drug resistance in - molecular tuberculosis · 1 5 10 50 wt various population drug concen-tration...
TRANSCRIPT

Drug Resistance inDrug Resistance inMycobacterium tuberculosis Mycobacterium tuberculosis ––
Fitness, Laboratory TestingFitness, Laboratory Testingand Beyondand Beyond
Erik C. Böttger
Universität ZürichInstitut für Medizinische MikrobiologieNationales Zentrum für MykobakterienSwitzerland
Tunis 2010 - 2
• Drug resistance and clinical implications
• Drug resistance and fitness
Drug Resistance inMycobacterium tuberculosis
- genetic basis of resistance
- principles of mycobacterial drug susceptibility testing
- laboratory versus clinical resistance
- biological cost of drug resistance
- epidemiological aspects

Tunis 2010 - 3
1. Why is standard short-course therapy reportedly an effectivetreatment for a significant part of multidrug resistant (MDR)tuberculosis?Böttger, E.C. Lancet 2001, 357: 1288-1289
2. Does DOTS (directly observed therapy short-course) work as ameans to control TB in populations with drug-resistanttuberculosis?”Even in settings with moderate rates of MDR tuberculosis, directly observedtherapy (DOTS) can rapidly reduce the transmission and incidence of both drug-susceptible and drug-resistant tuberculosis.“De Riemer, K. et al. Lancet 2005, 365: 1235-1245
Laboratory versus ClinicalResistance
“We found that many control programs that have been the most successful inreducing wild-type sensitive TB (as a result of high case detection and treatmentrates) have paradoxically been the most likely to evolve into hot zones of MDR.”Blower, S.M. and Chou, T. Nature Med. 2004, 10: 1111-1116

Tunis 2010 - 4
1. Critical proportion(proportion method)
2. Critical concentration(drug concentration))
Pecularities of MycobacterialDrug Susceptibility Testing (DST)

Tunis 2010 - 5
Principle of the method
"All strains of tuberculosis contain some bacilli that areresistant to antibacillary drugs - in resistant strains, theproportion of such bacilli is considerably higher than insensitive strains."
Canetti et al. Bull. WHO 1969, 41: 21-43
Drug Critical Proportionfor Resistance %
IsoniazidRifampicinPyrazinamidEthambutolStreptomycin
Concentration(µg/ml)
0.2410024
11101010
The Proportion Method

Tunis 2010 - 6
Antimicrobialagent
Conc(µg/ml)
in serum
Conc (µg/ml)
INHRMPPZAEMBSM
0.05 - 0.20.520
1 - 51
71045
2 - 525 - 50
0.12
1002.52
0.4
7.56
mostly a single drug concentration (termed critical concentration) is used to define susceptibility vs. resistance
The Critical Concentration
MIC(µg/ml) of
susceptibleM. tuberculosis
BACTEC 12Blow
BACTEC 12Bhigh
Tunis 2010 - 7
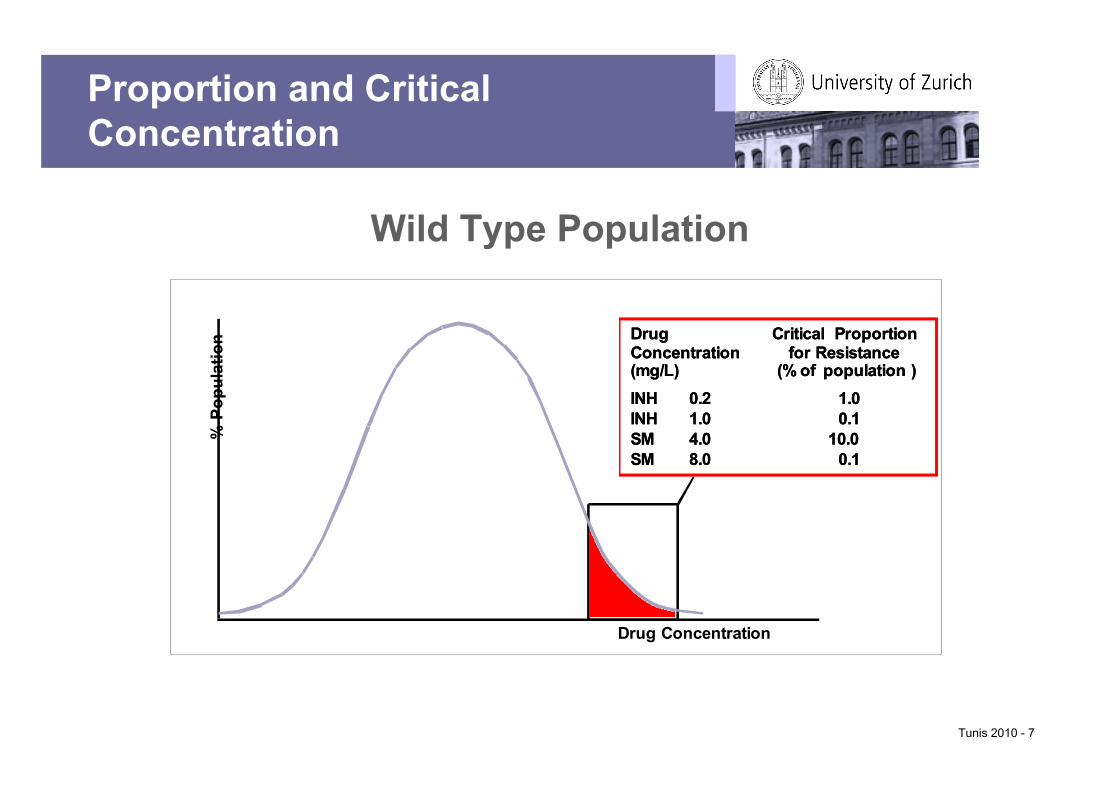
Wild Type Population
Proportion and CriticalConcentration
% P
opul
atio
n
Drug Concentration
Drug Critical ProportionConcentration for Resistance(mg/L) (% of population )
INH 0.2 1.0INH 1.0 0.1SM 4.0 10.0SM 8.0 0.1
Drug Critical ProportionConcentration for Resistance(mg/L) (% of population )
INH 0.2 1.0INH 1.0 0.1SM 4.0 10.0SM 8.0 0.1

Tunis 2010 - 8
Resistance is defined as a decrease in sensitivity
of sufficient degree to be reasonably certain that
the strain concerned is different from a sample of
wild strains of human type that have never come
into contact with the drug.
Mitchison, 1962
Drug Resistance inM. tuberculosis
…, strains that are resistant in this sense do notnecessarily fail to respond.
1 5 10 50
wt population
Drug Concen-tration mg/L
% P
opul
atio
nhigh level resistance,various rpoB mutationse.g. rpoB S531L, H526Y, H526D
1 5 10 20
wt population
low-level resistance,various mutationse.g. Δ gldB
moderate resistancee.g. rrs, rpsL K87 mut
high level resistance,i.e. rpsL K42L
Drug Concen-tration mg/L
% P
opul
atio
n
0.1 1 3 10
wt population
low-level resistance,various mutationse.g. inhA
moderate and high level resistance,various katG mutationse.g. katG S315T
"critical concentrations"
Drug Concen-tration mg/Ldrug serum level
% P
opul
atio
n
C
RIFAMPICIN
STREPTOMYCIN
ISONIAZID
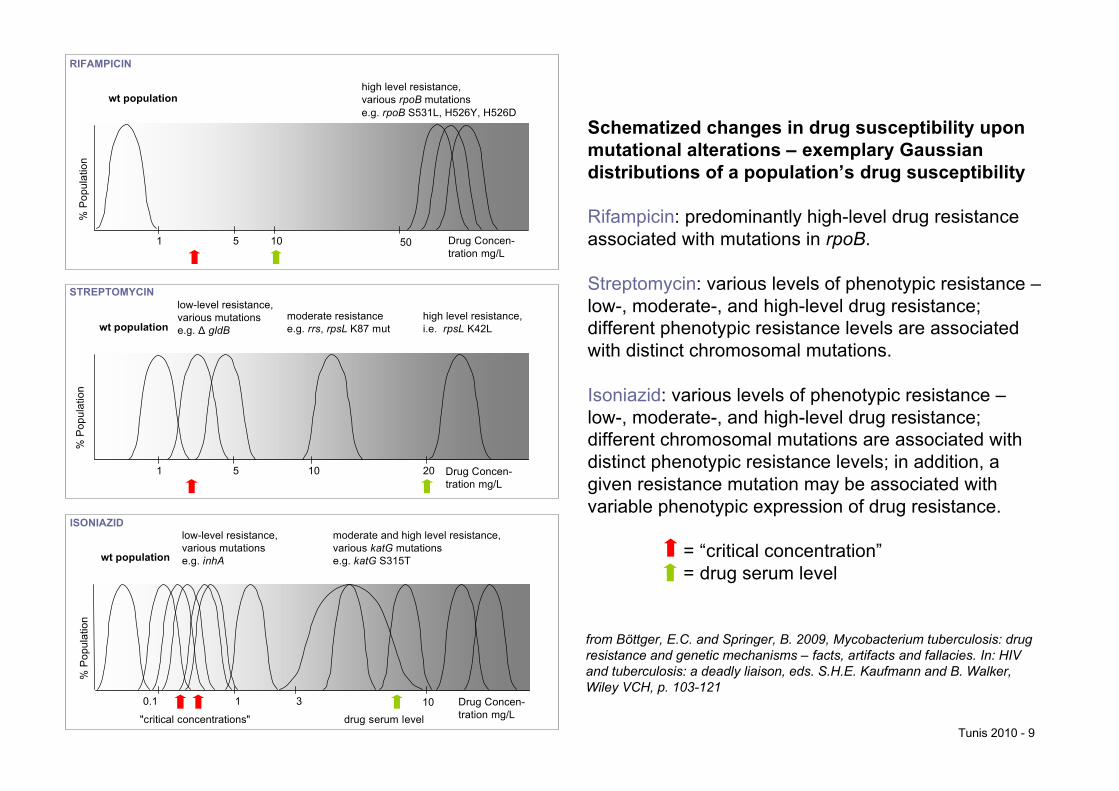
Schematized changes in drug susceptibility uponmutational alterations – exemplary Gaussiandistributions of a population’s drug susceptibility
Rifampicin: predominantly high-level drug resistanceassociated with mutations in rpoB.
Streptomycin: various levels of phenotypic resistance –low-, moderate-, and high-level drug resistance;different phenotypic resistance levels are associatedwith distinct chromosomal mutations.
Isoniazid: various levels of phenotypic resistance –low-, moderate-, and high-level drug resistance;different chromosomal mutations are associated withdistinct phenotypic resistance levels; in addition, agiven resistance mutation may be associated withvariable phenotypic expression of drug resistance.
= “critical concentration”= drug serum level
from Böttger, E.C. and Springer, B. 2009, Mycobacterium tuberculosis: drugresistance and genetic mechanisms – facts, artifacts and fallacies. In: HIVand tuberculosis: a deadly liaison, eds. S.H.E. Kaufmann and B. Walker,Wiley VCH, p. 103-121
Tunis 2010 - 9
Tunis 2010 - 10
>30%tlyACapreomycin
embBeis
gldB
inhA
Geneticlocus
>50%20-30%
20-30%20-30%
Frequency inclinical isolates
EthambutolKanamycin
StreptomycinIsoniazid
Drug
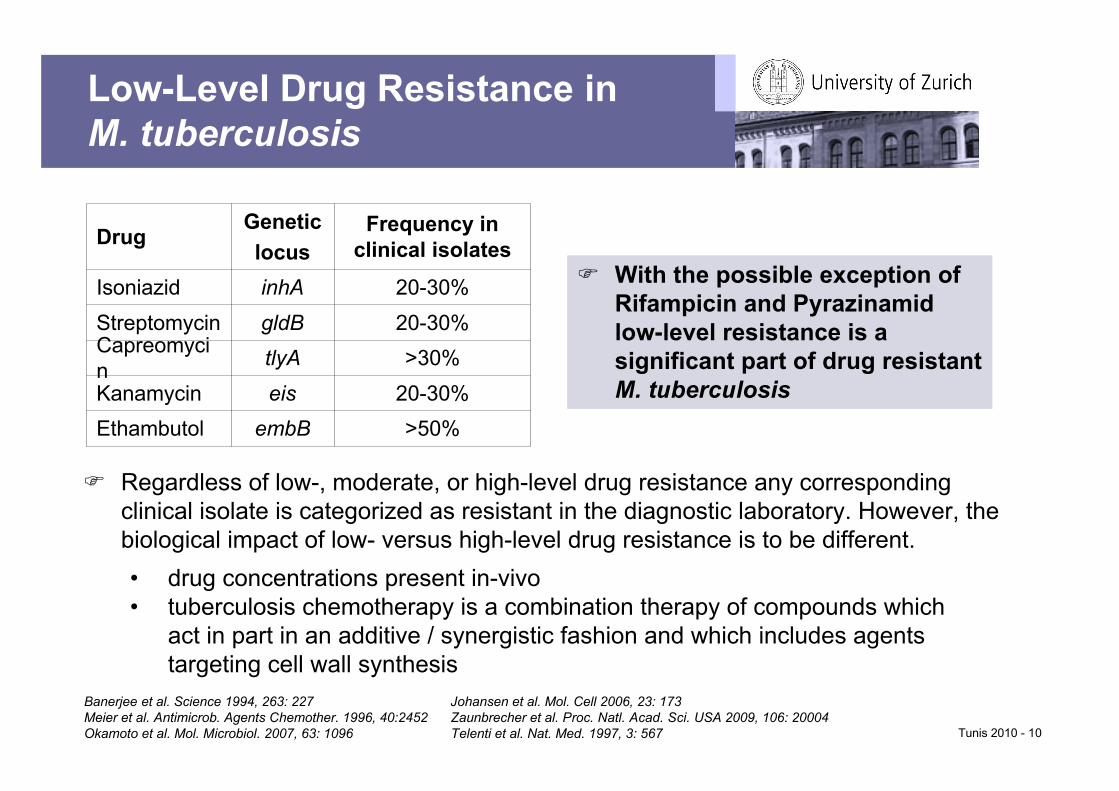
Low-Level Drug Resistance inM. tuberculosis
With the possible exception ofRifampicin and Pyrazinamidlow-level resistance is asignificant part of drug resistantM. tuberculosis
Regardless of low-, moderate, or high-level drug resistance any correspondingclinical isolate is categorized as resistant in the diagnostic laboratory. However, thebiological impact of low- versus high-level drug resistance is to be different.• drug concentrations present in-vivo• tuberculosis chemotherapy is a combination therapy of compounds which
act in part in an additive / synergistic fashion and which includes agentstargeting cell wall synthesis
Banerjee et al. Science 1994, 263: 227 Johansen et al. Mol. Cell 2006, 23: 173Meier et al. Antimicrob. Agents Chemother. 1996, 40:2452 Zaunbrecher et al. Proc. Natl. Acad. Sci. USA 2009, 106: 20004Okamoto et al. Mol. Microbiol. 2007, 63: 1096 Telenti et al. Nat. Med. 1997, 3: 567
Tunis 2010 - 11
1. Drug resistance is exclusively due to chromo-somal mutations and these occur in a stochasticfashion.
2. Drug resistance mutations found in clinicalstrains are a result of randomly occurringmutations and selection.
The Nature of Drug Resistance inMycobacterium tuberculosis
Are different phylogenetic lineages of M.tuberculosis associated with different resistancemutations and if – what are the explanations?

Are Different Phylogenetic Lineages Associated withDifferent Resistance Mutations?
RU2
USA1
Geogr.Area
29(10%)
3(1%)
287(89%)
319(100%)
21(22%)
20(21%)
51(55%)
92(100%)
nomut
mutinhA
mutkatG
Isoniazid resistantisolates (n)
absolute concentration method 1.0 mg/L
proportion method 0.1 mg/L, 0.4 mg/L
Laboratory Drug Susceptibility Testing
Isolates from United States of America: New York State1Somoski et al. J. Clin. Microbiol. 2006, 44: 4459-4463
Isolates from Russian Federation: Central region, Ural region, West Siberian region2Afamas‘ev et al. J. Antimicrob. Chemother. 2007, 59: 1057-1064
15(42%)
6(10%)
18(52%)
2(4%)
2(6%)
49(86%)
35(100%)
57(100%)
proportion testing < 0.4 mg/L
proportion testing > 0.4 mg/L
Tunis 2010 - 12

“We consider that the best type of sensitivity test is a fully quantitativedetermination in which the organisms‘ capability of growth on mediumcontaining a wide range of drug concentrations is known. This type of testwould provide full information on the degree of resistance. However, sincesuch a test requires large amounts of medium and is time-consuming, itcannot be recommended as a routine procedure.“Canetti et al. Bull. WHO 1963, 29: 565-579
≥ 16.08.04.0≤ 2.0Ciprofloxacin
≥ 16.08.04.0≤ 2.0Ofloxacin
≥ 16.08.04.0≤ 2.0Streptomycin
≥ 10.05.02.5≤ 1.25Ethionamide
≥ 16.08.01.0-4.0≤ 0.5Rifampicin
≥ 4.02.00.2-1.0≤ 0.1Isoniazid
≥ 16.08.04.0≤ 2.0Ethambutol
ResistantModeratelyresistant
ModeratelysusceptibleSusceptibleDrug
Heifets, L. Am. Rev. Resp. Dis. 1988, 137: 1217-1222Tunis 2010 - 13

What are the implications of this phenotypic heterogeneity forclinical outcome?Predictive value of laboratory drug susceptibility testing
Mycobacterial Drug Resistance and Susceptibility Testing –Drug Resistance in M. tuberculosis is a Mixed Bag:
significant heterogeneity is present, i.e. low-,moderate- and high-level drug resistance
• Successful treatment outcome despite a resistant phenotype – as defined byroutine drug susceptibility testing – reflects limitations of the procedures usedto determine drug susceptibility
• Low-level drug resistance does not correspond to clinical resistance
• Treatment of high-level drug resistance with standardized therapies will contributeto the build-up of further resistance and facilitate the development of XDRtuberculosis
screen with critical concentration testing
implement semi-quantitative measures of drug susceptibility testingTunis 2010 - 14

Tunis 2010 - 15
Antibiotic Resistance, FitnessCost and Compensatory Mutations
Schrag et al., Nature 1996; 381: 120Björkman et al., Proc. Natl. Acad. Sci. USA 1998; 95: 3949Nagaev et al., Mol. Microbiol. 2001; 40: 433
Drug resistance comes at a biological cost, e.g. reduced growth inthe absence of antibiotics. In-vitro, a resistance mutation associatedwith a fitness burden may be counteracted by secondary site,compensatory mutations ameliorating the fitness cost (frequency10-5 – 10-8).
Compensatory mutations have been suggested to maintain thespread of resistance in the absence of antibiotics.Björkman et al., Science 2000; 287: 1479Björkholm et al., Proc. Natl. Acad. Sci. USA 2001; 98: 14607Besier et al., Antimicrob. Agents Chemother. 2005; 49: 1426
What is the evidence for this scenario to take placein-vivo, e.g. in the infected patient or duringtransmission?

Tunis 2010 - 16
What is the evidence …
• that transmission of resistant strains is dependent onthe type of genetic mutation leading to resistance?
• that compensatory evolution mitigates the fitnessdeficits associated with drug resistance?
• that the impact of a resistance mutation on bacterialfitness is greatly influenced by the strains’ geneticbackground?
Antibiotic Resistance, FitnessCost and Compensatory Mutations

Tunis 2010 - 17
Use in-vitro experimental data on the genetics andcosts associated with a resistance determinant in theinterpretation of resistant clinical isolates in-vivo
• assess frequency of resistance mutations in clinicaldrug resistant isolates
• introduce mutations by genetic engineering into asuitable model system to generate isogenic mutants
• study mutants for drug susceptibility, generationtime and in fitness assays (in-vitro competitiongrowth experiments)
single rRNA allelic M. smegmatis
Experimental Procedure

-0.663216S rRNA 524G C
2%0.901616S rRNA 526C T
3%0.913216S rRNA 522C T
6%0.941616S rRNA 523A C
< 1%0.85> 128RpsL 42Lys Asp
< 1%0.86> 128RpsL 42Lys Thr
88%0.99> 128RpsL 42Lys Arg
-1.01.0wild-type
Frequency in clinicalSmR M. tuberculosis
isolatesFitnessMIC mg / LAlteration
Böttger et al., Nature Med. 1998; 12: 1343, Sander et al., Antimicrob. Agents Chemother. 2002; 46: 1204
Resistance mutations in rpsL aa position 88 and in rrs positions 501, 912 and 913 are not included;these mutations account for approximately 10% of clinical streptomycin resistant isolates in M.tb
Streptomycin Resistance Mutations inMycobacteria and Fitness
Tunis 2010 - 18

Relationship between Frequency of StreptomycinResistance Mutations in Clinical M. tuberculosis Isolates
and Relative Fitness
The vast majority of drug resistance in M. tuberculosis is primary resistance, indicating activetransmission. Thus, resistance mutations in clinical strains reflect the outcome of natural infectionexperiments, which capture the complexity of the life cycle of M. tuberculosis and its epidemiology,including development of drug resistance, competition between different resistance mutations,transmission and infection.
Böttger et al. Nature Med. 1998, 12: 1343, Sander et al. Antimicrob. Agents Chemother. 2002, 46: 1204 Tunis 2010 - 19
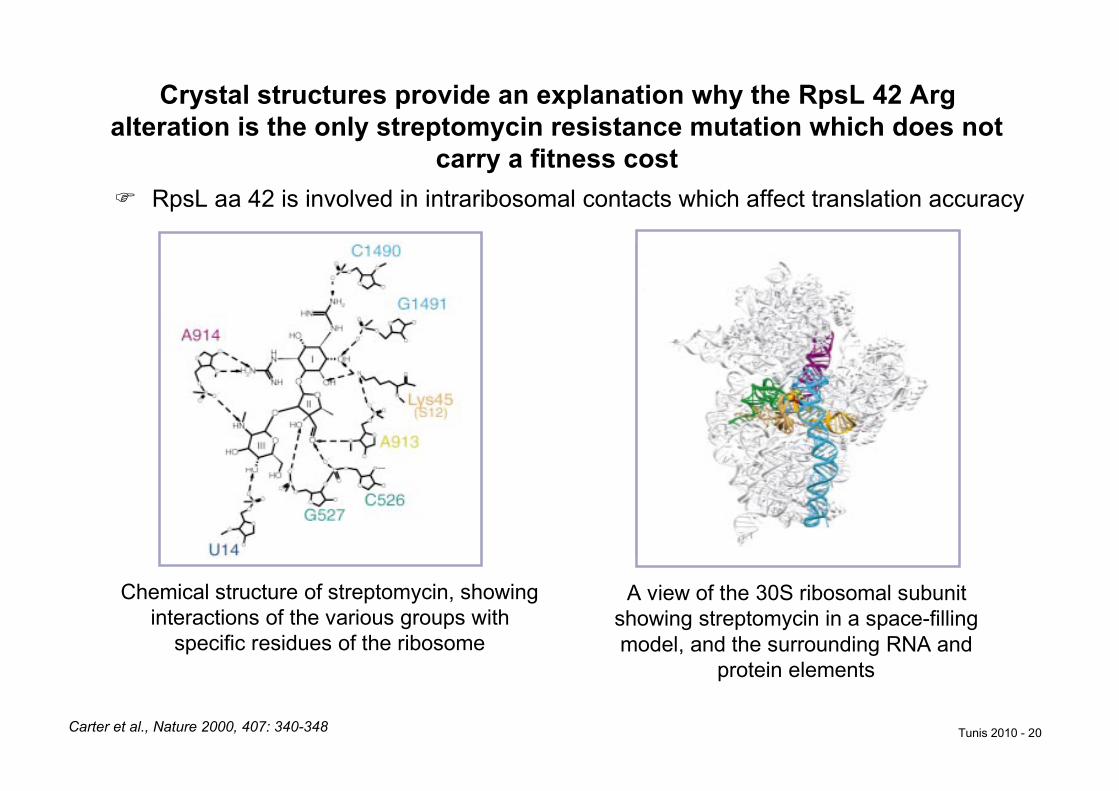
Chemical structure of streptomycin, showinginteractions of the various groups with
specific residues of the ribosome
A view of the 30S ribosomal subunitshowing streptomycin in a space-fillingmodel, and the surrounding RNA and
protein elements
Carter et al., Nature 2000, 407: 340-348
Crystal structures provide an explanation why the RpsL 42 Argalteration is the only streptomycin resistance mutation which does not
carry a fitness cost RpsL aa 42 is involved in intraribosomal contacts which affect translation accuracy
Tunis 2010 - 20
Tunis 2010 - 21
Primary Resistance versusAcquired Resistance
Primary resistance: infection with a resistant strain
Acquired resistance: infection with a drug susceptible strain withresistance developing under therapy
… Primary resistance is not a mere replication of acquired resistance. Other factors, such as altered virulence of the resistant strains, or instability inherent to certain types of resistance, may also be at work in producing the difference.
... If some of the strains with acquired resistance are incapable(through insufficient virulence) of producing new cases of
tuberculosis ... the relative frequency of resistance must necessarily be lower in primary than in acquired resistance.G. Canetti, Am. Rev. Respirat. Dis. 1965, 92: 687

Tunis 2010 - 22
Primary Resistance and AcquiredResistance to Streptomycin
G. Canetti, Am. Rev. Respirat. Dis. 1965, 92: 687
Concentration of Streptomycin(µg/ml)
≥ 4 10 ≥ 100Total of Cases
% % %% # # ##
Primary resistanceAcquired resistance
163426
100100
94267
5863
34102
2124
3557
2113

Tunis 2010 - 23
Primary Resistance and AcquiredResistance to Isoniazid
G. Canetti, Am. Rev. Respirat. Dis. 1965, 92: 687
Concentration of Isoniazid (µg/ml)
≥ 0.2 1 ≥ 10Total of Cases
% % %% # # ##
Primary resistanceAcquired resistance
98443
100100
49114
5026
3895
3921
11234
1153
Tunis 2010 - 24
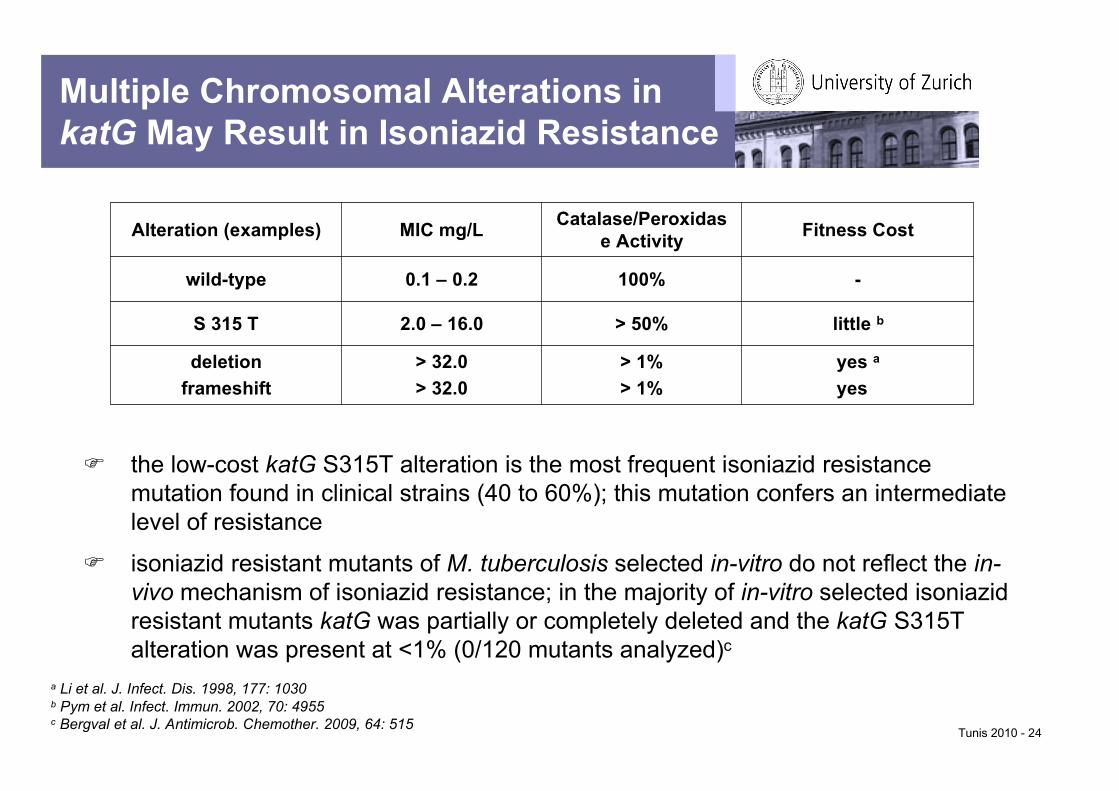
Multiple Chromosomal Alterations inkatG May Result in Isoniazid Resistance
> 32.0> 32.0
2.0 – 16.0
0.1 – 0.2
MIC mg/L
yes ayes a
> 1%> 1%
deletionframeshift
little b> 50%S 315 T
-100%wild-type
Fitness CostCatalase/Peroxidase ActivityAlteration (examples)
the low-cost katG S315T alteration is the most frequent isoniazid resistancemutation found in clinical strains (40 to 60%); this mutation confers an intermediatelevel of resistance
isoniazid resistant mutants of M. tuberculosis selected in-vitro do not reflect the in-vivo mechanism of isoniazid resistance; in the majority of in-vitro selected isoniazidresistant mutants katG was partially or completely deleted and the katG S315Talteration was present at <1% (0/120 mutants analyzed)c
a Li et al. J. Infect. Dis. 1998, 177: 1030b Pym et al. Infect. Immun. 2002, 70: 4955c Bergval et al. J. Antimicrob. Chemother. 2009, 64: 515

The rare presence of high cost resistance mutations in clinical isolates can best be explained by
It is under these circumstances that the scenario of costly resistance mutations ameliorated bycompensatory mutations may take place in-vivo.
i. stochastic probability of a resistance mutation under circumstances of a size limitedbacterial population
ii. bottleneck phenomena
n = 1691-716S rRNA alteration
21491G→U / 1409C→A
11491G→U
61409C→U
1601408A→G
View of the three-dimensional structure of the A-sitecomplexed with 4,5- and 4,6 disubstituted 2-deoxy-streptamines: the common neamine core is denoted inyellow; ring III of the 4,6 compounds is denoted in red;rings II and IV of the 4,5-compounds are denoted in blue.Key nucleotides of the binding site, which have beenaltered by site-directed mutagenesis to probe structuraldrug-target interactions, are given in bold.
1Sander et al. Mol. Microbiol. 1996, 22: 841-8482Alangaden et al. AAC 1998, 42: 1295-12973Suzuki et al. JCM 1998, 36: 1220-12254Krüüner et al. AAC 2003, 47: 2971-29735Maus et al. AAC 2005, 49: 3192-31976Feuerrigel et al. AAC 2009, 53: 3353-33567Jugheli et al. AAC 2009, 53: 5064-5068
Frequency of Resistance Mutations in Aminoglycoside Resistant Clinical M. tuberculosis
16S rRNA A-site
1408
1409 1491
A
GU UC
C G
AA
G C
Tunis 2010 - 25

4,5 Aminoglycosides 4,6 Aminoglycosides
Paramomycin (R = OH)Neomycin (R = NH 3
+)Geneticin (R = OH)Gentamicin (R = NH 3
+)Neamine (R = NH 3
+)
4,5 Aminoglycosides 4,6 Aminoglycosides
Paramomycin (R = OH)Neomycin (R = NH 3
+)Geneticin (R = OH)Gentamicin (R = NH 3
+)Neamine (R = NH 3
+)
4,5-Aminoglycosides
4,5 Aminoglycosides 4,6 Aminoglycosides
Paramomycin (R = OH)Neomycin (R = NH 3
+)Geneticin (R = OH)Gentamicin (R = NH 3
+)Neamine (R = NH 3
+)
4,5 Aminoglycosides 4,6 Aminoglycosides
Paramomycin (R = OH)Neomycin (R = NH 3
+)Geneticin (R = OH)Gentamicin (R = NH 3
+)Neamine (R = NH 3
+)
4,5 Aminoglycosides 4,6 Aminoglycosides
Paramomycin (R = OH)Neomycin (R = NH 3
+)Geneticin (R = OH)Gentamicin (R = NH 3
+)Neamine (R = NH 3
+)
4,5 Aminoglycosides 4,6 Aminoglycosides
Paramomycin (R = OH)Neomycin (R = NH 3
+)Geneticin (R = OH)Gentamicin (R = NH 3
+)Neamine (R = NH 3
+)
4,5 Aminoglycosides 4,6 Aminoglycosides
Paramomycin (R = OH)Neomycin (R = NH 3
+)Geneticin (R = OH)Gentamicin (R = NH 3
+)Neamine (R = NH 3
+)
4,5 Aminoglycosides 4,6 Aminoglycosides
Paramomycin (R = OH)Neomycin (R = NH 3
+)Geneticin (R = OH)Gentamicin (R = NH 3
+)Neamine (R = NH 3
+)
4,6-Aminoglycosides
• bind to the decoding A-site of the small ribosomal subunit(helix 44 in bacterial 16S rRNA)
• affect ribosomal accuracy by interfering with decoding to resultin misreading
• inhibit translocation
2-deoxystreptamines
Aminoglycoside Antibiotics
Tunis 2010 - 26

Tunis 2010 - 27
1.08.0-16.08.0-16.01.5 ± 2.93.1 ± 0.10C1409A/G1491U
0.51.01.04.5 ± 3.13.2 ± 0.06C1409U/G1491A
0.52.04.031.9 ± 1.93.8 ± 0.06C1409G/G1491C
1.0-2.08.0-16.04.0-8.09.3 ± 2.63.3 ± 0.05C1409U
8.016.0-32.02.050.4 ± 1.54.3 ± 0.06C1409G
16.0-32.032.0-64.032.0-64.011.7 ± 5.93.7 ± 0.06G1491U
2.0-4.016.0-32.016.0-32.067.1 ± 5.75.8 ± 0.15G1491C
0.51.0-2.02.0-4.045.5 ± 3.64.9 ± 0.12G1491A
>1024.0>1024.0>1024.05.0 ± 2.83.1 ± 0.06A1408G
0.50.5-1.00.5-1.0-3.0 ± 0.05ΔrrnB (parental)
AmikacinKanamycin AGentamycinCost per generation% ± SD
Generation timeh ± SDStrain
MIC (mg/L)
M. smegmatis strains constructed: generation time measurements, cost pergeneration and drug susceptibility
Results
Shcherbakov et al. Mol. Microbiol. 2010, 77: 830-840
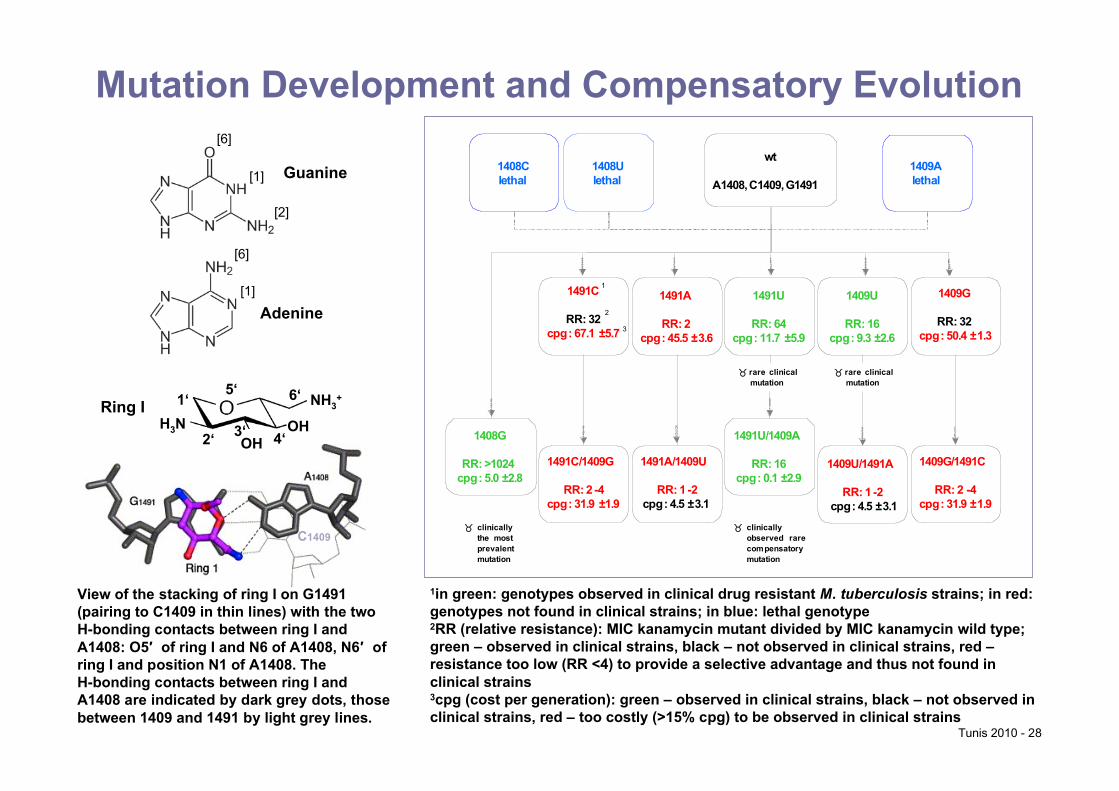
Mutation Development and Compensatory Evolutionwt
A1408, C1409, G1491
1491C
RR: 32cpg: 67.1 ±5.7
1491A
RR: 2cpg: 45.5 ±3.6
1491U
RR: 64cpg: 11.7 ±5.9
1409U
RR: 16cpg: 9.3 ±2.6
1409G
RR: 32cpg: 50.4 ±1.3
1408G
RR: >1024cpg: 5.0 ±2.8
1491C/1409G
RR: 2 -4cpg: 31.9 ±1.9
1491A/1409U
RR: 1 -2cpg: 4.5 ±3.1
1491U/1409A
RR: 16cpg: 0.1 ±2.9
1409G/1491C
RR: 2 -4cpg: 31.9 ±1.9
1409U/1491A
RR: 1 -2cpg: 4.5 ±3.1
1
2
3
1408Ulethal
1408Clethal
1409Alethal
! rare clinicalmutation
! clinicallythe mostprevalentmutation
! clinicallyobserved rarecompensatorymutation
! rare clinicalmutation
1in green: genotypes observed in clinical drug resistant M. tuberculosis strains; in red:genotypes not found in clinical strains; in blue: lethal genotype2RR (relative resistance): MIC kanamycin mutant divided by MIC kanamycin wild type;green – observed in clinical strains, black – not observed in clinical strains, red –resistance too low (RR <4) to provide a selective advantage and thus not found inclinical strains3cpg (cost per generation): green – observed in clinical strains, black – not observed inclinical strains, red – too costly (>15% cpg) to be observed in clinical strains
View of the stacking of ring I on G1491(pairing to C1409 in thin lines) with the twoH-bonding contacts between ring I andA1408: O5′ of ring I and N6 of A1408, N6′ ofring I and position N1 of A1408. TheH-bonding contacts between ring I andA1408 are indicated by dark grey dots, thosebetween 1409 and 1491 by light grey lines.
Guanine
Adenine
[6]
[1]
[2]
[6]
[1]
OHOH
NH3+
H3N1‘
2‘ 3‘ 4‘
5‘ 6‘Ring I
C1409
Tunis 2010 - 28

Tunis 2010 - 29
Drug Resistance, Fitnessand Transmission
Reconstructing the in-vivo evolution of drug resistance inM. tuberculosis – some general conclusions:
The presence of a dominant resistance mutation in clinical isolates(e.g. rpsL K42R, rrs A1408G) versus multiple different resistancemutations (e.g. pncA) presumably reflects different constraints onresistance alterations to maintain gene function.
1. The biological cost of resistance is a characteristic of both the drugtarget and the resistance mechanism involved.
2. The frequency of a resistance mutation in clinical isolates is a result ofits resistance level conferred and its fitness cost associated.
3. A high selection exists in clinical isolates for those resistancemutations which carry the least fitness cost.

Tunis 2010 - 30
Drug Resistance, Fitnessand Transmission
4. The finding of a significant correlation between the frequency of aresistance mutation in genetically heterogeneous clinical isolates andthe fitness cost – as assessed by study of genetically constructedisogenic mutants – argues against the belief that the strain geneticbackground plays a major role in resistance-related fitness cost inM. tuberculosis. Rather, the fitness cost is a dominant characteristicof the specific resistance mutation itself.
Mutations become highly selected during resistance evolution andthus occur in unrelated M. tuberculosis strains from around the world.The observation that common resistance mutations can be found indifferent and unrelated populations reflects convergent evolution.

Tunis 2010 - 31
Drug Resistance, Fitnessand Transmission
Considerations of fitness cost also have to address the periodavailable for transmission; i.e. any fitness deficit associated withresistance might easily be compensated for by longer infectivitydue to improper treatment and consequently extended timeperiods for transmission – explaining the emergence of MDRepidemics in competition with drug susceptible strains.
5. When a costly resistance mutation becomes dominant in a bacterialpopulation, compensatory secondary-site mutations amelioratingresistance-associated fitness cost may evolve and contribute tomutation fixation.

Acknowledgements
Grant Support:European Commission, Bundesamt für Gesundheit,
Swiss National Science Foundation, University of Zurich,Deutsche Forschungsgemeinschaft
D. AnderssonM. Pletschette
D. ScherbakovR. AkbergenovT. MattT. Janusic
B. SpringerP. Sander