drug eluting balloon in peripheral artery disease · critical limb ischemia • critical limb...
TRANSCRIPT

Drug Eluting Balloon in peripheral artery disease
Alessandro Furgieri MD Cardiovascular Department ICC Istituto Clinico Cardiologico Casal Palocco (RM) - Italy
CLI Overview and Challenges
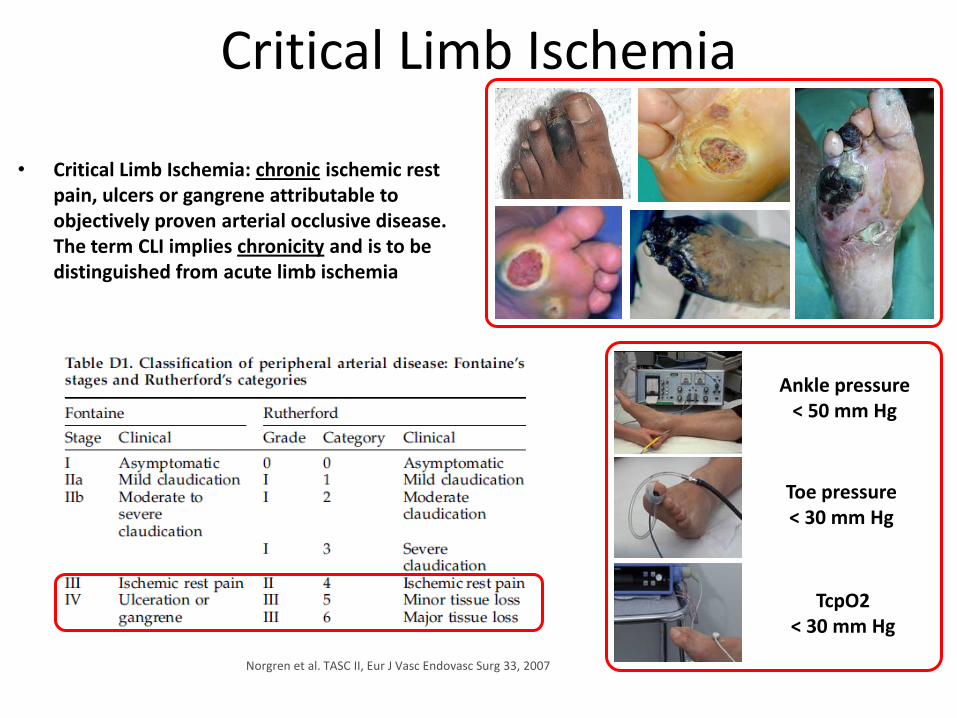
Critical Limb Ischemia
• Critical Limb Ischemia: chronic ischemic rest pain, ulcers or gangrene attributable to objectively proven arterial occlusive disease. The term CLI implies chronicity and is to be distinguished from acute limb ischemia
Ankle pressure < 50 mm Hg
Toe pressure < 30 mm Hg
TcpO2 < 30 mm Hg
Norgren et al. TASC II, Eur J Vasc Endovasc Surg 33, 2007
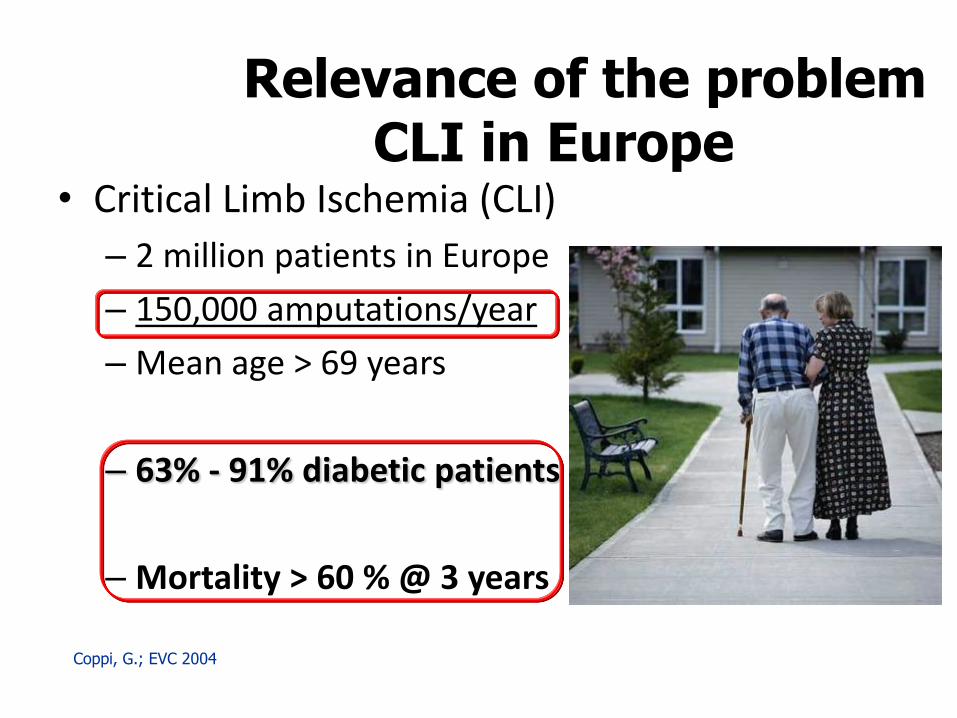
Relevance of the problem CLI in Europe
• Critical Limb Ischemia (CLI)
– 2 million patients in Europe
– 150,000 amputations/year
– Mean age > 69 years
– 63% - 91% diabetic patients
– Mortality > 60 % @ 3 years
Coppi, G.; EVC 2004
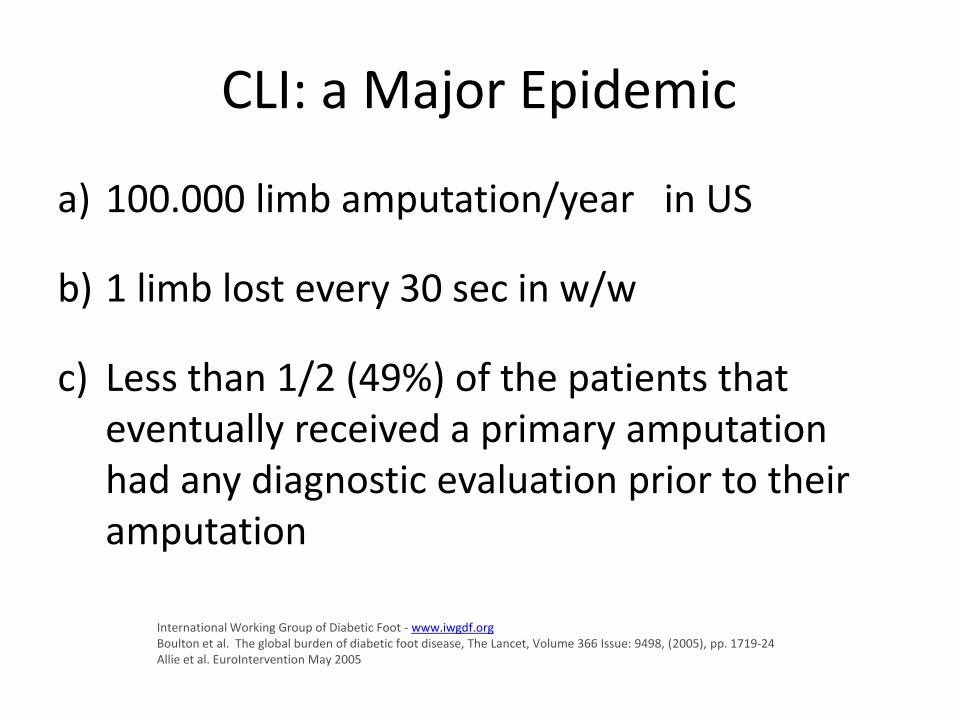
CLI: a Major Epidemic
a) 100.000 limb amputation/year in US
b) 1 limb lost every 30 sec in w/w
c) Less than 1/2 (49%) of the patients that eventually received a primary amputation had any diagnostic evaluation prior to their amputation
International Working Group of Diabetic Foot - www.iwgdf.org Boulton et al. The global burden of diabetic foot disease, The Lancet, Volume 366 Issue: 9498, (2005), pp. 1719-24 Allie et al. EuroIntervention May 2005
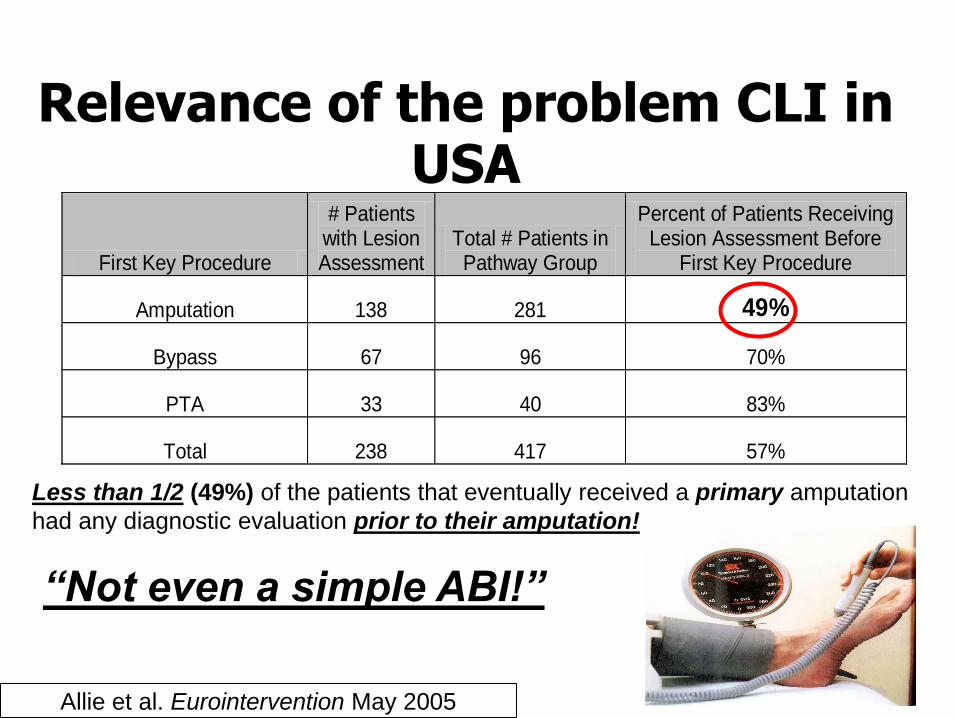
Relevance of the problem CLI in USA
First Key Procedure
# Patients with Lesion Assessment
Total # Patients in Pathway Group
Percent of Patients Receiving Lesion Assessment Before
First Key Procedure
Amputation 138 281 49%
Bypass 67 96 70%
PTA 33 40 83%
Total 238 417 57%
Less than 1/2 (49%) of the patients that eventually received a primary amputation
had any diagnostic evaluation prior to their amputation!
“Not even a simple ABI!”
Allie et al. Eurointervention May 2005
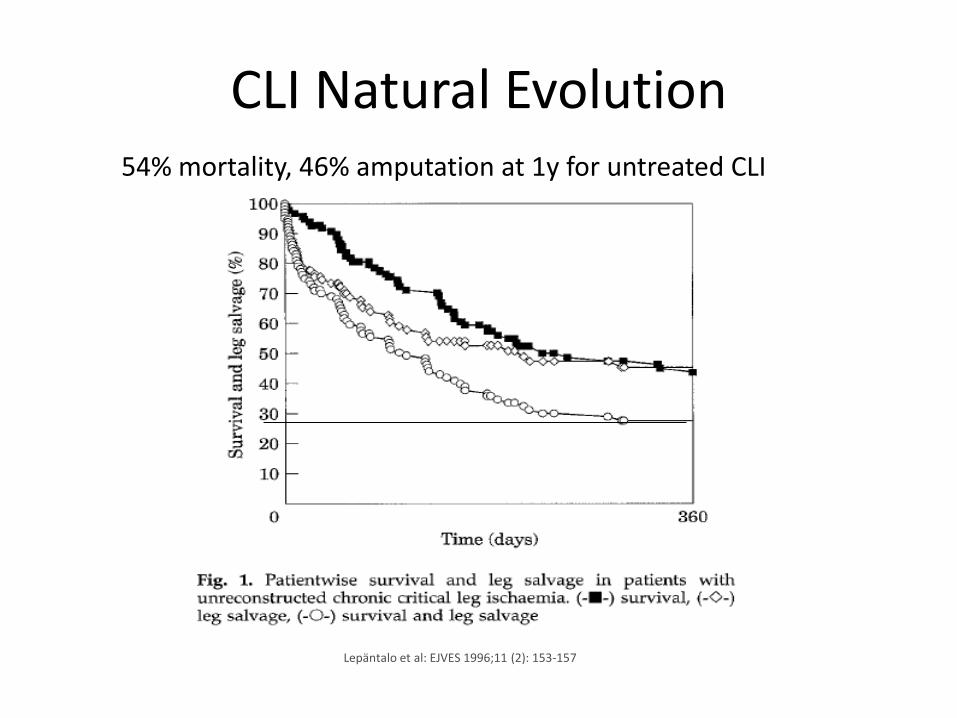
CLI Natural Evolution 54% mortality, 46% amputation at 1y for untreated CLI
Lepäntalo et al: EJVES 1996;11 (2): 153-157
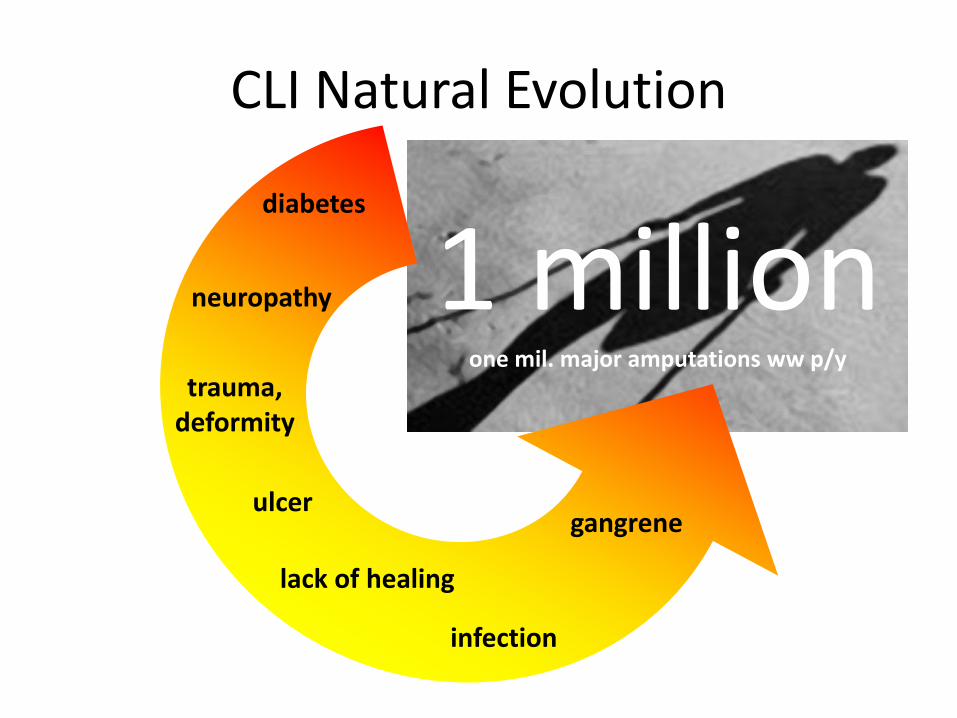
CLI Natural Evolution
diabetes
neuropathy
trauma, deformity
ulcer
lack of healing
infection
gangrene
1 million one mil. major amputations ww p/y
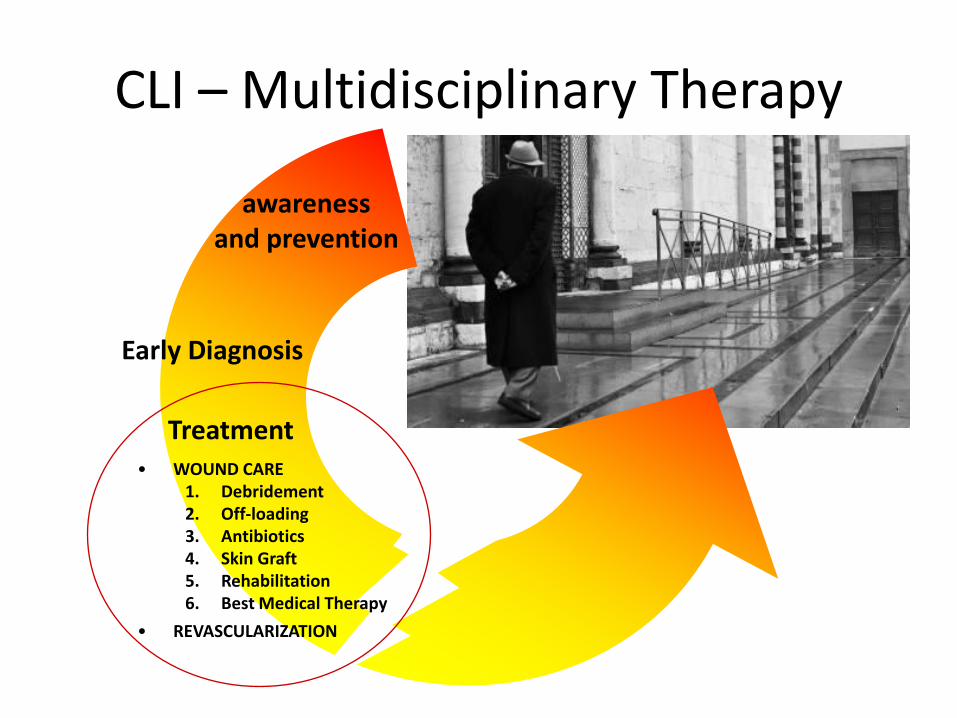
CLI – Multidisciplinary Therapy
awareness and prevention
Treatment • WOUND CARE
1. Debridement 2. Off-loading 3. Antibiotics 4. Skin Graft 5. Rehabilitation 6. Best Medical Therapy
• REVASCULARIZATION
Early Diagnosis

Clinical Variables and
Revascularization Strategies
affecting CLI Outcomes

Clinical Variables Affecting CLI Outcomes
• Predominance of BTK lesions (74% of all lower limb lesions)
• Prevalence of diffuse disease with long stenosis and occlusions (66% occlusions, 50% occlusions >10 cm)
Diabetes and diffuse disease
Graziani et al. Vascular Involvement in Diabetic Subjects with Ischemic Foot Ulcer: a New Morphologic Categorization of Disease Severity Eur J Vasc Endovasc Surg 33, 453 460 (2007)
44%50%
16%
0%
10%
20%
30%
40%
50%
60%
70%
Stenosis Occlusions
< 10 cm
> 10 cm
1% 8% 14% 36% 11% 27% 1%
BTK: 74% of 2893 lesions from 417 consecutive CLI diabetic subjects
with ischemic foot ulcer
Clinical Variables Affecting CLI Outcomes
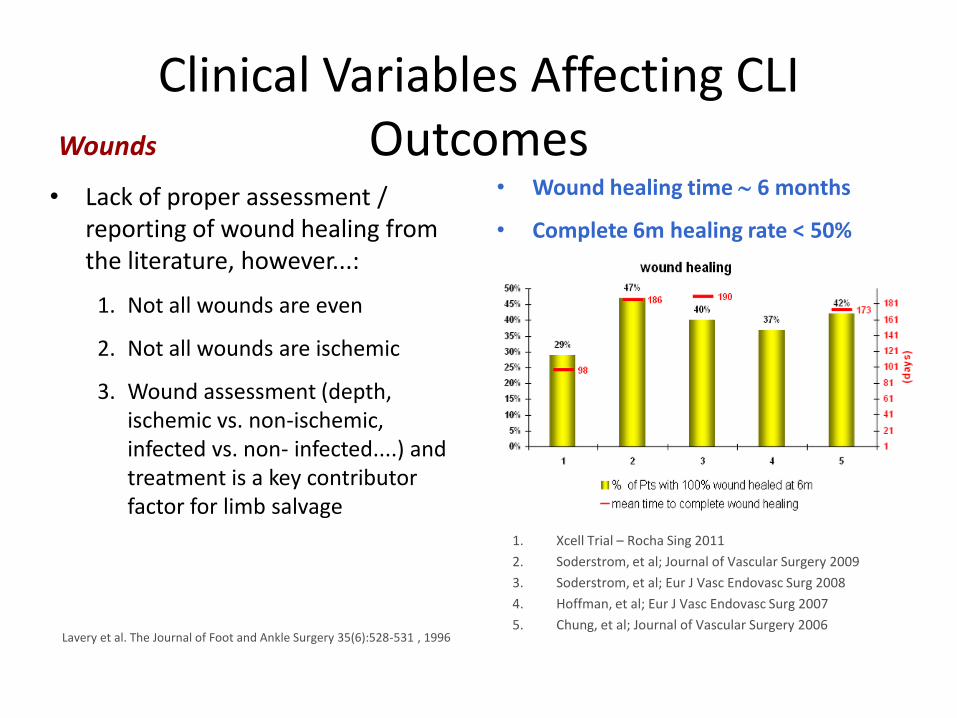
• Lack of proper assessment / reporting of wound healing from the literature, however...:
1. Not all wounds are even
2. Not all wounds are ischemic
3. Wound assessment (depth, ischemic vs. non-ischemic, infected vs. non- infected....) and treatment is a key contributor factor for limb salvage
Wounds
1. Xcell Trial – Rocha Sing 2011
2. Soderstrom, et al; Journal of Vascular Surgery 2009
3. Soderstrom, et al; Eur J Vasc Endovasc Surg 2008
4. Hoffman, et al; Eur J Vasc Endovasc Surg 2007
5. Chung, et al; Journal of Vascular Surgery 2006
Lavery et al. The Journal of Foot and Ankle Surgery 35(6):528-531 , 1996
• Wound healing time 6 months
• Complete 6m healing rate < 50%
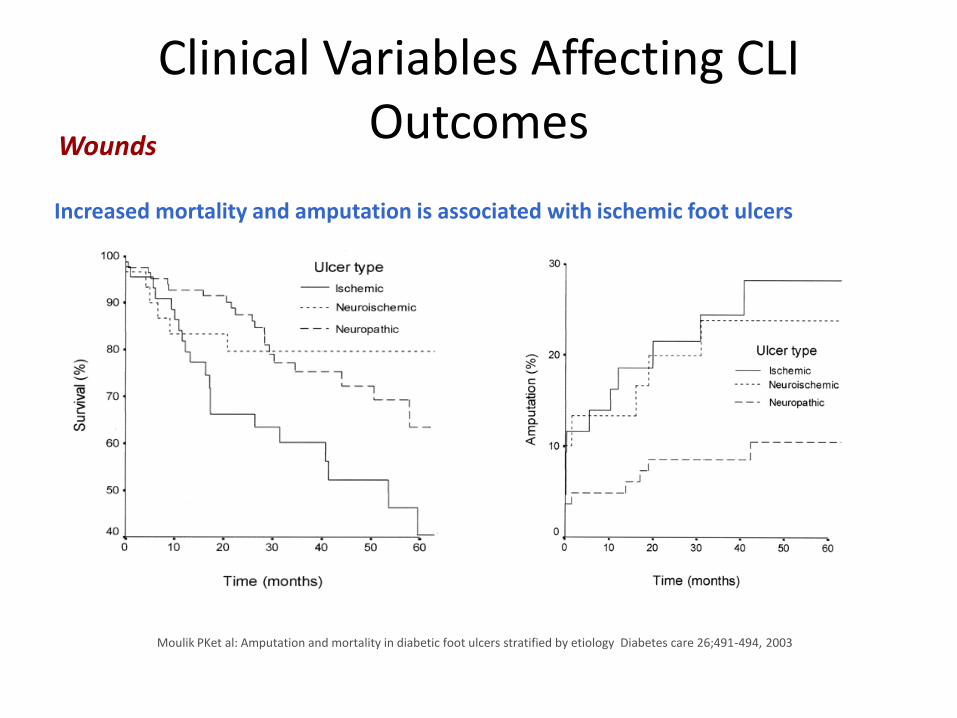
Clinical Variables Affecting CLI Outcomes
Wounds
Increased mortality and amputation is associated with ischemic foot ulcers
Moulik PKet al: Amputation and mortality in diabetic foot ulcers stratified by etiology Diabetes care 26;491-494, 2003
Revascularization Strategies Affecting CLI Outcomes
1. The most important factor affecting Limb Salvage is the number of patent arteries post-PTA [1;2]
1. 1 vessel better than 0
2. 2-3 vessels better than 1
3. Tibials better than peroneal
2. Direct revascularization (distal bypass) of the angiosome specific to the anatomy of the wound leads to a higher rate of healing and limb salvage [3]
3. Trade-off between driven by 1) procedural time and cost, and 2) technical access / success in treating the angiosome specific vessel
1. Peregrin et al. PTA of Infrapopliteal Arteries: Long-term Clinical Follow-up and Analysis of Factors Influencing Clinical Outcome Cardiovasc Intervent Radiol (2010) 33:720–725
2. Faglia et al. When is a technically successful peripheral angioplasty effective in preventing above-the-ankle amputation in diabetic patients with critical limb ischaemia Diabet Med. 2007 Aug;24(8):823-9
3. Neville et al. Revascularization of a Specific Angiosome for Limb Salvage: Does the Target Artery Matter? Ann Vasc Surg 2009; 23: 367-373
Targets in BTK PTA: complete vs. selected revascularization

Revascularization Strategies Affecting CLI Outcomes
Wound Related Artery: Detection and Treatment
Foot Angiosomes
Posterior Tibial Angiosome Posterior Tibial Artery (PTA) supplies the plantar aspect of the toes, the web spaces between the toes, the sole of the foot, and the inside of the heel. Three main branches of the PTA supply distinct portions of the sole: the calcaneal branch to the heel, the medial plantar artery to the instep, and the lateral plantar artery to the lateral midfoot and the forefoot
Anterior Tibial Angiosome Anterior Tibial Artery (ATA) becomes the dorsalis pedis artery that supplies the dorsum of the foot
Peroneal Angiosome
Peroneal Artery (PA) supplies the lateral border of the ankle and the outside of the heel. Two branches of the PA supply the anterolateral part of the ankle and the hind foot: the anterior perforating branch to the anterolateral part of the upper ankle and the calcaneal branch to the plantar aspect of the heel
Iida et al. Catheterization and Cardiovascular Interventions 75:830–836 (2010) Nevil et al. Ann Vasc Surg 2009

Clinical Variables Affecting CLI Outcomes
Wound Related Artery: Detection and Treatment
Angiosome based revascularization drives success
feeding artery flow to the site of ulceration successfully acquired
feeding artery flow to the site of ulceration NOT acquired
Iida et al. Importance of the Angiosome Concept for Endovascular Therapy in Patients with Critical Limb Ischemia - Catheterization and Cardiovascular Interventions 75:830–836 (2010)
RC and Nr of of Angiosomes: RC4 1 Angiosome, RC5 1–2 Angiosomes, RC6 > 1 Angiosome
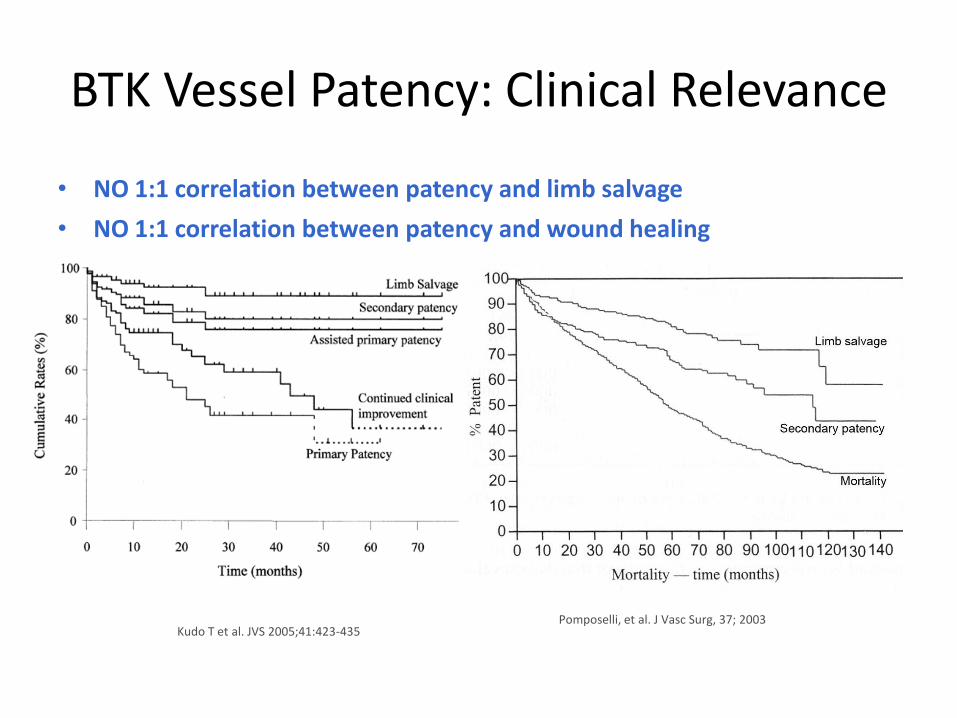
BTK Vessel Patency: Clinical Relevance
• NO 1:1 correlation between patency and limb salvage
• NO 1:1 correlation between patency and wound healing
Kudo T et al. JVS 2005;41:423-435 Pomposelli, et al. J Vasc Surg, 37; 2003
BTK Vessel Patency: Clinical Relevance
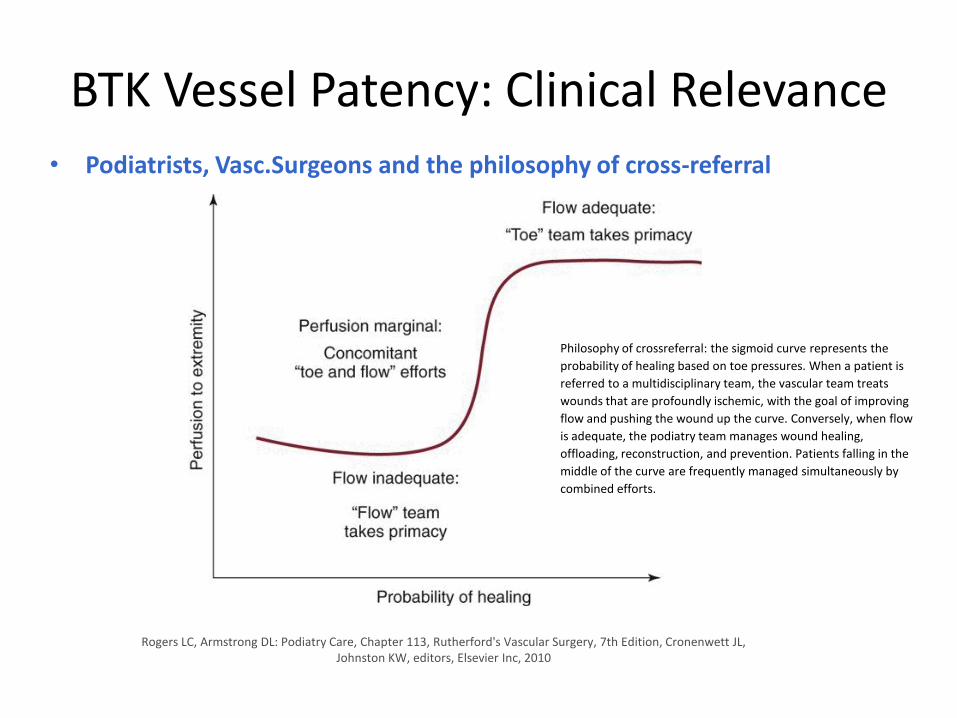
• Podiatrists, Vasc.Surgeons and the philosophy of cross-referral
Rogers LC, Armstrong DL: Podiatry Care, Chapter 113, Rutherford's Vascular Surgery, 7th Edition, Cronenwett JL, Johnston KW, editors, Elsevier Inc, 2010
Philosophy of crossreferral: the sigmoid curve represents the
probability of healing based on toe pressures. When a patient is
referred to a multidisciplinary team, the vascular team treats
wounds that are profoundly ischemic, with the goal of improving
flow and pushing the wound up the curve. Conversely, when flow
is adequate, the podiatry team manages wound healing,
offloading, reconstruction, and prevention. Patients falling in the
middle of the curve are frequently managed simultaneously by
combined efforts.
Significance of Patency in BTK-CLI
and Solutions for Improvement
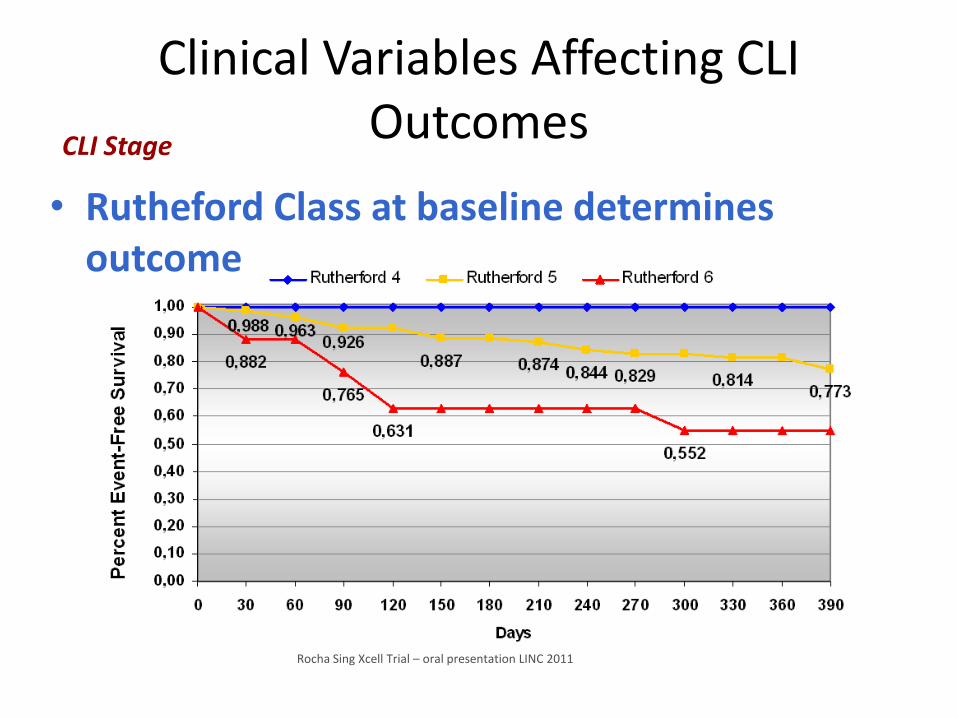
Clinical Variables Affecting CLI Outcomes
• Rutheford Class at baseline determines outcome
CLI Stage
Rocha Sing Xcell Trial – oral presentation LINC 2011
BTK Vessel Patency: Clinical Relevance
• 1) Baseline RC, 2) wound type and stage, 3) revascularization Strategy, 4) proper wound care are all key contributing factors to limb salvage
• Multidisciplinary close surveillance with secondary intervention is mandatory
• Vessel patency remains necessary but not sufficient for wound healing and limb salvage
• Vessel patency is necessary at least to the extent of time required for ischemic wounds to heal

Role of DES in BTK-CLI • DES have shown to significantly decrease restenosis vs PTA and BMS in short /
focal lesions BTK
• DEB are available in short length to address short lesions without stents
Length of BTK treated lesion (R.Ferraresi - EuroPCR 2011)

ACHILLES: Study Flowchart Total PatientPopulation n = 200 1:1 randomization
Balloon Angioplasty
n = 101 patients
n = 115 lesions
PTA (93 patients)
Cross over the Stent (8 patient)
CYPHER SELECT® PLUS n = 99 patients n = 113 lesions Stent(s) implantented (99patients) Stents/patient: 1.8 on avg.
12 months follow-up: Pts. comp. clinical f/u: n=74 (74.7%) -Deceased (n = 11) -Whithdrew consent (n = 4) -Lost to FU (n = 10) Lesions eval. Angio ff/u : n=67 (59.3%)
12 months follow-up: Pts. Comp. clinical f/u: n=80 (79.2%) Deceased (n =12) Whithdrew consent (n = 3) Lost to FU (n = 6 Lesions eval. angio f/u : n=74 (64.3%)
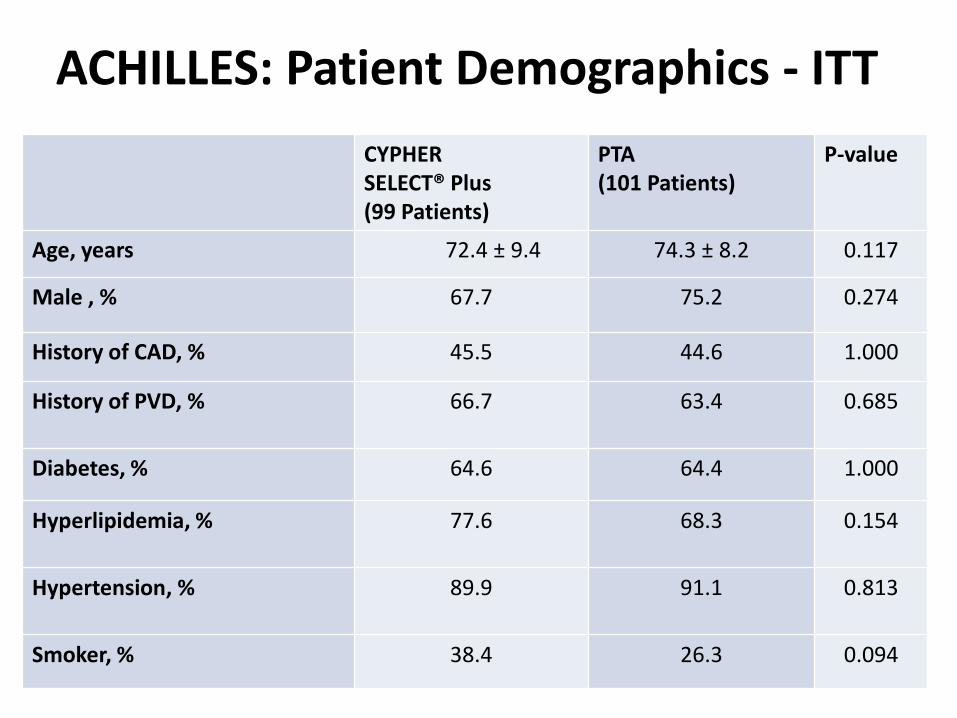
CYPHER SELECT® Plus (99 Patients)
PTA (101 Patients)
P-value
Age, years 72.4 ± 9.4 74.3 ± 8.2 0.117
Male , % 67.7 75.2 0.274
History of CAD, % 45.5 44.6 1.000
History of PVD, %
66.7 63.4 0.685
Diabetes, % 64.6 64.4 1.000
Hyperlipidemia, %
77.6 68.3 0.154
Hypertension, %
89.9 91.1 0.813
Smoker, % 38.4 26.3 0.094
ACHILLES: Patient Demographics - ITT
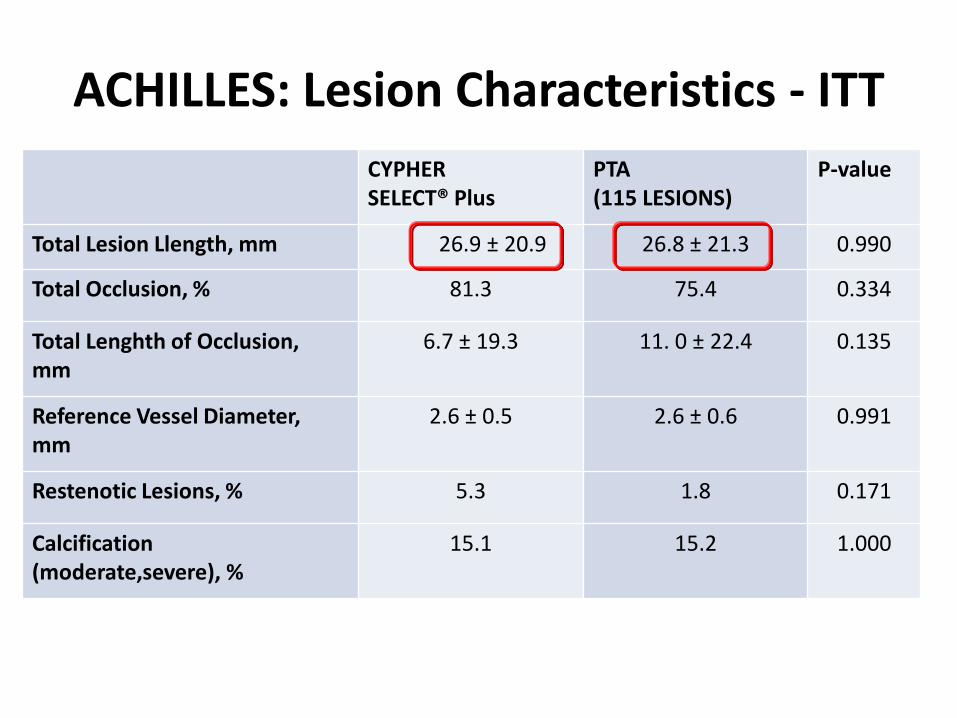
ACHILLES: Lesion Characteristics - ITT
CYPHER SELECT® Plus
PTA (115 LESIONS)
P-value
Total Lesion Llength, mm 26.9 ± 20.9 26.8 ± 21.3 0.990
Total Occlusion, % 81.3 75.4 0.334
Total Lenghth of Occlusion, mm
6.7 ± 19.3 11. 0 ± 22.4 0.135
Reference Vessel Diameter, mm
2.6 ± 0.5 2.6 ± 0.6 0.991
Restenotic Lesions, % 5.3 1.8 0.171
Calcification (moderate,severe), %
15.1 15.2 1.000
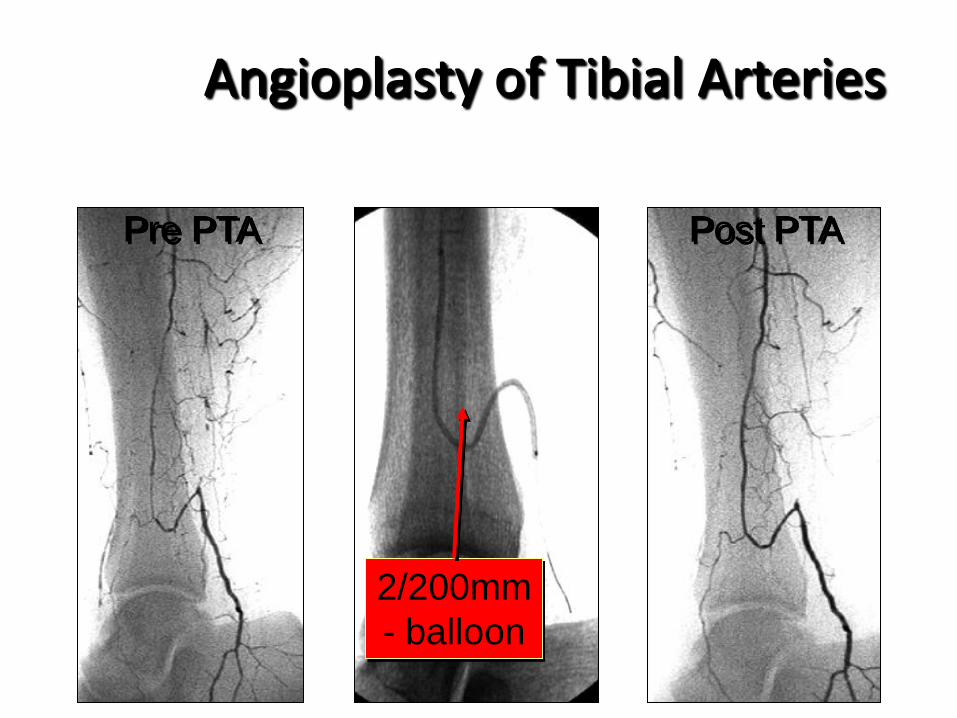
2/200mm
- balloon
Pre PTA
Angioplasty of Tibial Arteries
Post PTA
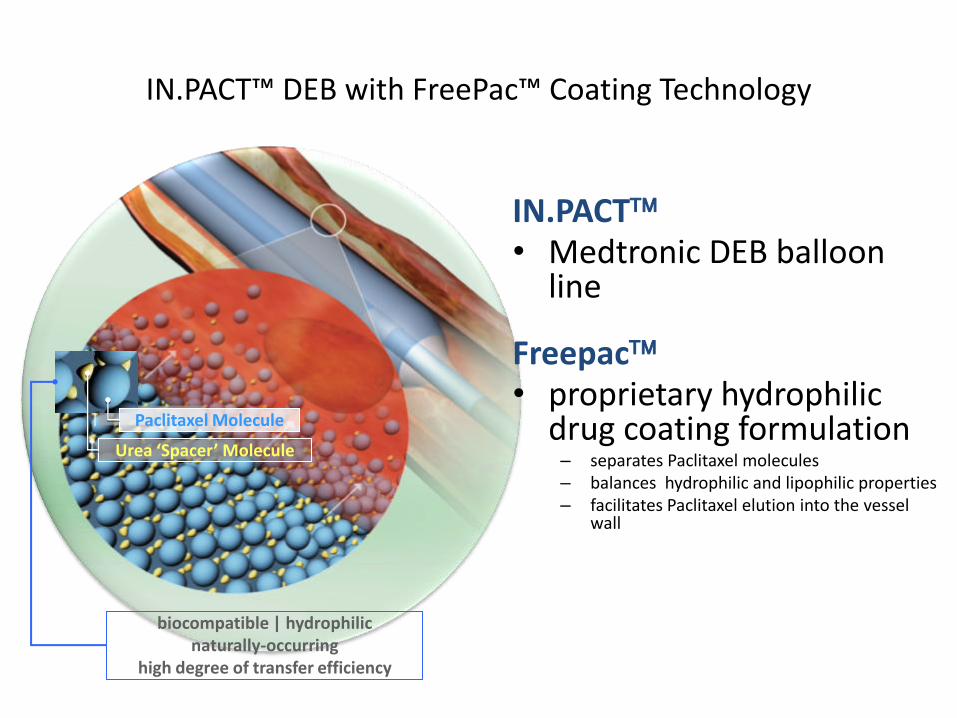
IN.PACT™ DEB with FreePac™ Coating Technology
Urea ‘Spacer’ Molecule
Paclitaxel Molecule
biocompatible | hydrophilic naturally-occurring
high degree of transfer efficiency
IN.PACT • Medtronic DEB balloon
line
Freepac • proprietary hydrophilic
drug coating formulation – separates Paclitaxel molecules – balances hydrophilic and lipophilic properties – facilitates Paclitaxel elution into the vessel
wall
Leipzig DEB-BTK Registry
Results and Interpretation
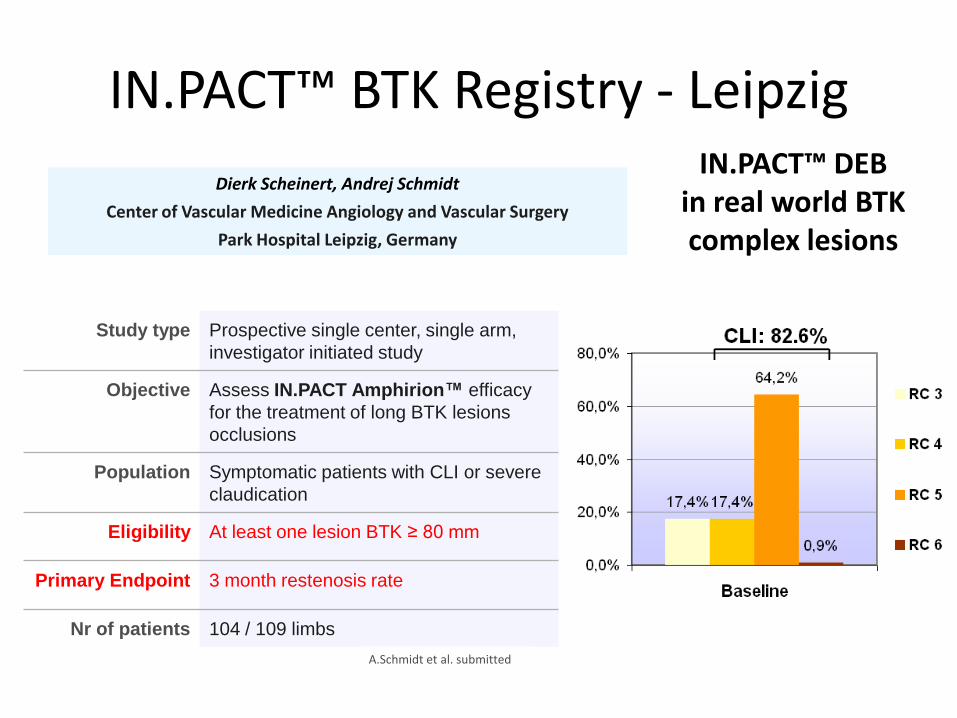
IN.PACT™ BTK Registry - Leipzig
Study type Prospective single center, single arm,
investigator initiated study
Objective Assess IN.PACT Amphirion™ efficacy
for the treatment of long BTK lesions
occlusions
Population Symptomatic patients with CLI or severe
claudication
Eligibility At least one lesion BTK ≥ 80 mm
Primary Endpoint 3 month restenosis rate
Nr of patients 104 / 109 limbs
Dierk Scheinert, Andrej Schmidt
Center of Vascular Medicine Angiology and Vascular Surgery
Park Hospital Leipzig, Germany
A.Schmidt et al. submitted
IN.PACT™ DEB in real world BTK complex lesions

IN.PACT™ BTK Registry – Leipzig (angio-subgroup)
DEB (angio subgroup)
# patients / limbs 74 / 79
Male gender 51 (68.9%)
mean age (y) 73.5 ± 9.3
diabetics 54 (73%)
Renal insuff. 34 (45.9%)
RC 3 16 (20.3%)
RC 4 14 (17.7%)
RC 5 49 (62%)
RC 6 0 (0%)
avg lesion length 173 ± 87 mm
Tot occlusions 61.9%
DEB (angio subgroup)
3m Ang. FU
Restenosis (>50%) 27.4%
Full-segment Resten. 10%
Restenosis Length 64 mm
12m
Clinical FU
Deaths 16.3%
Limb Salvage 95.6%
Clinical Improvement (1) 91.2% (2)
Compl. wound healing 74.2%
TLR 17.3%
(1) clinical improvement = reduction in size and/or depth of ulceration or improvement of rest-pain
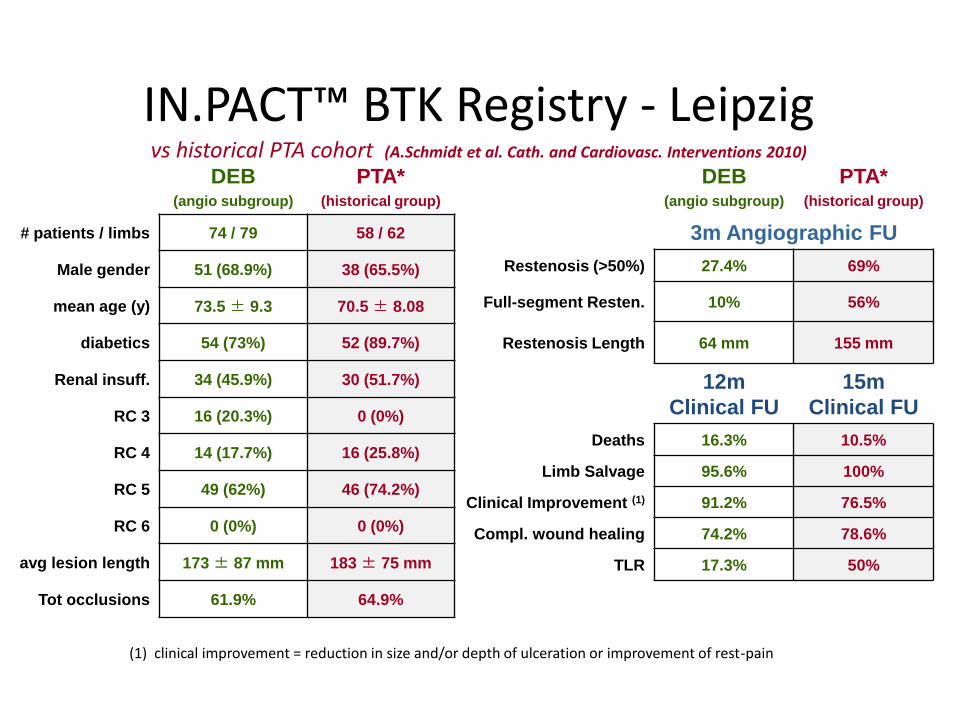
IN.PACT™ BTK Registry - Leipzig vs historical PTA cohort (A.Schmidt et al. Cath. and Cardiovasc. Interventions 2010)
DEB (angio subgroup)
PTA* (historical group)
# patients / limbs 74 / 79 58 / 62
Male gender 51 (68.9%) 38 (65.5%)
mean age (y) 73.5 ± 9.3 70.5 ± 8.08
diabetics 54 (73%) 52 (89.7%)
Renal insuff. 34 (45.9%) 30 (51.7%)
RC 3 16 (20.3%) 0 (0%)
RC 4 14 (17.7%) 16 (25.8%)
RC 5 49 (62%) 46 (74.2%)
RC 6 0 (0%) 0 (0%)
avg lesion length 173 ± 87 mm 183 ± 75 mm
Tot occlusions 61.9% 64.9%
DEB (angio subgroup)
PTA* (historical group)
3m Angiographic FU
Restenosis (>50%) 27.4% 69%
Full-segment Resten. 10% 56%
Restenosis Length 64 mm 155 mm
12m
Clinical FU
15m
Clinical FU
Deaths 16.3% 10.5%
Limb Salvage 95.6% 100%
Clinical Improvement (1) 91.2% 76.5%
Compl. wound healing 74.2% 78.6%
TLR 17.3% 50%
(1) clinical improvement = reduction in size and/or depth of ulceration or improvement of rest-pain
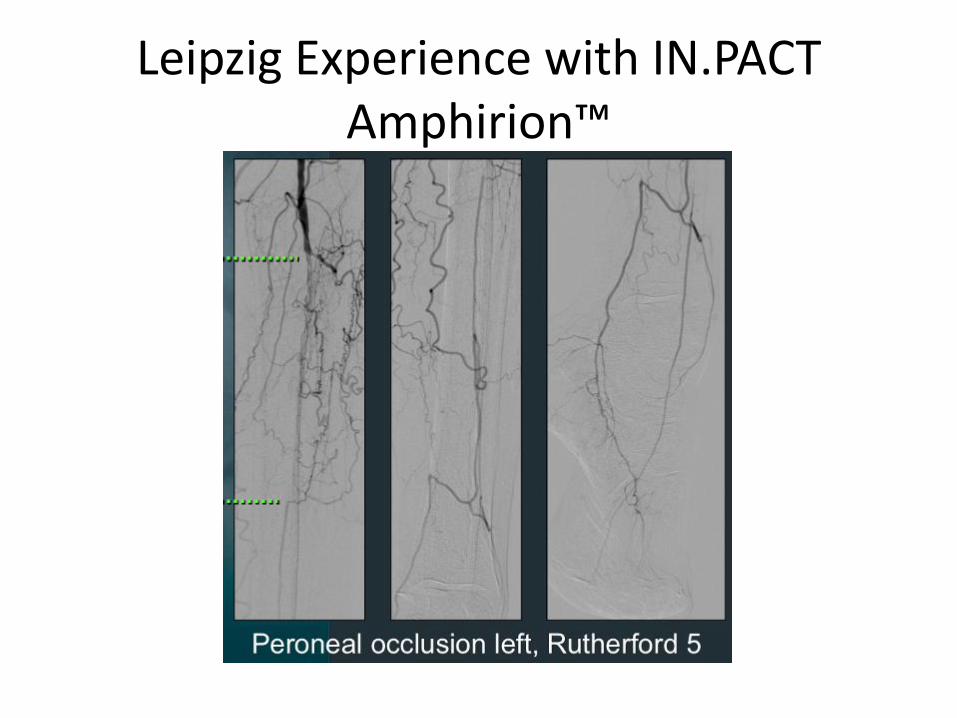
Leipzig Experience with IN.PACT Amphirion™
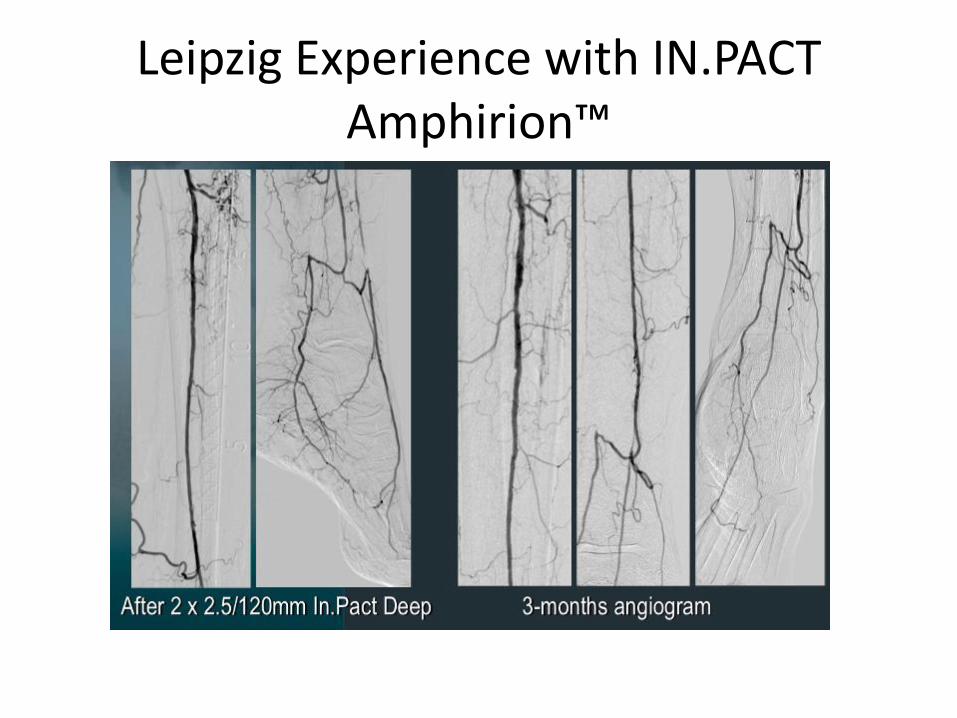
Leipzig Experience with IN.PACT Amphirion™
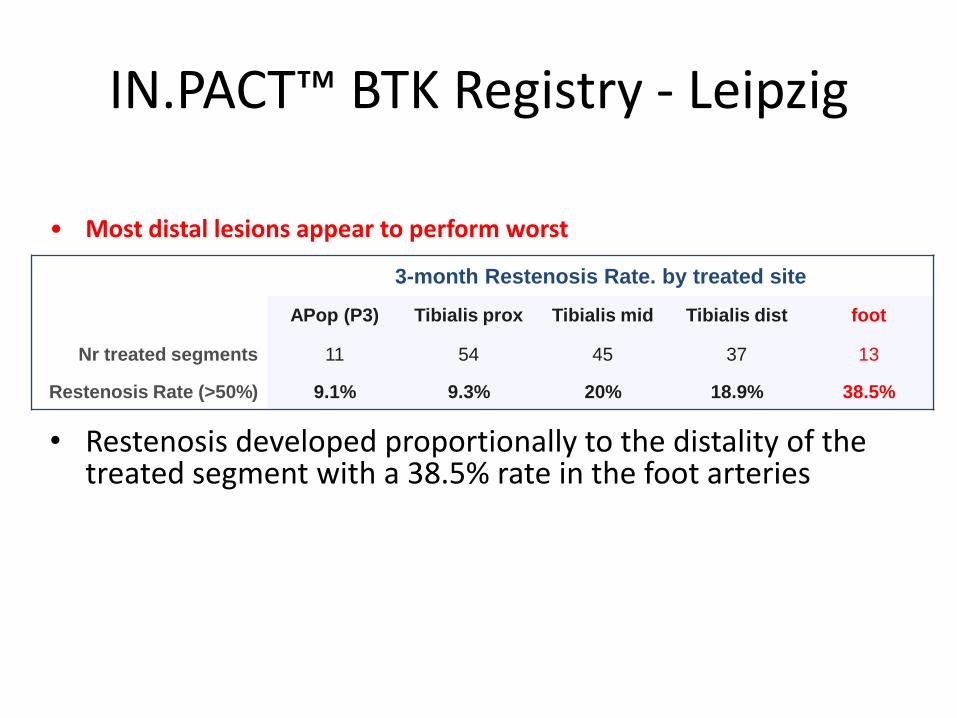
IN.PACT™ BTK Registry - Leipzig
• Restenosis developed proportionally to the distality of the treated segment with a 38.5% rate in the foot arteries
3-month Restenosis Rate. by treated site
APop (P3) Tibialis prox Tibialis mid Tibialis dist foot
Nr treated segments 11 54 45 37 13
Restenosis Rate (>50%) 9.1% 9.3% 20% 18.9% 38.5%
• Most distal lesions appear to perform worst

IN.PACT™ BTK Registry - Leipzig
• DEB usage for treating real world long BTK lesions and occlusions: – Remarkably low (27.4%) shown in the primary endpoint of 3-
month Angiographic Restenosis Rate – Very low restenosis burden (10% full segment restenosis) and
reintervention rate at 12 m (17.3%) – While lesion specific outcomes appear notably better vs
historical PTA cohorts, no meaningful differences were detectable in the hard clinical endpoints of amputation free survival and wound healing
– Properly designed head-to-head DEB-PTA trials with a parallel careful control of the full span of variables concurring to clinical outcome (ie. wound care) would be warrented

DEB SFA Italian Registry
Hypothesis
Drug Eluting Balloon can reduce Femoral-popliteal restenosis
in alternative to Stenting
Study Device
Urea ‘Spacer’ molecule
Paclitaxel molecule
• IN.PACT Admiral - Medtronic
• Freepac - proprietary hydrophilic
drug coating formulation
– separates Paclitaxel molecules
– balances hydrophilic and lipophilic properties
– facilitates Paclitaxel elution into the vessel wall
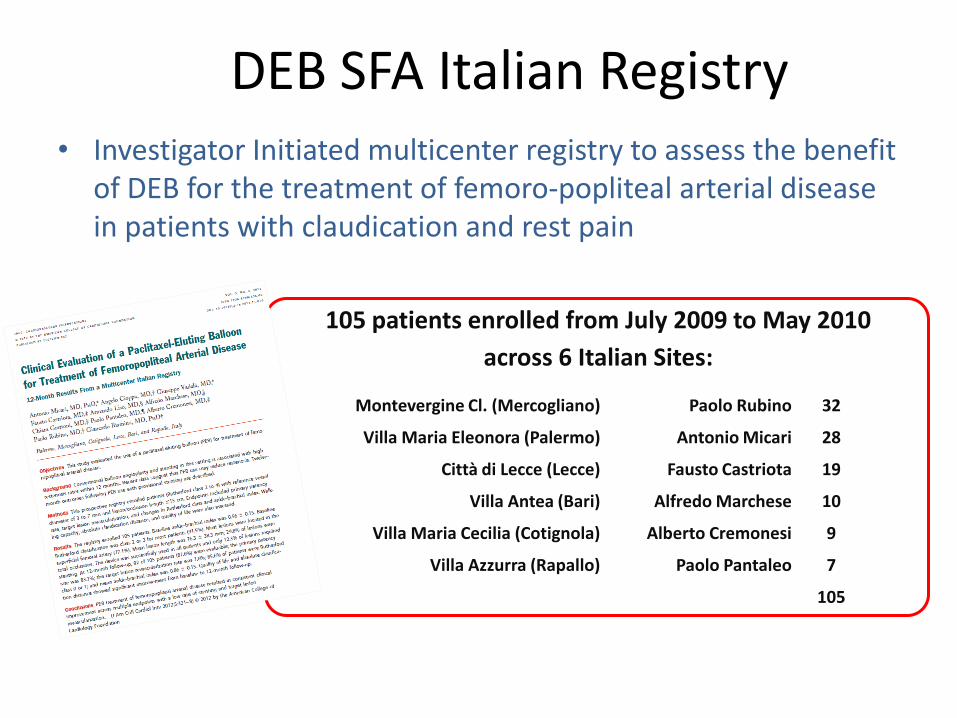
DEB SFA Italian Registry • Investigator Initiated multicenter registry to assess the benefit
of DEB for the treatment of femoro-popliteal arterial disease in patients with claudication and rest pain
Montevergine Cl. (Mercogliano) Paolo Rubino 32
Villa Maria Eleonora (Palermo) Antonio Micari 28
Città di Lecce (Lecce) Fausto Castriota 19
Villa Antea (Bari) Alfredo Marchese 10
Villa Maria Cecilia (Cotignola) Alberto Cremonesi 9
Villa Azzurra (Rapallo) Paolo Pantaleo 7
105
105 patients enrolled from July 2009 to May 2010
across 6 Italian Sites:
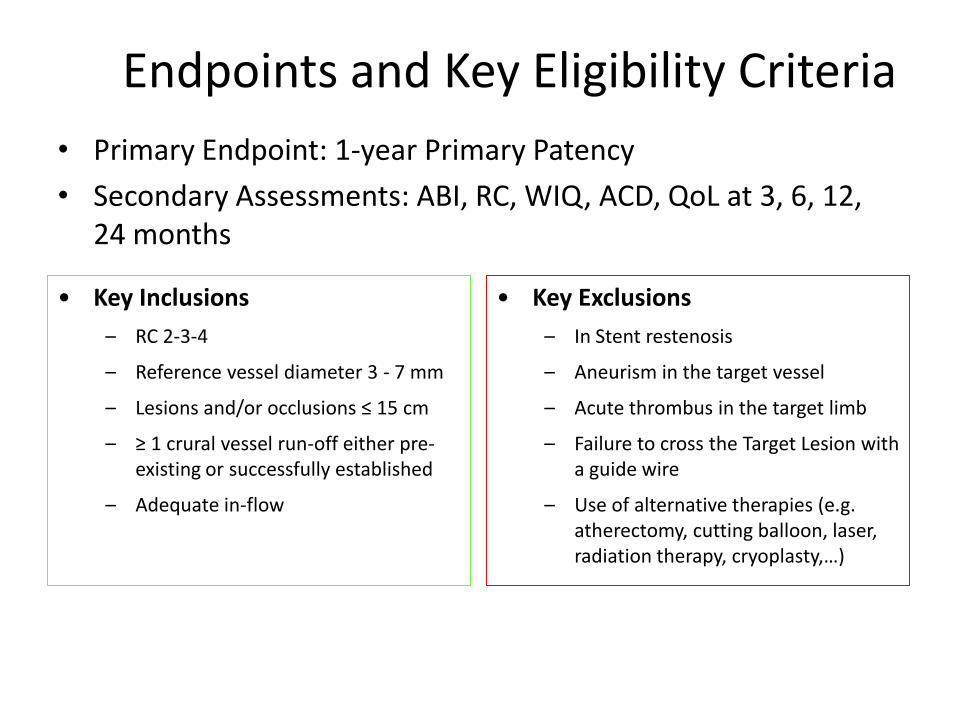
Endpoints and Key Eligibility Criteria
• Primary Endpoint: 1-year Primary Patency
• Secondary Assessments: ABI, RC, WIQ, ACD, QoL at 3, 6, 12, 24 months
• Key Inclusions
– RC 2-3-4
– Reference vessel diameter 3 - 7 mm
– Lesions and/or occlusions ≤ 15 cm
– ≥ 1 crural vessel run-off either pre-existing or successfully established
– Adequate in-flow
• Key Exclusions
– In Stent restenosis
– Aneurism in the target vessel
– Acute thrombus in the target limb
– Failure to cross the Target Lesion with a guide wire
– Use of alternative therapies (e.g. atherectomy, cutting balloon, laser, radiation therapy, cryoplasty,…)
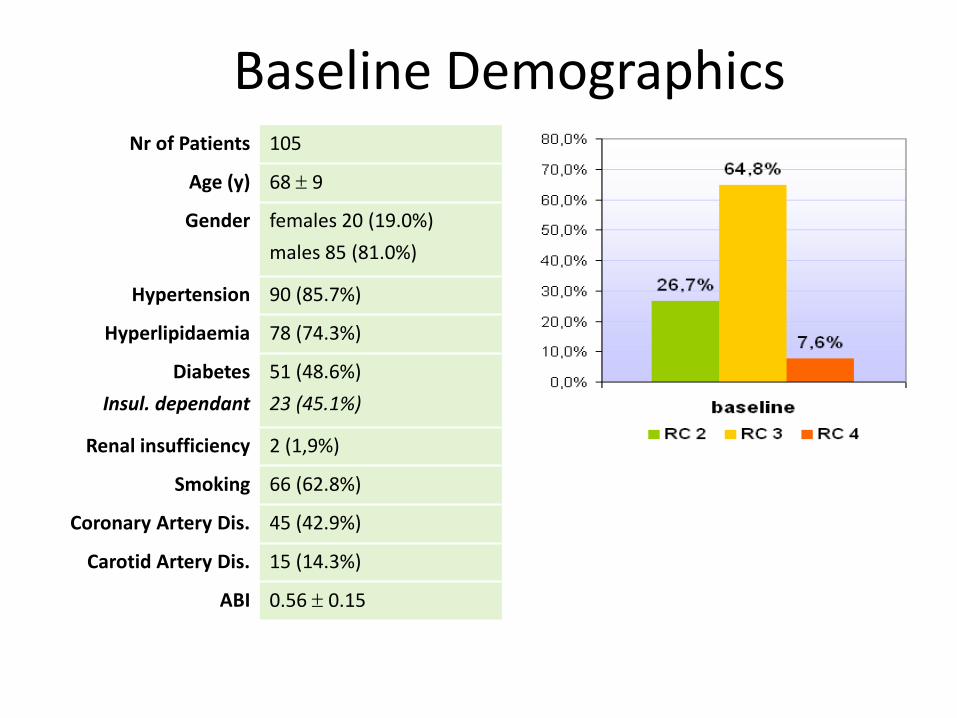
Baseline Demographics Nr of Patients 105
Age (y) 68 9
Gender females 20 (19.0%)
males 85 (81.0%)
Hypertension 90 (85.7%)
Hyperlipidaemia 78 (74.3%)
Diabetes
Insul. dependant
51 (48.6%)
23 (45.1%)
Renal insufficiency 2 (1,9%)
Smoking 66 (62.8%)
Coronary Artery Dis. 45 (42.9%)
Carotid Artery Dis. 15 (14.3%)
ABI 0.56 0.15
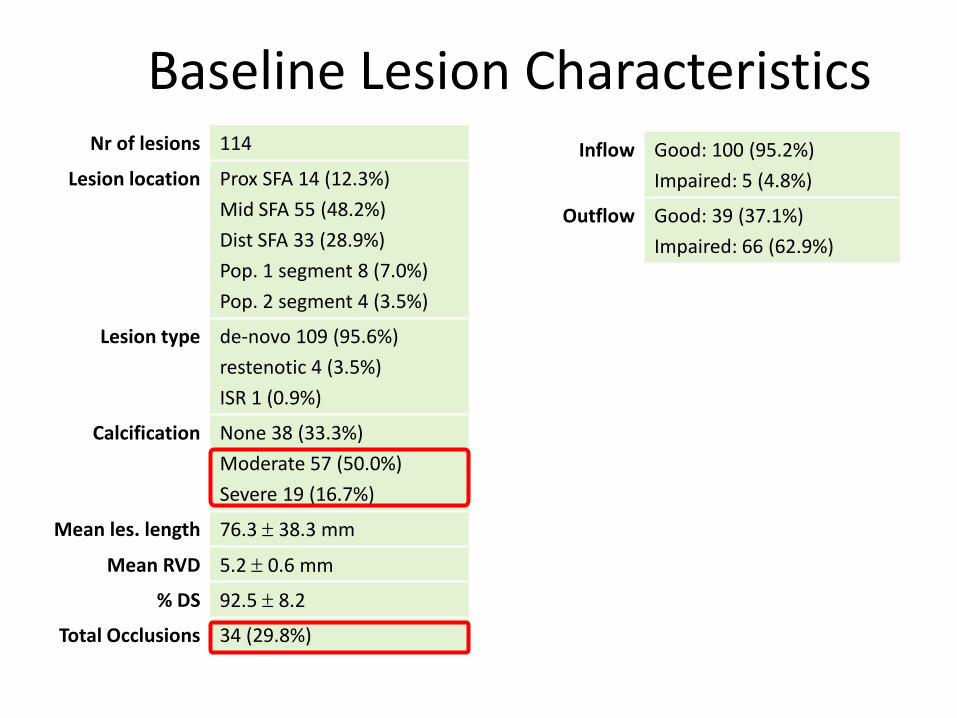
Baseline Lesion Characteristics Inflow Good: 100 (95.2%)
Impaired: 5 (4.8%)
Outflow Good: 39 (37.1%)
Impaired: 66 (62.9%)
Nr of lesions 114
Lesion location Prox SFA 14 (12.3%)
Mid SFA 55 (48.2%)
Dist SFA 33 (28.9%)
Pop. 1 segment 8 (7.0%)
Pop. 2 segment 4 (3.5%)
Lesion type de-novo 109 (95.6%)
restenotic 4 (3.5%)
ISR 1 (0.9%)
Calcification None 38 (33.3%)
Moderate 57 (50.0%)
Severe 19 (16.7%)
Mean les. length 76.3 38.3 mm
Mean RVD 5.2 0.6 mm
% DS 92.5 8.2
Total Occlusions 34 (29.8%)

Procedural and Acute Outcome
1. Predilatation with standard undersized (-0.5 mm) PTA balloon
2. DEB dilatation with 1:1 balloon: RVD for 180 sec
3. Provisional stenting in case of flow limiting dissections and persistent residual stenosis > 50%
Inflow re-established 5 (100%)
Outflow re-established 66 (100%)
Lesion crossing True lumen 105 (92.1%)
Subintimal 9 (7.9%)
pre-dilatation 113 (99.1%)
DEB infl. time 181 20.4 sec
Nr DEB p/lesion 135/114 = 1.18
Device Success 135 (100%)
Tech. Success 121 (89.6%)
Post-Dilatation 20 (17.5%)
Stenting 14 (12.3%)
11 (9.6%) flow limit. dissection
3 (2.6%) persistent stenosis
Residual % DS 12.2 ± 9.5%, range 0 – 40%

Case Example
Villa Maria Eleonora Hospital
pre-dilatation: Admiral 4.0-80 DEB: In.Pact Admiral 5.0-120 mm

Primary Patency
• 1-year Primary Patency[1] = 83.7%
• 2-year[2] Primary Patency[1] = 72.4%
Survival from TLR, Occlusion, >50% Restenosis
1. Rates calculated on actual events (PSVR < 2.5) 2. Mean follow up time = 27± 3 months
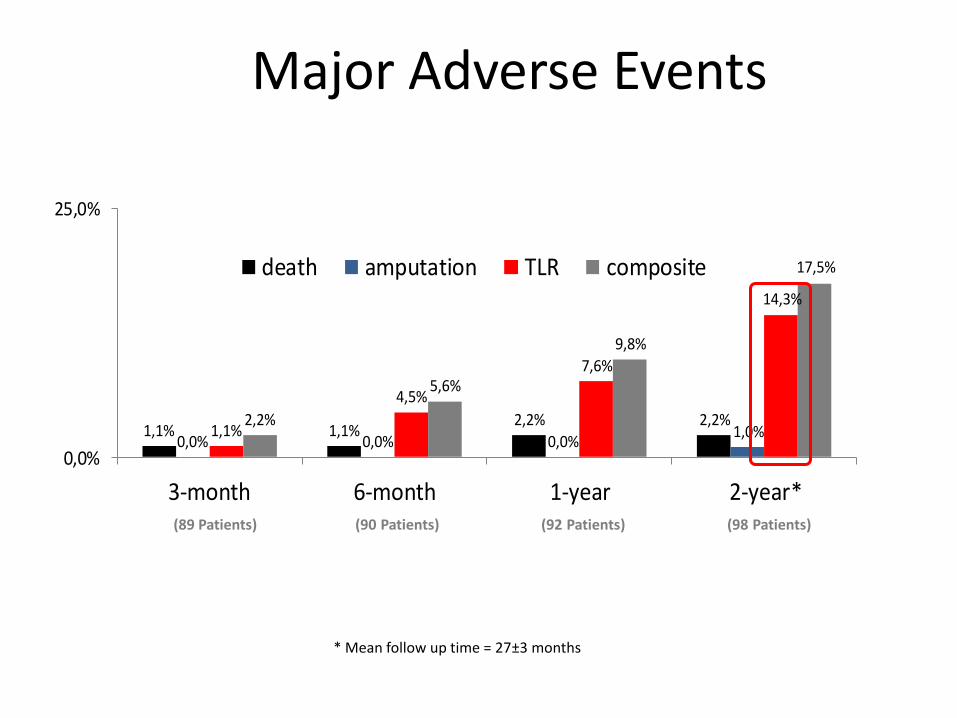
Major Adverse Events
1,1% 1,1%2,2% 2,2%
0,0% 0,0% 0,0%1,0%1,1%
4,5%
7,6%
14,3%
2,2%
5,6%
9,8%
17,5%
0,0%
25,0%
3-month 6-month 1-year 2-year*
death amputation TLR composite
(89 Patients) (90 Patients) (92 Patients) (98 Patients)
* Mean follow up time = 27±3 months
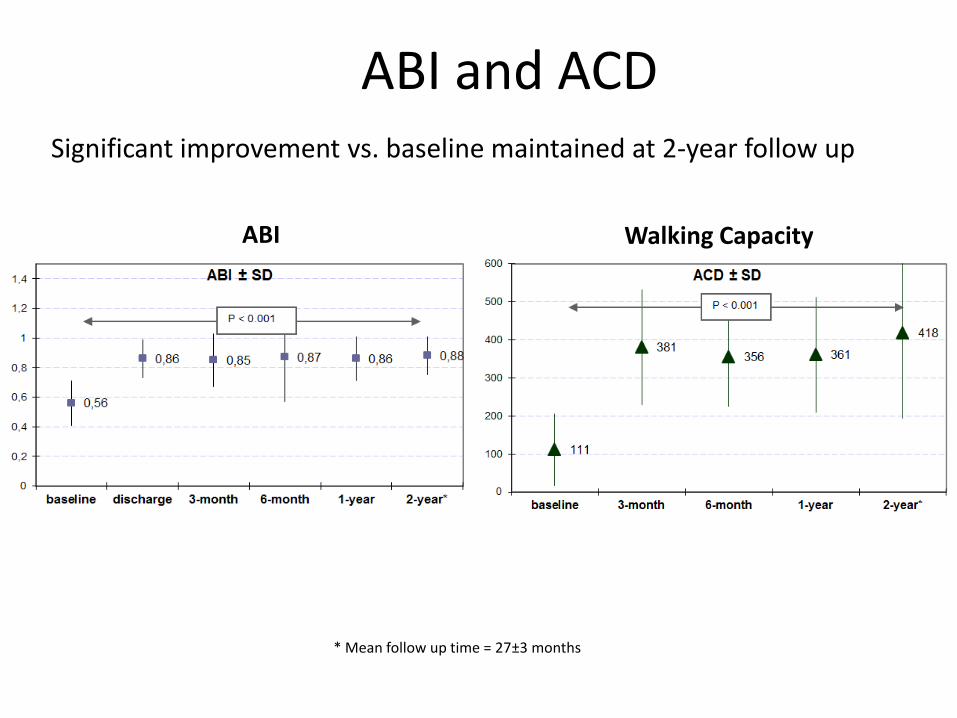
ABI and ACD
ABI Walking Capacity
Significant improvement vs. baseline maintained at 2-year follow up
* Mean follow up time = 27±3 months
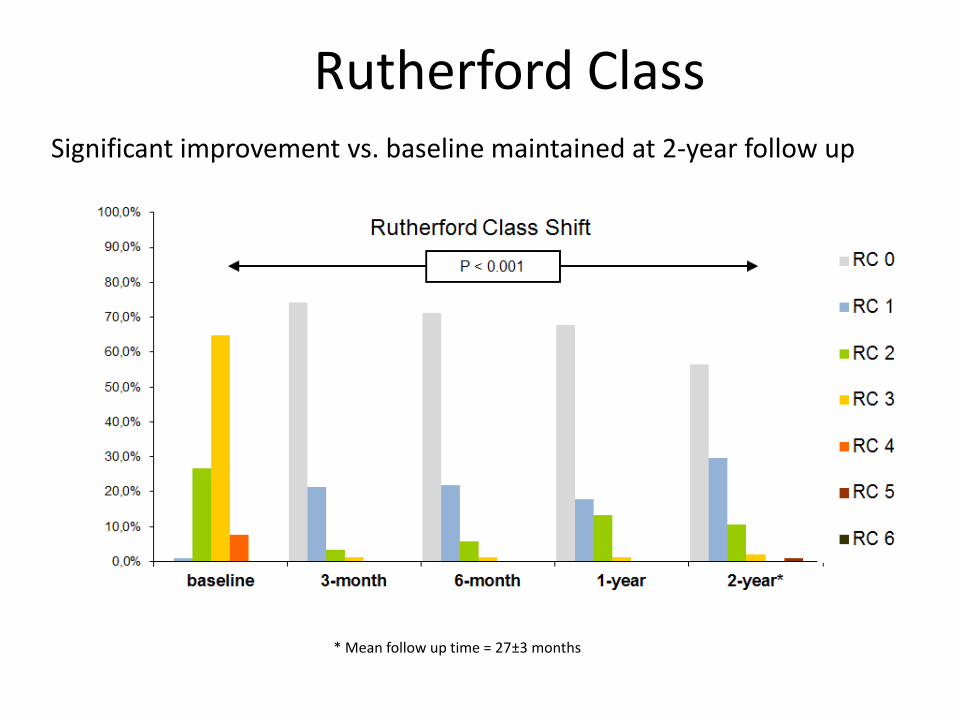
Rutherford Class Significant improvement vs. baseline maintained at 2-year follow up
* Mean follow up time = 27±3 months
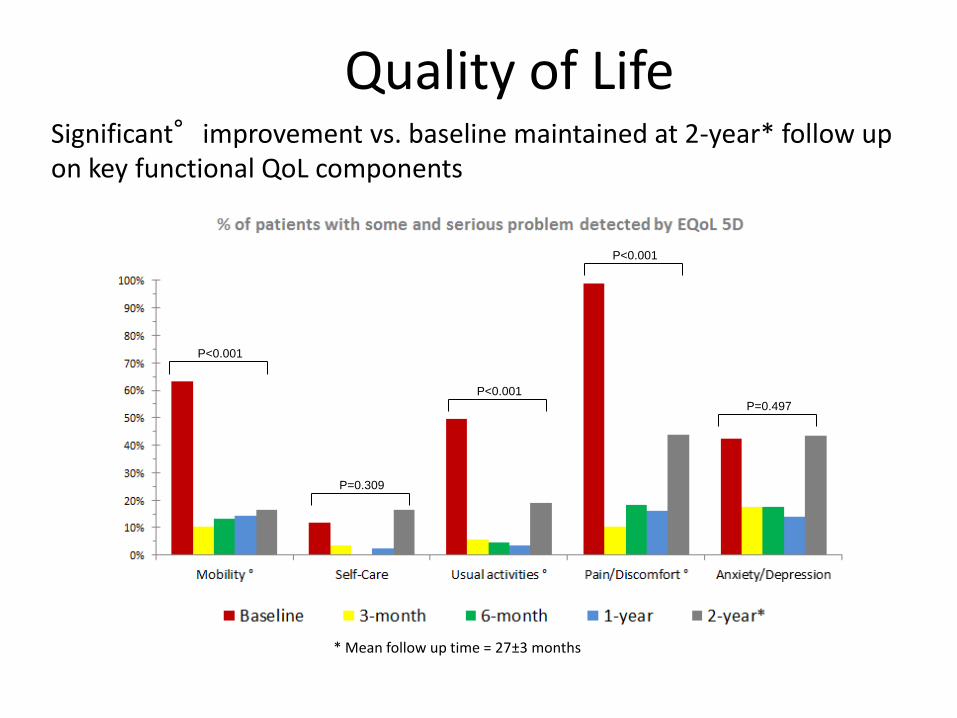
Quality of Life
P<0.001
P<0.001
P=0.309
P<0.001
P=0.497
Significant°improvement vs. baseline maintained at 2-year* follow up on key functional QoL components
* Mean follow up time = 27±3 months
DEB: where else and how to use it
+ Conclusions

BTK restenosis: how to stop the clock... • Refractory, relapsing restenosis
patency
restenosis 6w
(PTA) 4m
(Stent) 5m
(PTA)
RC5 Left
6m (DEB)
6m after IN.PACT Amphirion™:
courtesy of Andrej Schmidt MD
Conclusions
• CLI is a complex multifactorial disease requiring multidisciplinary approach
• Vessel patency remains necessary but not sufficient for wound healing and limb salvage
• DEB is the only device able to treat long lesions BTK while “leaving nothing behind”
• DEB showed optimal results in SFA lesions of primary and secondary patency
• Early DEB data show reduction of angiographic restenosis rates and TLR
• Further study results are awaited to better understand the role of DEB in BTK/CLI
Thank You for your attention