drugs for heart failure
TRANSCRIPT

Drugs for heart failure
Dr. Karun Kumar
JR – II
Dept. of Pharmacology





Pathophysiology
• End stage of CVD that impair the ability of ventricle• To fill with blood ; or
• Eject blood into the circulation
• Causes IHD (m/c), HTN, valvular disorders, arrhythmias, CMP, and constrictive pericarditis.
• Less common Severe anaemia, B1 deficiency, or the use of certain anticancer drugs, such as doxorubicin, Transtuzumab

Cardiac or ventricular remodeling
• characterized by 1.cardiac dilatation, 2.ventricular wall thinning, 3.interstitial fibrosis, 4.wall stiffness.
• Impair the ability of the heart to relax or contract.
1. Activation of neuroendocrine systems (RAAS, SNS, inflammatory cytokines, local mediators [endothelin]) in response to myocardial ischemia Eg. angiotensin II induces collagen production and proliferation of fibroblasts.
2. Excessive stretch of muscle fibers

• Hallmark of HF ↓ SV & CO at any given diastolic muscle fiber length, by measuring the ventricular end diastolic pressure (preload).
• ↓ stroke volume Due to
1. Diastolic dysfunction (Inability of the ventricles to fill properly) ↓ compliance (↑ stiffness) of ventricular tissue secondary to LVH/fibrosis
2. Systolic dysfunction (Inability of the ventricles to empty properly) Due to ↓ cardiac contractility secondary to a dilated or ischemic myocardium.
• Both SHF/DHF caused by cardiac remodeling
• LVF - LV does not adequately pump blood forward Pr. in pulm. Circul. ↑ Forces fluid into lung interstitium Congestion & edema
Pulmonary edema
• ↓ diffusion of O2 & CO2 b/w alveoli & pulmonary capillaries Hypoxemia (deficient oxygenation of the blood) dyspnea (difficulty in breathing), including exertional dyspnea (dyspnea provoked by exercise), orthopnea (intensified dyspnea when lying flat), and paroxysmal nocturnal dyspnea(edema induced bronchoconstriction when sleeping)

• RVF – Cong. in peripheral veins ankle edema(ambulatory pt) & sacral edema(bedridden patient)
• Also, hepatojugular reflux (↑ jugular vein distention when pressure is applied over liver)
• RHF leads to LHF (LV forced to work harder for CO) .
• ↓ CO Compensatory neuroendocrine responses (RAAS & SNS) which are counterproductive

• Both RAAS & SNS cause vascoconstriction
• Arterial vc↑ aortic impedance to LV ejection & ↓ CO
• Angn II ADH,Ald.,cardiac remodeling & vent.wallthinning or fibrosis (↓ systolic & diastolic function)
• Net result Further ↓ CO & ↑ circul. congestion

Drug therapy goals
1. Improve symptoms
2. Slow / reverse deterioration in myocardial func.
3. Prolong survival
• Drugs can also be used to treat underlying conditions, control arrhythmias, prevent thrombosis, and treat anemia.


Drugs used for heart failure
1. ↑ CO (+ve inotropic drugs & vasodilators)
2. ↓ pulmonary & systemic congestion (Diuretics)
3. Slow or reverse cardiac remodeling (Ang & sym. Inh.)
• Most significant dev. Ang. inhibitors, β blockers,
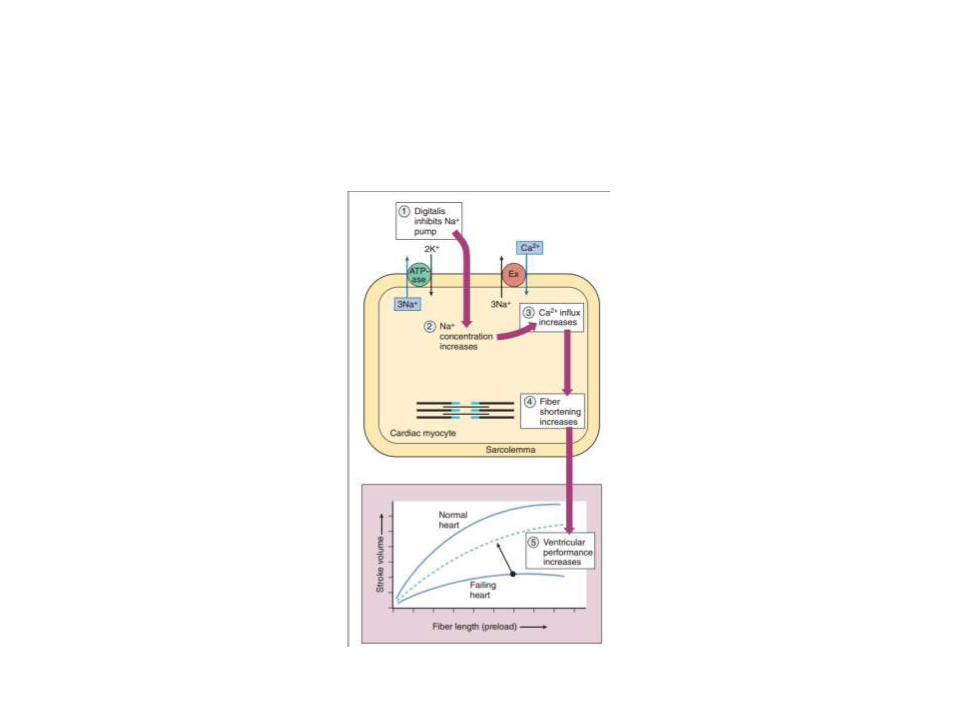
• +ve inotropic drugs (Greek words for “fier” (inos) and “turning” or “to turn” (tropikos), the term inotropic refers to a change in muscle (fiber) contractility. (Digoxin, dobutamine, milrinone) [All 3 act by ↑ Calcium level in cardiac myocytes]

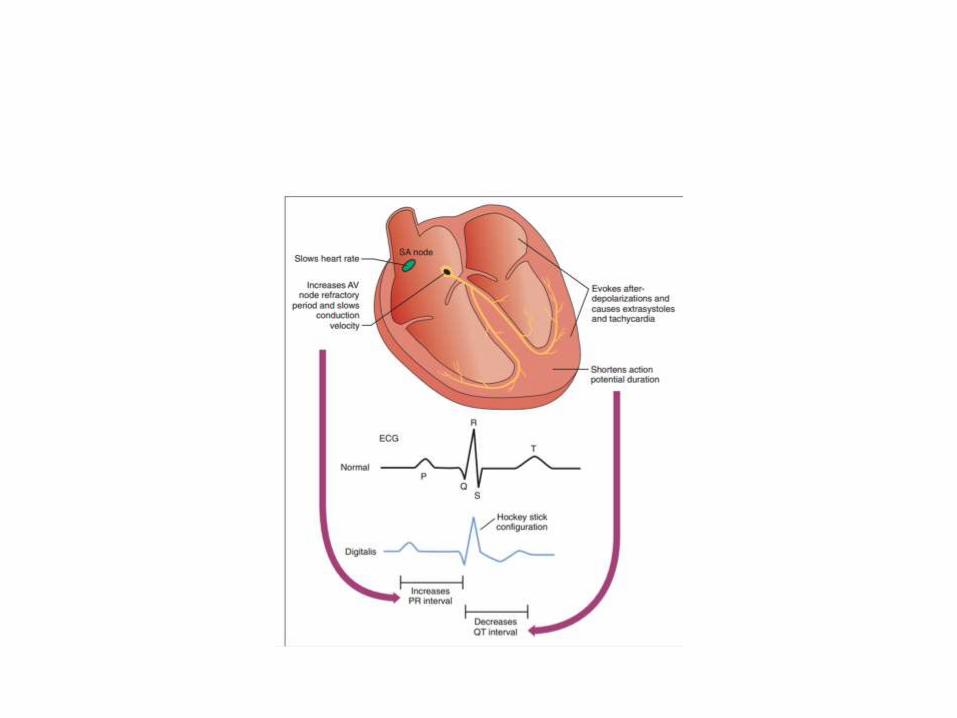
Digoxin
• t1/2 36 hours (Elim. by renal excretion)
• Narrow TI (Dose range 0.5 – 2 ng/ml)
• +ve inotropic,-ve chronotr & -ve dromo effect
• +ve Inotropic ↑ intracell Ca (inh. Na +,K+ATPase)
• -ve chrono & dromo↑ parasympathetic (vagal) tone & ↓ HR & AVN conduction velocity while ↑ AVN refractory period (slows rate in AF)
• At the same time ↓ sympathetic tone (↓ vc)


Adverse Effects
• GI, cardiac & neurologic reactions
• Earliest signs of toxicity anorexia, N & V
• Arrhythmias (most serious manifestation) AV block and various tachyarrhythmias.
• Hypokalemia can precipitate arrhythmias in patients receiving digoxin
• neurologic blurred vision and yellow, green, or blue chromatopsia (a condition in which objects appear unnaturally colored); seizures.
• gynecomastia (estrogenic activity)

Interactions
• Antacids and cholestyramine ↓ abs. of Digoxin
• Diltiazem, quinidine & verapamil ↓ Digoxin clearance
• Loop & thiazide diuretics hypokalemia (↓ K conc. ↑ digitalis binding to Na pump)
• Hypokalemia can also contribute directly to arrhythmias

Indications
• Syst. HF Inotropic effect & -ve chr., drom
• NOT in diastolic HF contractility not impaired
• HF + AF Most certain indication
• Digoxin Immune Fab (i.v.( Igs from sheep immunized with a digoxin derivative.
Dobutamine (cont. i.v. infusion)
• HF More freq. (selectively stimulates cardiac contractility & causes less tachycardia than other β-agonists)
• Also activates β2 in vascular smooth muscle
• Short term mx Acute HF & cardiogenic shock
Milrinone (Inodilator)
• Inhibits type 3 PDE in heart & vasc. Sm. Musc.
• Short term mx of HF, advanced HF & inotropic support of infants & children awaiting cardiac transplantation
• Long term use Thrombocytopenia & ventricular arrhythmias and is associated with increased mortality in patients with severe heart failure

Vasodilators
• angiotensin inhibitors, Hydral. + IDN, nesiritide
• ↓ venous pressure (↓ edema)
• ↓ arterial pressure (↓ cardiac afterload & ↑ CO)
• Also, angiotensin inhibitors slow or reverse cardiac remodeling
• ACE I DNephr, HTN & HF (counteract card. Rem.)
• Ang II Vc, cardiac remodelling, ald., ADH
• Ace i prevent the transition from asymptomatic to overt heart failure
• Acute MI improve survival (within 24 hours) [prevents cardiac remodelling by Ang II]

Angiotensin Receptor Blockers
• Do not inhibit bradykinin degradation and are not prone to induce chronic cough
• As effective as ACE inhibitors in treating heart failure.
• Indic. pts. who cannot tolerate ACE inhibitor.
• Valsartan, Candesartan

Hydralazine and Nitrates
• IDN Relaxes venous smooth muscle,
• Hydralazine relaxes arterial smooth muscle
• combined use ↓ cardiac preload (↓ venous pressure and edema) & afterload (↑ CO)
• pts with HF who cannot tolerate an angiotensin inhibitor.

Nesiritide (only i.v.)
• human B-type NP from E. coli using rDNA
• T/t of patients with acutely decompensated heart failure who have shortness of breath (dyspnea) at rest or with minimal activity.
• Nesiritide binds to g.c. receptor in vascular smooth muscle and endothelial cells ↑ cGMP dilate venous and arterial smooth muscle
• A/E hypotension

PCWP

β-blockers
• Exc. SNS Cardiac remodeling by :-
1. Tachycardia (β1 receptors) ↑ MOD
2. RAAS
3. Chr. Stim. of cardiac β rec. myocytehypertrophy & apoptosis Cardiac dilatation & ventricular wall thinning
4. ↑ cardiac cytokines (TNF α & Ils) induce myocyte hypertrophy and apoptosis Fibrosis & ventricular wall stiffness.
• β bl. ↓ exc. Sympath. Stimul. of heart (Mild to severe HF caused by LV systolic dysfunction)
•

• Carvedilol β1,β2, α1 (vd); antioxidant, antiinflmmatory and antiapoptotic (multiple-action neuroendocrine antagonist).
• Given in symptomatic HF without hypotension, pulmonary congestion, or AV block.
• A/E Bradycardia, worsening heart failure, and dizziness or light headedness (vd & ↓ BP)
• Started on low doses & then gradually ↑ (beneficial effects have a delayed onset of action & a/e occur immediately)
• Also, can lead to ↑ symptoms for 4 to 10 weeks before any improvement is noted

Aldosterone antagonists
• Prev. A/E of exc. Ald. on heart
• patients should be monitored closely (hyperkal.)
• Spironolactone produces endocrine side effects resulting from its binding to androgen and progesterone receptors and leading to gynecomastia and impotence in some male patients.
• Eplerenone produces fewer endocrine side effects than spironolactone

Diuretics
• HF - ↓ plasma volume & edema Relieve symptoms of volume overload (dyspnea)
• Loop diuretics are preferred but must be used carefully to avoid dehydration, hyponatremia, and hypokalemia
• Hypokalemia ↑ risk of digoxin toxicity
• Thiazide diuretics used when a lesser degree of diuresis is required
Management of heart failure• Goals of therapy
1. Relieve symptoms
2. improve quality of life
3. prolong survival.
• Acute HF Hospitalization & i.v. vasodilators (NO3& Nesiritide), diuretics, inotropic agents, & O2
• Once stabilized Oral medications, dietary restrictions, & exercise guidelines
• Bed rest early course of therapy
• Incremental exercise program After improving
Management of chronic HF
• Depends on
1. underlying cause
2. degree of cardiac dysfunction
3. Signs & symptoms exhibited by patient
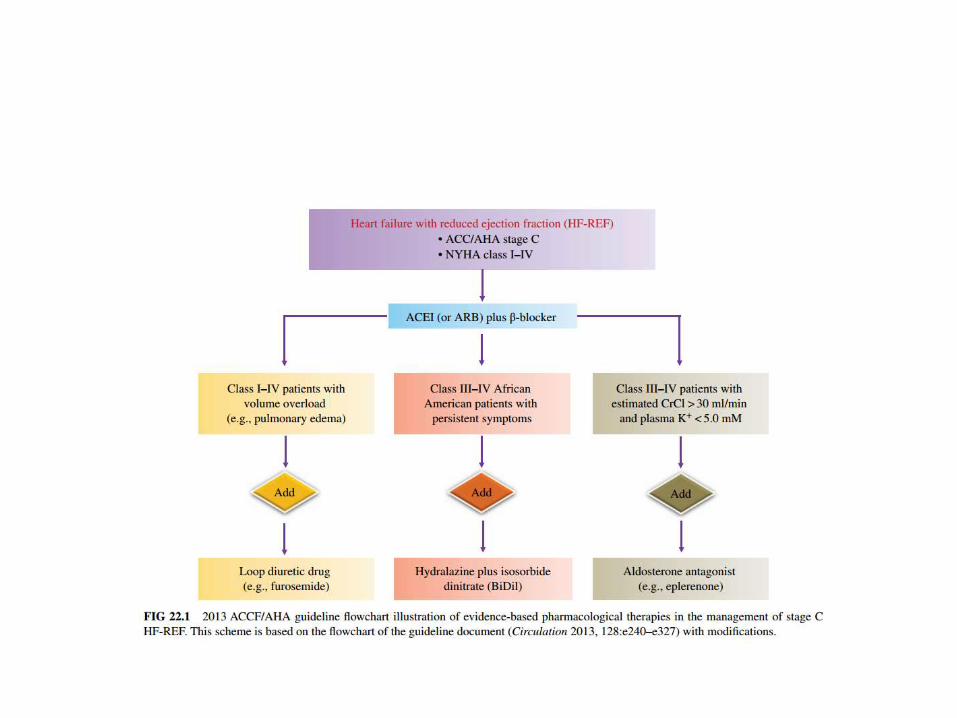
• Systolic HF ACE i.+ BB + loop diur. + ald. Antag.
• Some patients benefit by addition of digoxin &/or combination of hydralazine and a nitrate, whereas anticoagulant and antiplatelet drugs may be needed by some patients.
• ARBs Cannot tolerate an ACE inhibitor.