATP
OCT1
OSTα OSTβ
MRP3
ENT1 ENT2
Hillgren KM et al. Clin Pharmacol Ther 2013;94:52-63
Clinical relevance – P-gp and BCRP limit
oral bioavailability of drug substrates
– Inhibition of P-gp or BCRP => increased substrate bioavailability
– High gut concentrations of inhibitors lead to max. transport inhibition
König J et al. Pharmacol Rev 2013;65:944-66

GRÜNENTHAL Name der Präsentation Datum GRÜNENTHAL Page 9 DDI - Transporter 13 Mar 2014
Digoxin-clarithromycin interaction trial – Cross-over trial in 12 healthy subjects – Digoxin 0.75 mg SD p.o., in n=3 also i.v. – Clarithromycin 250 mg BID for 3 days
PK interaction results – Digoxin AUC after p.o. ▲ 1.7-fold – Renal tubular digoxin secretion ▼ by 40% – Digoxin AUC after i.v. ▲ only 1.2-fold
Intestinal absorption interaction via P-gp: digoxin-clarithromycin
0 2 4 6 8 10 12 24
0
1
2
3
4
5
6
Time (hours)
Plas
ma
Dig
oxin
(µg
l-1)
Placebo Clarithromycin05
101520253035
Dig
oxin
AU
C(0
,24)
(µg
l-1 h
)
P = 0.002
0 2 4 6 8 100
5
10
15
20
25
30
35
Time (hours)
Plas
ma
Dig
oxin
(µg
l-1)
A
Rengelshausen J et al. Br J Clin Pharmacol 2003;56:32-8
○ Placebo ● Clarithromycin

GRÜNENTHAL Name der Präsentation Datum GRÜNENTHAL Page 10 DDI - Transporter 13 Mar 2014
Inhibitor concentration effects – Highest interaction effect (digoxin ratios)
during absorption phase of clarithromycin – Est. plasma / gut conc.: 2.7 / 1337 µM – In vitro IC50 for interaction: 4.1 µM
Clinical consequences – Digoxin therapeutic range: 0.9 – 2 µg/l – Due to narrow therapeutic index of digoxin
AUC▲ >1.25-fold clinically important – Clinically relevant DDI
Intestinal P-gp inhibition by clarithromycin: digoxin toxicity risk
Rengelshausen J et al. Br J Clin Pharmacol 2003;56:32-8
0 2 4 6 8 10 12200
400
600
800
1000
1200
1400
Time (hours)
Plas
ma
Cla
rithr
omyc
in (µ
g l-1
)
200 400 600 800 1000 1200
11.21.41.61.8
22.2
Plasma Clarithromycin (µg l-1)P
lasm
a D
igox
in R
atio
10 min
12 h
Zhang L et al. Xenobiotica 2008;38:709-24
GRÜNENTHAL Name der Präsentation Datum GRÜNENTHAL Page 11
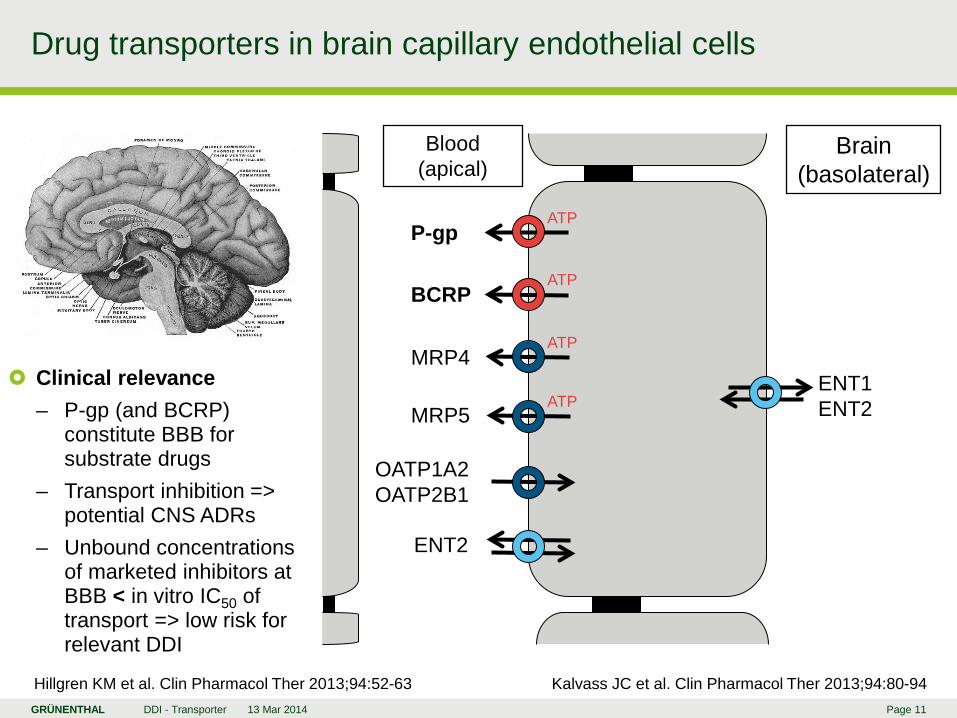
Drug transporters in brain capillary endothelial cells
DDI - Transporter 13 Mar 2014
Blood (apical)
Brain (basolateral)
ATP P-gp
BCRP ATP
MRP4
MRP5
ENT2
OATP1A2 OATP2B1
ATP
ENT1 ENT2
Hillgren KM et al. Clin Pharmacol Ther 2013;94:52-63
ATP Clinical relevance
– P-gp (and BCRP) constitute BBB for substrate drugs
– Transport inhibition => potential CNS ADRs
– Unbound concentrations of marketed inhibitors at BBB < in vitro IC50 of transport => low risk for relevant DDI
Kalvass JC et al. Clin Pharmacol Ther 2013;94:80-94

GRÜNENTHAL Name der Präsentation Datum GRÜNENTHAL Page 12
Drug transporters in the hepatocytes
DDI - Transporter 13 Mar 2014
Blood (sinusoidal)
ATP P-gp
BCRP ATP
MRP2 MATE1
OCT1
ATP
MRP3 MRP4 MRP6
NTCP
ENT2 ENT2
Hillgren KM et al. Clin Pharmacol Ther 2013;94:52-63
ENT1
BSEP
OATP1B1
OAT2 OAT7
Bile (canalicular)
ATP
ATP
OATP1B3
OATP2B1
OSTα OSTβ
Clinical relevance – Liver uptake transport
basis for subsequent drug metabolism
– Inhibition of liver uptake => increased plasma exposure of substrate
– Drug inhibition of MRP or BSEP => DILI risk
– Canalicular MRP with sinusoidal salvage
König J et al. Pharmacol Rev 2013;65:944-66

GRÜNENTHAL Name der Präsentation Datum GRÜNENTHAL Page 13 DDI - Transporter 13 Mar 2014
Rosuvastatin-cyclosporine interaction – 10 patients after heart transplantation – Rosuvastatin 10 mg SD and MD – Stable cyclosporin treatment – Historic control with 21 healthy subjects – Rosuvastatin AUC▲ 7.1-fold after MD
Pharmacogenetic impact on statin PK – OATP1B1 c.521T>C and BCRP c.421C>A
both influence rosuvastatin AUC – OATP1B1 SNP: Simvastatin AUC▲ 3.2-
fold in CC vs. TT; Odds ratio for myopathy after 80 mg simvastatin 16.9 in CC vs. TT
– Clinically relevant DDI between rosuvastatin and cyclosporine
Hepatic excretion interaction via OATP1B1 and BCRP
Healthy controls Heart transplant recipients0
100
200
300
400
Rosuvasatin AUC(0-24) (ng*h/mL)
OATP1B1 BCRP1
1.2
1.4
1.6
1.8
2
2.2
2.4
2.6
Fold increase in rosuvastatin AUC
c.521CC/TT c.421AA/CC
Simonson SG et al. Clin Pharmacol Ther 2004;76:167-77 Niemi M. Clin Pharmacol Ther 2010;87:130-33

GRÜNENTHAL Name der Präsentation Datum GRÜNENTHAL Page 14
Drug transporters in the renal proximal tubules
DDI - Transporter 13 Mar 2014
Tubule lumen (apical)
Blood (basolateral)
ATP P-gp
BCRP ATP
MRP2, MRP4
MATE1 MATE2K URAT1
PEPT1, PEPT2
OCTN1, OCTN2
ATP
OCT2
OATP4C1
ENT2
Hillgren KM et al. Clin Pharmacol Ther 2013;94:52-63
ENT1
OAT4
OAT1
OAT2
OAT3
Clinical relevance – Renal drug clearance =
glomerular filtration + tubular secretion – tubular re-absorption
– Drugs with high tubular secretion at risk for renal transport DDIs
– Uptake inhibition may prevent nephrotoxicity
König J et al. Pharmacol Rev 2013;65:944-66

GRÜNENTHAL Name der Präsentation Datum GRÜNENTHAL Page 15
Drug interactions influencing renal tubular drug secretion
DDI - Transporter 13 Mar 2014
DDIs via OCT2 and MATE1 and 2K DDIs via OAT1 and OAT3
Broad substrate overlap Probenecid potent inhibitor but extent of
drug-drug interactions is moderate: – Cephradine AUC▲ 3.6-fold – Acyclovir AUC▲ 1.4-fold – Furosemide AUC▲ 2.9-fold – Methotrexate Css▲ 2-fold
Beneficial use of probenecid interactions: – Increase of exposure and t1/2 of
benzylpenicillin – Protection against cidofovir nephrotoxicity
=> probenecid must be co-administered
Broad substrate overlap Cimetidine potent inhibitor (MATE > OCT)
but extent of interactions is moderate: – Metformin AUC▲ 1.4-fold – Dofetilide AUC▲ 1.5-fold – Procainamide AUC▲ 1.4-fold – Pindolol AUC▲ 1.5-fold
Interactions previously attributed to OCT2 may predominantly be mediated by MATEs due to higher inhibitor affinity
Zhang L et al. Clin Pharmacol Ther 2011;89:481-4 Hillgren KM et al. Clin Pharmacol Ther 2013;94:52-63

GRÜNENTHAL Name der Präsentation Datum GRÜNENTHAL Page 16
Transporter Studies in Drug Development: ITC + FDA view
DDI - Transporter 13 Mar 2014
Evaluation of an investigational drug as substrate for drug transporters – Decision tree from FDA Guidance (2012) modified by ITC after second workshop (2012)
All NMEs
Determine whether NME is P-gp and/or BCRP
substrate in vitro
Hepatic or biliary secretion major? e.g. ≥ 25% of total clearance or unknown?
Renal active secretion major? e.g. ≥ 25% of total clearance or unknown?
Determine whether NME is OATP1B1 and/or OATP1B3
substrate in vitro
Determine whether NME is OAT1, OAT3, OCT2 and/or
MATE substrate in vitro
Refer to OATP1B1/1B3 decision tree for need to conduct in vivo studies
Refer to OAT1/3 and OCT2/MATE decision tree for potential in vivo studies
Refer to P-gp and BCRP decision tree for need to conduct in vivo studies
Giacomini KM and Huang SM. Clin Pharmacol Ther 2013;94:3-9
Yes Yes

GRÜNENTHAL Name der Präsentation Datum GRÜNENTHAL Page 17
PBPK modeling and drug-drug interactions – principles
DDI - Transporter 13 Mar 2014
Physiologically based pharmacokinetic (PBPK) modeling and simulation – Dynamic tool to predict PK of drugs and effects of intrinsic + extrinsic factors in humans
System component (drug-independent)
Physicochemical
Distribution
Elimination
Zhao P et al. Clin Pharmacol Ther 2011;89:259-67
Absorption and first pass metabolism
Drug-dependent component
Absorption
Distribution
In vitro human ADME and MOA data In vivo human PK data
Metabolism and transport
DDI
MOA
PK of metabolite(s)
PK-PD relationship
Lung
Rapidly perfused organs
Slowly perfused organs
Kidney
Liver
Intestines
Blood
Blood
Dosing Ellimination
PBPK model
Model refine-ment

GRÜNENTHAL Name der Präsentation Datum GRÜNENTHAL Page 18
PBPK modeling and drug-drug interactions – practice
DDI - Transporter 13 Mar 2014
Prediction of transporter-mediated DDIs Chances and limits of PBPK modeling
Help optimizing clinical trials: – dosing regimens – sampling schemes – need for additional trials
Prediction of complex DDIs involving transporters and metabolic enzymes
Quality of in vitro model information may limit utility of PBPK approaches
Integration of in vivo data to refine PBPK model: “predict, learn, confirm“ iterations
15 submissions to FDA containing PBPK analyses on DDIs (2008 – 2011)
Specialized PBPK database software available, e.g. Simcyp Simulator
PBPK models to incorporate permeability-limited tissue compartments for intestine, liver and kidney with active transport
Detailed kinetic characterization needed Transporter interaction related changes in
tissue concentrations may be predicted Examples of successful prediction of
transporter-mediated DDIs still limited: – Cyclosporine – repaglinide (OATP1B1) – Gemfibrozil – pravastatin (OATP1B1) – Verapamil – digoxin (P-glycoprotein)
Zamek-Gliszczynski MJ et al. Clin Pharmacol Ther 2013;94:64-79 Zhao P et al. Clin Pharmacol Ther 2011;89:259-67

GRÜNENTHAL Name der Präsentation Datum GRÜNENTHAL Page 19
Transporter-mediated drug-drug interactions: summary
DDI - Transporter 13 Mar 2014
Relevance
Transporter-mediated DDIs may have high clinical relevance, but their extent is rather lower than of DDIs mediated by metabolic enzymes.
Transporter-mediated intestinal absorption, hepatic uptake and renal tubular secretion are main sites of transporter-mediated DDIs.
Clinical relevance of transporter-mediated DDIs at BBB is still unclear. Emerging data on newly characterized transporters may change
mechanistic understanding of clinically relevant DDIs.
Actions
Transporter-medicated DDIs are to be considered in drug development. NMEs are recommended to be investigated as potential substrates and/or
inhibitors of relevant drug transporters according to decision trees. Results need to be reflected in drug labels in order to prevent adverse drug
reaction or lack of efficacy caused by transporter-mediated DDIs. Well refined PBPK modeling may enable optimal predictions of transporter-
mediated DDIs and help optimizing or even omitting clinical trials.

GRÜNENTHAL Name der Präsentation Datum GRÜNENTHAL Page 20