drug interactions in managing hiv/hcv...
TRANSCRIPT

Drug Interactions in Managing HIV/HCV Co-InfectionPresenter: Christopher Keeys, Pharm.D., BCPS
28 October 2015

Drug-Drug Interactions between Direct Acting Antiviral (DAA) and Antiretroviral Therapy (ART) in
HIV/HCV Co-infected Patients
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.
P R E S E N T E R : C H R I S T O P H E R K E E Y S , P H A R M . D . , B C P S
P R E S I D E N T , C L I N I C A L P H A R M A C Y A S S O C I A T E S , I N C .C E O , M E D N O V A T I O N S , I N C .
P R E S E N T A T I O N B Y : X I R U I C H E N , P H A R M . D . , P R A C T I C E F E L L O W

Disclaimer
No conflict of interest to disclose by presenters
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

Objectives
Identify the basic epidemiology of chronic hepatitis C (CHC) infection and CHC/HIV coinfection in the population
Recognize the availability and clinical importance of newer direct acting antivirals (DAAs) in the medical management of CHC and CHC/HIV infections
Identify and discuss the importance of DAA and antiretroviral (ARV) drug drug interactions in the management of CHC and CHC/HIV
Identify and utilize basic pharmacologic and pharmacokinetic information to minimize drug interactions in care of patients
Recognize and support medication management strategies that limit drug interactions and adverse health outcomes for patients
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

Background on HCV
Epidemiology: An estimated 2.7 million persons in the United States have chronic hepatitis C virus infection (all genotypes). Approximately 75%–85% of people who become infected with Hepatitis C virus develop chronic infection1,2,3
Screening: people with risk factors and all patients with HIV infections3
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

Risk Factors2,3
Recipient of blood transfusions and organ transplants before July 1992 (no screening tools available prior to 1992)
IV drug use Sexual exposure Other, including occupational
exposure and perinatal exposure
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

HIV/HCV Co-infection4
Statistics: 50%–90% of HIV IV drug users are co-infected with HCV due to common route of transmission (IV drug use); 25% overall coinfection in population in the USA
Prognostics of co-infection: Lower rate of spontaneous clearance of virus during acute infection due to low CD4 counts HIV/HCV coinfection accelerates hepatic fibrosis in HCV infected patients, and poor outcomes
following transplantation Higher rate of liver decompensation in HIV/HCV co-infected patients, especially in the
absence of ART (e.g. ascites, spontaneous bacterial peritonitis, etc.) Higher liver-related mortality rates in HIV-infected patients.
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

Direct Acting Antivirals (DAAs)2,5,6
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

What’s the Holdup? Evidence?6
MANY drug interactions between DAA and antiretroviral therapy (ART) limit patient’s choice of treatment options By understanding the basic mechanism of
interactions will allow a healthcare provider to choose a therapy that is effective and safe for the patient
FDA approval USPHS, AASLD and IDSA guidance
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.
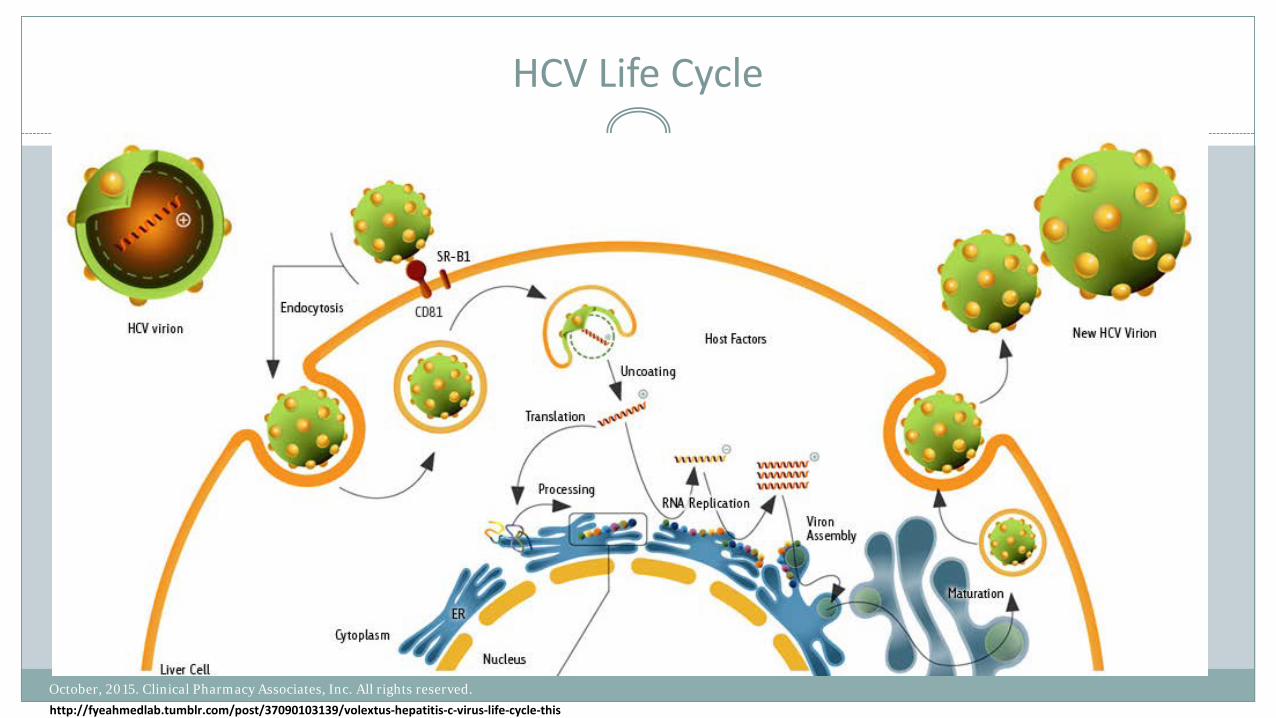
HCV Life Cycle
http://fyeahmedlab.tumblr.com/post/37090103139/volextus-hepatitis-c-virus-life-cycle-thisOctober, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

HCV Pharmacological Targets2
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.
http://fyeahmedlab.tumblr.com/post/37090103139/volextus-hepatitis-c-virus-life-cycle-this

Oral anti-HCV pharmacological agents
Name Mechanism of Action
Approved Indication Dosing
Simeprevir(OLYSIO®)7
NS3/4A protease inhibitors
CHC genotype 1 or 4 infection in combination with PEG-IFN alfa and ribavirin
150 mg daily with food
Not recommended in patients with moderate to severe hepatic impairment
Sofosbuvir (SOVALDI®)8
NS5B polymerase inhibitor
CHC genotypes 1, 2, 3, and 4 infection in combination with ribavirin and/or PEG-IFN alfa
HCV/HIV-1 co-infection
400 mg daily
No dose adjustment required for mild to moderate renal impairment (eGFR >30 ml/min/1.73m2)
No dose adjustment required for any degree of hepatic impairment
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

Oral anti-HCV pharmacological agents
Name Mechanism of Action
Approved Indication Dosing
Ledipasvir/Sofosbuvir (HARVONI ®)9
NS5A protein inhibitor/NS5B polymerase inhibitor
CHC genotype 1 infection Ledipasvir/Sofosbuvir: 90/400 mg fixed dose, one tablet daily
No dose adjustment required for mild to moderate renal impairment (eGFR >30 ml/min/1.73m2)
No dose adjustment required for any degree of hepatic impairment
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

Oral anti-HCV pharmacological agents
Name Mechanism of Action
Approved Indication Dosing
Paritaprevir/rOmbitasvirDasabuvir(VIEKIRA PAK®)10
NS3/4Aprotease inhibitor/NS5A proteininhibitor/NS5Bpolymerase inhibitor
CHC genotype 1 infection with or without ribavirin
• Ombitasvir, paritaprevir, ritonavir: 12.5/75/50 mg fixeddose, one tablet daily in the morning
• Dasabuvir: 250 mg morning and evening
No dose adjustment required for any degree of renal impairment
No dose adjustment required for mild hepatic impairment. Contraindicated in patients with moderate tosevere hepatic impairment
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

Oral anti-HCV pharmacological agents
Name Mechanism of Action
Approved Indication Dosing
Daclatasvir(DAKLINZA®)11
NS5A protein inhibitor
CHC genotype 3 infection in combination with sofosbuvir
60 mg once daily, taken with sofosbuvir
No dose adjustment required for any degree of renal impairment
No dose adjustment required for any degree of hepatic impairment
Ombitasvir/paritaprevir/ritonavir(TECHNIVIE®)12
NS5A protein inhibitor/NS3/4A protease inhibitor/CYP3A inhibitor
CHC genotype 4 infection in combination with ribavirin
Ombitasvir, paritaprevir, ritonavir: 12.5/75/50 mg fixed dose tablet, 2 tablets once daily in the morning with food
No dose adjustment required for any degree of renal impairment
No dose adjustment required for mild hepatic impairment. Contraindicated in patients with moderate to severe hepatic impairment
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

Why so many DDI?
Protein (enzyme/transporter) induction and inhibition
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.
https://en.wikipedia.org/wiki/Membrane_transport_protein#/media/File:Scheme_facilitated_diffusion_in_cell_membrane-en.svghttp://classes.midlandstech.edu/carterp/Courses/bio225/chap05/ss2.htm

Sample Pharmacokinetics Study13
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

Pharmacokinetics of DAA7-18
DDA Substrate of … Metabolized by … Inhibitor of …
Simeprevir (OLYSIO®) P-gp, BCRP, OATP1B1, MRP2 CYP3A CYP2A6, CYP2C8, CYP2D6CYP2C19, CYP3AP-gp, BCRP, OATP1B1, MRP2
Sofosbuvir (SOVALDI®) P-gp, BCRP (active metabolite not affected)
Not metabolized by CYP P-gp
Ledipasvir/Sofosbuvir(HARVONI®)
P-gp, BCRP Not metabolized by CYP P-gp, BCRP
Paritaprevir/rOmbitasvirDasabuvir(VIEKIRA PAK®)
P-gp, BCRP, OATP1B1/B3 CYP3A CYP3A (ritonavir), P-gp, BCRP,OATP1B1/B3
P-gp Amide hydrolysisoxidative metabolism
P-gp, BCRP CYP2C8, CYP3A P-gp, BCRP
Daclatasvir (DAKLINZA®) P-gp, BCRP, OATP1B1/B3 CYP3A P-gp,BCRP, OATP1B1/B3
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

Summary of DAA and ARV interactions7,14,15,17,18
DAA ARV Mechanism of Interaction
Effect on DAA Effect on ART Comment
Simeprevir(OLYSIO®)
Efavirenz, Etravirine, Nevirapine
CYP3A4 induction by ARV
↓ Simeprevir No significant effect on ART
Co-administration not recommended
Stribild (boosted with COBI)
CYP3A4 Inhibition by COBI
↑ Simeprevir
Ritonavir containing combination
CYP3A4 inhibition by ritonavir
↑ Simeprevir (AUC: ↑159%, Cmax:↑79%, Cmin: ↑358%)
In general, not recommended to coadminister with moderate to severe CYP3A inhibitors (e.g. anticonvulsants, dexamethasone, azoleantifungals, macrolide antibiotics etc.) of CYP3A inhibitors (e.g. phenytoin, carbamazepine, rifampin, St. John’s Worts). No significant interactions with tacrolimus or cyclosporine, therefore, it may be a good choice for patients who underwent liver transplants.
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

Summary of DAA and ARV interactions8,9,15,17,18
DAA ARV Mechanism of Interaction
Effect on DAA Effect on ART Comment
Sofosbuvir (SOVALDI ®)
Tipranavir/r P-gp induction by tipranavir/r
↓ sofosbuvir No significant effect on ART
Co-administrationnot recommended
Ledipasvir/Sofosbuvir (HARVONI ®)
Tenofovir P-gp inhibition by ledipasvir
No significant effect on DAA
↑ Tenofovir Co-administrationwith Stribild® not recommended
Atazanavir/r P-gp inhibition by Atazanavir/r
↑ Ledipasvir ↑ Atazanavir Consider alternativetherapy
Tipranavir/r P-gp induction bytipranavir
↓ Ledipasvir/sofosbuvir
No significant effect on ART
Co-administrationnot recommended
In general, not recommended to coadminister with P-gp inducers (e.g. rifampin, St. John’s wort). SOVALDI® has relatively few significant interactions with ART, may be a good choice for HIV/HCV co-infected patients receiving ART. No significant interaction with tacrolimus or cyclosporine, therefore, it may be a good choice for patients who underwent transplants.
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

Summary of DAA and ARV interactions10,13,16,17,18
DAA ARV Mechanism of Interaction
Effect on DAA Effect on ART Comment
Paritaprevir/rOmbitasvirDasabuvir(VIEKIRA PAK®)
Protease Inhibitors (Atazanavir/r, Darunavir, Lopinavir/r)
CYP3A inhibition by Ritonavir
↑ Paritaprevir↑ or ↓ Ombitasavir↓ Dasabuvir
↑ Atazanavir↑ Lopinavir
Dose Atazanaviralone without COBI or Ritonavir boost
NNRTIs (Rilpivirine)
3A4 induction Predicted ↓ DAA ↑ Rilpivirine Co-administration not recommended
Elvitegravir, Stribild 3A4 inhibition by Ritonavir
Predicted ↑ ART
Maraviroc 3A4 inhibition by Ritonavir
Predicted ↑ ART
In general, not recommended to co-administer with CYP3A inducers (e.g. Phenytoin, Carbamazepine, Rifampin, etc.) or substrates. Co-administration with strong CYP2C8 inhibitor (e.g. Gemfibrozil) is contraindicated.
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.
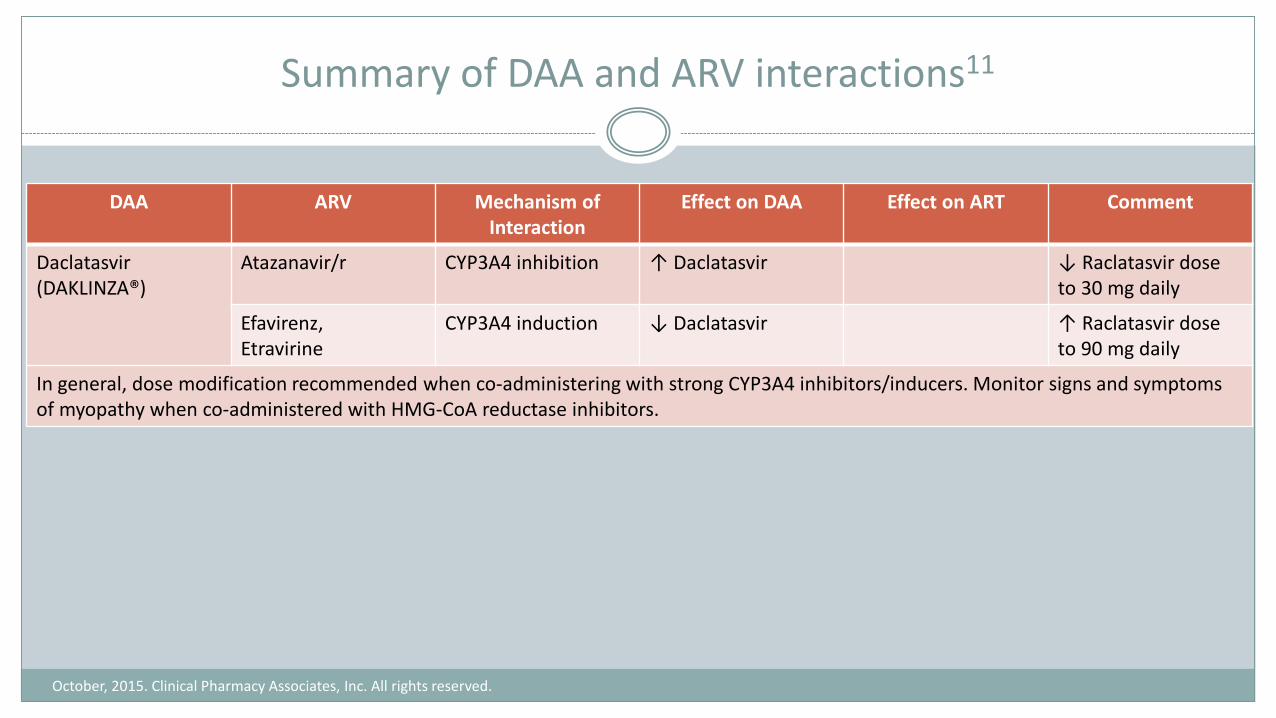
Summary of DAA and ARV interactions11
DAA ARV Mechanism of Interaction
Effect on DAA Effect on ART Comment
Daclatasvir(DAKLINZA®)
Atazanavir/r CYP3A4 inhibition ↑ Daclatasvir ↓ Raclatasvir dose to 30 mg daily
Efavirenz,Etravirine
CYP3A4 induction ↓ Daclatasvir ↑ Raclatasvir dose to 90 mg daily
In general, dose modification recommended when co-administering with strong CYP3A4 inhibitors/inducers. Monitor signs and symptomsof myopathy when co-administered with HMG-CoA reductase inhibitors.
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

Commonly co-prescribed drugs16
Oral contraceptives: metabolized by CYP3A, CYP2C9 Cyclosporine/Tacrolimus: metabolized by CYP3A, substrate for P-gp Selective Serotonin Reuptake Inhibitors : CYP2D6 inhibition Methadone: CYP3A4 substrate Digoxin: P-gp substrate “Statins”: CYP3A4 substrate Antimicrobials: CYP3A4 inhibitor P-gp inhibitor (e.g. azithromycin, azole
antifungal)
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

Prescribing (Selection of Agents )19
Efficacy- genotype (FDA, USPHS, guidelines) Comorbidities and HIV treatment status Prior Treatment Stage of fibrosis Route (e.g. injections vs oral/ both) Duration Contraindications/ Precautions/Warnings Adverse Drug Events Drug-Drug Interactions Access (Formulary status; insurance) and Cost
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

Dispensing
Pharmacist play pivotal role in evaluating the appropriateness of selection of agents, patient access and continuum of care Record and review COMPLETE and UP-TO-DATE list of patient’s medication,
including OTC products; especially at transitions in care (medication reconciliation) Timely communication with prescribers and other healthcare providers Patient education on adverse drug events and adherence Continuing education on newly approved DAA agents with better efficacy, safety and
fewer DDIs
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

Administration
DDI may alter oral absorption; check for …….. Avoidance of concomitant medication administrations Spacing of medications Taking with or without meals; special dietary adjustments Daily timing of medication administration to maximize treatment benefit Daily timing of medication administration to minimize adverse effects Special administration needs e.g., young children, tube feeding, impaired swallowing,
poor vision (look- alike/side alike medications)
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

Monitoring19
Adherence HCV RNA quantitative testing at week 4 Re-evaluate at week 6 if level was detectible at week 4 Week 12 level (end of therapy) level is unnecessary since most patient will achieve sustained
virologic response (SVR); exception is patients needing >/= 24 weeks Prescription fills, refills, mean possession rate (MPR), direct observation, etc.
Toxicity Lab work at baseline (CBC, BMP, liver enzyme and bilirubin levels) Routinely throughout the treatment (weeks 2,4,8,12 or more often if abnormal/concerning
lab results) Recommend treatment discontinuation for serious adverse effects, e.g., if AST >10x baseline,
or hyperbilirubinemia
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

Common Adverse Drug Reactions
DAA ADR (>5%) Labeled Warning
Simeprevir (OLYSIO®)7 Rash, pruritus, nausea, myalgia, dyspnea
Hepatic decompensation and hepatic failure. Usually within 1-4 weeks in therapy initiation. Not recommended in patients with severe cirrhosis.
Serious photosensitivity reactions resulting in hospitalization have been observed with OLYSIO in combination with Peg-IFN-alfa and RBV. Simeprevircontains sulfa-moiety, use caution in patients with sulfa allergy.
Paritaprevir/rOmbitasvir/ Dasabuvir(VIEKIRA PAK®)10
Fatigue, nausea, pruritus, skin reactions, insomnia, asthenia
Hepatic decompensation and hepatic failure. Usually within 1-4 weeks in therapy initiation. Not recommended in patients with severe cirrhosis.
Sofosbuvir (SOVALDI®)8 Headache, fatigue,diarrhea, nausea, insomnia, pruritus, decreased appetite
Serious symptomatic bradycardia has been reported in patients taking amiodarone who initiate treatment with sofosbuvir in combination with another HCV direct-acting antiviral.Ledipasvir/Sofosbuvir
(HARVONI®)9
Daclatasvir (DAKLINZA®)11
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

Case Example20 - #1Appreciation of the extent of potential DDI
Study Design: Cross sectional study among HIV/HCV co-infected patients Method:
1. Medications lists were collected from medical records2. Medication lists were entered into Lexi-Interact drug interaction software 3. Documented contraindicated DDI (XDDI) before/after the addition of either simeprevir or
sofosbuvir containing therapy Results: Before the addition of any HCV therapy: 20% patients had XDDIs Addition of simeprevir containing therapy: 88.4% (p<0.001) patients had XDDIs Addition of Sofosbuvir containing therapy: 24.5% (p<0.001) patients had XDDIs
NNRTI regimen (PR: 1.62; 95% CI: 1.38-1.91, p<0.001), PI regimen (PR: 1.64; 95% CI: 1.40-1.93, p<0.001), and ≥7 non-HIV medications (PR: 1.06; 95% CI: 1.00-1.14, p=0.09) were all associated with higher prevalence of XDDs.
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

Case Example21 - #2How to predict interactions
Many interactions can be predicted if healthcare professionals taking care of patients have an understanding of the mechanism of proposed interaction
DAA ART Mechanism of Interaction
Predicted Result Actual Result Recommend
Daclatasvir 60 mg daily
Atazanavir/Ritonavir
CYP3A4 inhibition ↑ Daclatasvir ↑ 3x AUC ↓ Daclatavir to 30 mg daily
Daclatasvir 60 mg daily
Efavirenz CYP3A4 induction ↓ Daclatasvir ↓ 2x AUC ↑ Daclatavir to 90 mg daily
Daclatasvir 60 mg daily
Tenofovir No effect on CYP3A4
No DDI No clinical significant DDI
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

Case Example22 - #3Pay attention to labeled warnings
Sofosbuvir has labeled warning regarding severe bradycardia when administered in combination with amiodarone.
Patient was on amiodarone and propranolol; 2 hours after the patient had received Sofosbuvir and Daclatasvir, the patient experienced severe bradycardia, heart rate was recorded as 27 beats/min. Amiodarone and propranolol were subsequently stopped, but DAA were continued for 3 days. Each time patient received DAA, he would demonstrate bradycardia. Upon discontinuation of Sofosbuvir and Daclatasvir, no bradycardic events were observed. Thirteen days after patient has stopped amiodarone and atenolol, patient was challenged with DAA, bradycardia was again recorded after 2 days. No bradycardic events were observed following a challenge 8 weeks after discontinuation of amiodarone.
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

Q&A
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved. http://hirecall.com/wp-content/uploads/2013/02/Questions1-1030x679.jpg

Database of Antiretroviral Drug Interactions
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.
http://arv.ucsf.edu/

References
1. Hepatitis C FAQs for the Public. Center for Disease Control and Prevention. http://www.cdc.gov/hepatitis/hcv/cfaq.htm. Updated October 15, 2015. Accessed October 20, 2015.
2. Hepatitis C. http://emedicine.medscape.com/article/177792-overview#a5. Medscape. Updated August 03, 2015. Accessed October 20, 20153. HCV Guidance: Recommendations for Testing, Managing, and Treating Hepatitis C. HCV Testing and Linkage to Care. IDSA and AASLD and IAS-USA.
http://www.hcvguidelines.org/full-report/hcv-testing-and-linkage-care. Updated June 28, 2015. Accessed October 20, 2015. 4. Chopra S, Muir A. Treatment regimens for chronic hepatitis C virus genotype 1. UpToDate. http://www.uptodate.com/contents/treatment-regimens-for-
chronic-hepatitis-c-virus-genotype-1?source=search_result&search=hepatitis+C&selectedTitle=3~150. Updated July 31, 2015. Accessed October 19, 2015. 5. Hepatitis C Treatment. Hep Your Guide to Hepatitis. http://www.hepmag.com/pdfs/hepatitis_c_drug_list.pdf. Updated September 2015. Accessed October
20, 2015. 6. EASL Recommendations on Treatment of Hepatitis C 2015. J Hepatol. 2015;63:199–2367. Prescribing Information for OLYSIO®. Janssen. https://www.olysio.com/shared/product/olysio/prescribing-information.pdf. Updated October 2015. Accessed
October 18, 2015.8. Prescribing Information for SOVALDI®. Gilead Sciences. http://www.gilead.com/~/media/Files/pdfs/medicines/liver-disease/sovaldi/sovaldi_pi.pdf. Updated
August 2015. Accessed October 18, 2015. 9. Prescribing Information for HARVONI®. Gilead Sciences. https://www.gilead.com/~/media/Files/pdfs/medicines/liver-disease/harvoni/harvoni_pi.pdf.
Updated March 2015. Accessed October 18, 2015. 10. Prescribing Information for VIEKIRA PAK®. AbbVie. http://www.rxabbvie.com/pdf/viekirapak_pi.pdf. Updated October 2015. Accessed October 18, 2015. 11. Prescribing Information for DAKLINZA®. Bristol-Myers Squibb. http://packageinserts.bms.com/pi/pi_daklinza.pdf. Updated July 2015. Accessed October 18,
2015.12. Prescribing Information for TECHNIVIE®. AbbVie. http://www.rxabbvie.com/pdf/technivie_pi.pdf. Updated October 2015. Accessed October 18, 2015.
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.

References
October, 2015. Clinical Pharmacy Associates, Inc. All rights reserved.
13. Menon RM, Badri PS, Wang T, Polepally AR, Zha J, Khatri A. Drug-drug interaction profile of the all-oral anti-hepatitis C virus regimen of paritaprevir/ritonavir, ombitasvir, and dasabuvir. J Hepatol. 2015 Jul;63(1):20-9.
14. Ouwerkerk-Mahadevan S, Snoeys J, Peeters M, Beumont-Mauviel M, Simion A. Drug-Drug Interactions with the NS3/4A Protease Inhibitor Simeprevir. ClinPharmacokinet. 2015. In Press.
15. Kaur K, Gandhi MA, Slish J. Drug-Drug Interactions Among Hepatitis C Virus (HCV) and Human Immunodeficiency Virus (HIV) Medications. Infect Dis Ther. 2015;4(2):159-72
16. Badri PS, King JR, Polepally AR, McGovern BH, Dutta S, Menon RM. Dosing Recommendations for Concomitant Medications During 3D Anti-HCV Therapy. ClinPharmacokinet. 2015. In Press.
17. Hull M, Shafran S, Tseng A, Giguère P, Klein MB, Cooper C. CIHR Canadian HIV Trials Network Co-Infection and Concurrent Diseases Core: Updated Canadian guidelines for the treatment of hepatitis C infection in HIV-hepatitis C coinfected adults. Can J Infect Dis Med Microbiol. 2014;25(6):311-20.
18. Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human Services. http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf. Accessed October 9, 2015. 39-79.
19. Kim Y. Epidemiology, natural history, and diagnosis of hepatitis C in the HIV-infected patient. UpToDate. http://www.uptodate.com/contents/epidemiology-natural-history-and-diagnosis-of-hepatitis-c-in-the-hiv-infected-patient?source=search_result&search=hepatitis+c+hiv&selectedTitle=2~150. Updated December 2014. Accessed October 19, 2015.
20. Patel N, Nasiri M, Koroglu A, Amin R, McGuey L, McNutt LA. Prevalence of drug-drug interactions upon addition of simeprevir- or sofosbuvir-containing treatment to medication profiles of patients with HIV and hepatitis C coinfection. AIDS Res Hum Retroviruses. 2015;31(2):189-97
21. Bifano M, Hwang C, Oosterhuis B, Hartstra J, Grasela D, Tiessen R. Assessment of pharmacokinetic interactions of the HCV NS5A replication complex inhibitor daclatasvir with antiretroviral agents: ritonavir-boosted atazanavir, efavirenz and tenofovir. Antivir Ther. 2013;18(7):931-40
22. Renet S, Chaumais MC, Antonini T, Zhao A, Thomas L, Savoure A. Extreme Bradycardia After First Doses of Sofosbuvir and Daclatasvir in Patients Receiving Amiodarone: 2 Cases Including a Rechallenge. Gastroenterology. 2015; In Press.