drug use in chronic liver disease dr ian coombes university of queensland safe medication practice...
TRANSCRIPT

Drug Use in Chronic Liver
DiseaseDr Ian Coombes
University of Queensland
Safe Medication Practice Medication Unit

Objectives
After this session you will be able to: Describe the relationship between chronic liver
disease and the development of a number of complications.
Discuss the strategies commonly used to manage these complications
Describe the influence of liver disease on the pharmacokinetics of drugs

Chronic liver disease (CLD)
Inflammation of the liver for > than 6 months
Have permanent structural changes in the liver
Eventually leads to reduced liver function

Blood supply
Liver receives 25% of resting cardiac output
Blood enters via hepatic artery (25%) & portal
vein (75%) carries blood from gut rich in absorbed nutrients portal flow increases after
meals Blood leaves via
hepatic vein Also leaving liver
hepatic ducts carry bile to gall bladder

Protein NH3
Bacteria
Systemic Circulation
Collateral
Splanchnic Circulation
UreaNormal Situation
GIT

Causes Of Chronic Hepatic Failure
Viral Hepatitis Hepatitis C Hepatitis B / D
Alcohol Autoimmune Disease
Primary Biliary Cirrhosis (PBC) Primary Sclerosing Cholangitis (PSC) Autoimmune Hepatitis
RISK FACTORS
• IVDU
• TATTOOS
• BODY PIERCING
• BLOOD TRANSFUSION (pre 1989/90)
RISK FACTORS
• IVDU
• MOTHER TO BABY (Vertical) - ASIA
• SEXUAL

Hereditary Metabolic Disorders Haemochromatosis - Iron overload Wilson’s Disease - Copper accumulation Alpha - 1 - antitrypsin deficiency
Fatty Liver Venous Outflow Obstruction (Budd-chiari
Syndrome) Drugs
eg methyldopa, isoniazid, nitrofurantoin, methotrexate, amiodarone
Cryptogenic

Major complications of liver disease Portal hypertension Ascites Bleeding Encephalopathy Hepato-renal syndrome Effects on drug handling and
sensitivity

Complications of ALD –Portal hypertension
Increased resistance to flow through the portal system blood forced down alternate channels
Collateral circulation Portosystemic shunting

Consequences of portal hypertension
Ascites Hepatic encephalopathy Increased risk of spontaneous
bacterial peritonitis Increased risk of hepatorenal
syndrome Splenomegaly-mild
panyctopenia Portacaval anastomoses
(oesophageal varices, haemorrhoids, caput medusae)

Complications of CLD – Ascites
Caused by: ↓ albumin Portal hypertension ↓ renal perfusion Na/water retention ↑ aldosterone
Treatment: Diuretics (spironolactone/frusemide) Ascitic taps shunts

Starling’s Forces – control of fluid movement in CV system
Arteriolar Level Capillary Bed Venule
Albumin
O2 + Nutrients
CO2
Movement of fluid controlled by hydrostatic pressue (BP) and Oncotic pressure (OP - generated by albumin).When albumin decreases (due to liver disease– fluid remains in tissue bed – ascites (as driven by portal hypertension).
BP>OP OP>BP

Complications of CLD – Bleeding
Caused by: Portal hypertension
Oesophageal / Gastric / Rectal varices Variceal bleeding mortality after 1st bleed 50% 60% re-bleed in 1 year
Decreased clotting factors Liver site of clotting factor production Increased prothrombin time/INR
Infection can exacerbate bleeding Endotoxin mediated

Complications of CLD- Hepatic encephalopathyMay be precipitated by:
GI bleeding, constipation, high dietary protein load Electrolyte disturbances Infection Drugs Renal impairment
Pathogenesis incompletely understood Ammonia
Treatment: Lactulose/neomycin Avoiding sedating agents
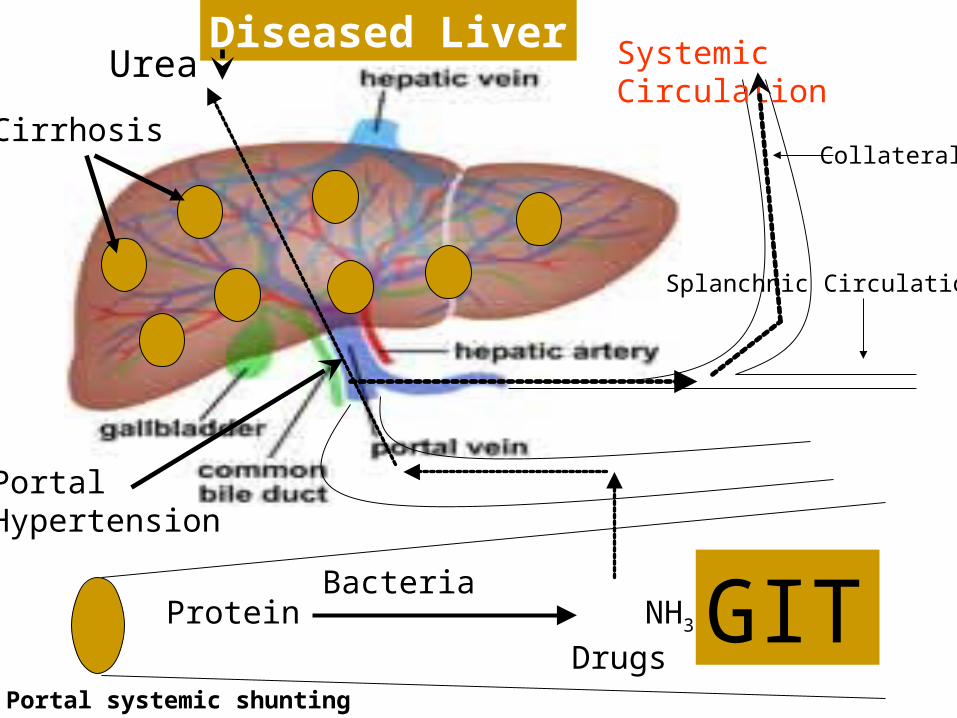
Protein NH3
Bacteria
Systemic Circulation
Collateral
Splanchnic Circulation
Urea Diseased Liver
Cirrhosis
PortalHypertension
DrugsPortal systemic shunting
GIT

Complications of CLD- Hepatorenal syndrome Acute oliguric RF with portal HT & ascites Intense vasoconstriction occurs in otherwise
normal kidneysCaused by: Pathogenesis unknown
Related to altered renocortical blood flow
Treatment: Avoid precipitating drugs & treatments No effective treatment – poor prognosis
terlipressin

Investigation of CLD
Signs and symptoms, history Liver enzymes Plasma protein, coagulation factors, auto
antibodies Imaging – ultrasound, cholangiography
(endoscopic, percutaneous, MR) Liver biopsy

Classification of CLD
Child-Pugh classification (modified version). Point score correlates with survival.
Parameter Number of Points
1 2 3
Bilirubin (umol/L) <34 34-51 >51
Albumin (g/L) >35 28-35 <28
Prothrombin time <3 3-10 >10
Ascites None Slight Moderate to severe
Encephalopathy None Mild Moderate to severe

What the points mean!
Class Total points 1 yr mortality
A 5 – 6 low
B 7 – 9 20 – 40%
C 10 – 15 40 – 60%

Management of CLD
Treatment of underlying cause if possible Adequate nutrition Prevention and symptomatic treatment of
complications Liver transplantation

Drug Use in Chronic Liver Disease Disease severity Pharmacokinetic response
absorption distribution elimination
hepatic clearance
Pharmacodynamic response Potentially hepatotoxic drugs

Consider…
Is it hepatically cleared? First pass?
What are the side effects? Constipation CNS side effects Renal toxicity
Is it hepatotoxic? Idiosyncratic or dose related?

PHARMACOKINETIC CONSIDERATIONS IN LIVER DISEASE
Five variable will affect the pharmacokinetics of a drug in liver disease.
HEPATIC BLOOD FLOW REDUCTION IN HEPATIC CELL MASS PORTAL – SYSTEMIC SHUNTING CHOLESTASIS DECREASE IN PROTEIN BINDING

1. HEPATIC BLOOD FLOW
Reduction occurs in: cardiac failure cirrhosis hepatic venous outflow obstruction portal vein thrombosis Large decrease in blood pressure e.g. shock
HIGH RISK DRUGS >60% first pass clearance

High Extraction Limited Extraction Low Extraction
ChlormethiazolePropranololLignocaineVerapamilGTN
ParacetamolDiazepam *Chlordiazepoxide*Theophylline
Oxazepam *Lorazepam *Frusemide *Spironolactone*DigoxinValproic AcidTolbutamideCimetidine
Hepatic Extraction of drugs

2. REDUCED HEPATIC CELL MASS
Associated with both acute and chronic liver disease:
Decrease first pass metabolism of drugswith a high hepatic extraction – increase in bioavailability
Decrease elimination of drugs with a low hepatic extraction i.e. capacity limited drugs – lead to increase in half-life.

3. PORTAL SYSTEMIC SHUNTING
80% blood entering liver – portal vein, Bioavailability of drugs with high extraction can
increase significantly, Peak plasma concentrations will be increased, Half-life will be prolonged, Elimination delayed – may lead to toxicity

4. CHOLESTASIS
Failure of passage of bile salts to duodenum. Directly affects hepatocellular function – drug clearance.
Lack of bile - reduces absorption of lipid soluble drugs
Reduced plasma protein binding of drugs – competition with bile salts.

5. REDUCTION IN PROTEIN BINDING
Majority of plasma proteins (PP) synthesised by liver, Reduction in PP – decrease binding potential – increase in
free drug concentrations e.g. phenytoin If drug highly extracted – no increase in plasma conc – but
for other drugs will result in increase in free drug plasma concs.
Competition may also occur for binding sites e.g. bile salts.

Case 1 48 year old 86 kg man PC – massive abdominal distension and pain HPC - abdominal distension, pain and lethargy,
confusion PMH includes
Alcoholic liver disease/haemochromatosis Social history
Lives alone Alcohol abuse
Allergies - NKA

Case 1 continued On examination
HR: 84 reg BP: 115/70 mmHg RR: 18/min Temp: 37.7C Ascites+++, abdominal pain Mild confusion
Medications Omeprazole 20mg bd Lactulose 20mL tds prn Thiamine 100mg daily Vitamin K 10mg daily Spironolactone 100mg daily

Laboratory Tests
U&Es Sodium 130 mmol/L Potassium 3.9 mmol/L Creatinine 130 micromol/L Glucose 4.3 mmol/L
Haemotology Hb 100 g/L WCC 16.7 x 109/L Platelets 256 x 109/L INR 1.9

Laboratory Tests LFT/Gastro
Total Protein 61 g/L Albumin 23 g/L Bilirubin 86 umol/L ALT 63 U/L GGT 96 U/L ALP 107 U/L AST 143 U/L

Diagnosis and Plan
Decompensated ALD with increasing ascites and mild encephalopathy
Lactulose 30mL 3-4 times daily Ascitic tap with albumin cover Fluid restrict 1.5L/day Low salt Weigh daily Add frusemide 40mg mane

1. Which lab tests indicate liver disease? Which tests are used to assess disease severity?
2. What are the common complications of chronic liver disease (seen in this patient + any others) and describe briefly the main forms of treatment for each of the complications. Consider current therapy
3. What pharmacokinetic changes occur in chronic liver disease that effect drug metabolism?
4. What are the pharmacodynamic changes that occur in chronic liver disease that effect drug dosing?
5. What are the potential problems with aminoglycoside and analgesic use in this patient?