drug(s) of choice in atrial fibrillation
TRANSCRIPT

CIC-P Nancy
ESC-HFA 2015Antithrombotics in heart failure: the controversy continues
Antithrombotic Drug(s) of choice in atrial fibrillation.(in pts with HF)
Faiez ZannadHypertension and Heart Failure Unit,Inserm Clinical Investigation Center
Institut Lorrain du Coeur et des VaisseauxCHU and Univeristé de Lorraine, France
DGOS
CIC-P Nancy

CIC-P Nancy
Disclosures• Relative to this presentation: Chair steering committee
COMMANDER HF (J&J)• Otherwise:
• steering committee fees : Bayer, Boston Scientific, Janssen, Novartis, Pfizer, Resmed, and Takeda
• Consultant/scientific advisory board fees : Air Liquide, Amgen, CVRx, Relypsa, Servier, St Jude, Stealth peptide, ZS Pharma; Quantuum Genomics.
• co-founder of CRS.• Institution receives research grant from Roche Diagnostics.

CIC-P Nancy
OutcomesHF
No HF
HF vs. No HFHR (95% CI) p
CV Outcomes Stroke or systemic embolization 1.99 2.32 0.94 (0.78, 1.13) 0.51Stroke, systemic embolization, or vascular death
5.00 3.50 1.28 (1.11, 1.47) <0.01
Stroke 1.84 2.16 0.95 (0.78, 1.15) 0.57Systemic embolization 0.17 0.17 0.93 (0.48, 1.82) 0.84All-cause death 5.26 3.37 1.34 (1.17, 1.55) <0.01Vascular death 3.53 1.75 1.65 (1.37, 1.98) <0.01Myocardial infarction 1.15 0.71 1.20 (0.89, 1.63) 0.23
Bleeding Outcomes Major or NMCR bleeding 14.12 15.73 1.00 (0.92, 1.08) 0.99Hemorrhagic stroke 0.29 0.45 0.73 (0.45, 1.20) 0.22Intracranial hemorrhage 0.53 0.77 0.84 (0.58, 1.22) 0.36
Rocket AF. Higher rate of thrombotic events in HF (LVEF<40%)
Sean van Diepen et al. Circ Heart Fail. 2013;6:740-747

CIC-P Nancy
Stroke or SE Vascular Death
With sHF Without sHF0
0.5
1
1.5
2
2.5
Rate
(% p
er y
ear)
1.75
1.35
HR=1.30 (1.08-1.57) P=0.005
With sHF Without sHF0
1
2
3
4
5
6
Rate
(% p
er y
ear)
4.69
1.67
HR=2.82 (2.47-3.21) P<0.001
N=4904 N=4904N=13209 N=13209
RELYSymptomatic HF is associated with higher
rates of stroke/SE and vascular death.
Adapted from Ferreira J et al , AHA 2011
CIC-P Nancy
Warfarin, The gold standard
• Guidelines (ACC/AHA and ESC): • class I recommendation in all patients with heart failure and
atrial fibrillation in the absence of contraindications.
• Evidence: • High-level evidence (A)• Meta-analysis of 29 clinical trials spanning 18 years: • warfarin reduces stroke risk in patients with Afib by
approximately 64%. (1)
(1) Hart RG et al. Ann Intern Med. 2007;146:857–867

CIC-P Nancy
Warfarin, not simple to use
• Limitations:– Narrow therapeutic window, – Variable amount of time spent in treatment range– Numerous drug-drug interactions– Variable dose requirements, – Unpredictable anticoagulant response– Need for frequent monitoring– Need for a stable diet– Slow onset of action– Bleeding risk most pronounced in older

CIC-P Nancy

CIC-P Nancy
Warfarin, underused
79.2% of warfarin-eligible patients were discharged without a prescription, despite being at high risk for stroke.
Not receiving warfarin was independently associated with a
higher risk of death 1 year after discharge
Hess PL et al. Clinical Cardiology 2012

CIC-P Nancy

CIC-P Nancy
Overall, NOACS, more efficacious than Warfarin
CIC-P Nancy
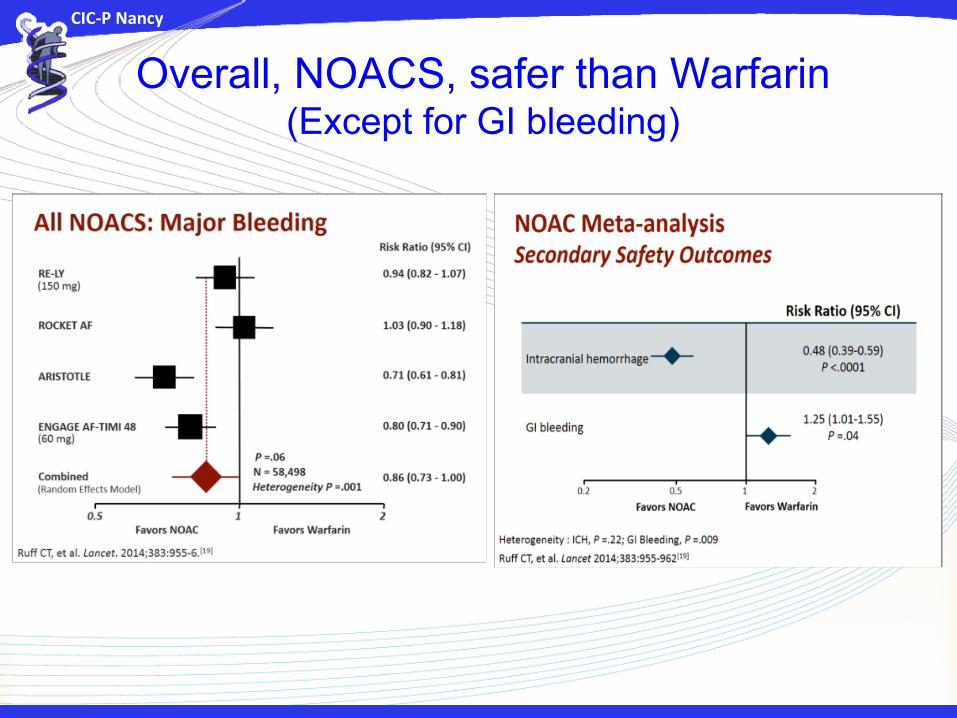
Overall, NOACS, safer than Warfarin(Except for GI bleeding)

CIC-P Nancy

CIC-P Nancy
DE 110 vs. Warfarin DE 150 vs. Warfarin
Rate (% per year)
DE 110 DE WWith sHFWithout sHF
1.90 1.44 1.921.41 1.00 1.64
Stroke or SE
P(Inter)
1.000.50 1.50
0.51
HR & 95% CI
0.50 1.50
0.39
1.00
P(Inter)HR & 95% CI
W better
Major BleedingDE 110 vs. Warfarin DE 150 vs. Warfarin
Rate (% per year)
DE 110 DE W
With sHFWithout sHF
3.26 3.10 3.902.73 3.39 3.45
P(Inter)
1.000.50 1.50
DE better
0.20
HR & 95% CI
0.50 1.50
0.74
1.00
P(Inter)HR & 95% CI
DE better W better
RE-LY , Overall benefits of dabigatran relative to warfarin unchanged in Pts with HF
Adapted from Ferreira J et al , AHA 2011
CIC-P Nancy
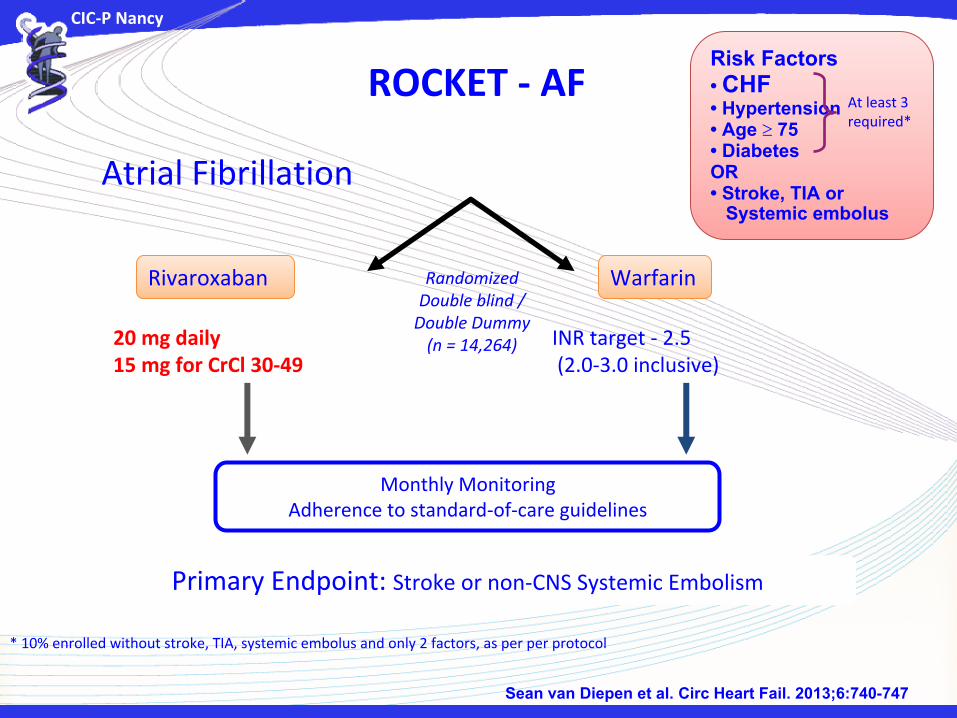
Rivaroxaban Warfarin
Primary Endpoint: Stroke or non-CNS Systemic Embolism
INR target - 2.5 (2.0-3.0 inclusive)
20 mg daily15 mg for CrCl 30-49
Atrial Fibrillation
RandomizedDouble blind /
Double Dummy(n = 14,264)
Monthly MonitoringAdherence to standard-of-care guidelines
ROCKET - AF
* 10% enrolled without stroke, TIA, systemic embolus and only 2 factors, as per per protocol
Risk Factors• CHF • Hypertension • Age 75 • Diabetes OR• Stroke, TIA or Systemic embolus
At least 3 required*
Sean van Diepen et al. Circ Heart Fail. 2013;6:740-747

CIC-P Nancy
Heart Failure Subgroup ITT (n)
Stroke or non-CNS embolism
Rivaroxaban WarfarinRivaroxaban vs.
WarfarinHR (95% CI)
p-valuefor interaction
Ejection Fraction ≥40% 4914 2.00 2.06 0.98 (0.74, 1.31) 0.38
<40% 2521 1.34 1.87 0.72 (0.46, 1.12)
NYHA Class I or II 6217 1.90 2.02 0.94 (0.73, 1.22) 0.68
III or IV 2676 1.88 2.10 0.90 (0.61, 1.32)
No Device 7937 1.96 2.08 0.94 (0.75, 1.18) 0.11
ICD or BiV-ICD 297 0.33 0.17 (0.02, 1.39)
CHADS2 Score 2 610 1.30 1.16 1.09 (0.44, 2.69) 0.48
≥3 8467 1.96 2.18 0.90 (0.72, 1.12)
ROCKET – AF Rivaroxaban and warfarin , both equally effective among pre-specified HF subgroups
Sean van Diepen et al. Circ Heart Fail. 2013;6:740-747

CIC-P Nancy
Heart Failure Subgroup
Safetyn
Major or Non-Major Clinically Relevant Bleeding
Rivaroxaban WarfarinRivaroxaban vs.
WarfarinHR (95% CI)
p-valuefor interaction
E F ≥ 40% 4893 14.18 14.81 1.00 (0.88, 1.13) 0.051< 40% 2497 15.34 14.10 1.15 (0.96, 1.36)
NYHA Class I or II 6205 14.83 14.15 1.08 (0.97, 1.21) 0.19III or IV 2645 12.45 13.54 0.96 (0.80, 1.15)
No Device 7899 13.08 13.72 0.99 (0.89, 1.09) 0.002ICD or BiV-ICD 298 32.43 16.37 2.00 (1.31, 3.05) CHADS2 score 2 610 15.96 10.02 1.54 (1.10, 2.16) 0.15
≥3 8423 14.06 14.42 1.02 (0.92, 1.12)
ROCKET – AF Rivaroxaban and warfarin , both equally safe among pre-specified HF subgroups
Sean van Diepen et al. Circ Heart Fail. 2013;6:740-747
CIC-P Nancy
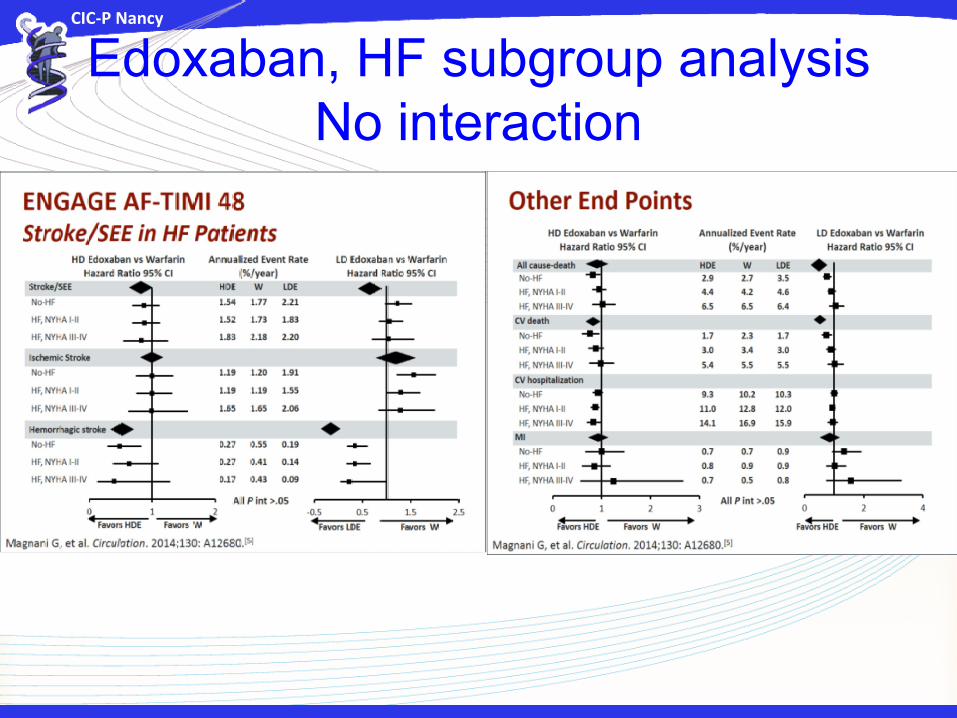
Edoxaban, HF subgroup analysis No interaction
CIC-P Nancy
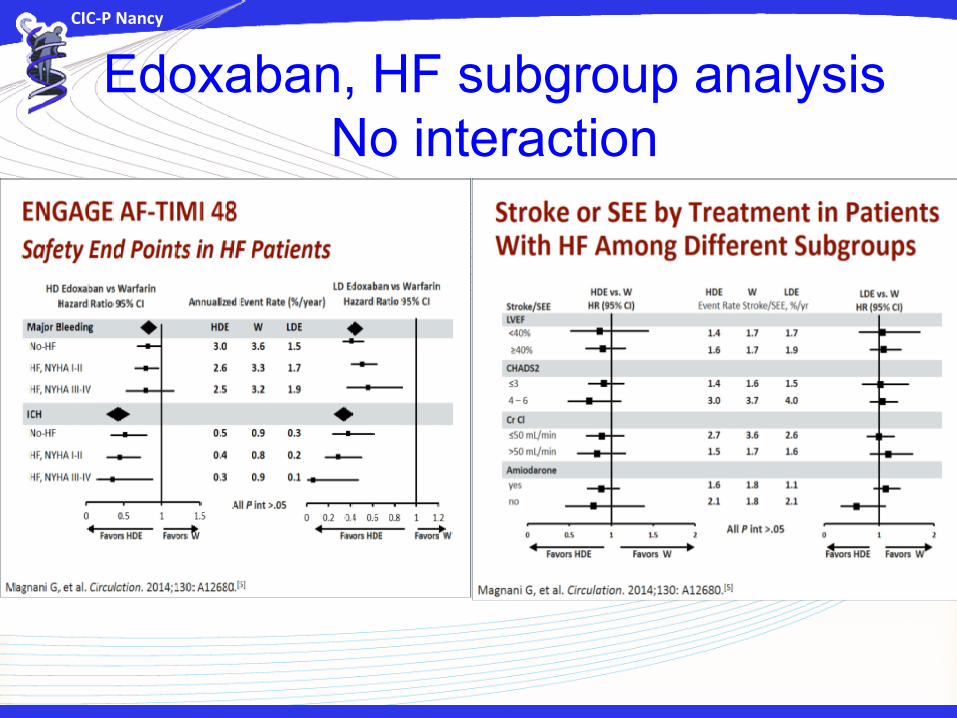
Edoxaban, HF subgroup analysis No interaction

CIC-P Nancy

CIC-P Nancy
CIC-P Nancy
New oral anticoagulant drugs (direct thrombin inhibitors and factor Xa inhibitors)
• contraindicated in severe renal impairment (creatinine clearance < 30 mL/min).
• Clearly a concern in many patients with HF• If used, serial monitoring of renal function is
required. • There is no known way to reverse the
anticoagulant action of these new drugs.

CIC-P Nancy
CIC-P Nancy
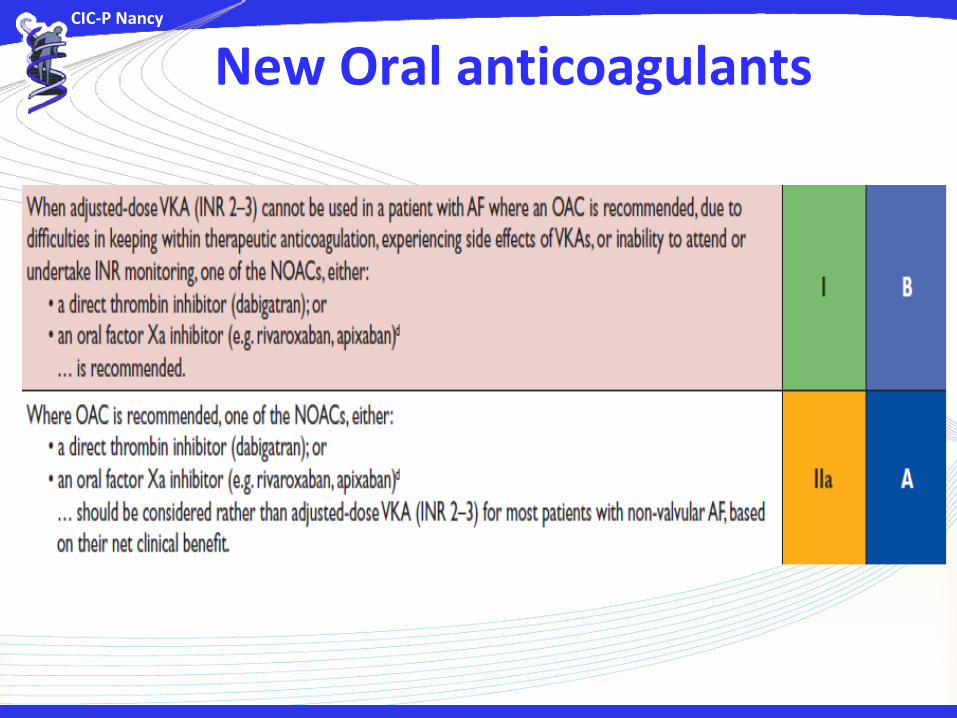
New Oral anticoagulants