dysmorphic neuromuscular junctions associated with motor ability in cerebral palsy
TRANSCRIPT

ABSTRACT: Cerebral palsy (CP) is the most prevalent neurologic diseasein children and a leading cause of severe physical disability. Research andclinical experience indicate that children with CP have abnormal neuromus-cular junctions (NMJs), and we present evidence that nonapposition ofneuromuscular junction components is associated with the severity of motorsystem deficit in CP. Leg muscle biopsies collected from ambulatory (n �21) or nonambulatory (n � 38) CP patients were stained in order to detectacetylcholine receptor (AChR) and acetylcholine esterase (AChE). Imageanalysis was used to calculate the extra-AChE spread (EAS) of AChRstaining to estimate the amount of AChR occurring outside the functional,AChE-delimited NMJ. Nonambulatory children exhibited higher averageEAS (P � 0.025) and had a greater proportion of their NMJs with signifi-cantly elevated EAS (P � 0.023) than ambulatory children. These resultsindicate that physical disability in children with CP is associated with struc-turally dysmorphic NMJs, which has important implications for the manage-ment of CP patients, especially during surgery and anesthesia.
Muscle Nerve 32: 626–632, 2005
DYSMORPHIC NEUROMUSCULAR JUNCTIONSASSOCIATED WITH MOTOR ABILITYIN CEREBRAL PALSY
MARY C. THEROUX, MD,1,2 KARYN G. OBERMAN, BA,1,3 JUSTINE LAHAYE, MS,1,4
BOBBIE A. BOYCE,1 DAVID DUHADAWAY, BS,1
FREEMAN MILLER, MD,5 and ROBERT E. AKINS, PhD1
1 Nemours Biomedical Research, A. I. duPont Hospital for Children, 1600 Rockland Road,Wilmington, Delaware 19803, USA2 Department of Anesthesiology and Critical Care, A. I. duPont Hospital for Children,Wilmington, Delaware, USA3 Department of Biological Sciences, University of Delaware, Newark, Delaware, USA4 Physiology and Informatics Program, University of Poitiers, Poitiers, France5 Department of Orthopaedics, A. I. duPont Hospital for Children, Wilmington,Delaware, USA
Accepted 25 May 2005
Previous studies suggest that children with cerebralpalsy (CP) have abnormal neuromuscular junctions(NMJs). Distribution of acetylcholine receptors(AChRs) at abnormal NMJs is clinically important asthe depolarization–repolarization characteristics ofthe muscle membrane may be affected by extrajunc-tional AChR. This is especially significant when neu-romuscular blocking agents (NMBAs) are used dur-ing anesthesia, as dangerous quantities of potassiummay be released into the extracellular fluid.9,10,29,30 It
has been shown that patients with CP have increasedsensitivity to the depolarizing NMBA succinylcho-line27 and increased resistance to the nondepolariz-ing NMBA vecuronium,11 but these results provideonly indirect support for the existence of abnormalNMJs. More recently, laboratory-based assessmentsof NMJs in erector spinae collected from childrenduring spinal fusion surgery gave direct evidencethat children with CP have dysmorphic NMJs.28 Inparticular, bungarotoxin (BTX)–labeled AChRstaining extended significantly beyond the func-tional NMJ as delimited by junctional acetylcholineesterase (AChE) immunoreactivity in CP patients,whereas AChE completely overlapped AChR stain-ing in samples from children with idiopathic scolio-sis.28
The presence of disorganized NMJs in childrenwith nonprogressive central nervous system lesionslike those found in CP is unexpected. The establish-ment and maintenance of NMJ organization has
Abbreviations: AChE, acetylcholine esterase; AChR, acetylcholine receptor;BTX, bungarotoxin; CP, cerebral palsy; EAS, extra AChE spread; GMFM,gross motor function measure; MAS, modified Ashworth score; NMBA, neu-romuscular blocking agent; NMJ, neuromuscular junction; PBS, phosphate-buffered saline.Key words: acetylcholine esterase; acetylcholine receptor; gross motorfunction measure; hyperkalemia; neuromuscular blocking agents; spasticityCorrespondence to: R. E. Akins; e-mail: [email protected]
© 2005 Wiley Periodicals, Inc.Published online 15 July 2005 in Wiley InterScience (www.interscience.wiley.com). DOI 10.1002/mus.20401
626 Neuromuscular Junctions in CP MUSCLE & NERVE November 2005

been well studied, and the colocalization of junc-tional components in NMJs is highly controlled.13,15
The nonapposition of AChR and AChE in CP there-fore suggests a fundamental dysregulation of nerve–muscle interactions or a lack of NMJ maturationassociated with the disease. An improved under-standing of AChR localization and the organizationof NMJ components in CP is needed to assure safeand adequate anesthesia, to define further the man-ifestations of CP, and to improve understanding ofpotential alterations in nerve–muscle interactions as-sociated with disease state. Of interest in this regardis whether the nonapposition of NMJ components isfunctionally related to the level of motor systemimpairment.
In this study, we examined the relationship be-tween the degree of motor system involvement in CPand the nonapposition of AChR and AChE. Wetested the hypothesis that the degree of AChR ex-pansion beyond the limits of the functional NMJincreases with disease severity. Motor system func-tion of CP children was estimated based on theability to ambulate without assistance and on GrossMotor Function Measure (GMFM). A digital imagingalgorithm was used to quantify the degree of AChR–AChE nonapposition.
MATERIALS AND METHODS
Patient Selection and Sample Acquisition. We en-rolled 59 CP patients in the study after obtaininginstitutional review board approval and signed in-formed consent. Signed assents were obtained whereappropriate. Patients were 2–20 years of age, hadspastic quadriplegic CP, and were scheduled to un-dergo muscle and tendon release surgery. Duringsurgery, muscle biopsies were obtained from gracilis,vastus lateralis, or gastrocnemius, depending on theexposure of muscles during the procedure. Sampleswere immediately snap frozen in N2(l)-chilled iso-pentane.
Preoperative Assessment of Patient. Prior to sur-gery, patients were assessed for their ability to beartheir own weight in a standing position without as-sistance. Experienced physiotherapists performedthis evaluation during a routine appointment beforethe day of surgery, and the results of the evaluationwere collected from patient charts. Those patientsthat could bear their own weight were classified asambulatory (n � 21) and those that could not wereclassified as nonambulatory (n � 38). Patients whodid not have their ambulatory status evaluated priorto surgery were excluded from the study. In addi-
tion, GMFM Section D scores were determined for51 patients (15 ambulatory and 36 nonambulatory)in a separate visit to our institutional Gait Labora-tory. The GMFM Section D score is a quantitativemeasure of motor ability associated with standing. Itincludes 13 separate assessments graded from 0 (nopart of the task was accomplished) to 3 (the task wascompleted); the total score is used to assess the levelof motor function. The GMFM has been vali-dated.21,25 It is predictive of the ambulatory status ofchildren with CP3,20 and correlates with CP sever-ity.19,21 Patients were also graded using the modifiedAshworth scale (MAS) to estimate spasticity.2 MASwas determined for 66 muscle groups (24 ankle plan-tar flexion, 22 hip adduction, 10 knee extension) in39 patients (15 ambulatory, 24 nonambulatory). TheMAS ranges from 0 to 5 and was assigned by aphysiotherapist based on the resistance to passivestretch within a particular muscle group.
Histological Assessment of Samples. To evaluate thepresence of AChRs outside functional NMJs, a pre-viously developed double-stain method to visualizeAChR and AChE was employed.28 This allowed thedirect determination of AChR–AChE nonappositionwithin histologic sections. AChE was chosen becauseof its well-characterized distribution pattern and itslocalization to the functional NMJ.13,16,23,24
Slides containing 8-�m-thick cryosections werefixed at room temperature for 5 min using 10%neutral-buffered formalin (Fisher, Fairlawn, New Jer-sey) and blocked at room temperature for 30 minusing 3% bovine serum albumin (Sigma, St. Louis,Missouri). Sections were rinsed with Dulbecco’sphosphate-buffered saline (PBS; Invitrogen, Carls-bad, California) and stained in a solution contain-ing 0.16 �g/ml tetramethylrhodamine-conjugated�-BTX (Molecular Probes, Eugene, Oregon). After1-h incubation at room temperature, the sectionswere rinsed with PBS and stained using a monoclo-nal antibody to AChE (AE-2; Biogenesis, Sansdown,New Hampshire) diluted 1:150 in PBS, followed by afluorescein-conjugated secondary antibody (JacksonLabs, Westchester, Pennsylvania). Samples wereviewed and digitally photographed on an OlympusBX-60 fluorescence microscope (Olympus, Tokyo,Japan) equipped with a Spot RT-Slider digital cam-era (Diagnostic Instruments, Sterling Heights, Mich-igan). Corrected lenses were used to minimizechromatic aberration, and the registration of fluo-rescence images was routinely verified using test im-ages. The distribution of AChR relative to AChE wasquantified using Image Pro software (Media Cyber-netics, Silver Spring, Maryland) and a customized
Neuromuscular Junctions in CP MUSCLE & NERVE November 2005 627
software macro. The value extra-AChE spread (EAS)was calculated as the fraction of pixels in digitizedimages exhibiting AChR but no AChE staining.
Statistical Analysis. The inter-rater reliability of thedigital image analysis was determined using paralleldeterminations carried out by blinded research as-sistants. To test whether EAS was related to ambula-tory status, a median value was determined for eachchild and ambulatory and nonambulatory groupswere compared using a Mann–Whitney test. Effectsize was estimated using Cohen’s d calculation: effectsize � (mean difference)/(pooled SD).5 The rela-tionship between GMFM score and EAS was evalu-ated using Pearson’s correlation. The relationshipbetween MAS and EAS values was evaluated usingSpearman’s correlation. All statistical analyses werecarried out using SPSS for Windows (SPSS, Chicago,Illinois).
RESULTS
Validation of Methodology and Determination of Normal
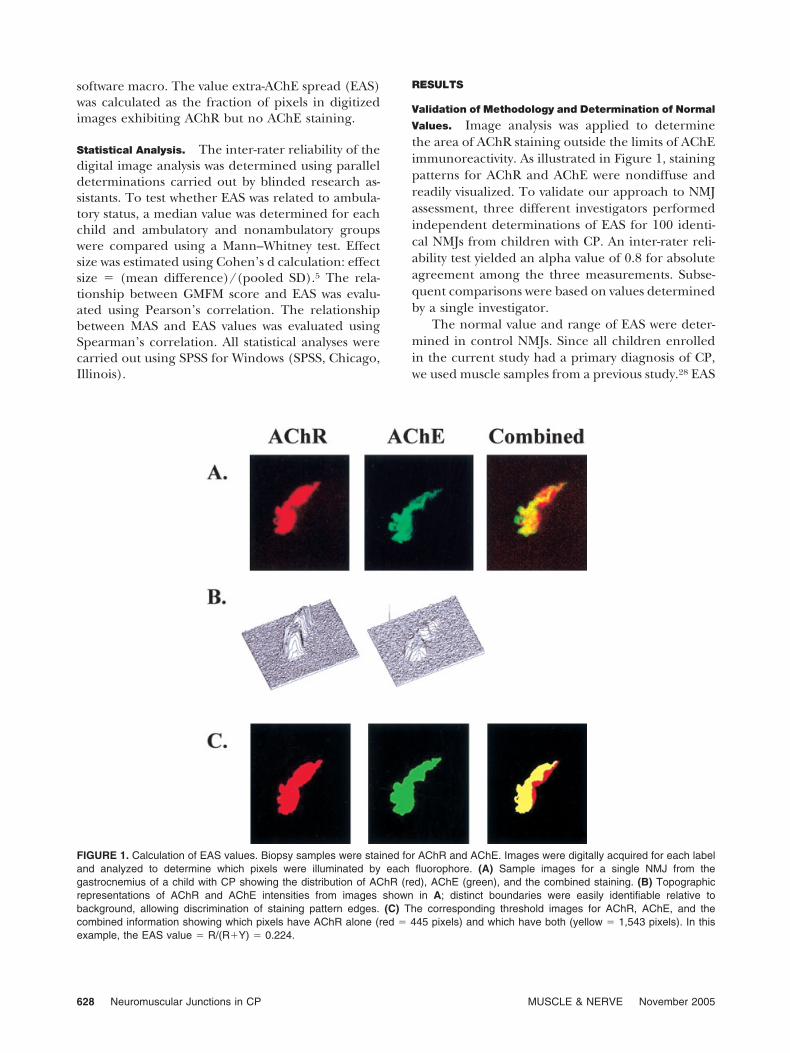
Values. Image analysis was applied to determinethe area of AChR staining outside the limits of AChEimmunoreactivity. As illustrated in Figure 1, stainingpatterns for AChR and AChE were nondiffuse andreadily visualized. To validate our approach to NMJassessment, three different investigators performedindependent determinations of EAS for 100 identi-cal NMJs from children with CP. An inter-rater reli-ability test yielded an alpha value of 0.8 for absoluteagreement among the three measurements. Subse-quent comparisons were based on values determinedby a single investigator.
The normal value and range of EAS were deter-mined in control NMJs. Since all children enrolledin the current study had a primary diagnosis of CP,we used muscle samples from a previous study.28 EAS
FIGURE 1. Calculation of EAS values. Biopsy samples were stained for AChR and AChE. Images were digitally acquired for each labeland analyzed to determine which pixels were illuminated by each fluorophore. (A) Sample images for a single NMJ from thegastrocnemius of a child with CP showing the distribution of AChR (red), AChE (green), and the combined staining. (B) Topographicrepresentations of AChR and AChE intensities from images shown in A; distinct boundaries were easily identifiable relative tobackground, allowing discrimination of staining pattern edges. (C) The corresponding threshold images for AChR, AChE, and thecombined information showing which pixels have AChR alone (red � 445 pixels) and which have both (yellow � 1,543 pixels). In thisexample, the EAS value � R/(R�Y) � 0.224.
628 Neuromuscular Junctions in CP MUSCLE & NERVE November 2005

was significantly lower in the erector spinae of chil-dren with idiopathic scoliosis (0.07 � 0.04; n � 26)than in children with CP (0.28 � 0.04; n � 7).
Assessment of Variability between Groups. Patientsin the ambulatory and nonambulatory groups werematched for age (8.1 � 5.2 and 8.2 � 4.4 years,respectively) and weight (24.7 � 14.0 and 19.7 � 9.1kg). There were no significant differences in theseparameters (P � 0.1; Student’s t-test). In addition,there was no correlation between EAS and age orweight (P � 0.8; Spearman’s correlation) for eithergroup.
Analysis of NMJ Components. Abnormal NMJs coex-isted in the same histological sections as normalNMJs (Fig. 2) in both ambulatory and nonambula-tory groups. Comparison of EAS values between thethree muscle types collected indicated no significantdifference in either patient group (P � 0.5 byKruskal–Wallis test), and the data obtained from allmuscles collected from an individual child werepooled for analysis. Descriptive statistics are summa-rized in Table 1.
EAS differed between the ambulatory andnonambulatory groups (P � 0.025 by Mann–Whit-
FIGURE 2. Nonapposed NMJs occur in the same region as apposed NMJs. Biopsy samples were stained for AChR and AChE, andimages were acquired separately for each label. Images were analyzed to determine which pixels were illuminated for each label. (A)Cross section of gracilis from a child with CP showing normal and abnormal NMJ distributions in the same anatomic location and in thesame histologic section. Examples of normal and abnormal NMJs are denoted by a square and a circle. (B) Higher magnification viewof normal NMJ from A, showing that AChE signal overlapped the AChR signal. (C) Higher magnification view of abnormal NMJ from A,showing AChR–AChE nonapposition.
Neuromuscular Junctions in CP MUSCLE & NERVE November 2005 629

ney test), with nonambulatory patients havinghigher EAS values. The mean EAS values for ambu-latory (0.16 � 0.08) and nonambulatory (0.23 �0.14) patients were each more than two standarddeviations above the mean EAS of normal NMJs(0.07 � 0.04) with the difference between groupsindicating a medium effect size (d � 0.54). Therewas also a significant correlation (R � �0.056; P �0.005) between EAS values and GMFM Section Dscore. There was no correlation between EAS andMAS (R � .028; P � 0.8; n � 66).
The prevalence of abnormal NMJs versus normalNMJs was also determined. On average, nonambula-tory CP patients had 45% of their NMJs with EASexceeding 2 standard deviations above normal (i.e.,EAS � 0.15) compared to ambulatory patients whohad 34% of their NMJs with EAS values that high.This was statistically significant (P � 0.023) byMann–Whitney test. The post-junctional area ofNMJs, as estimated by the number of pixels presentin BTX-stained images, was found to be about 10%smaller in nonambulatory than ambulatory children(P � 0.001).
DISCUSSION
We found that differences in NMJ structure exist inCP patients such that there is a greater degree ofNMJ nonapposition present in more highly affectedpatients. The analytical approach to estimate NMJnonapposition was based on the detection of AChRin the absence of corresponding AChE within digi-tized images. This approach may underestimate trueEAS since each digital image element comprisedoptical information from a full thickness (8 �m) ofthe histological section examined. Thus, AChR–
AChE mismatches along the z-axis would have beenoverlooked. Confocal microscopy or image deconvo-lution may have provided more accurate estimates ofEAS, but the reported approach allowed us to eval-uate a much larger number of tissue sections thanwould have been possible otherwise. The underlyingdifferences between ambulatory and nonambulatorypatients were substantial, and significant differenceswere found without the application of more involvedtechniques.
Patients with CP exhibit poor voluntary musclecontrol and decreased functional motor capability.These were estimated using the GMFM. GMFM Sec-tion D scores range from 0 to 39 and were consid-ered continuous variables. Pearson’s correlation wasapplied to compare EAS with motor function. Al-though there was a strong correlation betweenGMFM and EAS, there was little predictive value tothe relationship. GMFM scores tended to cluster intotwo groups (Table 1) with a large number of zerovalues present in the more highly affected patients.These GMFM clusters matched the independentlydetermined values for ambulatory status. Ambula-tory status was used as the principal grouping foranalysis. Our results indicate an association betweenAChR–AChE nonapposition and the degree of vol-untary motor function, with nonambulators havinghigher EAS values and a greater proportion of highlyabnormal NMJs than ambulators.
Spasticity is another characteristic feature of CPin which hyperexcitability of the stretch reflex resultsin increased motor neuron activity.12 Since motorneuron activity has been associated with AChR ex-pression and NMJ size,17,31 we suspected that CP-associated differences in NMJs were related to the
Table 1. Descriptive statistics for ambulatory and nonambulatory patients.*
Parameter Ambulatory Nonambulatory
No. of patients 21 38Mean GMFM Section D score† 23.0 � 13.1 (15) 2.2 � 7.3 (36)Mean EAS†‡ 0.16 � 0.08 (21) 0.23 � 0.14 (38)Percentage of NMJs with EAS � normal† 34 45No. of NMJs assessed 853 2,060No. of pixels per NMJ image† 1,142 � 657 (853) 1,026 � 626 (2,060)Mean EAS of NMJs in vastus§ 0.17 � 0.22 (45) 0.22 � 0.24 (352)Mean EAS of NMJs in gracilis§ 0.17 � 0.21 (319) 0.20 � 0.22 (1,120)Mean EAS of NMJs in gastrocnemius§ 0.15 � 0.18 (489) 0.22 � 0.25 (588)
EAS, extra acetylcholine esterase spread; GMFM, gross motor function measure; NMJ, neuromuscular junction.*Data presented as mean value � SD; numbers in parentheses indicate the number of determinations for each measurement.†Statistically significant comparisons (P � 0.05). Statistical comparisons between groups were carried out using parametric or nonparametric approaches asappropriate for the type of data (see text).‡Each child received an EAS score equivalent to the arithmetic average for all junctions assessed within that child. The mean and standard deviation of thesescores are reported.§EAS values did not vary by muscle type.
630 Neuromuscular Junctions in CP MUSCLE & NERVE November 2005

degree of spasticity. Surprisingly, no correlation wasfound between MAS and EAS, indicating that non-apposition of NMJ components may result frommechanisms that are independent of reflex musclecontrol. The MAS, however, does not distinguisheffectively heightened stretch reflex from increasedintrinsic stiffness,7 and in some cases it may notaccurately indicate spasticity per se, especially in thelower extremities.1,6 Thus, although it would be in-triguing to speculate that NMJ distortion in CP isassociated with voluntary muscle control but inde-pendent of reflex muscle control, such a conclusioncannot be made without improved means to assessspasticity.
The two groups of children in our study haddifferent levels of mobility, and certain types of im-mobilization can lead to NMJ disruption. Generally,immobilization implies decreased NMJ activationdue to disuse. Evidence suggests that gravitationalunloading increases the average size of motor end-plates in adult rats8 and that casting results in in-creased AChR expression.32 Other disease states as-sociated with decreased NMJ activation, e.g.,denervation, spinal cord injury, or burn, can alsolead to expansion of AChR staining and upregula-tion of AChR subunit expression.4,9,14,18,22,29 In-creased muscle impulse activity, by contrast, is asso-ciated with decreased NMJ size,17 and sustainedactivity inhibits �-AChR subunit expression in dener-vated muscle.31 Interestingly, because their lack ofmobility is largely due to weakness, spasticity, andloss of motor control, immobilization in CP patientsoccurs in conjunction with continuing NMJ activa-tion as opposed to the reduced NMJ activation com-monly associated with other conditions. Consistentwith this, nonambulatory (or less mobile) patientshad slightly smaller NMJs, perhaps associated withgreater spasticity, and in a previous study, the NMJsof CP patients appeared smaller than those of con-trols with no evidence for �-AChR expression.28
Thus, the pathways contributing to NMJ deforma-tion in CP may be unrelated to patient mobility anddistinct from those previously described for otherdiseases associated with disuse.
Our study has implications for the managementof CP patients, especially during surgery and anes-thesia. The increased oral secretions and gastro-esophageal reflux in children with CP26 often renderthe use of a rapidly acting NMBA, such as succinyl-choline, attractive in securing the airway during an-esthetic management. Given the NMJ abnormalitiesand known sensitivities of CP patients, however, an-esthesiologists should exercise caution in the use ofsuccinylcholine in patients with CP. Conversely, it is
important to be aware of the decreased potency ofnondepolarizing NMBAs in patients with disruptedNMJs because inadequate relaxation could result inprocedural difficulties during surgery. Our studyalso suggests that treatments, therapies, and diagnos-tics aimed at NMJs may be of benefit to CP patients,but further elucidation of the mechanisms andpathophysiology associated with NMJ disruption andAChR–AChE nonapposition is needed.
This research was presented in part to the Pediatric AcademicSociety, May 2004, San Francisco, California, and to the Societyfor Neuroscience, October 2004, San Diego, California. This workwas supported in part by NAG9-1339 from the Office of Biologicaland Physical Research at NASA, by 1P20-RR020173-01 from theNational Center for Research Resources at NIH, and by AI2003-026 from the Nemours Foundation. The authors thank KellyQuaile, Nancy Lennon, Lauren Kirstetter, Anusha Gopalrathnam,and Funbi Fagbami for their assistance with the preoperativeevaluation of patients and the validation of the image analysismethod.
REFERENCES
1. Avery LM, Russell DJ, Raina PS, Walter SD, Rosenbaum PL.Rasch analysis of the Gross Motor Function Measure: validat-ing the assumptions of the Rasch model to create an interval-level measure. Arch Phys Med Rehabil 2003;84:697–705.
2. Bohannon RW, Smith MB. Interrater reliability of a modifiedAshworth scale of muscle spasticity. Phys Ther 1987;67:206–207.
3. Boyce W, Gowland C, Rosenbaum P, Lane M, Plews N, Gold-smith C, et al. Gross motor performance measure for childrenwith cerebral palsy: study design and preliminary findings.Can J Public Health 1992;83(Suppl 2):S34–S40.
4. Carter JG, Sokoll MD, Gergis SD. Effect of spinal cord tran-section on neuromuscular function in the rat. Anesthesiology1981;55:542–546.
5. Cohen J. Statistical power analysis for the behavioral sciences.Hillsdale, NJ: Earlbaum; 1988. 567 p.
6. Damiano DL, Abel MF. Relation of gait analysis to gross motorfunction in cerebral palsy. Dev Med Child Neurol 1996;38:389–396.
7. Damiano DL, Quinlivan JM, Owen BF, Payne P, Nelson KC,Abel MF. What does the Ashworth scale really measure andare instrumented measures more valid and precise? Dev MedChild Neurol 2002;44:112–118.
8. Deschenes MR, Britt AA, Gomes RR, Booth FW, Gordon SE.Recovery of neuromuscular junction morphology following16 days of spaceflight. Synapse 2001;42:177–184.
9. Gronert GA, Theye RA. Pathophysiology of hyperkalemiainduced by succinylcholine. Anesthesiology 1975;43:89–99.
10. Gronert GA. Cardiac arrest after succinylcholine: mortalitygreater with rhabdomyolysis than receptor upregulation. An-esthesiology 2001;94:523–529.
11. Hepaguslar H, Ozzeybek D, Elar Z. The effect of cerebralpalsy on the action of vecuronium with or without anticon-vulsants. Anaesthesia 1999;54:593–596.
12. Hinderer SR, Dixon K. Physiologic and clinical monitoring ofspastic hypertonia. Phys Med Rehabil Clin N Am 2001;12:733–746.
13. Kummer TT, Misgeld T, Lichtman JW, Sanes JR. Nerve-inde-pendent formation of a topologically complex postsynapticapparatus. J Cell Biol 2004;164:1077–1087.
14. Levitt-Gilmour TA, Salpeter MM. Gradient of extrajunctionalacetylcholine receptors early after denervation of mammalianmuscle. J Neurosci 1986;6:1606–1612.
Neuromuscular Junctions in CP MUSCLE & NERVE November 2005 631

15. Lin W, Burgess RW, Dominguez B, Pfaff SL, Sanes JR, Lee KF.Distinct roles of nerve and muscle in postsynaptic differenti-ation of the neuromuscular synapse. Nature 2001;410:1057–1064.
16. Lomo T, Slater CR. Control of junctional acetylcholinesteraseby neural and muscular influences in the rat. J Physiol (Lond)1980;303:191–202.
17. Lomo T. What controls the position, number, size, and dis-tribution of neuromuscular junctions on rat muscle fibers?J Neurocytol 2003;32:835–848.
18. Martyn JA, White DA, Gronert GA, Jaffe RS, Ward JM. Up-and-down regulation of skeletal muscle acetylcholine recep-tors. Effects on neuromuscular blockers. Anesthesiology 1992;76:822–843.
19. Oeffinger DJ, Tylkowski CM, Rayens MK, Davis RF, GortonGE III, D’Astous J, et al. Gross Motor Function ClassificationSystem and outcome tools for assessing ambulatory cerebralpalsy: a multicenter study. Dev Med Child Neurol 2004;46:311–319.
20. Ostensjo S, Carlberg EB, Vollestad NK. Motor impairments inyoung children with cerebral palsy: relationship to gross mo-tor function and everyday activities. Dev Med Child Neurol2004;46:580–589.
21. Palisano RJ, Hanna SE, Rosenbaum PL, Russell DJ, Walter SD,Wood EP, et al. Validation of a model of gross motor functionfor children with cerebral palsy. Phys Ther 2000;80:974–985.
22. Ringel SP, Bender AN, Engel WK. Extrajunctional acetylcho-line receptors. Alterations in human and experimental neu-romuscular diseases. Arch Neurol 1976;33:751–758.
23. Rotundo RL. Expression and localization of acetylcholinest-erase at the neuromuscular junction. J Neurocytol 2003;32:743–766.
24. Rubin LL, Schuetze SM, Weill CL, Fischbach GD. Regulationof acetylcholinesterase appearance at neuromuscular junc-tions in vitro. Nature 1980;283:264–267.
25. Russell DJ, Avery LM, Rosenbaum PL, Raina PS, Walter SD,Palisano RJ. Improved scaling of the gross motor functionmeasure for children with cerebral palsy: evidence of reliabil-ity and validity. Phys Ther 2000;80:873–885.
26. Spiroglou K, Xinias I, Karatzas N, Karatza E, Arsos G, Pante-liadis C. Gastric emptying in children with cerebral palsy andgastroesophageal reflux. Pediatr Neurol 2004;31:177–182.
27. Theroux MC, Brandom BW, Zagnoev M, Kettrick RG, MillerF, Ponce C. Dose response of succinylcholine at the adductorpollicis of children with cerebral palsy during propofol andnitrous oxide anesthesia. Anesth Analg 1994;79:761–765.
28. Theroux MC, Akins RE, Barone C, Boyce B, Miller F, DabneyK. Neuromuscular junctions in cerebral palsy. Presence ofextrajunctional acetylcholine receptors. Anesthesiology 2002;96:330–335.
29. Tobey RE. Paraplegia, succinylcholine and cardiac arrest.Anesthesiology 1970;32:359–364.
30. Tobey RE, Jacobsen PM, Kahle CT, Clubb RJ, Dean MA. Theserum potassium response to muscle relaxants in neural in-jury. Anesthesiology 1972;37:332–337.
31. Witzemann V, Brenner HR, Sakmann B. Neural factors reg-ulate AChR subunit mRNAs at rat neuromuscular synapses.J Cell Biol 1991;114:125–141.
32. Yanez P, Martyn JA. Prolonged d-tubocurarine infusionand/or immobilization cause upregulation of acetylcholinereceptors and hyperkalemia to succinylcholine in rats. Anes-thesiology 1996;84:384–391.
632 Neuromuscular Junctions in CP MUSCLE & NERVE November 2005