early pregnancy problems feras izzat consultant gynaecologist – egu/epau lead university hospitals...
TRANSCRIPT

Early Pregnancy ProblemsFeras IzzatConsultant Gynaecologist – EGU/EPAU LeadUniversity Hospitals Coventry & Warwickshire NHS Trust

IntroductionIntroduction
• Ectopic Pregnancy
• Bleeding in early pregnancy and miscarriage
• Gestational Trophoblastic Disease

Ectopic Pregnancy

DefinitionDefinition
• Pregnancy occurring outside uterine cavity
• Approx 11/1000 of pregnancies – rate increasing
• Maternal mortality in 1/2500 ectopic pregnancies (11
deaths in most recent report)

SiteSite
• Tubal – Interstitial 2.4%– Isthmic 12%– Ampullary 70%– Fimbrial 11.1%
• Non Tubal– Ovary– Abdominal cavity– Cervix– CS Scar

Risk factorsRisk factors
• Previous PID • Previous ectopic pregnancy • Previous tubal surgery (e.g. sterilisation, reversal) • Pregnancy in the presence of IUCD
• POP
• ART (IVF)

SymptomsSymptoms
• Acute– Low abdominal pain – peritoneal irritation by blood
– Vaginal bleeding – shedding of decidua
– Shoulder tip pain – referred from diaphragm
– Fainting - hypovolaemia
• Chronic (Atypical)– Asymptomatic, gastrointestinal symptoms
SignsSigns
• Abdominal tenderness
• Adnexal tenderness / mass
• Shock – tachycardia, hypotension, pallor
• None
DiagnosisDiagnosis
• Ultrasound– Empty uterus, adnexal mass, free fluid, occasionally live
pregnancy outside of uterus
• Serum βhCG & Progesterone
• Laparoscopy

Ultrasound

Ultarsound
• Trans-Vaginal Ultrasonography
• Sensitivity 100%, specificity 98.2%.
• The positive predictive value 98%, and the negative predictive value was 100%
• FH seen in 23%
• Timor-Tritsch et al, 1990 Am J Obstet Gynecol.

Left Ectopic on laparoscopy

ManagementManagement
• Conservative – hCG <1000 , Progesterone < 5 stable, success 70%
• Medical– Methotrexate – hCG <4000 mass < 3cm, success 84%.
Susequent IUP 54% recurrent EP 8%
• Surgical - Laparoscopy– Salpingectomy, IUP 38.3%, EP 9.8– Salpingotomy, IUP 61.1%, EP 15.5
Yao et al, Fertility Sterility 1997

PUL
• Pregnancy of unknown location (PUL) - positive pregnancy test with no signs of intra- or extrauterine pregnancy on transvaginal sonography (TVS).
• 15-20% of all EPAU scans
• Management should be expectant if stable with an initial serum progesterone (<20) and a hCG ratio 0h/48h of <0.87
• Condous et al, Ultrasound Obstet Gynecol 2006

Bleeding in Early Pregnancy & Miscarriage

DefinitionsDefinitions
• Threatened miscarriage Vaginal bleeding at < 24 weeks gestation
• Delayed (silent) miscarriage Gestational sac with/without fetus present
(but no FH)
• Recurrent miscarriage 3 or more consecutive miscarriages (with
or without a known cause)

MiscarriageMiscarriage
• Approximately 30% of pregnant women will experience bleeding in early pregnancy
• At least 50% of women with threatened miscarriage will have continuing pregnancy
• Miscarriage occurs in 15-20% of clinically diagnosed pregnancies

Causes of miscarriageCauses of miscarriage
• Genetic abnormalities 85%
• Maternal illness e.g. diabetes, Thyroid disease
• Phospholipid / Lupus – 15% recurrent miscarriages
• Uterine abnormalities
• ‘Cervical incompetence’
• Progesterone deficiency?

History
• LMP
• When?
• Amount?
• Pain?
• Timing of Pain

Examination
• ABC (vital signs)
• Abdominal
• Vaginal (speculum)– Cx state
– Amount of bleeding

Cusc’o speculum Sim’s speculum

InvestigationsInvestigations
Ideally in dedicated ‘Early Pregnancy Assessment Unit’
• Ultrasound
• Measurement of serum βhCG
• Determination of blood & Rhesus group
• FBC, G&S and admit if significant bleeding
• Psychological support

UltrasoundUltrasound
• Expect to see viable fetus from around 6.5 weeks transabdominally, 5.5 weeks transvaginally
• Diagnosis can be made on TVS only
• CRL ≥ 7mm
• Empty GS with a mean diameter ≥ 25 mm

Gestational sac
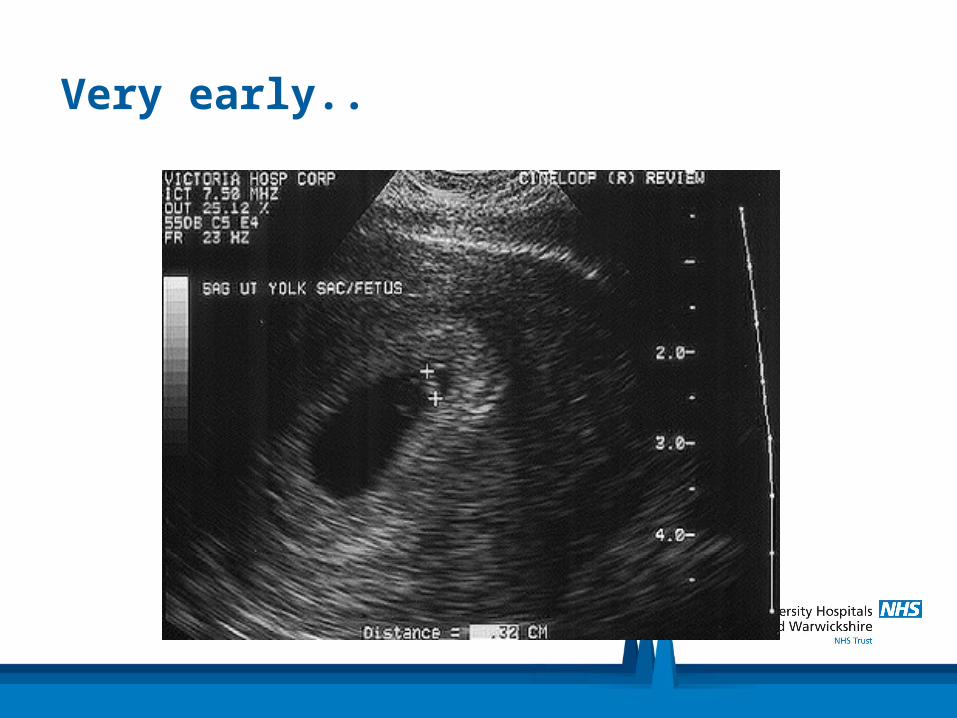
Very early..

Normal 8-9 wk pregnancy

Empty sac

Measurement of Measurement of ββhCGhCG
• Not necessary if diagnosis unequivocal on scan
• Useful as part of investigations to diagnose / exclude extrauterine pregnancy
• Doubling time approx 2 days in viable pregnancy
• Halving time 1-2 days in complete miscarriage
• Should see fetal pole with βhCG of 1500-2000

Management of incomplete miscarriageManagement of incomplete miscarriage
• Conservative 76% success
• Medical mifipristone & misoprostol – 82% success
• Nielsen et al, BJOG 1999
• Surgical (ERPC) No difference in satisfaction rate than medical – 95%
• Chipchase et al, BJOG 1995

Recurrent miscarriage• Loss of 3 or more consecutive pregnancies
• Affects 1% of women in reproductive age group
• Investigations can identify up to 50% with a cause
• Women aged <=30 years have a subsequent miscarriage rate of 25% which rises to 52% in women aged >=40 years.
• The risk of a subsequent miscarriage is 29% after 3 miscarriages, this rises to 53% in 6 or more previous miscarriages
• Clifford et al, Human Reproduction 1997

Gestational Trophoblastic Disease

GTD
• The abnormal proliferation of gestational trophoblast tissue
• Spectrum of disease
• Pre-Malignant
– Partial Molar Pregnancy
– Complete Molar Pregnancy
• Malignant
– Invasive mole
– Choriocarcinoma
– Placental site trophoblastic tumours
Molar PregnancyMolar Pregnancy
• 1 in 1000 live births
• Partial– Partial moles are triploid with 2 sets of paternal and 1 set of
maternal chromosomes– An embryo often present that dies at 8-9 weeks– 0.5% need chemotherapy for invasive disease
• Complete– No fetal pole, diplod chromosomes paternally derived –
androgenetic– No embryo– Chemo therapy rate 8-20%


PresentationPresentation
• Vaginal bleeding
• Excessive N&V ‘Hyperemesis gravidarum’
• Uterus large for dates

DiagnosisDiagnosis
• Ultrasound
• Histology after surgical evacuation



Complete mole at hysterectomy

Follow-upFollow-up
• Monitor via regional centre – London, Sheffield, Dundee
• CM – 8-20% risk of invasive disease
• PM – 0.5%
• Choriocarcinoma may follow any subsequent pregnancy – miscarriage, TOP, term delivery
• Choriocarcinoma is curable
• Monitor βhCG levels to check resolution – for 6 months to 2 years