early implant placement for a patient with ectodermal ... · teeth are complicating factors that...
TRANSCRIPT
CLINICAL REPORT
aProfessor, DbProfessor, DcAssistant PrdGraduate stu
702
Early implant placement for a patient with ectodermaldysplasia: Thirteen years of clinical care
Lisa A. Knobloch, DDS, MS,a Peter E. Larsen, DDS, MS,b Paola C. Saponaro, DDS, MS,c andEmilie L’Homme-Langlois, DMD, MSc, FRCD(c)d
ABSTRACTPatients with ectodermal dysplasia have abnormalities of 2 or more structures that originate fromthe ectoderm. The oral manifestations often include the congenital absence of teeth and mal-formed teeth. This clinical report describes the interdisciplinary care from childhood through thedefinitive dental rehabilitation completed at skeletal maturation to replace the missing teeth in apatient with ectodermal dysplasia. Treatment began at 9 years of age with an implant-assistedmandibular overdenture to improve function and replace the missing mandibular teeth. Ortho-dontic treatment for the consolidation of space, composite resin restorations, and interim remov-able dental prostheses were provided to improve esthetics and replace the missing maxillary teeth.Skeletal growth was monitored, and orthognathic surgery was performed at the cessation ofgrowth. The definitive rehabilitation consisted of a mandibular fixed dental prosthesis supported bydental implants and a maxillary removable dental prosthesis to restore the patient to esthetics andfunction. (J Prosthet Dent 2018;119:702-9)
Ectodermal dysplasia is a geneticdisorder that is usually trans-mitted as an X-linked recessivetrait.1-3 Ninety-five percent of pa-tients with ectodermal dysplasiahave the X-linked form.3 It is arare disorder that can affect thedevelopment of the teeth, hair,nails, and sweat glands.1-3 Thediagnosis of ectodermal dysplasiais often difficult to make in thefirst 2 years because the mani-festations are difficult to detect.3
Missing teeth are often an important part of the diag-nostic process. Dental manifestations of hypohidroticectodermal dysplasia include hypodontia, anodontia, andmalformed teeth.1-3 In the absence of teeth, the alveolarridge is compromised, making a removable prosthesisdifficult to wear.4 In addition, patients with hypohidroticectodermal dysplasia often begin wearing a removableprosthesis as young as 3 years of age.5 These patients canexperience difficulties with stability and retention of theremovable prostheses because of the compromised alve-olar ridge. Endosseous implants can improve the retentionof the removable prostheses; however, the acceptedstandard regarding the timing of implant placement is thatplacement should be delayed until the cessation ofgrowth.6-13 Severe situations of patients with ectodermaldysplasia have been reported as exceptions to this treat-ment guideline.5,7,9,14-17 In addition, the placement of
ivision of Restorative Science and Prosthodontics, The Ohio State Universivision of Oral and Maxillofacial Surgery, The Ohio State University Collegeofessor, Division of Restorative Science and Prosthodontics, The Ohio Statdent, Advanced Prosthodontics, The Ohio State University College of Den
Downloaded for scmh lib ([email protected]) at Show Chwan MemorFor personal use only. No other uses without permission.
implants helps maintain alveolar bone.18-22 Early treat-ments with dental implants can be considered whenpositive outcomes can improve the quality of life. If implantplacement is planned, the potential complications must bediscussedwith the parents, who should also know that theadvantages outweigh the risks.
Treatment of the dental manifestations of a patientwith ectodermal dysplasia often begins at a young age.Not only is treatment often initiated at a young age butalso managing care throughout the various transitions ofdental development can be challenging. The objective oftreatment is to improve function and esthetics; however,compromised alveolar development, the number ofmissing teeth, and the shape and position of the existingteeth are complicating factors that make the transitions ofgrowth difficult to manage. Treatment requires a multi-disciplinary team approach. A multidisciplinary team of
ity College of Dentistry, Columbus, Ohio.of Dentistry, Columbus, Ohio.e University College of Dentistry, Columbus, Ohio.tistry, Columbus, Ohio; and Private practice, Montreal, Quebec, Canada.
THE JOURNAL OF PROSTHETIC DENTISTRY
ial Hospital JC from ClinicalKey.com by Elsevier on June 04, 2018. Copyright ©2018. Elsevier Inc. All rights reserved.
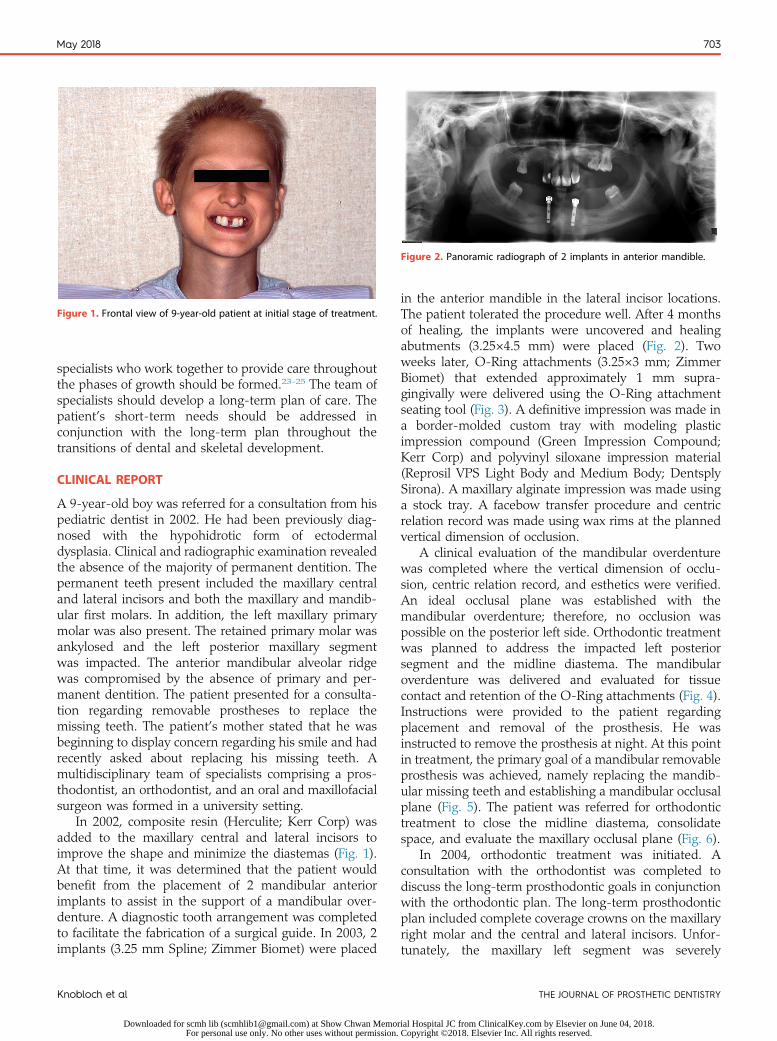
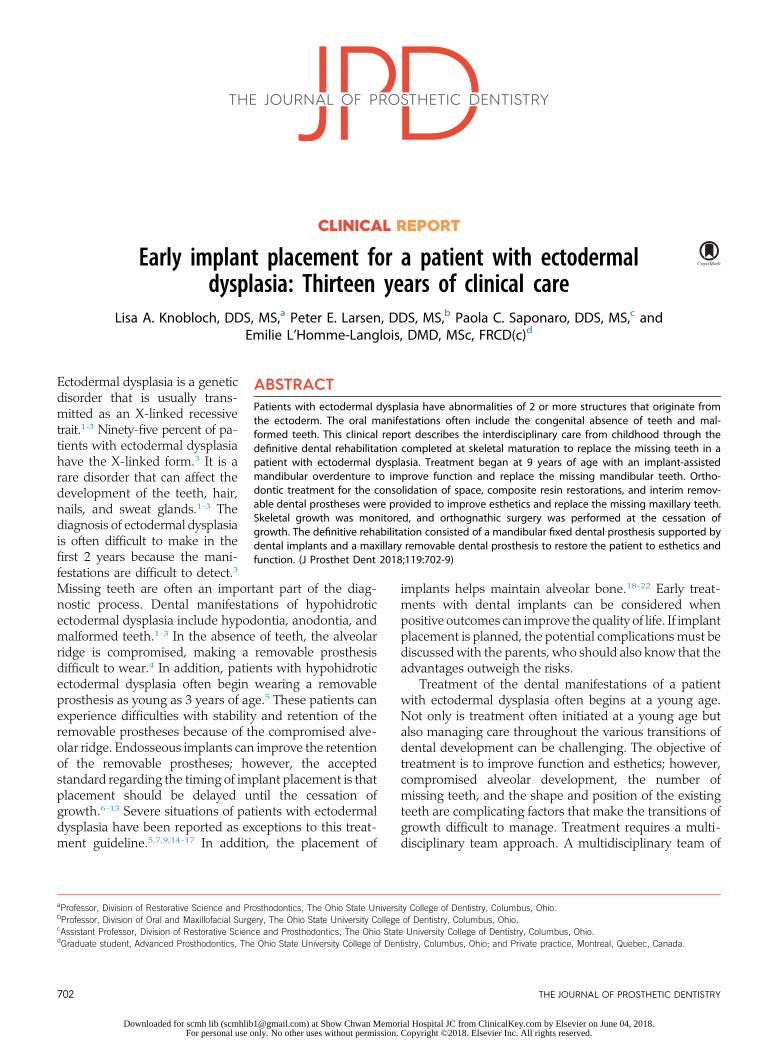
Figure 1. Frontal view of 9-year-old patient at initial stage of treatment.
Figure 2. Panoramic radiograph of 2 implants in anterior mandible.
May 2018 703
specialists who work together to provide care throughoutthe phases of growth should be formed.23-25 The team ofspecialists should develop a long-term plan of care. Thepatient’s short-term needs should be addressed inconjunction with the long-term plan throughout thetransitions of dental and skeletal development.
CLINICAL REPORT
A 9-year-old boy was referred for a consultation from hispediatric dentist in 2002. He had been previously diag-nosed with the hypohidrotic form of ectodermaldysplasia. Clinical and radiographic examination revealedthe absence of the majority of permanent dentition. Thepermanent teeth present included the maxillary centraland lateral incisors and both the maxillary and mandib-ular first molars. In addition, the left maxillary primarymolar was also present. The retained primary molar wasankylosed and the left posterior maxillary segmentwas impacted. The anterior mandibular alveolar ridgewas compromised by the absence of primary and per-manent dentition. The patient presented for a consulta-tion regarding removable prostheses to replace themissing teeth. The patient’s mother stated that he wasbeginning to display concern regarding his smile and hadrecently asked about replacing his missing teeth. Amultidisciplinary team of specialists comprising a pros-thodontist, an orthodontist, and an oral and maxillofacialsurgeon was formed in a university setting.
In 2002, composite resin (Herculite; Kerr Corp) wasadded to the maxillary central and lateral incisors toimprove the shape and minimize the diastemas (Fig. 1).At that time, it was determined that the patient wouldbenefit from the placement of 2 mandibular anteriorimplants to assist in the support of a mandibular over-denture. A diagnostic tooth arrangement was completedto facilitate the fabrication of a surgical guide. In 2003, 2implants (3.25 mm Spline; Zimmer Biomet) were placed
Knobloch et al
Downloaded for scmh lib ([email protected]) at Show Chwan MemorFor personal use only. No other uses without permission.
in the anterior mandible in the lateral incisor locations.The patient tolerated the procedure well. After 4 monthsof healing, the implants were uncovered and healingabutments (3.25×4.5 mm) were placed (Fig. 2). Twoweeks later, O-Ring attachments (3.25×3 mm; ZimmerBiomet) that extended approximately 1 mm supra-gingivally were delivered using the O-Ring attachmentseating tool (Fig. 3). A definitive impression was made ina border-molded custom tray with modeling plasticimpression compound (Green Impression Compound;Kerr Corp) and polyvinyl siloxane impression material(Reprosil VPS Light Body and Medium Body; DentsplySirona). A maxillary alginate impression was made usinga stock tray. A facebow transfer procedure and centricrelation record was made using wax rims at the plannedvertical dimension of occlusion.
A clinical evaluation of the mandibular overdenturewas completed where the vertical dimension of occlu-sion, centric relation record, and esthetics were verified.An ideal occlusal plane was established with themandibular overdenture; therefore, no occlusion waspossible on the posterior left side. Orthodontic treatmentwas planned to address the impacted left posteriorsegment and the midline diastema. The mandibularoverdenture was delivered and evaluated for tissuecontact and retention of the O-Ring attachments (Fig. 4).Instructions were provided to the patient regardingplacement and removal of the prosthesis. He wasinstructed to remove the prosthesis at night. At this pointin treatment, the primary goal of a mandibular removableprosthesis was achieved, namely replacing the mandib-ular missing teeth and establishing a mandibular occlusalplane (Fig. 5). The patient was referred for orthodontictreatment to close the midline diastema, consolidatespace, and evaluate the maxillary occlusal plane (Fig. 6).
In 2004, orthodontic treatment was initiated. Aconsultation with the orthodontist was completed todiscuss the long-term prosthodontic goals in conjunctionwith the orthodontic plan. The long-term prosthodonticplan included complete coverage crowns on the maxillaryright molar and the central and lateral incisors. Unfor-tunately, the maxillary left segment was severely
THE JOURNAL OF PROSTHETIC DENTISTRY
ial Hospital JC from ClinicalKey.com by Elsevier on June 04, 2018. Copyright ©2018. Elsevier Inc. All rights reserved.
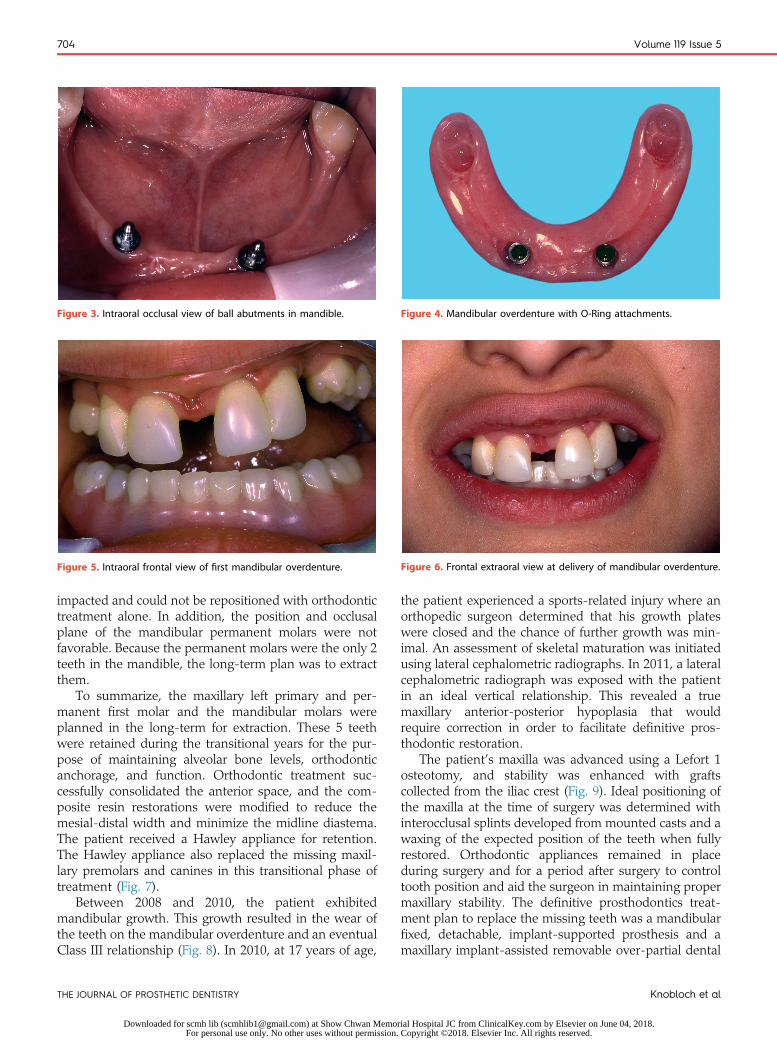
Figure 3. Intraoral occlusal view of ball abutments in mandible. Figure 4. Mandibular overdenture with O-Ring attachments.
Figure 5. Intraoral frontal view of first mandibular overdenture. Figure 6. Frontal extraoral view at delivery of mandibular overdenture.
704 Volume 119 Issue 5
impacted and could not be repositioned with orthodontictreatment alone. In addition, the position and occlusalplane of the mandibular permanent molars were notfavorable. Because the permanent molars were the only 2teeth in the mandible, the long-term plan was to extractthem.
To summarize, the maxillary left primary and per-manent first molar and the mandibular molars wereplanned in the long-term for extraction. These 5 teethwere retained during the transitional years for the pur-pose of maintaining alveolar bone levels, orthodonticanchorage, and function. Orthodontic treatment suc-cessfully consolidated the anterior space, and the com-posite resin restorations were modified to reduce themesial-distal width and minimize the midline diastema.The patient received a Hawley appliance for retention.The Hawley appliance also replaced the missing maxil-lary premolars and canines in this transitional phase oftreatment (Fig. 7).
Between 2008 and 2010, the patient exhibitedmandibular growth. This growth resulted in the wear ofthe teeth on the mandibular overdenture and an eventualClass III relationship (Fig. 8). In 2010, at 17 years of age,
THE JOURNAL OF PROSTHETIC DENTISTRY
Downloaded for scmh lib ([email protected]) at Show Chwan MemorFor personal use only. No other uses without permission.
the patient experienced a sports-related injury where anorthopedic surgeon determined that his growth plateswere closed and the chance of further growth was min-imal. An assessment of skeletal maturation was initiatedusing lateral cephalometric radiographs. In 2011, a lateralcephalometric radiograph was exposed with the patientin an ideal vertical relationship. This revealed a truemaxillary anterior-posterior hypoplasia that wouldrequire correction in order to facilitate definitive pros-thodontic restoration.
The patient’s maxilla was advanced using a Lefort 1osteotomy, and stability was enhanced with graftscollected from the iliac crest (Fig. 9). Ideal positioning ofthe maxilla at the time of surgery was determined withinterocclusal splints developed from mounted casts and awaxing of the expected position of the teeth when fullyrestored. Orthodontic appliances remained in placeduring surgery and for a period after surgery to controltooth position and aid the surgeon in maintaining propermaxillary stability. The definitive prosthodontics treat-ment plan to replace the missing teeth was a mandibularfixed, detachable, implant-supported prosthesis and amaxillary implant-assisted removable over-partial dental
Knobloch et al
ial Hospital JC from ClinicalKey.com by Elsevier on June 04, 2018. Copyright ©2018. Elsevier Inc. All rights reserved.
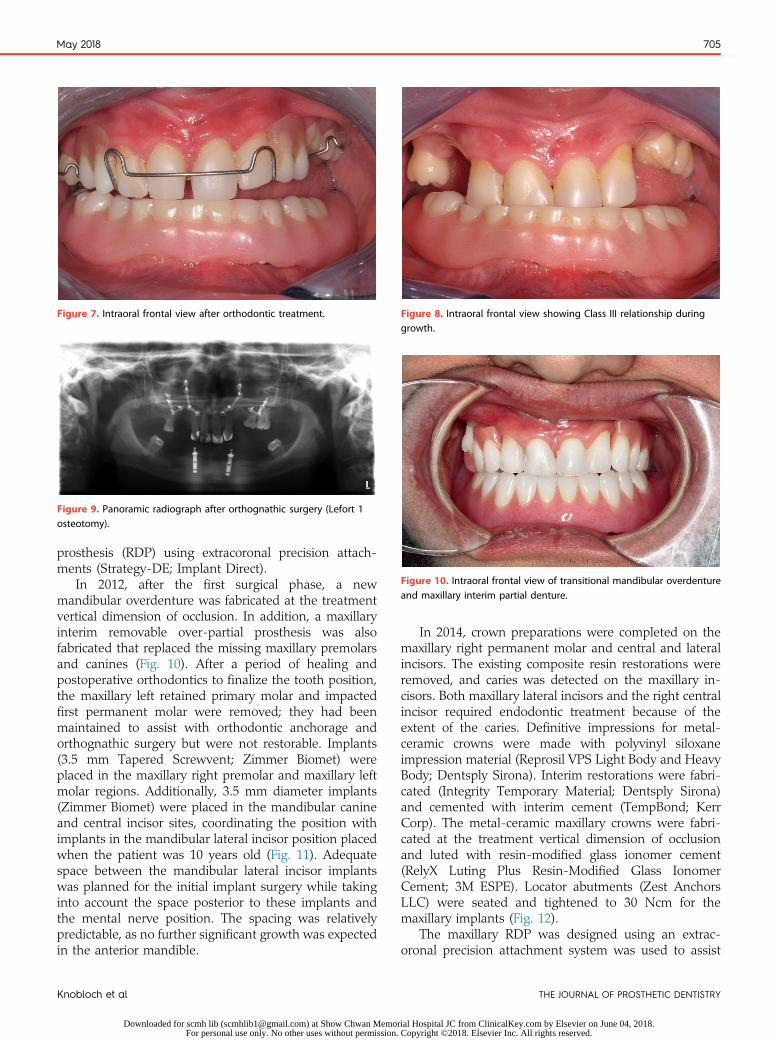
Figure 7. Intraoral frontal view after orthodontic treatment. Figure 8. Intraoral frontal view showing Class III relationship duringgrowth.
Figure 9. Panoramic radiograph after orthognathic surgery (Lefort 1osteotomy).
Figure 10. Intraoral frontal view of transitional mandibular overdentureand maxillary interim partial denture.
May 2018 705
prosthesis (RDP) using extracoronal precision attach-ments (Strategy-DE; Implant Direct).
In 2012, after the first surgical phase, a newmandibular overdenture was fabricated at the treatmentvertical dimension of occlusion. In addition, a maxillaryinterim removable over-partial prosthesis was alsofabricated that replaced the missing maxillary premolarsand canines (Fig. 10). After a period of healing andpostoperative orthodontics to finalize the tooth position,the maxillary left retained primary molar and impactedfirst permanent molar were removed; they had beenmaintained to assist with orthodontic anchorage andorthognathic surgery but were not restorable. Implants(3.5 mm Tapered Screwvent; Zimmer Biomet) wereplaced in the maxillary right premolar and maxillary leftmolar regions. Additionally, 3.5 mm diameter implants(Zimmer Biomet) were placed in the mandibular canineand central incisor sites, coordinating the position withimplants in the mandibular lateral incisor position placedwhen the patient was 10 years old (Fig. 11). Adequatespace between the mandibular lateral incisor implantswas planned for the initial implant surgery while takinginto account the space posterior to these implants andthe mental nerve position. The spacing was relativelypredictable, as no further significant growth was expectedin the anterior mandible.
Knobloch et al
Downloaded for scmh lib ([email protected]) at Show Chwan MemorFor personal use only. No other uses without permission.
In 2014, crown preparations were completed on themaxillary right permanent molar and central and lateralincisors. The existing composite resin restorations wereremoved, and caries was detected on the maxillary in-cisors. Both maxillary lateral incisors and the right centralincisor required endodontic treatment because of theextent of the caries. Definitive impressions for metal-ceramic crowns were made with polyvinyl siloxaneimpression material (Reprosil VPS Light Body and HeavyBody; Dentsply Sirona). Interim restorations were fabri-cated (Integrity Temporary Material; Dentsply Sirona)and cemented with interim cement (TempBond; KerrCorp). The metal-ceramic maxillary crowns were fabri-cated at the treatment vertical dimension of occlusionand luted with resin-modified glass ionomer cement(RelyX Luting Plus Resin-Modified Glass IonomerCement; 3M ESPE). Locator abutments (Zest AnchorsLLC) were seated and tightened to 30 Ncm for themaxillary implants (Fig. 12).
The maxillary RDP was designed using an extrac-oronal precision attachment system was used to assist
THE JOURNAL OF PROSTHETIC DENTISTRY
ial Hospital JC from ClinicalKey.com by Elsevier on June 04, 2018. Copyright ©2018. Elsevier Inc. All rights reserved.
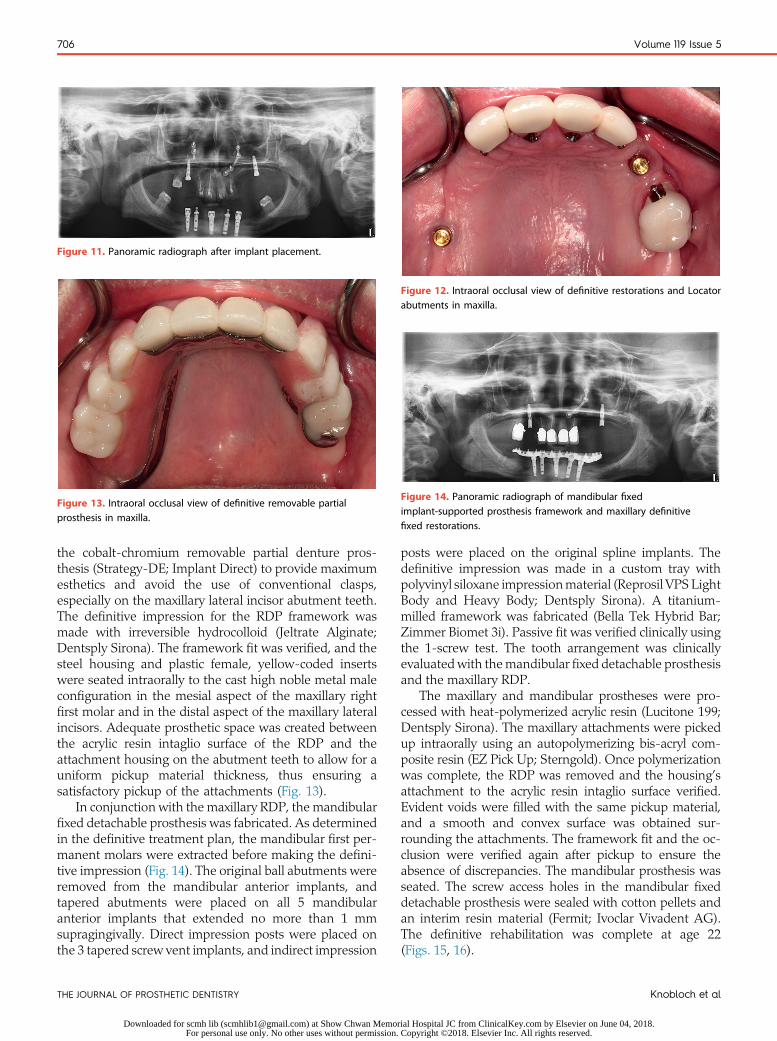
Figure 11. Panoramic radiograph after implant placement.
Figure 12. Intraoral occlusal view of definitive restorations and Locatorabutments in maxilla.
Figure 13. Intraoral occlusal view of definitive removable partialprosthesis in maxilla.
Figure 14. Panoramic radiograph of mandibular fixedimplant-supported prosthesis framework and maxillary definitivefixed restorations.
706 Volume 119 Issue 5
the cobalt-chromium removable partial denture pros-thesis (Strategy-DE; Implant Direct) to provide maximumesthetics and avoid the use of conventional clasps,especially on the maxillary lateral incisor abutment teeth.The definitive impression for the RDP framework wasmade with irreversible hydrocolloid (Jeltrate Alginate;Dentsply Sirona). The framework fit was verified, and thesteel housing and plastic female, yellow-coded insertswere seated intraorally to the cast high noble metal maleconfiguration in the mesial aspect of the maxillary rightfirst molar and in the distal aspect of the maxillary lateralincisors. Adequate prosthetic space was created betweenthe acrylic resin intaglio surface of the RDP and theattachment housing on the abutment teeth to allow for auniform pickup material thickness, thus ensuring asatisfactory pickup of the attachments (Fig. 13).
In conjunction with the maxillary RDP, the mandibularfixed detachable prosthesis was fabricated. As determinedin the definitive treatment plan, the mandibular first per-manent molars were extracted before making the defini-tive impression (Fig. 14). The original ball abutments wereremoved from the mandibular anterior implants, andtapered abutments were placed on all 5 mandibularanterior implants that extended no more than 1 mmsupragingivally. Direct impression posts were placed onthe 3 tapered screw vent implants, and indirect impression
THE JOURNAL OF PROSTHETIC DENTISTRY
Downloaded for scmh lib ([email protected]) at Show Chwan MemorFor personal use only. No other uses without permission.
posts were placed on the original spline implants. Thedefinitive impression was made in a custom tray withpolyvinyl siloxane impressionmaterial (Reprosil VPS LightBody and Heavy Body; Dentsply Sirona). A titanium-milled framework was fabricated (Bella Tek Hybrid Bar;Zimmer Biomet 3i). Passive fit was verified clinically usingthe 1-screw test. The tooth arrangement was clinicallyevaluatedwith themandibular fixed detachable prosthesisand the maxillary RDP.
The maxillary and mandibular prostheses were pro-cessed with heat-polymerized acrylic resin (Lucitone 199;Dentsply Sirona). The maxillary attachments were pickedup intraorally using an autopolymerizing bis-acryl com-posite resin (EZ Pick Up; Sterngold). Once polymerizationwas complete, the RDP was removed and the housing’sattachment to the acrylic resin intaglio surface verified.Evident voids were filled with the same pickup material,and a smooth and convex surface was obtained sur-rounding the attachments. The framework fit and the oc-clusion were verified again after pickup to ensure theabsence of discrepancies. The mandibular prosthesis wasseated. The screw access holes in the mandibular fixeddetachable prosthesis were sealed with cotton pellets andan interim resin material (Fermit; Ivoclar Vivadent AG).The definitive rehabilitation was complete at age 22(Figs. 15, 16).
Knobloch et al
ial Hospital JC from ClinicalKey.com by Elsevier on June 04, 2018. Copyright ©2018. Elsevier Inc. All rights reserved.
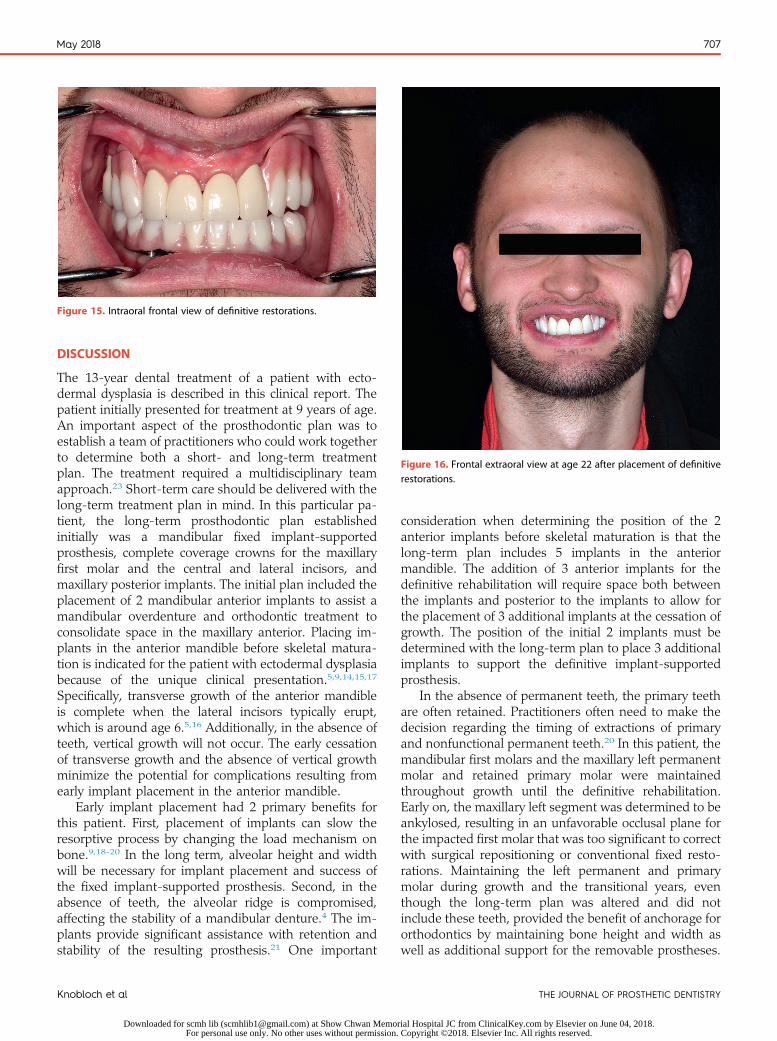
Figure 15. Intraoral frontal view of definitive restorations.
Figure 16. Frontal extraoral view at age 22 after placement of definitiverestorations.
May 2018 707
DISCUSSION
The 13-year dental treatment of a patient with ecto-dermal dysplasia is described in this clinical report. Thepatient initially presented for treatment at 9 years of age.An important aspect of the prosthodontic plan was toestablish a team of practitioners who could work togetherto determine both a short- and long-term treatmentplan. The treatment required a multidisciplinary teamapproach.23 Short-term care should be delivered with thelong-term treatment plan in mind. In this particular pa-tient, the long-term prosthodontic plan establishedinitially was a mandibular fixed implant-supportedprosthesis, complete coverage crowns for the maxillaryfirst molar and the central and lateral incisors, andmaxillary posterior implants. The initial plan included theplacement of 2 mandibular anterior implants to assist amandibular overdenture and orthodontic treatment toconsolidate space in the maxillary anterior. Placing im-plants in the anterior mandible before skeletal matura-tion is indicated for the patient with ectodermal dysplasiabecause of the unique clinical presentation.5,9,14,15,17
Specifically, transverse growth of the anterior mandibleis complete when the lateral incisors typically erupt,which is around age 6.5,16 Additionally, in the absence ofteeth, vertical growth will not occur. The early cessationof transverse growth and the absence of vertical growthminimize the potential for complications resulting fromearly implant placement in the anterior mandible.
Early implant placement had 2 primary benefits forthis patient. First, placement of implants can slow theresorptive process by changing the load mechanism onbone.9,18-20 In the long term, alveolar height and widthwill be necessary for implant placement and success ofthe fixed implant-supported prosthesis. Second, in theabsence of teeth, the alveolar ridge is compromised,affecting the stability of a mandibular denture.4 The im-plants provide significant assistance with retention andstability of the resulting prosthesis.21 One important
Knobloch et al
Downloaded for scmh lib ([email protected]) at Show Chwan MemorFor personal use only. No other uses without permission.
consideration when determining the position of the 2anterior implants before skeletal maturation is that thelong-term plan includes 5 implants in the anteriormandible. The addition of 3 anterior implants for thedefinitive rehabilitation will require space both betweenthe implants and posterior to the implants to allow forthe placement of 3 additional implants at the cessation ofgrowth. The position of the initial 2 implants must bedetermined with the long-term plan to place 3 additionalimplants to support the definitive implant-supportedprosthesis.
In the absence of permanent teeth, the primary teethare often retained. Practitioners often need to make thedecision regarding the timing of extractions of primaryand nonfunctional permanent teeth.20 In this patient, themandibular first molars and the maxillary left permanentmolar and retained primary molar were maintainedthroughout growth until the definitive rehabilitation.Early on, the maxillary left segment was determined to beankylosed, resulting in an unfavorable occlusal plane forthe impacted first molar that was too significant to correctwith surgical repositioning or conventional fixed resto-rations. Maintaining the left permanent and primarymolar during growth and the transitional years, eventhough the long-term plan was altered and did notinclude these teeth, provided the benefit of anchorage fororthodontics by maintaining bone height and width aswell as additional support for the removable prostheses.
THE JOURNAL OF PROSTHETIC DENTISTRY
ial Hospital JC from ClinicalKey.com by Elsevier on June 04, 2018. Copyright ©2018. Elsevier Inc. All rights reserved.
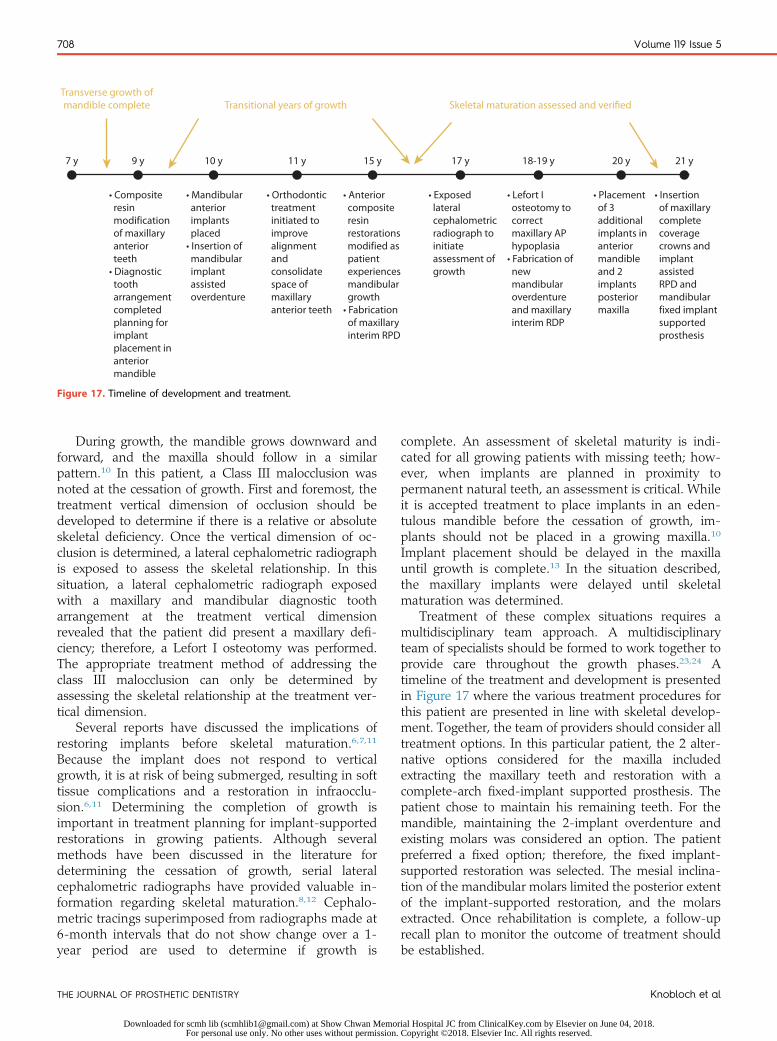
• Composite resin modification of maxillary anterior teeth• Diagnostic tooth arrangement completed planning for implant placement in anterior mandible
• Mandibular anterior implants placed• Insertion of mandibular implant assisted overdenture
• Orthodontic treatment initiated to improve alignment and consolidate space of maxillary anterior teeth
• Anterior composite resin restorations modified as patient experiences mandibular growth• Fabrication of maxillary interim RPD
• Exposed lateral cephalometric radiograph to initiate assessment of growth
• Lefort I osteotomy to correct maxillary AP hypoplasia• Fabrication of new mandibular overdenture and maxillary interim RDP
• Placement of 3 additional implants in anterior mandible and 2 implants posterior maxilla
• Insertion of maxillary complete coverage crowns and implant assisted RPD and mandibular fixed implant supported prosthesis
9 y
Transverse growth ofmandible complete Transitional years of growth Skeletal maturation assessed and verified
10 y 11 y 15 y 17 y 18-19 y 20 y 21 y7 y
Figure 17. Timeline of development and treatment.
708 Volume 119 Issue 5
During growth, the mandible grows downward andforward, and the maxilla should follow in a similarpattern.10 In this patient, a Class III malocclusion wasnoted at the cessation of growth. First and foremost, thetreatment vertical dimension of occlusion should bedeveloped to determine if there is a relative or absoluteskeletal deficiency. Once the vertical dimension of oc-clusion is determined, a lateral cephalometric radiographis exposed to assess the skeletal relationship. In thissituation, a lateral cephalometric radiograph exposedwith a maxillary and mandibular diagnostic tootharrangement at the treatment vertical dimensionrevealed that the patient did present a maxillary defi-ciency; therefore, a Lefort I osteotomy was performed.The appropriate treatment method of addressing theclass III malocclusion can only be determined byassessing the skeletal relationship at the treatment ver-tical dimension.
Several reports have discussed the implications ofrestoring implants before skeletal maturation.6,7,11
Because the implant does not respond to verticalgrowth, it is at risk of being submerged, resulting in softtissue complications and a restoration in infraocclu-sion.6,11 Determining the completion of growth isimportant in treatment planning for implant-supportedrestorations in growing patients. Although severalmethods have been discussed in the literature fordetermining the cessation of growth, serial lateralcephalometric radiographs have provided valuable in-formation regarding skeletal maturation.8,12 Cephalo-metric tracings superimposed from radiographs made at6-month intervals that do not show change over a 1-year period are used to determine if growth is
THE JOURNAL OF PROSTHETIC DENTISTRY
Downloaded for scmh lib ([email protected]) at Show Chwan MemorFor personal use only. No other uses without permission.
complete. An assessment of skeletal maturity is indi-cated for all growing patients with missing teeth; how-ever, when implants are planned in proximity topermanent natural teeth, an assessment is critical. Whileit is accepted treatment to place implants in an eden-tulous mandible before the cessation of growth, im-plants should not be placed in a growing maxilla.10
Implant placement should be delayed in the maxillauntil growth is complete.13 In the situation described,the maxillary implants were delayed until skeletalmaturation was determined.
Treatment of these complex situations requires amultidisciplinary team approach. A multidisciplinaryteam of specialists should be formed to work together toprovide care throughout the growth phases.23,24 Atimeline of the treatment and development is presentedin Figure 17 where the various treatment procedures forthis patient are presented in line with skeletal develop-ment. Together, the team of providers should consider alltreatment options. In this particular patient, the 2 alter-native options considered for the maxilla includedextracting the maxillary teeth and restoration with acomplete-arch fixed-implant supported prosthesis. Thepatient chose to maintain his remaining teeth. For themandible, maintaining the 2-implant overdenture andexisting molars was considered an option. The patientpreferred a fixed option; therefore, the fixed implant-supported restoration was selected. The mesial inclina-tion of the mandibular molars limited the posterior extentof the implant-supported restoration, and the molarsextracted. Once rehabilitation is complete, a follow-uprecall plan to monitor the outcome of treatment shouldbe established.
Knobloch et al
ial Hospital JC from ClinicalKey.com by Elsevier on June 04, 2018. Copyright ©2018. Elsevier Inc. All rights reserved.

May 2018 709
SUMMARY
The dental rehabilitation of a patient with ectodermaldysplasia presents several challenges to the practitioner.The team of dental specialists must establish both short-and long-term goals and work together to achieve afavorable result. Communication between the variouspractitioners at all stages is critical to accomplish a pos-itive outcome. This report presents early implant place-ment in a 9-year-old boy with ectodermal dysplasia andthe transitional treatment completed throughout skeletalmaturation over the course of 13 years to achievedefinitive rehabilitation. Early implant placement pro-vided the benefit of a functional mandibular prosthesisassisted by 2 anterior implants throughout growth. Thelocation of the early mandibular anterior implants wasplanned and carried out to allow for the addition of 3additional implants at the cessation of growth to supportthe definitive mandibular fixed implant-supported pros-thesis. Care is administered at each stage of treatmentthat is guided by the long-term goals established by theteam of providers.
REFERENCES
1. Bergendal B. Orodental manifestations in ectodermal dysplasia-a review. AmJ Med Genet A 2014;164A:2465-71.
2. Zou D, Wu Y, Wang XD, Huang W, Zhang Z. A retrospective 3- to 5-yearstudy of the reconstruction of oral function using implant-supported pros-theses in patients with hypohidrotic ectodermal dysplasia. J Oral Implan-tology 2014;5:571-9.
3. Deshmukh S, Prashanth S. Ectodermal dysplasia: a genetic review. Int J ClinPediatr Dent 2012;5:197-202.
4. Trivedi B, Bhati R. Complete and removable partial prosthesis for a child withhypohidrotic ectodermal dysplasia. Int J Pediatr Dent 2012;6:71-4.
5. Guckes AD, McCarthy GR, Brahmin J. Use of endosseous implants in a 3 yearold with ectodermal dysplasia. Case report and 5 year follow up. Pediatr Dent1997;19:282-5.
6. Brugnolo E, Mazzocco C, Cardioli G, Majzoub Z. Clinical and radiographicfindings following placement of single tooth implants in young patients-casereports. Int J Periodontics Restorative Dent 1996;16:421-33.
7. Percinoto C, Vieiera AE, Barbieri CM, Melhado FL, Moriera KS. Use of dentalimplants in children: a literature review. Quintessence Int 2001;32:381-3.
8. Brahmin JS. Dental implants in children. Oral Maxillofacial Surg Clin N Am2005;17:375-81.
Knobloch et al
Downloaded for scmh lib ([email protected]) at Show Chwan MemorFor personal use only. No other uses without permission.
9. Mishra SK, Chowdhary N, Chowdhary R. Dental implants in growing chil-dren. J Indian Soc Pedod Prev Dent 2013;31:3-9.
10. Cronin RJ, Oesterle LJ. Implant use in growing patients. Treatment planningconcerns. Dent Clin North Am 1998;42:1-33.
11. Ledermann PD, Hasell TM, Hefti AF. Osseointegrated dental implants asalternative therapy to bridge construction or orthodontics in the young pa-tients seven years of clinical experience. Pediatr Dent 1993;15:327-33.
12. Bhalla G, Agrawal K, Singh K, Singh B, Goel P. A preliminary study toanalyze the cranio-facial growth of an ectodermal dysplasia patient afterprosthetic rehabilitation. J Indian Prosthodont Soc 2013;13:43-8.
13. Mankani N, Chowdhary R, Patil B, Nagaraj E, Mandalli P. Osseointegrateddental implants in growing children: a literature review. J Oral Implantol2014;40:627-31.
14. Mittal M, Srivastava D, Kumar A, Sharma P. Dental management of hypo-hidrotic ectodermal dysplasia: a report of two cases. Contemp Clin Dent2015;6:414-7.
15. Kramer FJ, Baethge G, Tschernitschek H. Implants in children with ecto-dermal dysplasia. A case report and literature review. Clin Oral Implants Res2007;18:140-6.
16. Cronin RJ, Oesterle LJ, Ranly DM. Mandibular implants and the growingpatient. Int J Oral Maxillofac Implants 1994;9:55-62.
17. Filius MA, Vissink A, Raghoebar GM, Visser A. Implant-retained over-dentures for young children with severe oligodontia: a series of four cases.J Oral Maxillofac Surg 2014;72:1684-90.
18. Bergendal B. The role of prosthodontists in habilitation and rehabilitation ofrare disorders. The ectodermal dysplasia experience. Int J Prosthodont2001;14:466-70.
19. Bergendal B. Prosthetic habilitation of a young patient with hypohidroticectodermal dysplasia and oligodonita: a case report of 20 years of treatment.Int J Prosthodont 2001;14:471-9.
20. Bergendal B. When should we extract teeth and place implants in youngindividuals with tooth agenesis? J Oral Rehabil 2008;35(suppl 1):55-63.
21. Mericske-Stern R, Zarb GA. Overdentures: an alternative implant method-ology for edentulous patients. Int J Prosthodont 1993;6:203-8.
22. Kilic S, Altintas SH, Yilmaz Altintas N, Ozkaynak O, Bayram M, Kusgoz A,et al. Six-year survival of a mini dental implant-retained overdenture in achild with ectodermal dysplasia. J Prosthodont 2017;26:70-4.
23. Hobkirk JA, Nohl F, Bergendal B, Richter MK. The management of ecto-dermal dysplasia and severe hypodontia. International conference state-ments. J Oral Rehabil 2006;33:634-7.
24. Van Sickels J, Raybould T, Hicks E. Interdisciplinary management of patientswith ectodermal dysplasia. J Oral Implantol 2010;36:239-45.
25. Stanford CM, Gukes A, Fete M, Srun S, Richter MK. Perceptions of outcomesof implant therapy in patients with ectodermal dysplasia syndromes. Int JProsthodont 2008;21:195-200.
Corresponding author:Dr Lisa A. KnoblochDivision of Restorative Science and ProsthodonticsThe Ohio State University College of Dentistry305 West 12th AveColumbus, OH 43210Email: [email protected]
Copyright © 2017 by the Editorial Council for The Journal of Prosthetic Dentistry.
THE JOURNAL OF PROSTHETIC DENTISTRY
ial Hospital JC from ClinicalKey.com by Elsevier on June 04, 2018. Copyright ©2018. Elsevier Inc. All rights reserved.