drug handling in kidney and liver disease
DESCRIPTION
Drug Handling in kidney and liver disease. Dr. Geoff Isbister. Drug Action. Drugs tend to be small lipid-soluble molecules Drugs must get access to sites of action Drugs tend to bind to tissues, usually protein molecules Drugs alter the actions of enzymes, ion channels and receptors. - PowerPoint PPT PresentationTRANSCRIPT
Drug Handling in kidney and liver disease
Dr. Geoff Isbister

Drug Action
• Drugs tend to be small lipid-soluble molecules
• Drugs must get access to sites of action
• Drugs tend to bind to tissues, usually protein molecules
• Drugs alter the actions of enzymes, ion channels and receptors

Drug Action
• ENZYME: example Angiotensin Converting enzyme inhibitors A I ----
X---------->A II lowered A II -----> Reduced BP
• ION CHANNELS: example Local Anesthetics
Block Na channels--->Anesthesia
• Receptor Binding– Receptors are specialised binding sites - often on cell
surface- which have specificity for certain substances (incl drugs). Drugs may activate or block the receptor
– Activation of the receptor changes the activity of the cell: eg adrenaline activates the beta 1 receptors in the heart and speeds up the heart
– Drugs have selectivity for receptors: eg Histamine2 antagonists- reduce histamine-induced acid secretion and heal peptic ulcers

Pharmacokinetics
• The study of the action of the body on the drugs• Pharmacokinetics is the study of the time course
of concentrations of drug in the body• The way the body handles drugs determines the
dose, route and frequency of administration• The handling of drugs by the body can be split
into absorption, distribution and elimination

Pharmacokinetics
• Rate of absorption determines the time to the peak concentration
• The extent of absorption determines the height of the peak concentration and the AUC 0
5
10
15
20
25
30
0 1 5 9 13
Time after dosing

Pharmacodynamics
• The response of the tissue to the active free concentration of drug present at the site of action
• May also be changed by disease processes

Type of Disease
• Renal disease – the nature of the disease doesn’t matter very much, the main determinant is the decline in GFR

• Some drugs are water-soluble and are eliminated directly by the kidney– Molecules with MW below 20000 diffuse into glom
filtrate. – examples: gentamicin, digoxin, atenolol– involves no chemical change to the drug – in most cases occurs by filtration (and depends on
the GFR)– in a few cases (eg penicillin) some tubular secretion
contributes to elimination
• Highly lipid-soluble drugs are filtered into the tubules and then rapidly re-absorbed– High protein binding will reduce filtration
Routes of elimination - Kidney

• Assessing kidney function is straightforward– serum creatinine reflects GFR– relationship between serum creatinine and
GFR changes with age
Practical issues - treating real patients
Effects of age on renal function
• There is a steady and proportional decline in average GFR with increasing age
• However the serum creatinine remains unchanged
• Why is this?

Effects of age on renal function (constant serum creatinine of 0.10
mmol/l)
010
20
30
4050
60
70
80
90100
20 40 60 80

Multiple Dosing - renally excreted drug
00.1
0.2
0.3
0.40.5
0.6
0.7
0.80.9
1
0 12 24 36 48 60 72 84 96
Approx 5 half-lives to reach steady state
Elderly

Drug Types
• Water soluble - excreted unchanged (by
the kidney)
• Lipid soluble - filtered but fully reabsorbed in the kidney- metabolised to polar products (filtered without
reabsorption)

A number of drugs are handled by tubular mechanisms
• Two mechanisms– Active tubular secretion – important
• Acidic drugs – frusemide, methotrexate, penicillins, salicylate, uric acid, probenecid
• Bases – amiloride, morphine, quinine
• Passive diffusion– After filtration lipid-soluble drugs will be re-absorbed
passively.– Will depend on degree of ionization at certain pH
levels

Practical Examples of dosing in renal failure

Gentamicin• Practice is changing - trend to once/daily dosing• The interval between doses may be >24 hours
in the presence of renal failure and in the elderly• Toxicity relates to trough concentrations,
particularly with prolonged therapy• Toxicity mainly affects the kidney and 8th
cranial nerve

Digoxin
• In the presence of renal impairment the dose must be reduced
• The dose is given once daily
• Elderly people almost invariably have some renal impairment, so they usually require dose reduction - normally a halving of dose compared with young people
Summary
• Reduced elimination of drugs from the body in the elderly will lead to accumulation and toxicity
• Disease and old age lead to reduced renal elimination of water-soluble drugs
• Co-morbidity and concomitant drug therapy

Hepatic Disease
• Metabolism by the Liver :– role of metabolism– types of metabolism
• Clearance– hepatic clearance
• Liver disease
Type of Disease
• In liver disease the type of disease does matter:– Hepatitis – not much effect– Biliary obstruction – not much effect (initially)– Cirrhosis – has major effects on drug handling

Assessing Function
• Assessing liver function is hard - no single test of how well the liver metabolises drugs– Drug metabolism most likely to be impaired
when the patient has cirrhosis, and has evidence of coagulation disturbances and low albumin

Biotransformation
• Majority produces metabolites that are :– less active– more polar and water soluble
• Minority :– Pro-drugs that require metabolism to be active– active metabolites– more toxic (mutagenic, teratogenic etc.)
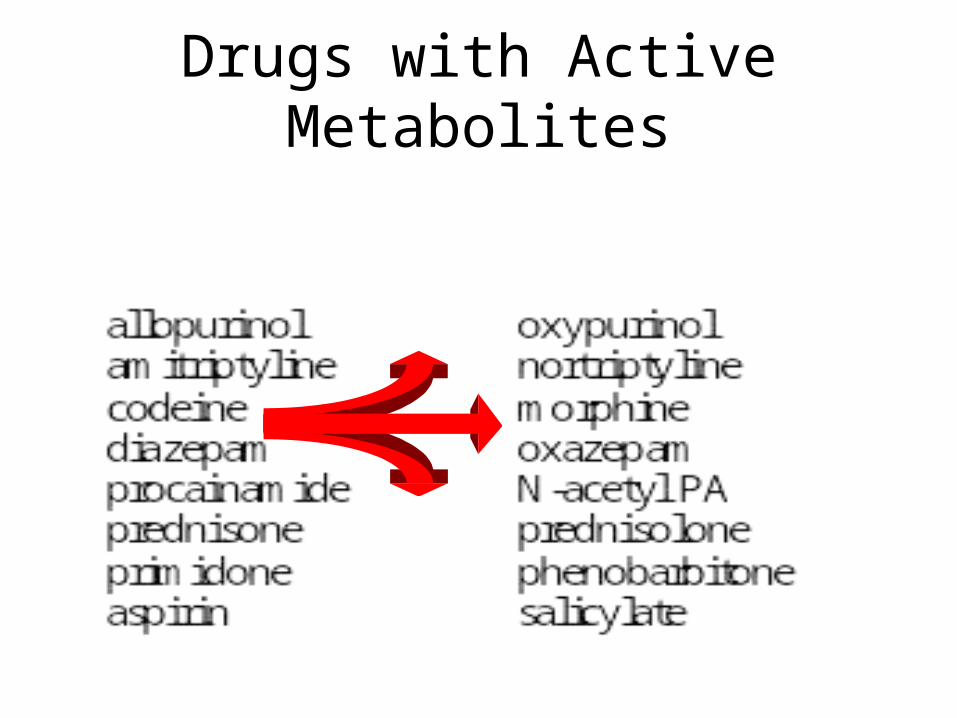
Drugs with Active Metabolites

Types of Metabolism
• Phase 1 Reactions– usually convert the parent drug into a more polar
metabolite by introducing or unmasking a functional group (-OH, -NH2, -SH). Metabolite is usually inactive.
• Phase 2 Reactions - Conjugation– an endogenous substrate (glucuronic acid,
sulfuric acid, acetic acid, or amino acid) is attached to a functional group on the drug or phase I metabolite.
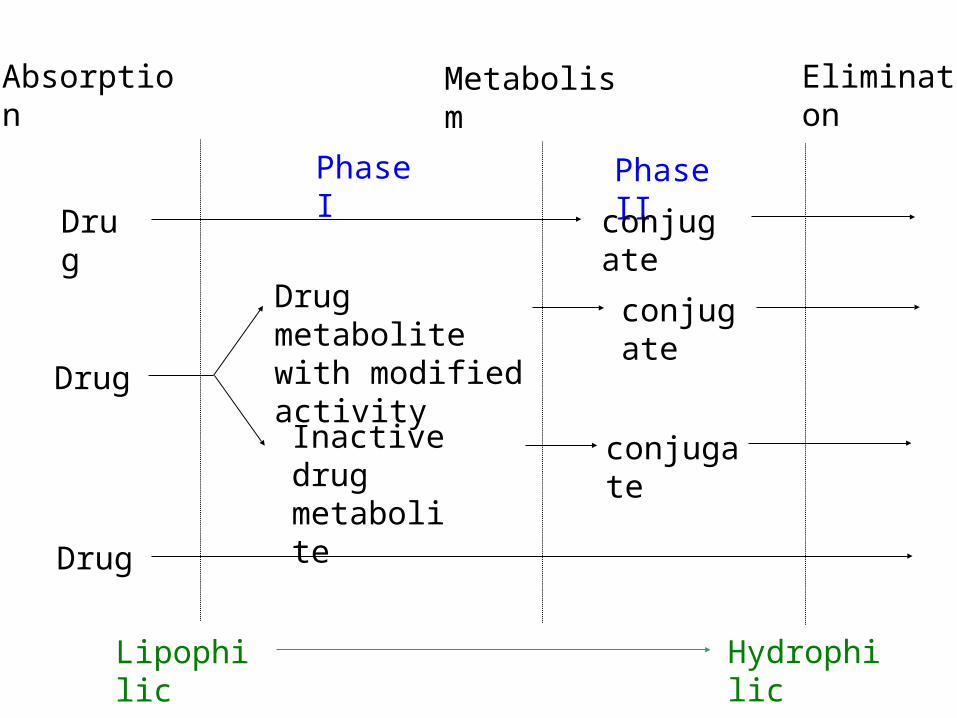
conjugate
Phase I Phase II
Drug metabolite with modified activity
Inactive drug metabolite
conjugate
Drug
Drug
Drug
conjugate
Lipophilic Hydrophilic
Absorption Metabolism Elimination
Phase I Reactions
• Mixed Function Oxidase:– P450 enzyme system– induced and inhibited– hydroxylation and demethylation– family of isoenzymes
• Monoamine Oxidase : catecholamines
• Dehydrogenases :eg. Alcohol dehydrogenase

Phase I - P450 System
• FRAGILE
• High specificity
• Low volume
• Energy dependent
• First affected by liver disease
Cytochrome P450 System
• Not a single entity
• Family of related isoenzymes (about 30)
• Important for drug interactions :– Enzyme induction– Enzyme inhibition
• Genetic polymorphism

Phase II ReactionsConjugation
• Glucuronidation
• Sulfation
• Acetylation
• Glutathione
• Glycine

Phase II ReactionsConjugation
• ROBUST
• High volume
• Low specificity
• Not energy dependent
• Less effected by liver disease

Paracetamol toxicity – failure of Phase II
NAPQI accumulates and binds to tissue macromolecules - cell death
Conjugation pathway saturates
oxidation by P450 cytochrome pathway
Formation of toxic metabolite NAPQI
Initially detoxified by glutathione
Glutathione depletion
Sites of Biotransformation
• Liver• Lung
• Kidney
• Large and small intestine
• Placenta
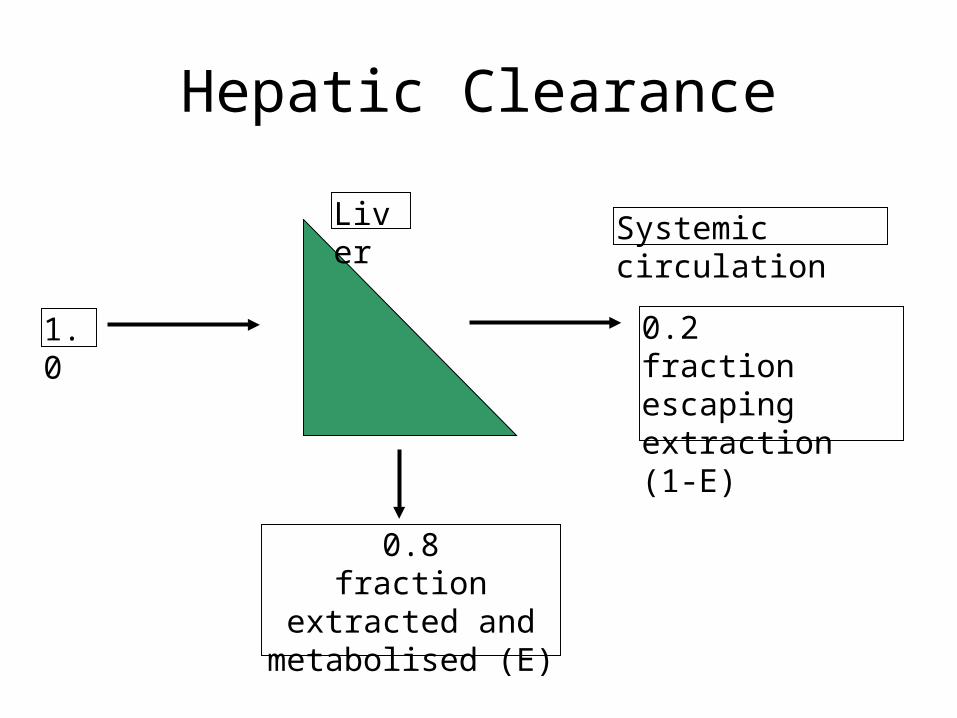
Hepatic Clearance
Liver Systemic circulation
0.2fraction escaping extraction (1-E)
1.0
0.8fraction extracted and
metabolised (E)

Extraction Ratio
• High extraction ratio :– Effectively removed by the liver– Limited by hepatic blood flow– High first pass metabolism – Eg. Lignocaine, propranolol, diltiazem,
morphine– Less effected by changes in intrinsic
clearance, such as induction and inhibition
Extraction Ratio
• High Extraction ratio– Clearance approximates organ blood flow
• Low Extraction ratio– Clearance proportional to free drug in the
blood and intrinsic clearance of the liver

Liver Disease
• Severe disease before major effects on metabolism
• Liver Disease :– Hepatocellular disease– Decrease liver perfusion
• Type of metabolism :– Phase I– Phase II

Disease Factors
• Disease Type :– Acute hepatitis – little effect– Biliary Obstruction – little effect – Chronic Active Hepatitis – major effects– Cirrhosis – major effects
• Indicators :– Established cirrhosis, varices, splenomegaly,
jaundice, increased prothrombin time.

Disease Factors
• Poor perfursion
• Cardiac failure : limits blood flow so effects those with high extraction ratios– Eg. Lignocaine– Combination with ischaemic liver injury
• Other low perfusion states :– Other causes of shock

Recent theories to account for impaired metabolism in cirrhosis
• Intact hepatocyte mass
• Sick cell theory
• Impaired drug uptake/shunting theory
• Oxygen limitation theory

Type of Metabolism
• Phase I, mainly P450– Affected first
• Phase II– Severe disease before any effect– Eg. Paracetamol poisoning.

Other considerations
• Renal function may be impaired in moderate to severe liver disease– Creatinine levels are not predictive
• Pro-drug metabolism impairment– Eg ACE inhibitors
• Pharmaco-dynamic disturbances– Tissues may be excessively sensitive to
even low concentrations of the drug – eg morphone in the brain in the presence of severe liver disease