dual antegrade his bundle pathways with alternating bundle branch block
TRANSCRIPT

1784 Ahmed et al.
intracardiac masses, often incidentally. However, in some patients such as ours, characterization of the mass may be difficult because of technical limitations. TEE offers better resolution and therefore diagnostic accuracy particularly with left-sided cardiac involvement. In a recent report by Fegan et al.,‘” TEE was able to detect a recurrent right ventricular myxoma that was missed by TTE. TEE has been used to guide catheter positioning in procedures such as ablation of accessary pathways in Wolf-Parkinson White syndrome. The endomyocardial biopsy procedure is a safe nonsurgical approach for obtaining biopsy samples from endocardial masses, where tissue confirmation is frequently needed before specific potentially harmful therapy in indi- cated (e.g., surgery, radiation therapy, chemotherapy, or thrombolysis/anticoagulation). The endomyocardial bi- opsy procedure is usually performed under fluoroscopic guidance.‘, 5 However, when the procedure is used under fluoroscopic guidance alone, only samples from the intra- ventricular septum can be obtained safely.’ Miller et al.” have recently reported the utility and safety of endomyo- cardial biopsy done under TTE guidance in patients after orthotropic cardiac transplantation. The biopt.ome tip could always be seen, and biopsy specimens could be obtained from the cardiac apex and the right ventricular free wall in those patients. Other investigators33 ’ used TTE with fluoroscopy for guidance of transvenous biopsy of in- tracardiac atria1 tumors. Our case demonstrates the use- fulness of TEE in obtaining tissue diagnosis in a patient with an intracardiac mass. Results of TTE were subopti- mal, whereas TEE was helpful in guiding the bioptome during transvenous endomyocardial biopsy. This tech- nique is safe and offers less radiation exposure and better image resolution, and it is more precise in positioning the bioptome.
REFERENCES
1.
2.
3.
4.
5.
6.
7.
8.
9.
Flipse TR, Tazelaar HD, Holmes Jr DR. Diagnosis of malig- nant cardiac disease by endomyocardial biopsy. Mayo Clin Proc 1990;65:1415-22. Miller LW, Labovitz AJ, McBride LA, Pennington DG, Kanter K. Echocardiography-guided encomyocardial biopsy. A 5-year experience. Circulation 1988;78(suppl III):III-99-102. Morrone A, Gaglione A, Bortone A, Ileceto, Caruso G, Cala- brese P, Chiddo A. Diagnosi mediante biopsia endomicardica di microcitoma polmonare metastatizzato in atrio. Cardiologia 1988;33:419-21. Copeland JG, Valdes-Cruz L, Sahn DJ. Endomyocardial biopsy with fluoroscopic and two-dimensional echocardio- graphic guidance: case report of a patient suspected of having muitiplecardiac tumors.-Clin Cardiol 1984;7:449-52. Aretz HT. The endomyocardial biopsy revisited [Editorial]. Mayo Clin Proc 1990;65:1506-9. Thomas AC, Mills PG, Giggs NM, Davies JM. Secondary car- cinoma of left atrium simulating mvxoma. Br Heart .I 1980; - ” 44:541-4. Roudaut R, Reynaud P, Koch M, Durandet P, Gosse, Dalloc- chio M. L’echocardiogrphie bidimensionnele dans le diagnos- tic des metastases intracardiaques. Arch Ma1 Coeur 1990; 83:1435-g. Malaret GE, Aliaga P. Metastatic disease to the heart. Cancer 1968;22:457-66. Kotler MN. Metastatic cardiac tumors: recognition of peri- cardial, myocardial and endocardial involvement by two-
10.
11.
12.
13.
June 1993 American Heart Journal
dimensional echocardiography. In: Kapoor A, ed (‘ancer 01 the heart. Berlin: Springer-Verlag, 1986:X)-61 Bisel HF, Wroblewski F, LaDue +JS. Incidence and clinicai manifestations of cardiac metastases. *JAMA 1953;15:?712-5. Hanfling SM. Metastatic cancer to the heart, Circulation 1960;22:474-83. Goldman AP, Kotler MN, Parry WR. Atrial tumors. In: Kapoor A, ed. Cancer of the heart. Berlin: Springer-Verlag. 1986:81-109. Fagan LF, Caste110 R, Barner H, Moran M, Labovitz AJ. Transesophageal echocardiographic diagnosis of recurrent right ventricular myxoma 2 years after excision of right atrial myxoma. AM HEAFX J 1990;120:1456-8.
Dual antegrade His bundle pathways with alternating bundle branch block
Rafique Ahmed, MD, PhD, Philip T. Sager, MD, Mahnaz Behboodikah, MD, and Bramah N. Singh, MD. PhD Los Angeles, Calif.
Longitudinal dissociation in the His bundle has been sug- gested based on experimental studies’ and the finding that distal His bundle pacing in some patients with an electro- cardiographic pattern of apparent bundle branch block (BBB) normalizes the ECG. ‘9 3 We report a case in which a dual His bundle pathway was observed during electro- physiologic study with a left or right BBB pattern depend- ing on which pathway conducted the impulse.
A 68-year-old man with a history of hypertension, coro- nary artery disease, and coronary artery bypass surgery was referred for evaluation of sustained ventricular tachycar- dia. Physical examination findings were unremarkable, and routine blood chemistry determinations were within nor- mal limits. ECG showed normal sinus rhythm, a normal PR interval, and a normal QRS axis with a nonspecific intra- ventricular conduction defect. The patient was not taking any cardioactive medication at the time of initial evalua- tion. Electrophysiologic study was performed with three quadripolar catheters introduced through the right fem- oral vein and placed in the high right atrium, right ventric- ular apex, and across the tricuspid valve for His bundle re- cording. During sinus rhythm the AH interval was 70 msec and the HV interval was 70 msec. Atria1 extrastimulus at a basic drive cycle length (BCL) of 600 msec demonstrated a normal QRS pattern at HI-Hz of 410 msec with an Ha-V2 interval of 75 msec (Fig. 1, top panel). At HI-HZ of 400 msec
From the Section of Cardiology, Department of Medicine, West Los Ange- les Veterans Administration Medical Center and UCLA School of Medicine. Reprint requests: Rafique Ahmed, MD, PhD, Section of Cardiology, Wl llE, West Los Angeles VA Medical Center. Wilshire and Sawtele Blvd., Los An- geles, CA 90073. AM HEART J 1993;125:1784-1786
Copyright ‘, 1993 by Mosby-Year Hook. Inc. 0002.8703/93/51.00 + .lO 4/4/45671
Volume 125, Number 6 American Heart Journal
Ahmed et al. 1785
CL: 600 ms Vl
V --I y VS
i* -s1 Sl S2 HRAh 4
H,H,:410 I
L I
H,V,:76 flEEI I
1 I
P , L p
1 n,v*:so
I
v1-' _
A,A,:320
Fig. 1. Electrophysiologic recording during atria1 extra- stimulus at BCL 600 msec (see text for details).
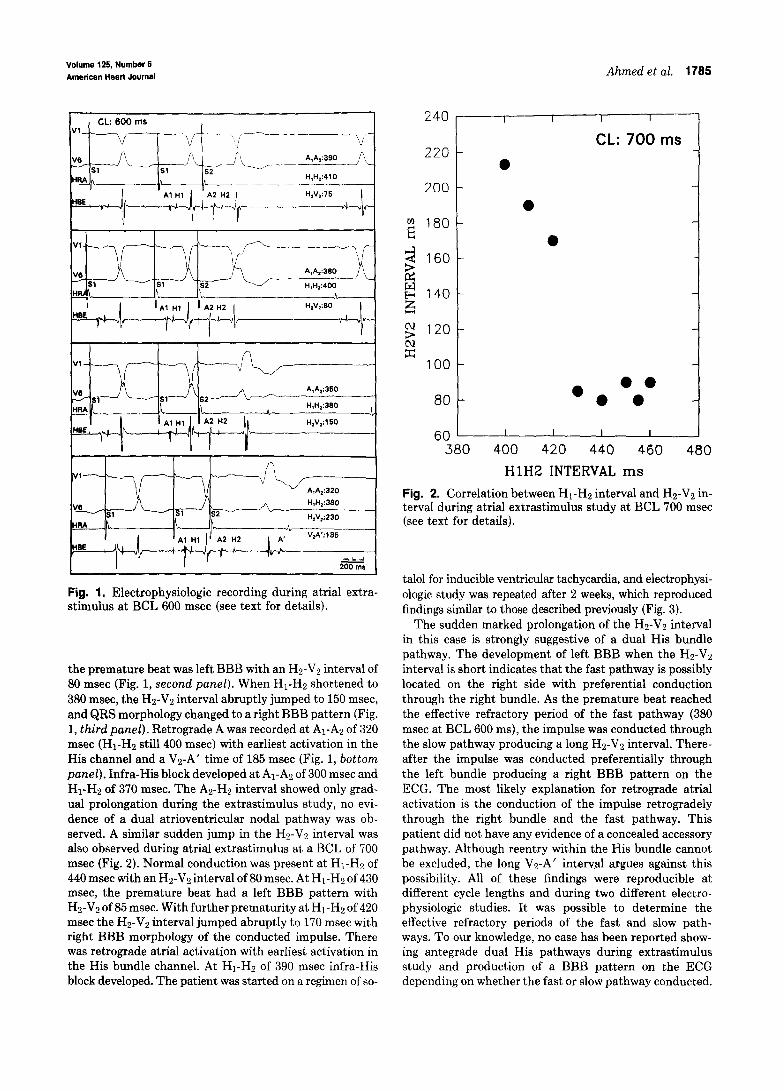
the premature beat was left BBB with an Hz-V2 interval of 80 msec (Fig. 1, second panel). When HI-HZ shortened to 380 msec, the Hs-Vs interval abruptly jumped to 150 msec, and QRS morphology changed to a right BBB pattern (Fig. 1, third panel). Retrograde A was recorded at Al-A:! of 320 msec (HI-HZ still 400 msec) with earliest activation in the His channel and a Vz-A’ time of 185 msec (Fig. 1, bottom panel). Infra-His block developed at Al-A2 of 300 msec and Hi-Hz of 370 msec. The As-H2 interval showed only grad- ual prolongation during the extrastimulus study, no evi- dence of a dual atrioventricular nodal pathway was ob- served. A similar sudden jump in the Hz-V2 interval was also observed during atria1 extrastimulus at a BCL of 700 msec (Fig. 2). Normal conduction was present at HI-HZ of 440 msec with an Hz-V2 interval of 80 msec. At Hi-Hz of 430 msec, the premature beat had a left BBB pattern with Hz-V2 of 85 msec. With further prematurity at Hi-H2 of 420 msec the Hz-V2 interval jumped abruptly to 170 msec with right BBB morphology of the conducted impulse. There was retrograde atria1 activation with earliest activation in the His bundle channel. At HI-HZ of 390 msec infra-His block developed. The patient was started on a regimen of so-
240 3,
220 - CL: 700 ms
l 200 -
UJ ?z
180-
< i=i
160-
2 140- w
g 120-
2 100 -
80 _
l
l
l e l e l
60 ' I I I I I 380 400 420 440 460 480
HlH2 INTERVAL ms
Fig. 2. Correlation between Hi-Hz interval and Hz-Vs in- terval during atria1 extrastimulus study at BCL 700 msec (see text for details).
talol for inducible ventricular tachycardia, and electrophysi- ologic study was repeated after 2 weeks, which reproduced findings similar to those described previously (Fig. 3).
The sudden marked prolongation of the Hz-V2 interval in this case is strongly suggestive of a dual His bundle pathway. The development of left BBB when the Hz-V2 interval is short indicates that the fast pathway is possibly located on the right side with preferential conduction through the right bundle. As the premature beat reached the effective refractory period of the fast pathway (380 msec at BCL 600 ms), the impulse was conducted through the slow pathway producing a long Hz-V2 interval. There- after the impulse was conducted preferentially through the left bundle producing a right BBB pattern on the ECG. The most likely explanation for retrograde atria1 activation is the conduction of the impulse retrogradely through the right bundle and the fast pathway. This patient did not have any evidence of a concealed accessory pathway. Although reentry within the His bundle cannot be excluded, the long Vs-A’ interv.al argues against this possibility. All of these findings were reproducible at different cycle lengths and during two different electro- physiologic studies. It was possible to determine the effective refractory periods of the fast and slow path- ways. To our knowledge, no case has been reported show- ing antegrade dual His pathways during extrastimulus study and production of a BBB pattern on the ECG depending on whether the fast or slow pathway conducted.

1786 Mendes and Davidoff June 1993
American Heart Journal
A,A,:490 __--
--\_ ,/- H,H,:605
.-- -___
Fig. 3. Atria1 extrastimulus study after administration of sotalol at BCL 700 msec. Upper panel, Normal conduction of premature beat with a Hz-V:! interval of 90 msec. Mid- dle panel, As HI-HZ interval shortens by 10 msec to 505, premature beat is conducted with left BBB pattern and Hz-V2 of 100 msec. Lower panel, Further shortening of HI-HZ interval to 490 msec causes sudden jump of HY-VZ interval to 220 msec with right. BBB morphology of conducted beat.
Narula” and El-Sherif et al.” have reported that patients with a prolonged HV interval and a BBB pattern on the ECG show normalization of the ECG if the distal His bundle is paced. They inferred that the main defect was slowed conduction in the His bundle with functional longitudinal dissociation, which resulted in asynchronous conduction in the bundle branches producing the BBB pattern. Anatomic studies have also shown longitudinal dissociation within the His bundle.4 The findings in the present study bridge the gap between the studies of Narulap and El-Sherif et al.” and experimental animal investigations demonstrating conduction disturbances in the bundle branches produced by lesions in the nonbranching portion of the His bundle.” The clinical implication of the present findings is the explanation of a mechanism of production of the BBB pattern in patients with a prolonged HV interval. Dual His pathways may also appear as alternating short and long PR intervals.” It is also possible that some instances of a rate-dependent aberration in ventricular conduction can be explained by dual His bundle pathways, especially if the aberrant beat is of the left BBB type. In addition, the presence of a dual His pathway has the potential to produce reentrant tach- yarrhythmia.
REFERENCES
1. W&ton A. Boineau J I’, Alexander JA, Sealy WC’. Dissociation and delayed conduction in the canine right bundle branch Circulation 1976;53:605-$3.
2. Narula OS. 1,crngitudinal dissociation in the His Bundle, hun- dle branch block due to asynchronous conduction within His bundle in man. Circulation 1977;56:996-1006.
3. El-Sherit’ Xi. Amat-T-Leon F, Schonfeld C, Scherlag ELI. Rosen K, I,azzara R, Wyndham C. Normalization of bundle branch block patterns by distal bundle pacing; clinical and experimental evidence ol’ longitudinal dissociation in the pathologic His bundle. Circulation 1978;57:473-83,
4. Massing GK, *James TN. Anat,omical configuration of’t.he His bundle and bundle branches in the human heart. Circulation 1976;53:609-‘1.
5, Fabregas RA. Tse WW, Han J. Conduction dist,urbances ofthe bundle branches produced by lesions in the nonbranching portion of His bundle. A&f HEAKT .J 1976;92:356-62,
6. Alboni P, Filippi I,. Padovan (;. Pirani R, Scarf’0 S, Masoni A. Dual antegrade His bundle pathways in man. AV HEXHT J 1984;108:fjl I-1.
Cardiogenic seizure with bradyarrhythmia: Documentation of the mechanism during asystole
Lisa A. Mendes, MD, and Ravin Davidoff, MB, BCh Boston, Mass.
Cardiac syncope is a potentially life-threatening problem in which an inadequate cardiac output results in sudden interruption of cerebral perfusion and loss of conscious- ness.’ Various neurologic disturbances may be associated with the unconscious period including motor twitches, tonic-clonic jerks and, rarely, frank convulsions, making the differentiation between syncope of cardiac origin and epilepsy potentially difficult.:! Failure to distinguish be- tween these two disorders may result in inappropriate therapy and harm to the patient. The following report of an elderly woman with recurrent seizures illustrates the importance of establishing the cause of new-onset seizures in adults, especially elderly patients. Although it is widely believed that profound bradycardia may precipitate sei- zures, the mechanism has never been clearly documented. It is presumed that severe hypotension causes cerebral an- oxia with resultant triggering of a seizure focus. This is the first such case to demonstrate the mechanism of seizure
From the Evans Memorial Department of Clinical Research and the Divi- sion of Cardiology. Department of Medicine. Boston lrniversity Medical Center and Cardiac Unit.
Reprint requests: Lisa A. Mendes, MD, Section uf Cardiology, Universitv Hospital, 88 E. Newton St., Boston, MA 02118.
AIVI HEART .I 1993;1%:1786-1788
Copyright 1993 by Mosby-Year Book. Inc. 0002.8703/93/$1.00 + .lO 4/4/45672