ductal carcinoma in situ (dcis) joanne zujewski, md head, breast cancer therapeutics clinical...
TRANSCRIPT
Ductal Carcinoma In Situ (DCIS)
JoAnne Zujewski, MDHead, Breast Cancer Therapeutics
Clinical Investigations BranchCancer Therapy Evaluation ProgramDivision of Cancer Diagnostics and
TreatmentMay 2011
Questions
• How DCIS differs from Stage 1 breast cancer
• Types of DCIS that affect prognosis of DCIS/development of breast cancer
• Standard of Care: surgery, radiation risks of under-treatment and overtreatment
• Can we improve diagnosis through MRI and sentinel lymph node biopsy?
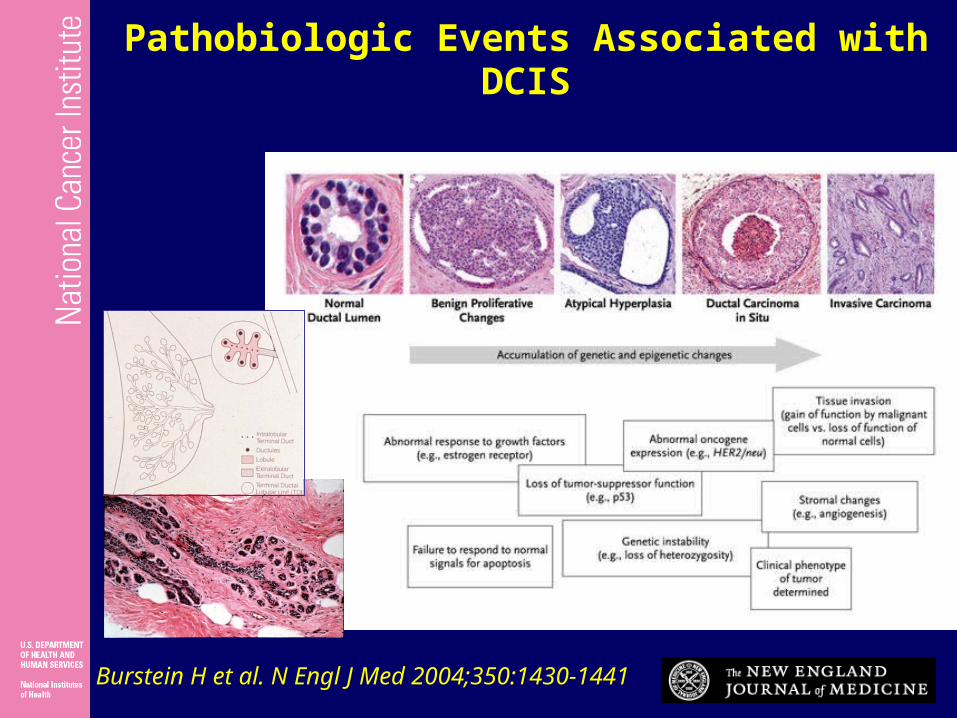
Burstein H et al. N Engl J Med 2004;350:1430-1441
Pathobiologic Events Associated with DCIS

DCIS: Pathology
Rosen’s Breast Pathology, 1997
Comedo Solid,Low grade
Cribiform,High grade
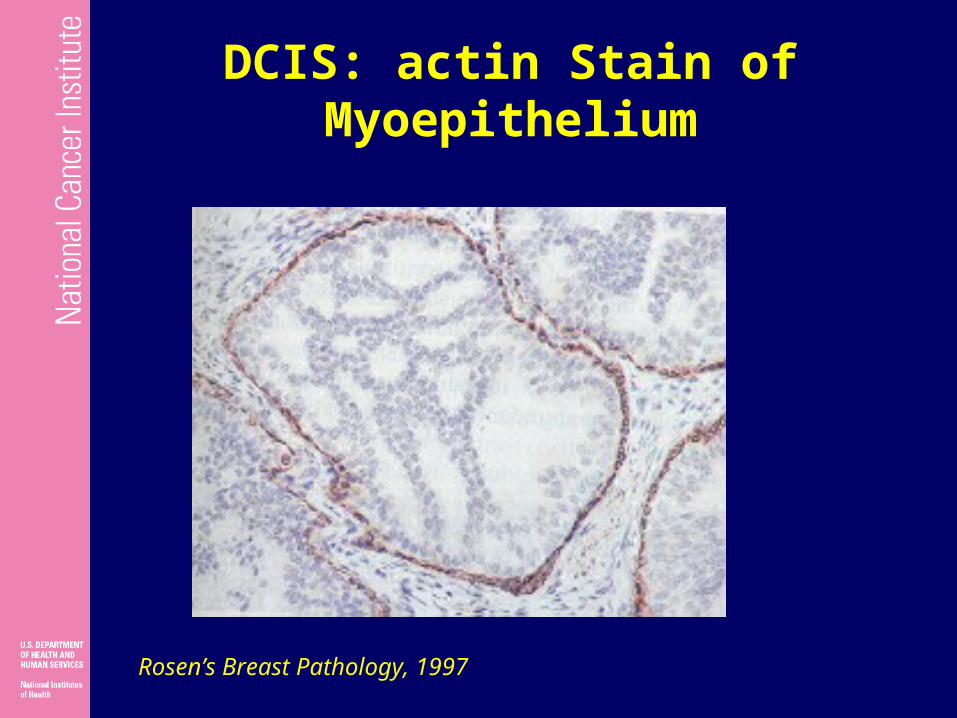
DCIS: actin Stain of Myoepithelium
Rosen’s Breast Pathology, 1997

SEER Breast Carcinoma in situ5-year Survival : 1992-1999
All < 50 50+
All 100.0 99.9 100.0
White 100.0 100.0 100.0
Black 100.0 99.5 100.0
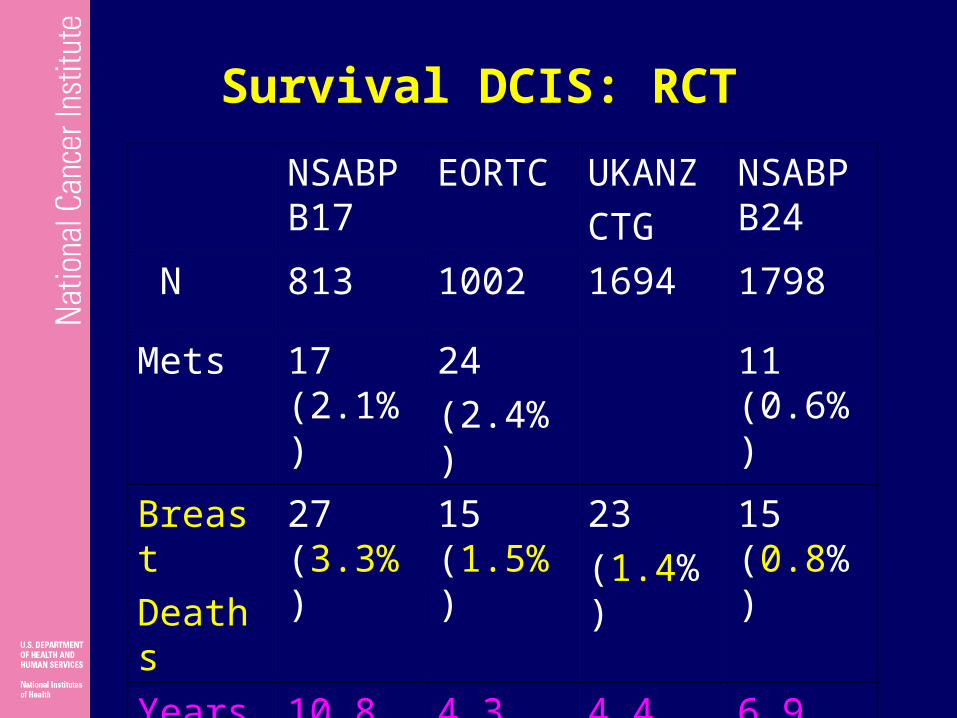
Survival DCIS: RCT
NSABP B17
EORTC UKANZCTG
NSABPB24
N 813 1002 1694 1798
Mets 17 (2.1%)
24(2.4%)
11 (0.6%)
BreastDeaths
27 (3.3%)
15 (1.5%)
23(1.4%)
15 (0.8%)
YearsF/up
10.8 4.3 4.4 6.9
Natural History
• 25 cases untreated with 16 yrs follow up– 28% developed invasive cancer– 11 fold increase in relative risk to
controls
• Contralateral relative risk 2-3
Page et al Cancer 1985;55:2698-708

Role of Total Mastectomy
YearNo.cases
% mortality
Ashikari 1971 182 0.9
Rosner 1980 182 2.0
Farrow 1970 181 2.0
Silverstein
1996 228 0
Bradley 1990 588 1.7
Surgery
• Mastectomy has not been compared to BCT in randomized trials of DCIS
• Breast cancer deaths within 10 years after the diagnosis of DCIS occurs in 1-2% of all patients, irrespective of surgery type

RATIONALE FOR RADIATION TREATMENT AFTER LUMPECTOMY FOR DCIS
• All reported randomized trials show that radiation reduces the rate of local recurrence after lumpectomy by about half
• “[P]atients who may avoid radiation therapy have not been reproducibly and reliably identified by any clinical trials.” (1999 DCIS Consensus Conference Statement, Cancer, 2000)
Slide courtesy of L. Solin
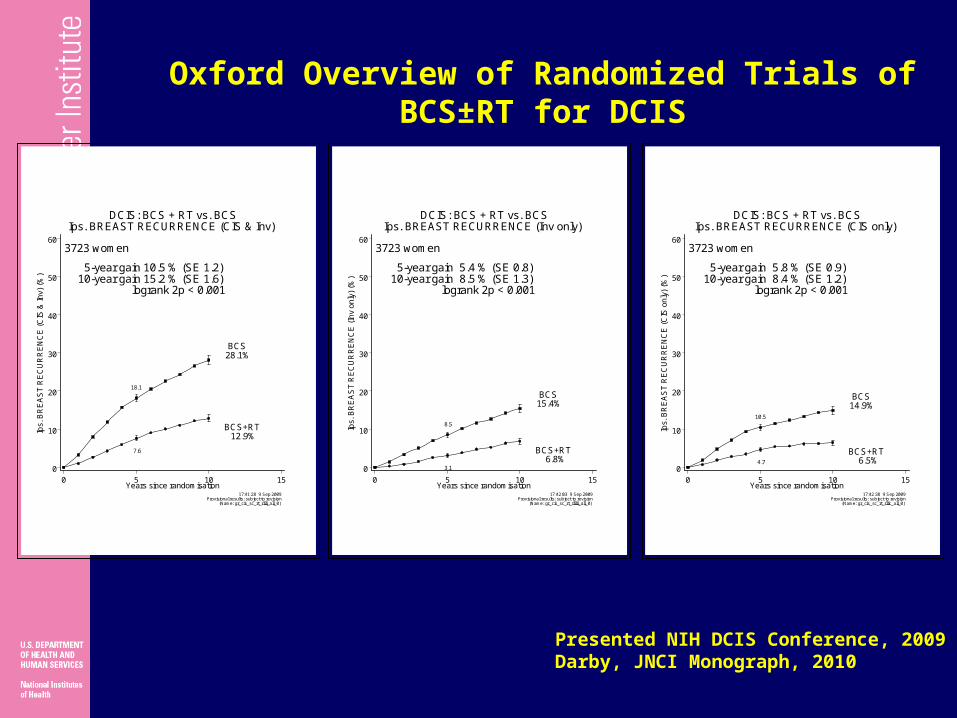
5-year gain 5.4 % (SE 0.8)10-year gain 8.5 % (SE 1.3)
logrank 2p < 0.001
BCS+RT 6.8%
8.5
3.1
BCS15.4%
3723 women
17:42:03 9 Sep 2009Provisional results: subject to revision
(Name: gr_cis_sc_rt_rlilii_all_0)
0
10
20
30
40
50
60
Ips.
BR
EA
ST
RE
CU
RR
EN
CE
(In
v on
ly)
(%)
0 5 10 15Years since randomisation
DCIS: BCS + RT vs. BCSIps. BREAST RECURRENCE (Inv only)
5-year gain 5.8 % (SE 0.9)10-year gain 8.4 % (SE 1.2)
logrank 2p < 0.001
BCS+RT 6.5%
10.5
4.7
BCS14.9%
3723 women
17:42:38 9 Sep 2009Provisional results: subject to revision
(Name: gr_cis_sc_rt_rllic_all_0)
0
10
20
30
40
50
60
Ips.
BR
EA
ST
RE
CU
RR
EN
CE
(C
IS o
nly
) (%
)
0 5 10 15Years since randomisation
DCIS: BCS + RT vs. BCSIps. BREAST RECURRENCE (CIS only)
5-year gain 10.5 % (SE 1.2)10-year gain 15.2 % (SE 1.6)
logrank 2p < 0.001
BCS+RT12.9%
18.1
7.6
BCS28.1%
3723 women
17:41:28 9 Sep 2009Provisional results: subject to revision
(Name: gr_cis_sc_rt_rlili_all_0)
0
10
20
30
40
50
60
Ips.
BR
EA
ST
RE
CU
RR
EN
CE
(C
IS &
Inv)
(%
)
0 5 10 15Years since randomisation
DCIS: BCS + RT vs. BCSIps. BREAST RECURRENCE (CIS & Inv)
Oxford Overview of Randomized Trials of BCS±RT for DCIS
Presented NIH DCIS Conference, 2009 Darby, JNCI Monograph, 2010
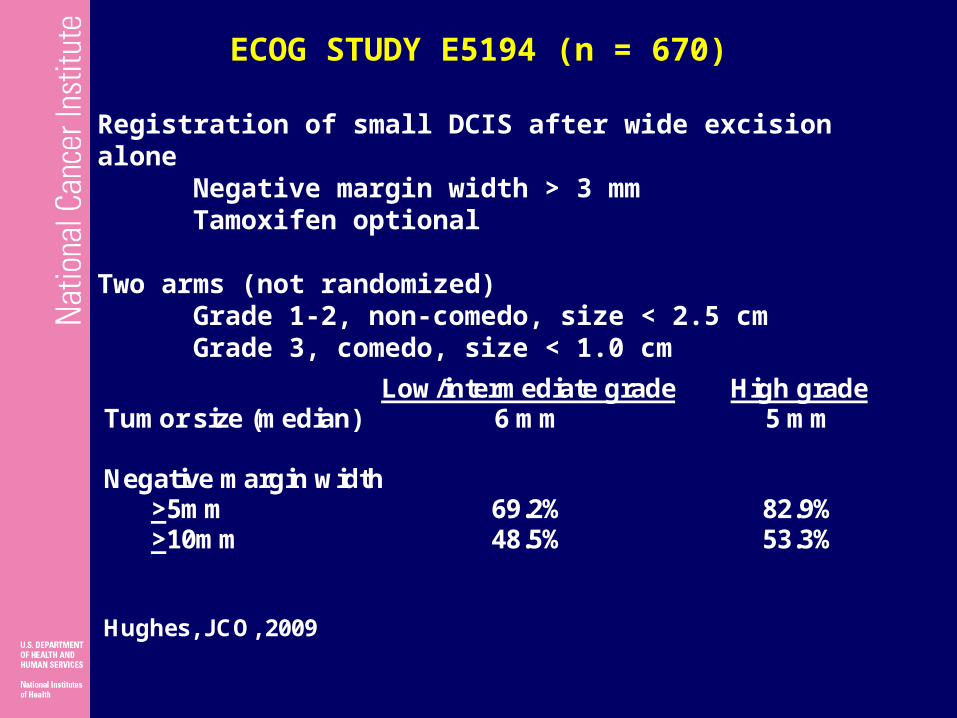
Registration of small DCIS after wide excision aloneNegative margin width > 3 mmTamoxifen optional
Two arms (not randomized)Grade 1-2, non-comedo, size < 2.5 cmGrade 3, comedo, size < 1.0 cm
ECOG STUDY E5194 (n = 670)
Low/intermediate grade High grade Tumor size (median) 6 mm 5 mm Negative margin width >5mm 69.2% 82.9% >10mm 48.5% 53.3% Hughes, JCO, 2009

0 2 4 6 8
0.0
0.05
0.15
Ipsilateral (43 events/ 572 cases)Contralateral (18 events/ 572 cases)
6%
4%
Year
15%
Low or intermediate grade
High gradeECOG E5194: EXCISION WITHOUT RADIATION (+/-TAM)
Hughes, JCO, 2009
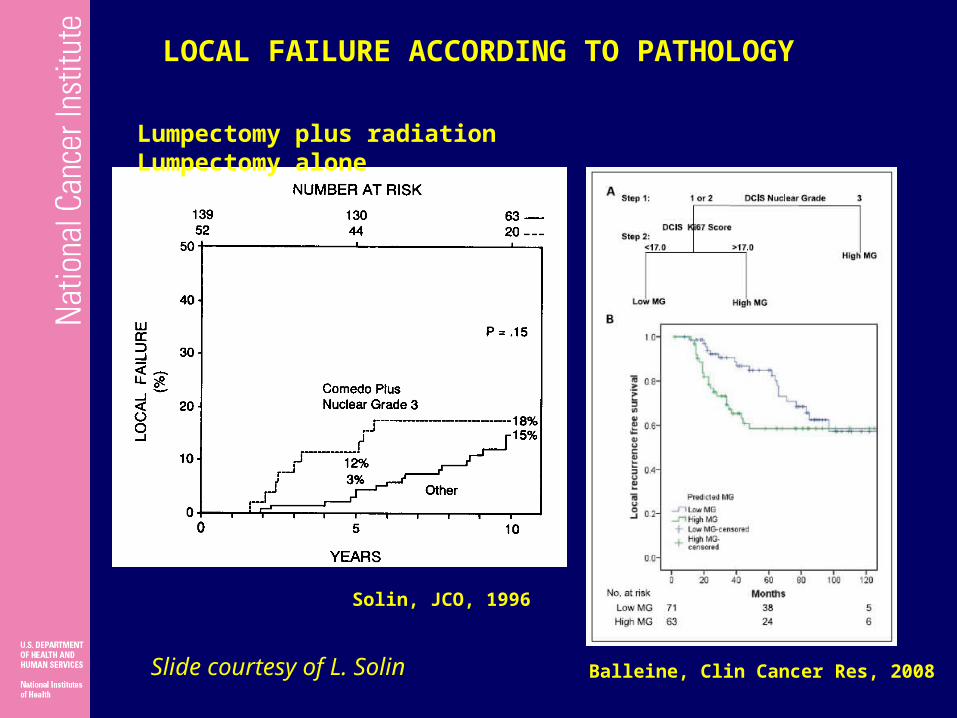
LOCAL FAILURE ACCORDING TO PATHOLOGY
Balleine, Clin Cancer Res, 2008
Solin, JCO, 1996
Lumpectomy plus radiation Lumpectomy alone
Slide courtesy of L. Solin
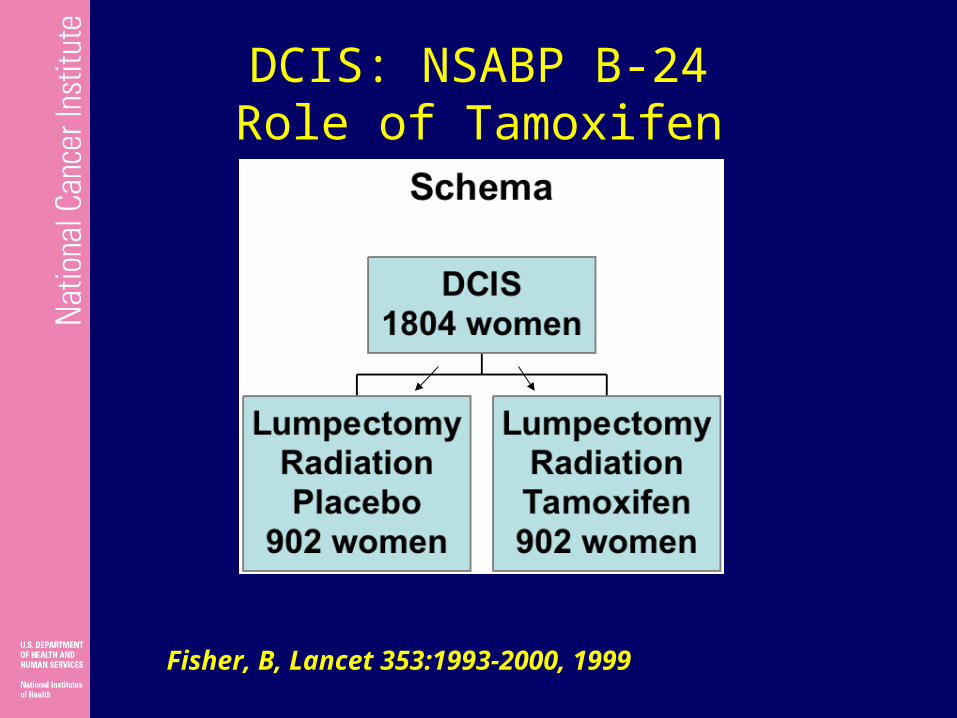
DCIS: NSABP B-24Role of Tamoxifen
Fisher, B, Lancet 353:1993-2000, 1999
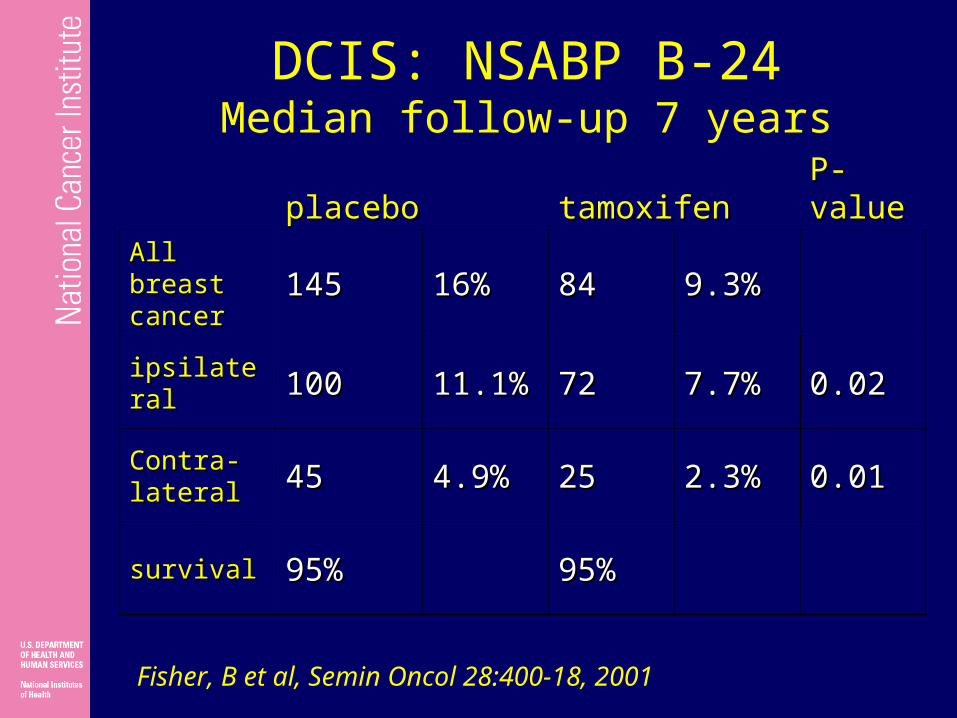
DCIS: NSABP B-24Median follow-up 7 years
placeboplacebo tamoxifentamoxifenP-P-valuevalue
All breast All breast cancercancer 145145 16%16% 8484 9.3%9.3%
ipsilateralipsilateral 100100 11.1%11.1% 7272 7.7%7.7% 0.020.02
Contra-Contra-laterallateral 4545 4.9%4.9% 2525 2.3%2.3% 0.010.01
survivalsurvival 95%95% 95%95%
Fisher, B et al, Semin Oncol 28:400-18, 2001
NSABP B-24: Conclusions
• Tamoxifen decreases risk of breast cancer events by 40%
• No difference in overall survival
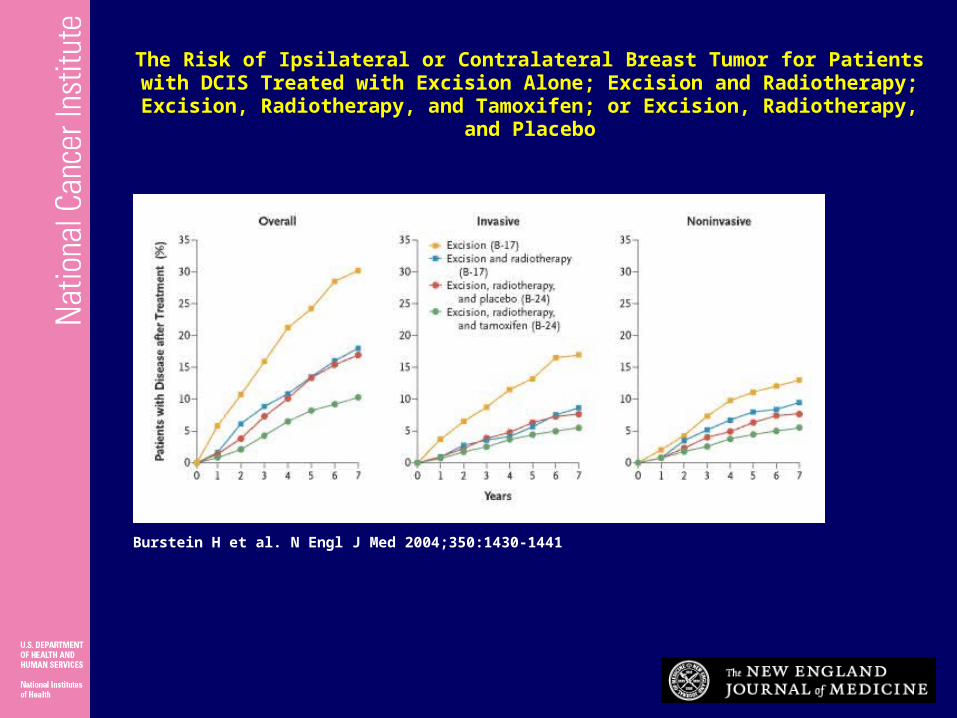
Burstein H et al. N Engl J Med 2004;350:1430-1441
The Risk of Ipsilateral or Contralateral Breast Tumor for Patients with DCIS Treated with Excision Alone; Excision and Radiotherapy; Excision, Radiotherapy, and
Tamoxifen; or Excision, Radiotherapy, and Placebo
DCIS: Conclusions• Local therapy
– Mastectomy– Breast Conserving Surgery plus
radiotherapy• Consider omission if
– Short lifespan– Sever co-morbidities
• Systemic therapy: Tamoxifen– “Prevention” intervention– Consider individual risk/benefits

What about lymph nodes?
• Axillary lymph node involvement is <1% therefore axillary lymph node dissection is not recommended
• Sentinel lymph node biopsy?– Not recommended due to low risk of
disease unless performing a mastectomy (in the chance that invasive disease is found)
– Consider: extensive high grade DCIS or palpable mass (increased chance of invasive disease being found)

Potential Benefits
• SLNB at time of definitive surgery avoids 2nd operation in 2-21 % of patients who have IDC at definitive surgery
• May identify subset of patients who would benefit from systemic therapy
Risks of SLNB in DCIS
• Increase anxiety: curable prognosis to one that is life-threatening
• SLNB risks– infection, bleeding, seroma,
paresthesias, anaphylaxis, lymphedema (3%)
• Risks of full ALND in up to 13%• Risks of systemic chemotherapy ?• Public health costs
Mammography is the current standard for detection of DCIS,
MRI could help improve the ability to diagnose DCIS, especially in
high-grade DCIS

DCIS: Calcifications Cannot be diagnosed as non-invasive with
cytology
Irregular clusters
Branching (comedo)
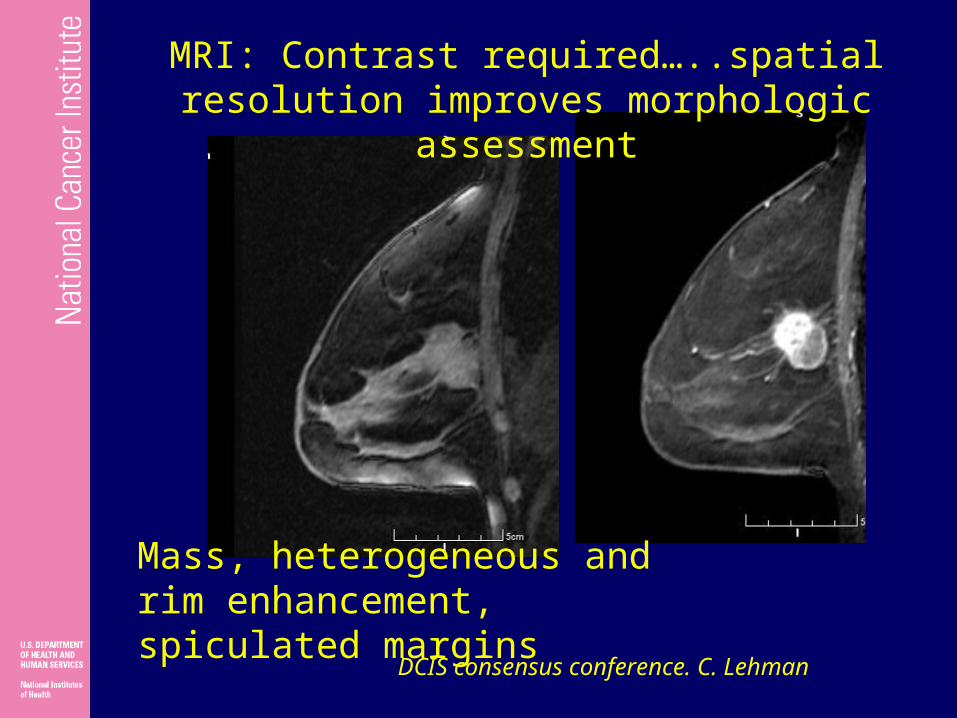
Mass, heterogeneous and rim enhancement, spiculated margins
MRI: Contrast required…..spatial resolution improves morphologic assessment
DCIS consensus conference. C. Lehman

DCIS diagnosed in high risk patient on screening MRI with negative screening mammogram
Fine linear, branching NMLE in ductal distribution
DCIS consensus conference. C. Lehman
ACR-ASS-CAP-SSO 2006 practice guideline
• The role of other image modalities, especially MRI, has yet to be established in DCIS.
• Berg found that MRI was more sensitive than mammography and sonography in detecting DCIS; however, disease extent was overestimated in 50% of involved breasts.
• The impact of MRI on clinical outcomes such as local recurrence in the preserved breast remains to be demonstrated.

KEY QUESTIONS FOR THE MANAGEMENT OF DCIS
Answers 1. Is there a subgroup of patients for which the risk of local recurrence is low enough that the risk/benefit ratio warrants omission of radiation? Probably 2. If so, can one identify reproducibly and prospectively that subgroup of patients for treatment with excision alone (without radiation)? No 3. After lumpectomy, should (almost) all patients receive maximal treatment to reduce the risk of local recurrence? - Radiation Yes - Tamoxifen, if ER/PR positive Yes
Courtesy of L. Solin 2010