early mobility in the icu, how is it going?...early mobility in the icu, how is it going? ucsf...
TRANSCRIPT
5/30/2014
1
Early Mobility in the ICU, How is It Going?
UCSF Critical Care & Trauma Medicine Conference May 29-31 2014
Presented by Heidi Engel, PT, DPT
Why Early ICU Patient Mobility?
Diaphragm muscle thinning and atrophy begins within 18 to 48 hours after intubation
Levine, S., T. Nguyen, et al. (2008). "Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans." N Engl J Med 358 (13): 1327-1335.
Grosu HB, Lee YI, Lee J, Eden E, Eikermann M, Rose KM: Diaphragm muscle thinning in patients who are mechanically ventilated. Chest 2012, 142(6):1455-1460.
Rectus Femoris protein breakdown begins within 24 hours of ICU admission, cross sectional area declining rapidly during first week Puthucheary ZA, Rawal J, McPhail M, Connolly B, Ratnayake G, Chan P, Hopkinson NS, Padhke R, Dew T, Sidhu PS et al: Acute Skeletal Muscle Wasting in Critical Illness. Jama 2013.
Why Early ICU Patient Mobility?
The duration of bed rest during critical illness was consistently associated with weakness throughout 24-month follow-up. Fan E, Dowdy DW, Colantuoni E, Mendez-Tellez PA, Sevransky JE, Shanholtz C, Himmelfarb CR, Desai SV, Ciesla N, Herridge MS et al: Physical Complications in Acute Lung Injury Survivors: A 2-Year Longitudinal Prospective Study. Crit Care Med 2013.
Based on available evidence, early exercise/PT seems to be the only treatment yet shown to improve long-term physical function of ICU survivors. Calvo-Ayala E, Khan BA, Farber MO, Ely EW, Boustani MA: Interventions to improve the physical function of ICU survivors: a systematic review. Chest 2013, 144(5):1469-1480.
Astronauts are on Bed Rest
They exercise for at least 2 hours/day to counter the adverse effects to their bone density and muscles
5/30/2014
2
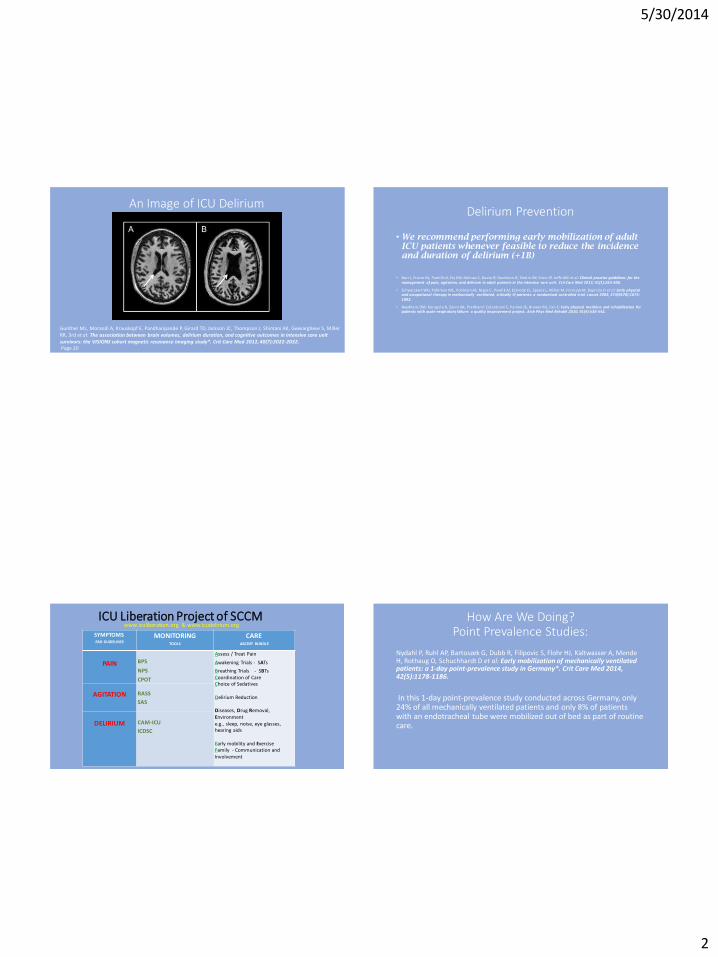
An Image of ICU Delirium
Gunther ML, Morandi A, Krauskopf E, Pandharipande P, Girard TD, Jackson JC, Thompson J, Shintani AK, Geevarghese S, Miller RR, 3rd et al: The association between brain volumes, delirium duration, and cognitive outcomes in intensive care unit survivors: the VISIONS cohort magnetic resonance imaging study*. Crit Care Med 2012, 40(7):2022-2032. Page 20
Delirium Prevention
• We recommend performing early mobilization of adult ICU patients whenever feasible to reduce the incidence and duration of delirium (+1B)
• Barr J, Fraser GL, Puntil lo K, Ely EW, Gelinas C, Dasta JF, Davidson JE, Devlin JW, Kress JP, Joffe AM et al: Clinical practice guidelines for the
management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit Care Med 2013, 41(1):263-306.
• Schweickert WD, Pohlman MC, Pohlman AS, Nigos C, Pawlik AJ, Esbrook CL, Spears L, Miller M, Franczyk M, Deprizio D et al: Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial. Lancet 2009, 373(9678):1874-1882.
• Needham DM, Korupolu R, Zanni JM, Pradhan P, Colantuoni E, Palmer JB, Brower RG, Fan E: Early physical medicine and rehabilitation for patients with acute respiratory failure: a quality improvement project. Arch Phys Med Rehabil 2010, 91(4):536-542.
ICU Liberation Project of SCCM SYMPTOMS
PAD GUIDELINES MONITORING
TOOLS
CARE
ABCDEF BUNDLE
PAIN
BPS
NPS
CPOT
Assess / Treat Pain
Awakening Trials - SATs
Breathing Trials - SBTs Coordination of Care Choice of Sedatives Delirium Reduction Diseases, Drug Removal, Environment e.g., sleep, noise, eye glasses, hearing aids Early mobility and Exercise Family - Communication and Involvement
AGITATION
RASS
SAS
DELIRIUM
CAM-ICU
ICDSC
www.iculiberation.org & www.icudelirium.org How Are We Doing?
Point Prevalence Studies:
Nydahl P, Ruhl AP, Bartoszek G, Dubb R, Filipovic S, Flohr HJ, Kaltwasser A, Mende H, Rothaug O, Schuchhardt D et al: Early mobilization of mechanically ventilated patients: a 1-day point-prevalence study in Germany*. Crit Care Med 2014, 42(5):1178-1186.
In this 1-day point-prevalence study conducted across Germany, only 24% of all mechanically ventilated patients and only 8% of patients with an endotracheal tube were mobilized out of bed as part of routine care.

5/30/2014
3
How Are We Doing? Point Prevalence Studies:
Berney SC, Harrold M, Webb SA, Seppelt I, Patman S, Thomas PJ, Denehy L: Intensive care unit mobility practices in Australia and New Zealand: a point prevalence study. Crit Care Resusc 2013, 15(4):260-265.
45% were mechanically ventilated. Mobilisation activities were classified into five categories that were not mutually exclusive: 140 patients (28%) completed an in-bed exercise regimen, 93 (19%) sat over the side of the bed, 182 (37%) sat out of bed, 124 (25%) stood and 89 (18%) walked. Predefined adverse events occurred on 24 occasions (5%). No patient requiring mechanical ventilation sat out of bed or walked.
How Are We Doing? Point Prevalence Studies:
Terri Hough University of Washington Medical Center, Presenting at The 7th International Physical Medicine and Rehabilitation of Critically Ill Patients Meeting 5/17/2014, Across the US:
64% of ICU patients experienced any activity, 50% of those were bed level activity, 20% of those were transfers to a chair, 10% of those were walking
Profoundly variable practice patterns
Moving From Information to Practice: How Exercise Can Help You Live Longer By GRETCHEN REYNOLDS, April 2, 2014, New York Times
Having unhealthy cholesterol numbers, elevated blood pressure or an expanding waistline substantially increases your chances of developing heart disease. But an encouraging new study finds that exercise may slash that risk, even if your other risk factors stay high.
Top 10 Excuses for Keeping An ICU Patient Immobile
5/30/2014
4
SAFETY:
Excuse: The Patient is too…,
Excuse # 1. SAFETY: The patient is too sick, or too big
TRUE: New onset sepsis or respiratory distress (think of hours NOT days)
Unstable bleeding or surgical site
Terminal disease (comfort care measures),
Comatose
Acute unstable cardiovascular event
Solution # 1. SAFETY: The patient is too sick, or too big
Collaborate with RN,RT, MD
Use Clinical judgment
Every diagnosis in context
Context
Is it a beautiful sunny day after so much rain, or are we in the middle of a drought?
5/30/2014
5
Excuse # 1. SAFETY: The patient is too sick, or too big
FALSE: The patient has a DVT (reference the American College of Chest Physicians 2012 guidelines: people with acute DVT do not need a period of bed rest)
FALSE: The obese patient was admitted able to walk at home (think of how crucial prevention can be)
FALSE: The patient is on ARDS Net Protocol
FALSE: The patient is a new admit to the ICU
Excuse # 2. SAFETY: The patient is too sleepy RASS -1 to -4 Hypoactive delirious Goal targeted sedation?
True: Delirium is Brain Failure Brain Failure Looks Like This
Solution# 2. SAFETY: The patient is too sleepy
Collaborate with RN,RT, MD
Use Clinical judgment
Every level of delirium
in context
Consider the environment
5/30/2014
6
Solution# 2. SAFETY: The patient is too sleepy and may respond well to being up
Excuse # 3. SAFETY: The patient is too agitated
Solution # 3. SAFETY: The patient is too agitated Society of Critical Care Medicine Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium
“We recommend performing early mobilization of adult ICU patients whenever feasible to reduce the incidence and duration of delirium” (+1B)
• Barr J, Fraser GL, Punti l lo K, Ely EW, Gel inas C, Dasta JF, Davidson JE, Devl in JW, Kress JP, Joffe AM et al: Clinical practice guidelines for the
management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit Care Med 2013, 41(1):263-306.
• Schweickert WD, Pohlman MC, Pohlman AS, Nigos C, Pawl ik AJ, Esbrook CL, Spears L, Mi l ler M, Franczyk M, Deprizio D et al: Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial. Lancet 2009, 373(9678):1874-1882.
• Needham DM, Korupolu R, Zanni JM, Pradhan P, Colantuoni E, Pa lmer JB, Brower RG, Fan E: Early physical medicine and rehabilitation for patients with acute respiratory failure: a quality improvement project. Arch Phys Med Rehabil 2010, 91(4):536-542.
Excuse # 4. SAFETY: the patient has challenging lines or endotracheal tube

5/30/2014
7
What About All Those Critical Lines?
Patient lines and drains can be accommodated
Including Femoral Lines
Mechanical ventilation and CVVH lines
Damluji, A., et al. (2013). "Safety and feasibility of femoral catheters during physical rehabilitation in the intensive care unit." J Crit Care.
Winkelman, C. (2011). "Ambulating with pulmonary artery or femoral catheters in place." Crit Care Nurse 31(5): 70-73.
What About All Those Critical Lines?
Lines, catheters and drains can be accommodated, secured
EVD line stationary bike
Excuse #5 Timing: The patient is leaving
The patient is going for:
A procedure
A CT scan
Transferring to the floor
Will be extubated soon
Solution #5 Timing: Soon to be Extubated
Activity trumps extubation:
A pre- and post-activity rest period with assist-control ventilation for 30 min was employed as needed to support early activity.
If the patient was intubated and able to participate in activity, the FIO2 was increased by 0.2 before initiation of activity. We deferred ventilator weaning in support of activity, as necessary.
Bailey P, Thomsen GE, Spuhler VJ, Blair R, Jewkes J, Bezdjian L, Veale K, Rodriquez L, Hopkins RO: Early activity is feasible and safe in respiratory failure patients. Crit Care Med 2007, 35(1):139-145.

5/30/2014
8
Excuse #6 Timing: The patient needs a nap
The patient
Had a bad night
Feels tired
Didn’t sleep last night
Wants to sleep now to make up for it
Kamdar BB, Needham DM, Collop NA: Sleep deprivation in critical illness: its role in physical and psychological recovery. Journal of intensive care medicine 2012, 27(2):97-111.
Solution #6 Timing: The patient needs a nap
Schedule a time
Create a sleep hygiene program in your ICU
Address night staff as well as day
Set circadian rhythms
Excuse #7 Staffing/Equipment : No one is available to manage the lines
No portable ventilator
No high back chairs
No minimal lift equipment
No full time PT
Lord RK, Mayhew CR, Korupolu R, Mantheiy EC, Friedman MA, Palmer JB, Needham DM: ICU early physical rehabilitation programs: financial modeling of cost savings. Crit Care Med 2013, 41(3):717-724.
Solution # 7. Staffing/Equipment Overcome the Barriers
Establish the program for your local culture
Begin with the easier smaller success stories
Collect data to evaluate and re-evaluate
• Kress JP: Sedation and mobility: changing the paradigm. Crit
Care Clin 2013, 29(1):67-75.
5/30/2014
9
Excuse#8 Staffing/Equipment : My other patient is too sick, I can’t help or watch this patient
Solution #8. Patients Expectations and Patient Centered Goals
Returning to life as they knew it
Not a new life of disability or perpetual patient
Misak C: ICU psychosis and patient autonomy: some thoughts from the inside. The Journal of medicine and philosophy 2005, 30(4):411-430.
Muller M, Strobl R, Grill E: Goals of patients with rehabilitation needs in acute hospitals: goal achivement is an indicator for improved functioning. J Rehabil Med 2011, 43(2):145-150.
What Are the Expectations? Excuse #9. Staffing/Equipment : the attending MD doesn’t think it’s a going to work for this patient

5/30/2014
10
Solution # 9. Learning opportunities
Engel HJ, Needham DM, Morris PE, Gropper MA: ICU early mobilization: from recommendation to implementation at three medical centers. Crit Care Med 2013, 41(9 Suppl 1):S69-80.
Excuse #10. Staffing/Equipment : The physical therapist is not here
The PT has higher priority patients outside the ICU
The PT leaves the difficult
to transfer patient in the chair
Solution #10. Staffing Equipment : the PT is not here
Build the case for a full time dedicated ICU PT
Lord RK, Mayhew CR, Korupolu R, Mantheiy EC, Friedman MA, Palmer JB, Needham DM: ICU early physical rehabilitation programs: financial modeling of cost savings. Crit Care Med 2013, 41(3):717-724.
Plan ahead and coordinate care
In Summary
Critical illness is catabolic and depleting, rapidly and potentially lasting for years
A prolonged ICU stay can cause delirium and cognitive changes for most patients
Mobility combined with minimal or no sedation started at the beginning of an ICU stay is protective and preventative
Approach the task with structured QI project, collaboration, barrier identification

5/30/2014
11
Mobility is Life
Early mobility is profoundly beneficial to your patients
Don’t be afraid, they do better than you expect
It is a MULTIDISCIPLINE task