drug treatment of parasitic infections jf regal april 24, 2009 medical school duluth
TRANSCRIPT

Drug Treatment of Parasitic Infections
JF RegalApril 24, 2009
Medical School Duluth

Parasites
Protozoal Diseases LecturesMalaria ICMIntestinal Protozoal diseases GITropical and Sub-tropical Protozoa ICM
Helminth InfectionNematodes
Intestinal Roundworms GITissue Roundworms ICM
Trematodes or Flukes GICestodes or Tapeworms GI

Objectives Know drug names and general
category of organisms that the drug is used for i.e. protozoa, roundworm, cestode (tapeworms), trematode (flukes) etc.
Don't memorize the specific drug of first choice for each infecting organism.
Understand the mechanism of action and the basis for selective toxicity for each of the anti-parasitic drugs.
Know major toxicities and relevant aspects of drug distribution.

Drug Names
In bold throughout the handout The drug list on p. 2 of the word
handout will be covered on the ICM exam
Summary tables on p. 3 (protozoa) and p. 9 (worms) of the handout

ProtozoaSingle cells
HelminthMulticellular
Parasites

Summary of Protozoal Disease Treatment
Metronidazole Tinidazole
Reduction of drug liberates toxic intermediates which damage DNA
Species difference in redox system
Iodoquinol Unknown Selective distribution; loss of visual acuity
Nitazoxanide Interferes with pyruvate:ferredoxin oridoreductase enzyme dependent electron transfer; essential for anaerobic metabolism
Species difference in electron transfer
Paromomycin Aminoglycoside mechanism Selective distribution Species difference in ribosomes
Tetracycline Tetracycline mechanism Selective distribution Species difference in ribosomes
Trimethoprim-sulfamethoxazole
Folate inhibitor Species difference in enzymes
Intestinal protozoa
Entamoeba histolytica Giardia lamblia Cryptosporidium parvum Balantidium coli Isospora belli
Pyrimethamine- Sulfadiazine
Folate inhibitor Species difference in enzymes
Other protozoa
Babesia spp Toxoplasma gondii Trichomonas vaginalis Pneumocystis jiroveci
Various Antibacterial drugs
Mechanism Selectivity

Arsenicals (melarsoprol)
Bind to –SH, principally trypanothione, a substitute for glutathione in trypanosomes
Selective accumulation
Liposomal amphotericin B
Ergosterol binding with pore formation
Species difference in sterols
Nifurtimox Generates reactive oxygen species which cause damage
Unknown
Miltefosine Unknown; maybe protein kinase C inhibitor or phosphatidylcholine synthesis inhibitor
Unknown
Organic antimonials (Sodium stibogluconate, Meglumine antimonate)
Interferes with glycolysis and fatty acid beta-oxidation; interfere with trypanothione redox system
Unknown
Pentamidine Hypothesized to interfere with kinetoplast DNA replication as a type II topoisomerase inhibitor
Species difference in enzymes
Tissue Protozoa (Tropical and sub-tropical protozoa)
Leishmania Trypanosoma brucei gambiense or rhodesiense Trypanosoma cruzi
Suramin Unknown Selective accumulation
Summary cont.

Chemotherapy of Protozoal Infections
Protozoal Diseases Protozoans are unicellular organisms with a nucleus and cytoplasm.
Two major protozoal diseases are:Plasmodium – malariaEntamoeba – amebiasis

Infecting organism Drug of Choice Alternative
Entamoeba histolytica Asymptomatic cyst passer Iodoquinol or
paromomycin Diloxanide
Intestinal disease Metronidazole followed by Paromomycin or Iodoquinol
Tinidazole
Hepatic abscess Metronidazole followed by Paromomycin
Balantidium coli Tetracycline Metronidazole
Cryptosporidium parvum Nitazoxanide
Dientamoeba fragilis Iodoquinol Tetracycline
Giardia lamblia Tinidazole or Nitazoxanide Metronidazole
Isospora sp. (coccidiosis) Trimethoprim-
Sulfamethoxazole
Pneumocystis jiroveci Trimethoprim- Sulfamethoxazole
Toxoplasma gondii Pyrimethamine plus Sulfadiazine
Trichomonas vaginalis Metronidazole
Luminal amebicide
Tissue amebicide

Entamoeba histolytica
Asymptomatic cyst passerTreated only with a luminal
amebicide• Iodoquinol or paromomycin
Intestinal disease and hepatic abscessTreated with tissue amebicide
followed by a luminal amebicide•Metronidazole (tissue)• Iodoquinol or paromomycin (lumen)
Iodoquinol
Unknown mechanism Selective distribution – only 10% of
the drug is absorbed so it works locally on the protozoa in the GI tract
Effective only against intestinal form of the disease i.e. luminal amebicide
Most serious side effect is loss of visual acuity and even blindness at higher doses.

Paromomycin
Aminoglycoside Minimal absorption after oral
administration Luminal amebicide that is not
effective against extraintestinal forms
GI upset and diarrhea High potential for ototoxicity and
nephrotoxicity if given parenterally

Infecting organism Drug of Choice Alternative
Entamoeba histolytica Asymptomatic cyst passer Iodoquinol or
paromomycin Diloxanide
Intestinal disease Metronidazole followed by Paromomycin or Iodoquinol
Tinidazole
Hepatic abscess Metronidazole followed by Paromomycin
Balantidium coli Tetracycline Metronidazole
Cryptosporidium parvum Nitazoxanide
Dientamoeba fragilis Iodoquinol Tetracycline
Giardia lamblia Tinidazole or Nitazoxanide Metronidazole
Isospora sp. (coccidiosis) Trimethoprim-
Sulfamethoxazole
Pneumocystis jiroveci Trimethoprim- Sulfamethoxazole
Toxoplasma gondii Pyrimethamine plus Sulfadiazine
Trichomonas vaginalis Metronidazole
Luminal amebicide
Tissue amebicide

Metronidazole
Mechanism Tissue amebicide Not adequate as a luminal
(intestinal) amebicide because it does not always achieve adequate concentrations in the intestine
Should not be used alone in asymptomatic cyst passer

Metronidazole
Headache, nausea, dry mouth and a metallic taste; potentially neurotoxic
Disulfiram reaction possibleAbdominal distress, vomiting,
flushing or headache with consumption of alcohol

Tinidazole
Mechanism and adverse effects are similar to metronidazole
Treatment course with tinidazole is shorter in general than with metronidazole
May be better tolerated than metronidazole
More expensive than metronidazole May be effective in patients with
metronidazole-resistant trichomoniasis

Tetracycline
Incompletely absorbed Not for use in children or during
pregnancy Alters intestinal flora that is
essential for proliferation of the amoeba

Infecting organism Drug of Choice Alternative
Entamoeba histolytica Asymptomatic cyst passer Iodoquinol or
paromomycin Diloxanide
Intestinal disease Metronidazole followed by Paromomycin or Iodoquinol
Tinidazole
Hepatic abscess Metronidazole followed by Paromomycin
Balantidium coli Tetracycline Metronidazole
Cryptosporidium parvum Nitazoxanide
Dientamoeba fragilis Iodoquinol Tetracycline
Giardia lamblia Tinidazole or Nitazoxanide Metronidazole
Isospora sp. (coccidiosis) Trimethoprim-
Sulfamethoxazole
Pneumocystis jiroveci Trimethoprim- Sulfamethoxazole
Toxoplasma gondii Pyrimethamine plus Sulfadiazine
Trichomonas vaginalis Metronidazole
Used in Immunocompromised No treatment in healthy individuals

Nitazoxanide
Recently approved for use in children for Giardia and Cryptosporidium
Interferes with pyruvate:ferredoxin oxidoreductase enzyme dependent electron transfer; essential for anaerobic metabolism
DNA damaging radicals are not formed; free of potential mutagenic effects

Infecting organism Drug of Choice Alternative
Entamoeba histolytica Asymptomatic cyst passer Iodoquinol or
paromomycin Diloxanide
Intestinal disease Metronidazole followed by Paromomycin or Iodoquinol
Tinidazole
Hepatic abscess Metronidazole followed by Paromomycin
Balantidium coli Tetracycline Metronidazole
Cryptosporidium parvum Nitazoxanide
Dientamoeba fragilis Iodoquinol Tetracycline
Giardia lamblia Tinidazole or Nitazoxanide Metronidazole
Isospora sp. (coccidiosis) Trimethoprim-
Sulfamethoxazole
Pneumocystis jiroveci Trimethoprim- Sulfamethoxazole
Toxoplasma gondii Pyrimethamine plus Sulfadiazine
Trichomonas vaginalis Metronidazole

Pyrimethamine orTrimethoprim
Sulfadiazine orSulfamethoxazole
Probably act on both the protozoa and the intestinal flora

Arsenicals (melarsoprol)
Bind to –SH, principally trypanothione, a substitute for glutathione in trypanosomes
Selective accumulation
Nifurtimox Generates reactive oxygen species which cause damage
Unknown
Miltefosine Unknown; maybe protein kinase C inhibitor or phosphatidylcholine synthesis inhibitor
Unknown
Organic antimonials (Sodium stibogluconate, Meglumine antimonate)
Interferes with glycolysis and fatty acid beta-oxidation; interfere with trypanothione redox system
Unknown
Pentamidine Hypothesized to interfere with kinetoplast DNA replication as a type II topoisomerase inhibitor
Species difference in enzymes
Tissue Protozoa (Tropical and sub-tropical protozoa)
Leishmania Trypanosoma brucei gambiense or rhodesiense Trypanosoma cruzi
Suramin Unknown Selective accumulation
Tropical and Sub-tropical Protozoa

Tropical and Sub-tropical Protozoa
Tissue protozoa – serious diseases Leishmaniasis – Sandfly bite transmits parasite into
bloodstream where it infects macrophages at various sites. Cutaneous Mucocutaneous Diffuse cutaneous Visceral
Trypanosomes – Transmitted by the bite of the assassin bug or tsetse fly, depositing the organism into the eye or the bloodstream. African sleeping sickness -T brucei moves from
bloodstream and lymph nodes into CNS Chagas disease, South American, Serious
cardiomyopathy -T. cruzi
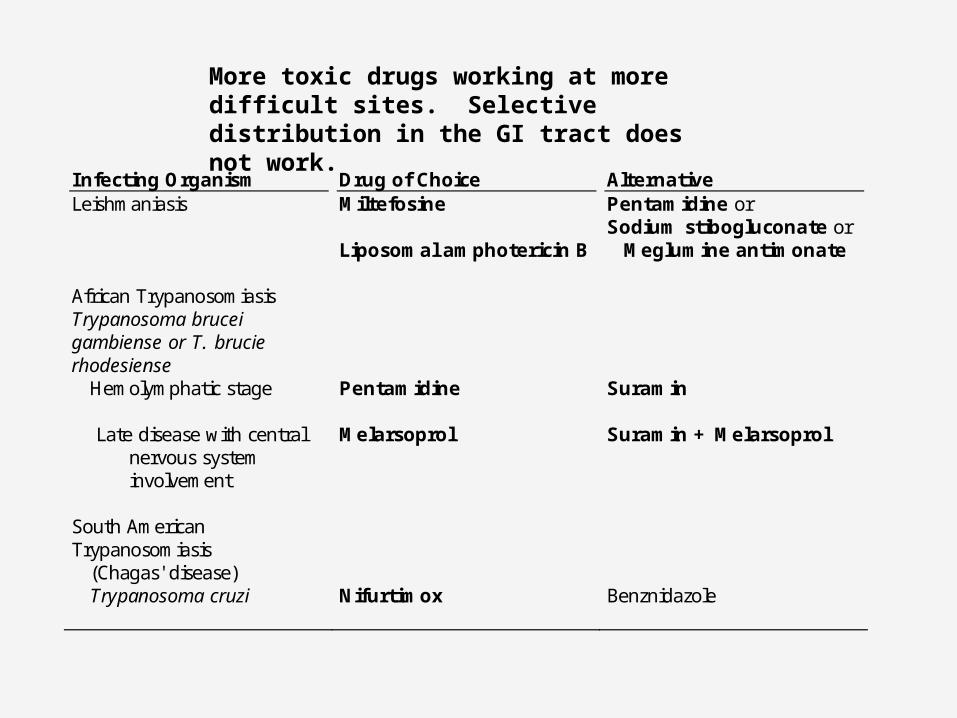
Infecting Organism Drug of Choice Alternative Leishmaniasis Miltefosine
Liposomal amphotericin B
Pentamidine or Sodium stibogluconate or
Meglumine antimonate African Trypanosomiasis Trypanosoma brucei gambiense or T. brucie rhodesiense
Hemolymphatic stage Pentamidine Suramin Late disease with central
nervous system involvement
Melarsoprol
Suramin + Melarsoprol
South American Trypanosomiasis (Chagas' disease) Trypanosoma cruzi Nifurtimox Benznidazole
More toxic drugs working at more difficult sites. Selective distribution in the GI tract does not work.

Organic antimonialsLeishmania and macrophages
Sodium stibogluconateMeglumine antimonate
• Interferes with glycolysis and fatty acid beta-oxidation in leishmania with a net reduction in the generation of ATP and GTP
• More recent studies suggest that the drug interferes with the trypanothione (like glutathione) redox system
• Incidence of treatment failures is increasing and resistance occurs
• Fairly well tolerated initially, but toxicity increases over time
• Adverse effects can include coughing, vomiting, myalgia, arthralgia, EKG changes

Liposomal Amphotericin B
Only for visceral leishmaniasis Drug of choice for antimonial
resistant organisms Only liposomal formulation shown
to be effective Antifungal drug that binds to
ergosterol to form pores in membranes
Nephrotoxicity and infusion toxicity

Miltefosine
Unknown mechanism; maybe inhibition of protein kinase C or phosphatidylcholine synthesis
Vomiting and diarrhea in up to 60% of patients
Promising treatment for leishmaniasis especially where resistance to antimonials is a problem (India)

Infecting Organism Drug of Choice Alternative Leishmaniasis Miltefosine
Liposomal amphotericin B
Pentamidine or Sodium stibogluconate or
Meglumine antimonate African Trypanosomiasis Trypanosoma brucei gambiense or T. brucie rhodesiense
Hemolymphatic stage Pentamidine Suramin Late disease with central
nervous system involvement
Melarsoprol
Suramin + Melarsoprol
South American Trypanosomiasis (Chagas' disease) Trypanosoma cruzi Nifurtimox Benznidazole
More toxic drugs working at more difficult sites. Selective distribution in the GI tract does not work.

PentamidineT. brucei, extracellular
Used in early trypanosomiasis before CNS involvement
Does not penetrate the CNS Mechanism of action is thought to be
interference with kinetoplast DNA replication as a type II topoisomerase inhibitor. A kinetoplast is a specialized structure in the trypanosome which is part of the mitochondrial system
Resistance can occur from altered drug uptake Can be quite toxic - Hypotension,
tachycardia, vomiting, hypoglycemia

Suramin Unknown mechanism Does not penetrate the CNS appreciably Selectively accumulates in trypanosome
vs host Quite toxic
nausea, vomiting, shock, loss of consciousness
peripheral neuropathyphotophobiaurticariapruritisnephrotoxicity

Arsenicals - Melarsoprol First line drug used for sleeping sickness which
has progressed to CNS involvement. Penetrates into CNS Mechanism of action probably involves
sulfhydryl binding. The principal target is believed to be trypanothione, a substitute for glutathione in trypanosomes. Trypanothione maintains a reducing environment intracellularly and this is upset in the presence of melarsoprol.
Very toxic - Encephalopathy, Fever, Hypertension, Vomiting, Albuminuria
Resistance can occur from altered drug uptake.

NifurtimoxT. cruzi, Chagas disease
Mainly for Trypanosome cruzi which multiplies within cells
Mechanism thought to be similar to nitrofurantoin; formation of reactive oxygen species resulting in cellular damage
Most effective in acute stages and ineffective in chronic stages of the infection.
Side effects are common; nausea, vomiting, myalgia, weakness, peripheral neuropathy

Summary of Protozoal Disease Treatment
Metronidazole Tinidazole
Reduction of drug liberates toxic intermediates which damage DNA
Species difference in redox system
Iodoquinol Unknown Selective distribution; loss of visual acuity
Nitazoxanide Interferes with pyruvate:ferredoxin oridoreductase enzyme dependent electron transfer; essential for anaerobic metabolism
Species difference in electron transfer
Paromomycin Aminoglycoside mechanism Selective distribution Species difference in ribosomes
Tetracycline Tetracycline mechanism Selective distribution Species difference in ribosomes
Trimethoprim-sulfamethoxazole
Folate inhibitor Species difference in enzymes
Intestinal protozoa
Entamoeba histolytica Giardia lamblia Cryptosporidium parvum Balantidium coli Isospora belli
Pyrimethamine- Sulfadiazine
Folate inhibitor Species difference in enzymes
Other protozoa
Babesia spp Toxoplasma gondii Trichomonas vaginalis Pneumocystis jiroveci
Various Antibacterial drugs
Mechanism Selectivity

Arsenicals (melarsoprol)
Bind to –SH, principally trypanothione, a substitute for glutathione in trypanosomes
Selective accumulation
Liposomal amphotericin B
Ergosterol binding with pore formation
Species difference in sterols
Nifurtimox Generates reactive oxygen species which cause damage
Unknown
Miltefosine Unknown; maybe protein kinase C inhibitor or phosphatidylcholine synthesis inhibitor
Unknown
Organic antimonials (Sodium stibogluconate, Meglumine antimonate)
Interferes with glycolysis and fatty acid beta-oxidation; interfere with trypanothione redox system
Unknown
Pentamidine Hypothesized to interfere with kinetoplast DNA replication as a type II topoisomerase inhibitor
Species difference in enzymes
Tissue Protozoa (Tropical and sub-tropical protozoa)
Leishmania Trypanosoma brucei gambiense or rhodesiense Trypanosoma cruzi
Suramin Unknown Selective accumulation
Summary cont.

ProtozoaSingle cells
HelminthMulticellular
Parasites

Chemotherapy of Helminth Infections
Phylum NemathelminthesNematodes or roundworms
Ascaris, whipworm, pinworm, hookworm, trichinosis
Phylum PlatyhelminthesCestodes or tapeworms Trematodes including flukes (schistosomes)
Helminth Infections
Multicellular organisms with crude organ systems
Pathogenic forms of most of the worm infections amenable to chemotherapy are the adult, non-growing stages of the parasites life cycle.
Growth inhibitors are not particularly useful.

Two effective targets
Mechanisms essential for motor activity
Reactions that generate metabolic energy

Strategies for selective toxicity
Exploiting the biochemical differences between the parasite and host
Differential distribution of the drug.The parasite is exposed to high
concentrations of the drug in its intestinal habitat by the use of orally administered non-absorbable drugs.

HELMINTHIC DISEASES AND TREATMENT Albendazole Mebendazole
Inhibits tubulin polymerization and microtubule formation
Species difference in tubulin Selective distribution
Ivermectin Paralysis by potentiating GABA-mediated signal transmission or by activating glutamate-gated chloride channels
Unknown
Intestinal Nematodes
(Roundworms)
Ascaris spp (roundworm) Trichuris spp (whipworm) Enterobius
vermicularis (pinworm)
Ancylostoma duodenale (hookworm)
Necator americanus (hookworm)
Strongyloides stercoralis
Pyrantel pamoate Binds to the nicotinic receptor and causes spastic paralysis of the worm
Species differences in receptors; selective distribution
Diethylcarbamazine Immobilizes microfilaria
Unknown Tissue
Nematodes (Roundworms)
Wuchereria bancrofti Brugia malayi Loa loa Onchocerca volvulus
Ivermectin Paralysis as above
Unknown
Helminthic Disease Treatment
GI

HELMINTHIC DISEASES AND TREATMENT Trematodes (flukes)
Schistosoma spp Clonorchis sinensis Fasciola hepatica Fasciolopsis buski Heterophyes heterophyes Metagonimus yokogawai Opisthorchis viverrini Paragonimus westermani
Praziquantal Contracts and dislocates worm by increasing calcium permeability; tegumental damage
Species difference in receptors
Albendazole Inhibits tubulin polymerization
and microtubule formation
Species difference in tubulin
Cestodes (tapeworms)
Diphyllobothrium latum Echinococcus granulosis Taenia spp
Praziquantal Contracts and dislocates worm by increasing permeability to calcium; tegumental damage
Species difference in receptors
GI
Helminthic Disease Treatment

Infecting Organism Drug of Choice
Intestinal roundworms
Ascaris lumbricoides Mebendazole or Enterobius vermicularis (pinworm) Pyrantel Pamoate or Ancylostoma duodenale (hookworm) Albendazole Necator americanus (hookworm) Strongyloides stercoralis Ivermectin or Albendazole Trichuris trichiura (whipworm) Albendazole or Mebendazole Tissue roundworms Wuchereria bancrofti Diethylcarbamazine or Ivermectin Brugia malayi Diethylcarbamazine or Ivermectin Loa loa Diethylcarbamazine or Ivermectin Onchocerca volvulus Ivermectin (not diethylcarbamazine)
Nematode or Roundworm Infections

Pyrantel Pamoate
Depolarizing neuromuscular blocker - binds to the nicotinic receptor causing depolarization and spastic paralysis of the worm. Paralyzed worms are then expelled from the intestine.
Also inhibits cholinesterase Poorly absorbed (selective
distribution) Causes nausea, vomiting, diarrhea

Mebendazole, Albendazole
Binds to parasite tubulin and inhibits assembly of tubulin dimers into tubulin polymers. This causes a lack of formation of microtubules which are important in larval development, transport of carbohydrates (glucose uptake) and enzyme function.
Good for treatment of multiple worm infections
Resistance involves mutations in parasite tubulin

Mebendazole, Albendazole
Mebendazole interacts with mammalian tubulin but is more selective for the parasite tubulin. Mebendazole is embryotoxic
Differences in absorption, spectrum of activity and kinetics
•Less absorption of mebendazole than albendazole
•Albendazole is variably absorbed

Infecting Organism Drug of Choice
Intestinal roundworms
Ascaris lumbricoides Mebendazole or Enterobius vermicularis (pinworm) Pyrantel Pamoate or Ancylostoma duodenale (hookworm) Albendazole Necator americanus (hookworm) Strongyloides stercoralis Ivermectin or Albendazole Trichuris trichiura (whipworm) Albendazole or Mebendazole Tissue roundworms Wuchereria bancrofti Diethylcarbamazine or Ivermectin Brugia malayi Diethylcarbamazine or Ivermectin Loa loa Diethylcarbamazine or Ivermectin Onchocerca volvulus Ivermectin (not diethylcarbamazine)
Nematode or Roundworm Infections

Tissue Roundworms
Filariasis – caused by nematodes that inhabit the bloodstream or lymphatics and subcutaneous tissues as adults and microfilaria.
Adverse effects of the drugs may be due in part to the host response to destruction of microfilaria.

Ivermectin Produces a paralysis of the peripheral
musculature of the parasite, possibly by potentiating GABA-mediated signal transmission or by activating glutamate-gated chloride channels.
Well tolerated Transient side effects include itching,
swollen lymph glands and rarely dizziness and postural hypotension
Adverse effects may be due in part to the host response to destruction of microfilaria.

Diethylcarbamazine Immobilizes the microfilaria by an
unknown mechanism Headache, malaise, weakness,
nausea, vomiting Adverse effects may be due in part to
the host response to destruction of microfilaria.
Use in River Blindness (Onchocerca volvulus) increases risk of ocular side effects, including blindness, associated with rapid killing of the worms

HELMINTHIC DISEASES AND TREATMENT Trematodes (flukes)
Schistosoma spp Clonorchis sinensis Fasciola hepatica Fasciolopsis buski Heterophyes heterophyes Metagonimus yokogawai Opisthorchis viverrini Paragonimus westermani
Praziquantal Contracts and dislocates worm by increasing calcium permeability; tegumental damage
Species difference in receptors
Albendazole Inhibits tubulin polymerization
and microtubule formation
Species difference in tubulin
Cestodes (tapeworms)
Diphyllobothrium latum Echinococcus granulosis Taenia spp
Praziquantal Contracts and dislocates worm by increasing permeability to calcium; tegumental damage
Species difference in receptors
Flukes and Tapeworms

Infecting organism Drug of Choice Flukes (Trematodes) Schistosoma haematobium Praziquantel Schistosoma japonicum Praziquantel Schistosoma mansoni Praziquantel Schistosoma mekongi Praziquantel Clonorchis sinensis (Chinese liver fluke) Praziquantel Fasciola hepatica (Sheep liver fluke) Triclabendazole Fasciolopsis buski (intestinal fluke) Praziquantel Heterophyes heterophyes (intestinal fluke) Praziquantel Metagonimus yokogawai (intestinal fluke) Praziquantel Opisthorchis viverrini (liver fluke) Praziquantel Paragonimus westermani (lung fluke) Praziquantel Tapeworms (Cestodes) Diphyllobothrium latum (fish tapeworm) Praziquantel Taenia saginata (beef tapeworm) Praziquantel Taenia solium (pork tapeworm) Praziquantel Hymenolepis nana (dwarf tapeworm) Praziquantel Echinococcus granulosus (hydatid cyst) Albendazole

Praziquantal
Mechanism of action involves an increased permeability of the parasite to divalent cations, particularly calciumRapid contraction of the worm's
musculature occurs and dislocates the organism
Influx of calcium across the tegument causes tegumental damage
Sedation, abdominal discomfort, fever, sweating, nausea, eosinophilia

HELMINTHIC DISEASES AND TREATMENT Trematodes (flukes)
Schistosoma spp Clonorchis sinensis Fasciola hepatica Fasciolopsis buski Heterophyes heterophyes Metagonimus yokogawai Opisthorchis viverrini Paragonimus westermani
Praziquantal Contracts and dislocates worm by increasing calcium permeability; tegumental damage
Species difference in receptors
Albendazole Inhibits tubulin polymerization
and microtubule formation
Species difference in tubulin
Cestodes (tapeworms)
Diphyllobothrium latum Echinococcus granulosis Taenia spp
Praziquantal Contracts and dislocates worm by increasing permeability to calcium; tegumental damage
Species difference in receptors

Chemotherapy of Infection
Principles CoursePrinciples of Chemotherapy Inhibitors of Cell Wall SynthesisInhibitors of Protein and Nucleic Acid Synthesis
Respiratory Course Review of antibacterials Antifungals, antiviralsDrugs used in tuberculosis
Fluids and ElectrolytesUrinary tract infections and review of antibacterials
ICMAntiparasitic drugs including malaria

Board Study for Chemotherapy
Combine the antibacterial, antifungal, antiviral and antiparasitic drugs and make sure you can put each name in a drug class Mechanism Differences amongst drugs in a class Major toxicities Major issues of distribution and elimination
Try to put the bugs and drugs together when it makes sense Example: Ineffectiveness of aminoglycosides
against anaerobes; What are the anaerobes? Penicillinase producing Staph; What drug would
you use?